Gender-Related Patterns of Emotion Regulation among Patients with Eating Disorders

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Assessment
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. ER and Negative Affect Measures and Comparison between Groups
3.3. Comparison of ER between ED Subtypes
3.4. Predictive Capacity of the Study Variables on ER
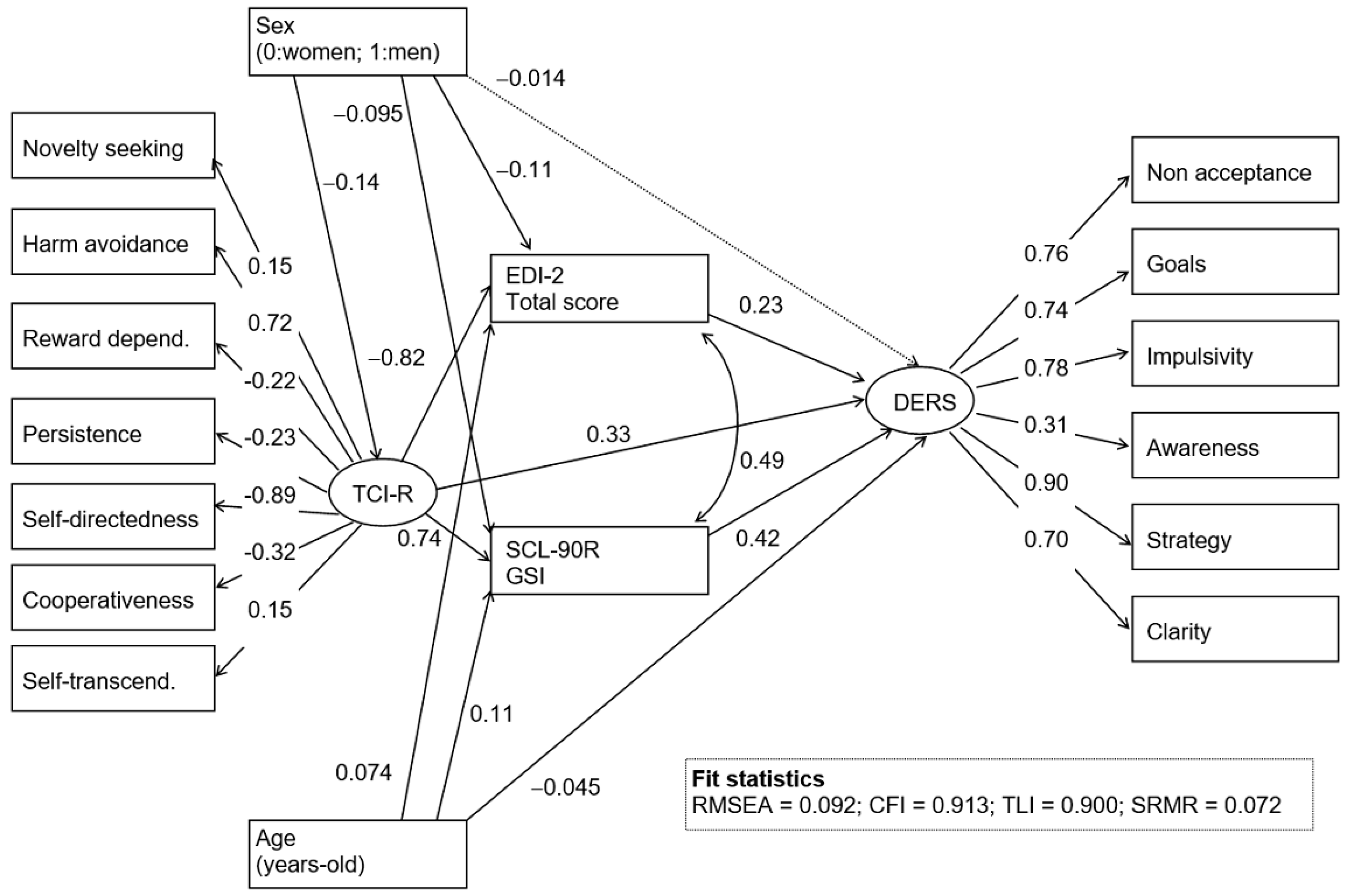
3.5. Pathways Analysis
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gratz, K.L.; Weiss, N.H.; Tull, M.T. Examining emotion regulation as an outcome, mechanism, or target of psychological treatments. Curr. Opin. Psychol. 2015, 3, 85–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neacsiu, A.D.; Herr, N.R.; Fang, C.M.; Rodriguez, M.A.; Rosenthal, M.Z. Identity disturbance and problems with emotion regulation are related constructs across diagnoses. J. Clin. Psychol. 2015, 71, 346–361. [Google Scholar] [CrossRef]
- Sloan, E.; Hall, K.; Moulding, R.; Bryce, S.; Mildred, H.; Staiger, P.K. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: A systematic review. Clin. Psychol. Rev. 2017, 57, 141–163. [Google Scholar] [CrossRef]
- Macht, M. How emotions affect eating: A five-way model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef]
- Brockmeyer, T.; Skunde, M.; Wu, M.; Bresslein, E.; Rudofsky, G.; Herzog, W.; Friederich, H.C. Difficulties in emotion regulation across the spectrum of eating disorders. Compr. Psychiatry 2014, 55, 565–571. [Google Scholar] [CrossRef]
- Kittel, R.; Brauhardt, A.; Hilbert, A. Cognitive and emotional functioning in binge-eating disorder: A systematic review. Int. J. Eat. Disord. 2015, 48, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Haynos, A.F.; Roberto, C.A.; Attia, E. Examining the associations between emotion regulation difficulties, anxiety, and eating disorder severity among inpatients with anorexia nervosa. Compr. Psychiatry 2015, 60, 93–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, T.E.; Singleton, C.; Carter, J.C. Testing predictions of the emotion regulation model of binge-eating disorder. Int. J. Eat. Disord. 2017, 50, 1297–1305. [Google Scholar] [CrossRef]
- Schaumberg, K.; Welch, E.; Breithaupt, L.; Hübel, C.; Baker, J.H.; Munn-Chernoff, M.A.; Yilmaz, Z.; Ehrlich, S.; Mustelin, L.; Ghaderi, A.; et al. The science behind the academy for eating disorders’ nine truths about eating disorders. Eur. Eat. Disord. Rev. 2017, 25, 432–450. [Google Scholar] [CrossRef]
- Svaldi, J.; Caffier, D.; Tuschen-Caffier, B. Emotion suppression but not reappraisal increases desire to binge in women with binge eating disorder. Psychother. Psychosom. 2010, 79, 188–190. [Google Scholar] [CrossRef]
- Danner, U.N.; Sternheim, L.; Evers, C. The importance of distinguishing between the different eating disorders (sub)types when assessing emotion regulation strategies. Psychiatry Res. 2014, 215, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Svaldi, J.; Griepenstroh, J.; Tuschen-Caffier, B.; Ehring, T. Emotion regulation deficits in eating disorders: A marker of eating pathology or general psychopathology? Psychiatry Res. 2012, 197, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, A.; Ryan, D.; Konstantakopoulos, G.; Stroumpa, S.; Kaçar, A.S.; Renshaw, S.; Landau, S.; Kravariti, E. Lifetime prevalence of non-suicidal self-injury in patients with eating disorders: A systematic review and meta-analysis. Psychol. Med. 2016, 46, 1345–1358. [Google Scholar] [CrossRef] [PubMed]
- Dingemans, A.; Danner, U.N.; Parks, M. Emotion regulation in binge eating disorder: A review. Nutrients 2017, 9, 1274. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.; Steward, T.; Agüera, Z.; Mestre-Bach, G.; Magaña, P.; Granero, R.; Jiménez-Murcia, S.; Claes, L.; Gearhardt, A.N.; Menchón, J.M.; et al. Associations of food addiction and nonsuicidal self-injury among women with an eating disorder: A common strategy for regulating emotions? Eur. Eat. Disord. Rev. 2018, 26, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Brockmeyer, T.; Holtforth, M.G.; Bents, H.; Kämmerer, A.; Herzog, W.; Friederich, H.C. Starvation and emotion regulation in anorexia nervosa. Compr. Psychiatry 2012, 53, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Hatch, A.; Madden, S.; Kohn, M.; Clarke, S.; Touyz, S.; Williams, L.M. Anorexia nervosa: Towards an integrative neuroscience model. Eur. Eat. Disord. Rev. 2010, 18, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Oldershaw, A.; Lavender, T.; Sallis, H.; Stahl, D.; Schmidt, U. Emotion generation and regulation in anorexia nervosa: A systematic review and meta-analysis of self-report data. Clin. Psychol. Rev. 2015, 39, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.; Sullivan, S.; Tchanturia, K.; Treasure, J. Emotional functioning in eating disorders: Attentional bias, emotion recognition and emotion regulation. Psychol. Med. 2010, 40, 1887–1889. [Google Scholar] [CrossRef]
- Brown, T.A.; Avery, J.C.; Jones, M.D.; Anderson, L.K.; Wierenga, C.E.; Kaye, W.H. The impact of alexithymia on emotion dysregulation in anorexia nervosa and bulimia nervosa over time. Eur. Eat. Disord. Rev. 2018, 26, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Polivy, J.; Herman, C.P. Etiology of binge eating: Psychological mechanisms. In Binge Eating: Nature, Assessment and Treatment; Fairburn, C.G., Wilso, G.T., Eds.; Guilford Press: New York, NY, USA, 1993; pp. 173–205. [Google Scholar]
- Haedt-Matt, A.A.; Keel, P.K. Revisiting the affect regulation model of binge eating: A meta-analysis of studies using ecological momentary assessment. Psychol. Bull. 2011, 137, 660–681. [Google Scholar] [CrossRef] [PubMed]
- Mallorquí-Bagué, N.; Vintró-Alcaraz, C.; Sánchez, I.; Riesco, N.; Agüera, Z.; Granero, R.; Jiménez-Múrcia, S.; Menchón, J.M.; Treasure, J.; Fernández-Aranda, F. Emotion regulation as a transdiagnostic feature among eating disorders: Cross-sectional and longitudinal approach. Eur. Eat. Disord. Rev. 2018, 26, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Safer, D.L.; Telch, C.F.; Chen, E.Y. Dialectical Behavior Therapy for Binge Eating and Bulimia; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Sipos, V.; Schweiger, U.; Jauch-Chara, K.; Faßbinder, E. Treatment of eating disorders by emotion regulation. Psychother. Psychosom. Med. Psychol. 2017, 67, 431–435. [Google Scholar] [PubMed]
- Hayaki, J.; Free, S. Positive and negative eating expectancies in disordered eating among women and men. Eat. Behav. 2016, 22, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Ambwani, S.; Slane, J.D.; Thomas, K.M.; Hopwood, C.J.; Grilo, C.M. Interpersonal dysfunction and affect-regulation difficulties in disordered eating among men and women. Eat. Behav. 2014, 15, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.M.; Reilly, E.E.; Thomas, J.J.; Eddy, K.T.; Franko, D.L.; Hormes, J.M.; Anderson, D.A. Associations among fear, disgust, and eating pathology in undergraduate men and women. Appetite 2018, 125, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Opwis, M.; Schmidt, J.; Martin, A.; Salewski, C. Gender differences in eating behavior and eating pathology: The mediating role of rumination. Appetite 2017, 110, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Lavender, J.M.; Anderson, D.A. Contribution of emotion regulation difficulties to disordered eating and body dissatisfaction in college men. Int. J. Eat. Disord. 2010, 43, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Pisetsky, E.M.; Haynos, A.F.; Lavender, J.M.; Crow, S.J.; Peterson, C.B. Associations between emotion regulation difficulties, eating disorder symptoms, non-suicidal self-injury, and suicide attempts in a heterogeneous eating disorder sample. Compr. Psychiatry 2017, 73, 143–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivanova, I.V.; Tasca, G.A.; Proulx, G.; Bissasda, H. Contribution of interpersonal problems to eating disorder psychopathology via negative affect in treatment-seeking men and women: Testing the validity of the interpersonal model in an understudied population. Clin. Psychol. Psychother. 2017, 24, 952–964. [Google Scholar] [CrossRef] [PubMed]
- Masheb, R.M.; Grilo, C.M. Emotional overeating and its associations with eating disorder psychopathology among overweight patients with Binge eating disorder. Int. J. Eat. Disord. 2006, 39, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Goddard, E.; Carral-Fernández, L.; Denneny, E.; Campbell, I.C.; Treasure, J. Cognitive flexibility, central coherence and social emotional processing in males with an eating disorder. World J. Biol. Psychiatry 2014, 15, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.C.; McCabe, G.A.; Southard, A.C.; Zeigler-Hill, V. Pathological personality traits and emotion regulation difficulties. Personal. Individ. Differ. 2016, 95, 168–177. [Google Scholar] [CrossRef]
- Borges, L.M.; Naugle, A.E. The role of emotion regulation in predicting personality dimensions. Personal. Ment. Health 2017, 11, 314–334. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Agüera, Z.; Krug, I.; Sanchez, I.; Granero, R.; Penelo, E.; Penas-Lledo, E.; Jimenez-Murcia, S.; Menchon, J.M.; Fernández-Aranda, F. Personality changes in bulimia nervosa after a cognitive behaviour therapy. Eur. Eat. Disord. Rev. 2012, 20, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Atiye, M.; Miettunen, J.; Raevuori-Helkamaa, A. A meta-analysis of temperament in eating disorders. Eur. Eat. Disord. Rev. 2015, 23, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Navarro, A.; Agüera, Z.; Krug, I.; Jiménez-Murcia, S.; Sánchez, I.; Araguz, N.; Gorwood, P.; Granero, R.; Penelo, E.; Karwautz, A.; et al. Do men with eating disorders differ from women in clinics, psychopathology and personality? Eur. Eat. Disord. Rev. 2012, 20, 23–31. [Google Scholar] [CrossRef]
- Claes, L.; Jiménez-Murcia, S.; Agüera, Z.; Castro, R.; Sánchez, I.; Menchón, J.M.; Fernández-Aranda, F. Male eating disorder patients with and without non-suicidal self-injury: A comparison of psychopathological and personality features. Eur. Eat. Disord. Rev. 2012, 20, 335–338. [Google Scholar] [CrossRef]
- Hintsanen, M.; Jokela, M.; Cloninger, C.R.; Pulkki-Råback, L.; Hintsa, T.; Elovainio, M.; Josefsson, K.; Rosenström, T.; Mullola, S.; Raitakari, O.T.; et al. Temperament and character predict body-mass index: A population-based prospective cohort study. J. Psychosom. Res. 2012, 73, 391–397. [Google Scholar] [CrossRef]
- Rodríguez-Cano, T.; Beato-Fernandez, L.; Rojo-Moreno, L.; Vaz-Leal, F.J. The role of temperament and character in the outcome of depressive mood in eating disorders. Compr. Psychiatry 2014, 55, 1130–1136. [Google Scholar] [CrossRef]
- Wolz, I.; Agüera, Z.; Granero, R.; Jiménez-Murcia, S.; Gratz, K.L.; Menchón, J.M.; Fernández-Aranda, F. Emotion regulation in disordered eating: Psychometric properties of the Difficulties in Emotion Regulation Scale among Spanish adults and its interrelations with personality and clinical severity. Front. Psychol. 2015, 6, 907. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M. Eating Disorder Inventory-2; Psychological Assessment Resources: Odessa, Ukraine, 1991. [Google Scholar]
- Garner, D.M. Inventario de Trastornos de la Conducta Alimentaria (EDI-2)—Manual; TEA: Madrid, Spain, 1998. [Google Scholar]
- Derogatis, L.R. SCL-90-R: Symptom Checklist-90-R. Administration, Scoring and Procedures Manuall—II for the Revised Version; Clinical Psychometric Research: Towson, MD, USA, 1994. [Google Scholar]
- Derogatis, L.R. SCL-90-R. Cuestionario de 90 Síntomas-Manual; TEA: Madrid, Spain, 2002. [Google Scholar]
- Cloninger, C.R. The Temperament and Character Inventory—Revised; Center for Psychobiology of Personality, Washington University: St Louis, MO, USA, 1999. [Google Scholar]
- Gutiérrez-Zotes, J.A.; Bayón, C.; Montserrat, C.; Valero, J.; Labad, A.; Cloninger, C.R. Temperament and Character Inventory-Revised (TCI-R). Standardization and normative data in a general population sample. Actas Espa. Psiquiatr. 2004, 32, 8–15. [Google Scholar]
- Gratz, K.L.; Roemer, L. multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Kelley, K.; Preacher, K.J. On effect size. Psychol. Methods 2012, 17, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Finner, H. On a monotonicity problem in step-down multiple test procedures. J. Am. Stat. Assoc. 1993, 88, 920–923. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Gilford Press: New York, NY, USA, 2005. [Google Scholar]
- Barrett, P. Structural equation modelling: Adjudging model fit. Personal. Individ. Differ. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- Lavender, J.M.; Wonderlich, S.A.; Engel, S.G.; Gordon, K.H.; Kaye, W.H.; Mitchell, J.E. Dimensions of emotion dysregulation in anorexia nervosa and bulimia nervosa: A conceptual review of the empirical literature. Clin. Psychol. Rev. 2015, 40, 111–122. [Google Scholar] [CrossRef] [Green Version]
- Donahue, J.M.; Reilly, E.E.; Anderson, L.M.; Scharmer, C.; Anderson, D.A. Evaluating associations between perfectionism, emotion regulation, and eating disorder symptoms in a mixed-gender sample. J. Nerv. Ment. Dis. 2018, 206, 900–904. [Google Scholar] [CrossRef]
- Kinnaird, E.; Norton, C.; Tchanturia, K. Clinicians’ views on treatment adaptations for men with eating disorders: A qualitative study. BMJ Open 2018, 8, e021934. [Google Scholar] [CrossRef]
- Aloi, M.; Rania, M.; Caroleo, M.; De Fazio, P.; Segura-García, C. Social cognition and emotional functioning in patients with binge eating disorder. Eur. Eat. Disord. Rev. 2017, 25, 172–178. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Svrakic, D.M.; Przybeck, T.R. A psychobiological model of temperament and character. Arch. Gen. Psychiatry 1993, 50, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, S.T.; Schoen, E.G. Males and eating disorders: Gender-based therapy for eating disorder recovery. Prof. Psychol. Res. Pract. 2008, 39, 464–471. [Google Scholar] [CrossRef]
- Agüera, Z.; Sánchez, I.; Granero, R.; Riesco, N.; Steward, T.; Martín-Romera, V.; Jiménez-Murcia, S.; Romero, X.; Caroleo, M.; Segura-García, C.; et al. Short-Term Treatment Outcomes and Dropout Risk in Men and Women with Eating Disorders. Eur. Eat. Disord. Rev. 2017, 25, 293–301. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| ED Females | ED Males | HC Females | HC Males | ||||||
|---|---|---|---|---|---|---|---|---|---|
| (n = 656) | (n = 62) | (n = 286) | (n = 78) | ||||||
| n | % | n | % | n | % | n | % | p-Value | |
| Civil status | |||||||||
| Single | 486 | 74.1% | 42 | 67.7% | 278 | 97.2% | 77 | 98.7% | <0.001 * |
| Married-partner | 114 | 17.4% | 17 | 27.4% | 3 | 1.0% | 0 | 0.0% | |
| Separated-divorced | 56 | 8.5% | 3 | 4.8% | 5 | 1.7% | 1 | 1.3% | |
| Education | |||||||||
| Primary | 261 | 39.8% | 28 | 45.2% | 6 | 2.1% | 2 | 2.6% | <0.001 * |
| Secondary | 271 | 41.3% | 22 | 35.5% | 276 | 96.5% | 75 | 96.2% | |
| University | 124 | 18.9% | 12 | 19.4% | 4 | 1.4% | 1 | 1.3% | |
| Employed | |||||||||
| Student | 259 | 39.5% | 22 | 35.5% | 120 | 42.0% | 42 | 53.8% | 0.077 |
| Unemployed | 397 | 60.5% | 40 | 64.5% | 166 | 58.0% | 36 | 46.2% | |
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | p-Value | |
| Age (years-old) | 29.78 | 11.07 | 33.56 | 12.73 | 21.06 | 4.19 | 21.30 | 4.53 | <0.001 * |
| ED Women | ED Men | HC Women | HC Men | ED Women vs. ED Men | HC Women vs. HC Men | ED Women vs. HC Women | ED Men vs. HC Men | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 656) | (n = 62) | (n = 286) | (n = 78) | |||||||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| | |
| DERS scales | ||||||||||||||||
| Non-acceptance | 19.63 | 6.87 | 17.33 | 6.68 | 12.35 | 5.29 | 10.99 | 4.59 | 0.007 * | 0.34 | 0.089 | 0.27 | <0.001 * | 1.19 † | <0.001 * | 1.11 † |
| Pursuing goals | 17.64 | 5.03 | 16.07 | 4.89 | 12.98 | 4.12 | 12.47 | 4.31 | 0.013 * | 0.32 | 0.402 | 0.12 | <0.001 * | 1.01 † | <0.001 * | 0.78 † |
| Impulse behaviors | 17.00 | 6.47 | 14.69 | 6.23 | 10.71 | 4.01 | 9.89 | 3.16 | 0.003 * | 0.36 | 0.267 | 0.23 | <0.001 * | 1.17 † | <0.001 * | 0.97 † |
| Emotional awareness | 17.91 | 5.10 | 18.25 | 4.51 | 14.56 | 4.12 | 14.29 | 4.31 | 0.594 | 0.07 | 0.659 | 0.06 | <0.001 * | 0.72 † | <0.001 * | 0.90 † |
| Emotional regulation | 25.54 | 8.24 | 22.39 | 8.05 | 15.13 | 5.87 | 14.26 | 5.47 | 0.002 * | 0.39 | 0.370 | 0.15 | <0.001 * | 1.45 † | <0.001 * | 1.18 † |
| Emotional clarity | 14.76 | 5.07 | 13.51 | 5.08 | 10.22 | 3.63 | 9.42 | 3.67 | 0.043 * | 0.25 | 0.182 | 0.22 | <0.001 * | 1.03 † | <0.001 * | 0.92 † |
| Total score | 112.46 | 26.94 | 102.25 | 26.02 | 75.95 | 19.27 | 71.31 | 16.95 | 0.002 * | 0.39 | 0.143 | 0.26 | <0.001 * | 1.56 † | <0.001 * | 1.41 † |
| EDI-2 scales | ||||||||||||||||
| Drive for thinness | 14.23 | 6.02 | 10.51 | 5.60 | 3.74 | 5.04 | 2.75 | 3.45 | <0.001 * | 0.64 † | 0.206 | 0.23 | <0.001 * | 1.89 † | <0.001 * | 1.67 † |
| Body dissatisfaction | 17.22 | 7.88 | 11.10 | 8.32 | 6.37 | 6.75 | 4.63 | 4.87 | <0.001 * | 0.75 † | 0.094 | 0.30 | <0.001 * | 1.48 † | <0.001 * | 0.95 † |
| Interoceptive awareness | 11.83 | 7.06 | 8.32 | 6.43 | 2.83 | 2.89 | 1.94 | 1.99 | <0.001 * | 0.52 † | 0.249 | 0.36 | <0.001 * | 1.67 † | <0.001 * | 1.34 † |
| Bulimia | 7.21 | 5.59 | 3.74 | 4.15 | 1.49 | 1.68 | 1.01 | 0.93 | <0.001 * | 0.70 † | 0.454 | 0.35 | <0.001 * | 1.39 † | 0.001 * | 0.91 † |
| Interpersonal distrust | 5.76 | 4.81 | 5.67 | 4.52 | 2.54 | 2.92 | 2.57 | 2.76 | 0.880 | 0.02 | 0.969 | 0.01 | <0.001* | 0.81 † | <0.001 * | 0.83 † |
| Ineffectiveness | 11.90 | 7.70 | 8.21 | 7.22 | 2.26 | 3.05 | 2.02 | 2.65 | <0.001 * | 0.51 † | 0.788 | 0.09 | <0.001 * | 1.65 † | <0.001 * | 1.14 † |
| Maturity fears | 8.79 | 5.97 | 7.33 | 5.03 | 4.46 | 3.72 | 4.20 | 3.38 | 0.036 * | 0.27 | 0.725 | 0.07 | <0.001 * | 0.87 † | 0.001 * | 0.73 † |
| Perfectionism | 6.18 | 4.36 | 5.05 | 4.00 | 3.99 | 3.55 | 4.08 | 3.34 | 0.037 * | 0.27 | 0.874 | 0.03 | <0.001 * | 0.55 † | 0.186 | 0.27 |
| Impulse regulation | 6.84 | 6.03 | 5.55 | 5.21 | 1.28 | 2.27 | 1.47 | 3.06 | 0.047 * | 0.23 | 0.783 | 0.07 | <0.001 * | 1.22 † | <0.001 * | 0.95 † |
| Ascetism | 7.36 | 4.09 | 5.81 | 4.25 | 2.35 | 2.22 | 2.57 | 2.10 | 0.001 * | 0.37 | 0.653 | 0.10 | <0.001 * | 1.52 † | <0.001 * | 0.96 † |
| Social insecurity | 8.11 | 5.37 | 6.56 | 4.74 | 2.63 | 2.85 | 2.40 | 2.82 | 0.013 * | 0.31 | 0.725 | 0.08 | <0.001 * | 1.28 † | <0.001 * | 1.07 † |
| Total score | 105.43 | 42.63 | 77.88 | 42.60 | 33.89 | 21.52 | 29.50 | 15.65 | <0.001 * | 0.65 † | 0.355 | 0.23 | <0.001 * | 2.12 † | <0.001 * | 1.51 † |
| Binge eating/purging | ||||||||||||||||
| Binge episodes | 3.76 | 6.32 | 1.86 | 2.60 | --- | --- | --- | --- | 0.019 * | 0.39 | --- | --- | --- | --- | --- | --- |
| Purging episodes | 3.96 | 8.75 | 1.29 | 3.60 | --- | --- | --- | --- | 0.018 * | 0.40 | --- | --- | --- | --- | --- | --- |
| n | % | n | % | n | % | n | % | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| | |
| 1 NSSI | 290 | 44.2% | 10 | 16.1% | 62 | 21.8% | 19 | 25.0% | <0.001 * | 0.64 † | 0.544 | 0.08 | <0.001 * | 0.50 † | 0.260 | 0.22 |
| Subsample | AN | BN | BED | OSFED | AN-BN | AN-BED | AN-OSFED | BN-BED | BN-OSFED | BED-OSFED | ||||||||||
| n = 140 | n = 236 | n = 100 | n = 180 | |||||||||||||||||
| Women | Mean | SD | Mean | SD | Mean | SD | Mean | SD | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| |
| Nonacceptance | 17.62 | 7.26 | 20.99 | 6.42 | 19.36 | 6.68 | 19.70 | 6.89 | <0.001 * | 0.52 † | 0.046 * | 0.25 | 0.007 * | 0.29 | 0.042 * | 0.25 | 0.046 * | 0.19 | 0.700 | 0.05 |
| Pursuing goals | 16.47 | 5.16 | 18.55 | 4.76 | 17.51 | 5.11 | 17.18 | 5.05 | <0.001 * | 0.42 | 0.128 | 0.20 | 0.209 | 0.14 | 0.092 | 0.21 | 0.006 * | 0.28 | 0.606 | 0.07 |
| Impulse behavior | 15.44 | 6.97 | 18.56 | 6.03 | 16.51 | 6.47 | 16.39 | 6.26 | <0.001 * | 0.51 † | 0.225 | 0.16 | 0.186 | 0.14 | 0.010 * | 0.33 | 0.001 * | 0.35 | 0.893 | 0.02 |
| Emot-awareness | 17.44 | 5.27 | 18.01 | 4.87 | 18.58 | 5.15 | 17.62 | 5.24 | 0.295 | 0.11 | 0.042 * | 0.22 | 0.749 | 0.03 | 0.367 | 0.11 | 0.443 | 0.08 | 0.155 | 0.18 |
| Emot-regulation | 23.16 | 8.79 | 27.29 | 7.97 | 25.31 | 7.75 | 24.95 | 7.97 | <0.001 * | 0.50 † | 0.041 * | 0.26 | 0.049 * | 0.21 | 0.049 * | 0.25 | 0.004 * | 0.29 | 0.739 | 0.05 |
| Emot-clarity | 13.77 | 5.50 | 15.22 | 5.00 | 14.49 | 4.53 | 14.77 | 5.02 | 0.008 * | 0.28 | 0.303 | 0.14 | 0.042 * | 0.19 | 0.241 | 0.15 | 0.371 | 0.09 | 0.673 | 0.06 |
| Total score | 103.9 | 29.7 | 118.6 | 24.8 | 111.7 | 25.5 | 110.6 | 26.3 | <0.001 * | 0.54 † | 0.032 * | 0.28 | 0.025 * | 0.24 | 0.035 * | 0.27 | 0.003 * | 0.31 | 0.752 | 0.04 |
| Subsample | AN | BN | BED | OSFED | AN-BN | AN-BED | AN-OSFED | BN-BED | BN-OSFED | BED-OSFED | ||||||||||
| n = 16 | n = 12 | n = 15 | n = 19 | |||||||||||||||||
| Men | Mean | SD | Mean | SD | Mean | SD | Mean | SD | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| | p-Value | |d| |
| Nonacceptance | 16.14 | 7.86 | 17.95 | 5.65 | 17.90 | 7.78 | 17.79 | 5.46 | 0.507 | 0.26 | 0.499 | 0.22 | 0.494 | 0.24 | 0.985 | 0.01 | 0.950 | 0.03 | 0.965 | 0.02 |
| Pursuing goals | 13.69 | 4.68 | 15.83 | 5.17 | 16.66 | 4.52 | 17.32 | 4.75 | 0.266 | 0.53 † | 0.048 * | 0.65 † | 0.035 * | 0.77 † | 0.661 | 0.17 | 0.415 | 0.30 | 0.711 | 0.14 |
| Impulse behavior | 11.66 | 4.22 | 16.11 | 6.33 | 14.07 | 6.24 | 16.85 | 6.64 | 0.043 * | 0.83 † | 0.286 | 0.51 † | 0.015 * | 0.93 † | 0.386 | 0.32 | 0.740 | 0.12 | 0.203 | 0.51 † |
| Emot-awareness | 17.96 | 4.75 | 18.21 | 3.55 | 19.28 | 4.73 | 17.21 | 4.81 | 0.893 | 0.06 | 0.455 | 0.28 | 0.644 | 0.16 | 0.561 | 0.26 | 0.570 | 0.24 | 0.227 | 0.52 † |
| Emot-regulation | 20.43 | 9.44 | 21.45 | 7.05 | 21.68 | 6.53 | 24.66 | 8.14 | 0.737 | 0.12 | 0.668 | 0.15 | 0.049 * | 0.53 † | 0.942 | 0.03 | 0.275 | 0.52 † | 0.293 | 0.50 † |
| Emot-clarity | 14.31 | 6.38 | 12.20 | 5.19 | 13.75 | 4.63 | 12.71 | 4.27 | 0.315 | 0.36 | 0.777 | 0.10 | 0.387 | 0.29 | 0.458 | 0.31 | 0.798 | 0.11 | 0.591 | 0.23 |
| Total score | 94.2 | 29.3 | 101.7 | 25.1 | 103.3 | 24.1 | 106.5 | 25.0 | 0.466 | 0.28 | 0.356 | 0.34 | 0.180 | 0.55 † | 0.878 | 0.06 | 0.628 | 0.19 | 0.737 | 0.13 |
| ED Women (n = 656) | ED Men (n = 62) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coefficients (Model Obtained in the Fifth Block-Step) | Change | Coefficients (Model Obtained in the Fifth Block-Step) | Change | |||||||||||||
| B | SE | Beta | p-Value | 95% CI (B) | ΔR2 | p-Value | B | SE | Beta | p-Value | 95% CI (B) | ΔR2 | B | |||
| Covariates | 0.009 | 0.131 | 0.055 | 0.395 | ||||||||||||
| Age (years-old) | −0.13 | 0.19 | −0.054 | 0.497 | −0.51 | 0.25 | 0.11 | 0.43 | 0.053 | 0.809 | −0.77 | 0.98 | ||||
| Civil status (married) | 3.33 | 1.95 | 0.055 | 0.089 | −0.50 | 7.15 | −0.51 | 5.42 | −0.009 | 0.926 | −11.45 | 10.44 | ||||
| Education level | 1.51 | 0.94 | 0.041 | 0.107 | −0.33 | 3.36 | 2.65 | 2.43 | 0.077 | 0.283 | −2.27 | 7.56 | ||||
| ED variables | 0.533 | <0.001 * | 0.488 | <0.001 * | ||||||||||||
| EDI-2 total | 0.19 | 0.03 | 0.294 | <0.001 * | 0.13 | 0.24 | 0.09 | 0.07 | 0.158 | 0.183 | −0.05 | 0.24 | ||||
| Onset of ED | −0.02 | 0.21 | −0.005 | 0.934 | −0.42 | 0.39 | −0.17 | 0.35 | −0.076 | 0.635 | −0.88 | 0.54 | ||||
| Duration of ED | 0.05 | 0.20 | 0.017 | 0.798 | −0.34 | 0.44 | −0.37 | 0.28 | −0.155 | 0.196 | −0.94 | 0.20 | ||||
| Psychopathology | 0.073 | <0.001 * | 0.219 | <0.001 * | ||||||||||||
| SCL-90R GSI | 14.61 | 1.55 | 0.397 | <0.001 * | 11.57 | 17.65 | 19.39 | 3.72 | 0.609 | <0.001 * | 11.88 | 26.91 | ||||
| Fourth block/step | 0.001 | 0.946 | 0.006 | 0.268 | ||||||||||||
| NSSI (0 = no; 1 = yes) | 0.20 | 0.84 | 0.006 | 0.809 | −1.45 | 1.86 | −0.28 | 2.97 | −0.007 | 0.924 | −6.29 | 5.72 | ||||
| TCI-R | 0.025 | <0.001 * | 0.076 | 0.018 * | ||||||||||||
| Novelty seeking | 0.08 | 0.05 | 0.048 | 0.044 * | 0.01 | 0.17 | 0.06 | 0.15 | 0.042 | 0.688 | −0.24 | 0.35 | ||||
| Harm avoidance | 0.00 | 0.05 | −0.004 | 0.926 | −0.10 | 0.09 | 0.00 | 0.17 | 0.000 | 0.997 | −0.34 | 0.34 | ||||
| Reward dependence | −0.09 | 0.05 | −0.054 | 0.047 * | −0.18 | −0.01 | −0.11 | 0.15 | −0.060 | 0.470 | −0.40 | 0.19 | ||||
| Persistence | −0.05 | 0.04 | −0.039 | 0.174 | −0.12 | 0.02 | −0.41 | 0.14 | −0.256 | 0.005 * | −0.69 | −0.13 | ||||
| Self-directedness | −0.25 | 0.05 | −0.197 | <0.001 * | −0.34 | −0.15 | −0.21 | 0.16 | −0.189 | 0.195 | −0.54 | 0.11 | ||||
| Cooperativeness | 0.12 | 0.05 | 0.070 | 0.023 * | 0.02 | 0.22 | 0.13 | 0.17 | 0.075 | 0.456 | −0.21 | 0.47 | ||||
| Self-transcendence | −0.04 | 0.05 | −0.026 | 0.335 | −0.14 | 0.05 | 0.02 | 0.13 | 0.012 | 0.891 | −0.25 | 0.28 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agüera, Z.; Paslakis, G.; Munguía, L.; Sánchez, I.; Granero, R.; Sánchez-González, J.; Steward, T.; Jiménez-Murcia, S.; Fernández-Aranda, F. Gender-Related Patterns of Emotion Regulation among Patients with Eating Disorders. J. Clin. Med. 2019, 8, 161. https://doi.org/10.3390/jcm8020161
Agüera Z, Paslakis G, Munguía L, Sánchez I, Granero R, Sánchez-González J, Steward T, Jiménez-Murcia S, Fernández-Aranda F. Gender-Related Patterns of Emotion Regulation among Patients with Eating Disorders. Journal of Clinical Medicine. 2019; 8(2):161. https://doi.org/10.3390/jcm8020161
Chicago/Turabian StyleAgüera, Zaida, Georgios Paslakis, Lucero Munguía, Isabel Sánchez, Roser Granero, Jessica Sánchez-González, Trevor Steward, Susana Jiménez-Murcia, and Fernando Fernández-Aranda. 2019. "Gender-Related Patterns of Emotion Regulation among Patients with Eating Disorders" Journal of Clinical Medicine 8, no. 2: 161. https://doi.org/10.3390/jcm8020161