Gestational Exercise and Maternal and Child Health: Effects until Delivery and at Post-Natal Follow-up

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Experimental Section
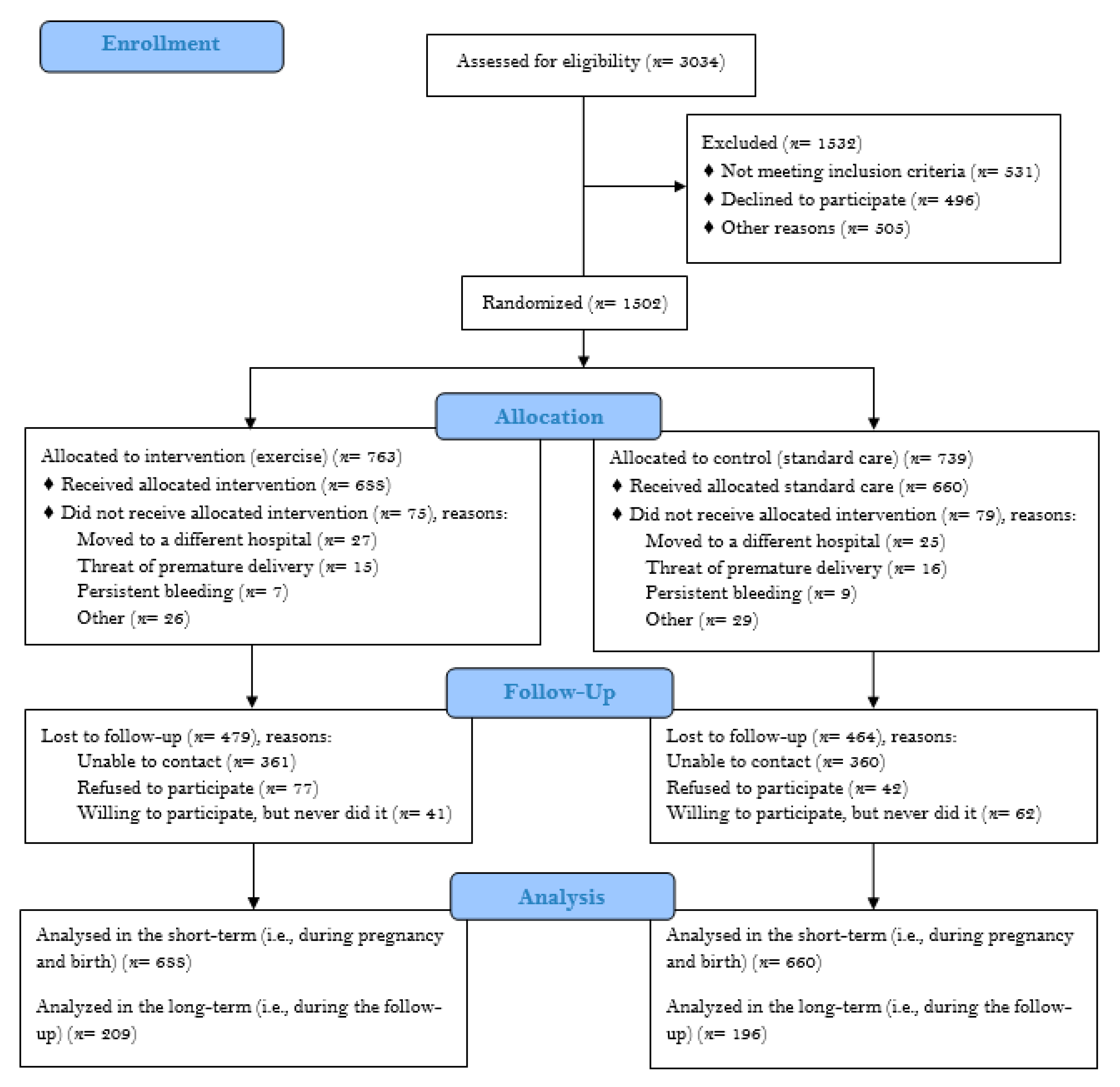
2.1. Experimental Design
2.2. Intervention
2.3. Safety
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Adherence and Safety
3.2. Maternal and Newborn Outcomes up to Delivery
3.3. Maternal and Childhood Outcomes at Post-Natal Follow-up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain with Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Mamun, A.A.; Kinarivala, M.; O’Callaghan, M.J.; Williams, G.M.; Najman, J.M.; Callaway, L.K. Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: Evidence from 21 y postpartum follow-up. Am. J. Clin. Nutr. 2010, 91, 1336–1341. [Google Scholar] [CrossRef] [Green Version]
- Voerman, E.; Santos, S.; Patro Golab, B.; Amiano, P.; Ballester, F.; Barros, H.; Bergström, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: An individual participant data meta-analysis. PLoS Med. 2019, 16, e1002744. [Google Scholar] [CrossRef] [PubMed]
- Bouvier, D.; Forest, J.C.; Dion-Buteau, E.; Bernard, N.; Bujold, E.; Pereira, B.; Giguère, Y. Association of Maternal Weight and Gestational Weight Gain with Maternal and Neonate Outcomes: A Prospective Cohort Study. J. Clin. Med. 2019, 8, 2074. [Google Scholar] [CrossRef] [Green Version]
- Hrolfsdottir, L.; Rytter, D.; Olsen, S.F.; Bech, B.H.; Maslova, E.; Henriksen, T.B.; Halldorsson, T.I. Gestational weight gain in normal weight women and offspring cardio-metabolic risk factors at 20 years of age. Int. J. Obes. 2015, 39, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Neiger, R. Long-Term Effects of Pregnancy Complications on Maternal Health: A Review. J. Clin. Med. 2017, 6, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priest, J.R.; Yang, W.; Reaven, G.; Knowles, J.W.; Shaw, G.M. Maternal Midpregnancy Glucose Levels and Risk of Congenital Heart Disease in Offspring. JAMA Pediatr. 2015, 169, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, E.P.; Jaffe, M.G. Pregnancy and Subsequent Glucose Intolerance in Women of Childbearing Age: Heeding the Early Warning Signs for Primary Prevention of Cardiovascular Disease in Women. JAMA Int. Med. 2017, 177, 1742–1744. [Google Scholar] [CrossRef]
- Tobias, D.K.; Stuart, J.J.; Li, S.; Chavarro, J.; Rimm, E.; Rich-Edwards, J.W.; Hu, F.B.; Manson, J.E.; Zhang, C. Association of History of Gestational Diabetes with Long-term Cardiovascular Disease Risk in a Large Prospective Cohort of US Women. JAMA Int. Med. 2017, 177, 1735–1742. [Google Scholar] [CrossRef]
- Behrens, I.; Basit, S.; Lykke, J.A.; Ranthe, M.F.; Wohlfahrt, J.; Bundgaard, H.; Melbye, M.; Boyd, H.A. Association between Hypertensive Disorders of Pregnancy and Later Risk of Cardiomyopathy. JAMA 2016, 315, 1026–1033. [Google Scholar] [CrossRef] [Green Version]
- Palinski, W. Effect of maternal cardiovascular conditions and risk factors on offspring cardiovascular disease. Circulation 2014, 129, 2066–2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muktabhant, B.; Lawrie, T.A.; Lumbiganon, P.; Laopaiboon, M. Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst. Rev. 2015, 1, CD007145. [Google Scholar] [CrossRef] [PubMed]
- Ruchat, S.M.; Mottola, M.F.; Skow, R.J.; Nagpal, T.S.; Meah, V.L.; James, M.; Riske, L.; Sobierajski, F.; Kathol, A.J.; Marchand, A.A.; et al. Effectiveness of exercise interventions in the prevention of excessive gestational weight gain and postpartum weight retention: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Perales, M.; Artal, R.; Lucia, A. Exercise during Pregnancy. JAMA 2017, 317, 1113–1114. [Google Scholar] [CrossRef] [PubMed]
- ACOG. Committee Opinion No. 650: Physical Activity and Exercise during Pregnancy and the Postpartum Period. Obstet. Gynecol. 2015, 126, e135–e142. [Google Scholar] [CrossRef] [PubMed]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, J.E.; Reynolds, R.M. Prescribing Exercise and Lifestyle Training for High Risk Women in Pregnancy and Early Post-partum-Is It Worth It? PLoS Med. 2016, 13, e1002093. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, J.R.; Perales, M.; Pelaez, M.; Lopez, C.; Lucia, A.; Barakat, R. Supervised exercise-based intervention to prevent excessive gestational weight gain: A randomized controlled trial. Mayo Clin. Proc. 2013, 88, 1388–1397. [Google Scholar] [CrossRef]
- Artal, R. Exercise and diabetes mellitus in pregnancy. A brief review. Sports Med. 1990, 9, 261–265. [Google Scholar] [CrossRef]
- Di Mascio, D.; Magro-Malosso, E.R.; Saccone, G.; Marhefka, G.D.; Berghella, V. Exercise during pregnancy in normal-weight women and risk of preterm birth: A systematic review and meta-analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 2016, 215, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009. [Google Scholar]
- Perales, M.; Santos-Lozano, A.; Sanchis-Gomar, F.; Luaces, M.; Pareja-Galeano, H.; Garatachea, N.; Barakat, R.; Lucia, A. Maternal Cardiac Adaptations to a Physical Exercise Program during Pregnancy. Med. Sci. Sports Exerc. 2016, 48, 896–906. [Google Scholar] [CrossRef] [PubMed]
- Rooney, B.L.; Schauberger, C.W. Excess pregnancy weight gain and long-term obesity: One decade later. Obstet. Gynecol. 2002, 100, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar]
- World Health Organization. The WHO Child Growth Standards. Available online: http://www.who.int/childgrowth/standards/Technical_report.pdf (accessed on 17 November 2018).
- Centers for Diseases Control and Prevention. 2000 CDC Growth Charts (ages 2 to <20 Years). Available online: https://www.cdc.gov/healthyweight/bmi/calculator.html (accessed on 12 October 2018).
- Forczek, W.; Curylo, M.; Forczek, B. Physical Activity Assessment during Gestation and Its Outcomes: A Review. Obstet. Gynecol. Surv. 2017, 72, 425–444. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Skow, R.; Louise Meah, V.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef]
- Garnaes, K.K.; Morkved, S.; Salvesen, O.; Moholdt, T. Exercise Training and Weight Gain in Obese Pregnant Women: A Randomized Controlled Trial (ETIP Trial). PLoS Med. 2016, 13, e1002079. [Google Scholar] [CrossRef] [Green Version]
- Luoto, R.; Kinnunen, T.I.; Aittasalo, M.; Kolu, P.; Raitanen, J.; Ojala, K.; Mansikkamäki, K.; Lamberg, S.; Vasankari, T.; Komulainen, T.; et al. Primary prevention of gestational diabetes mellitus and large-for-gestational-age newborns by lifestyle counseling: A cluster-randomized controlled trial. PLoS Med. 2011, 8, e1001036. [Google Scholar] [CrossRef]
- Hopkins, S.A.; Cutfield, W.S. Exercise in pregnancy: Weighing up the long-term impact on the next generation. Exerc. Sport Sci. Rev. 2011, 39, 120–127. [Google Scholar] [CrossRef]
- Hoffmann, J.; Gunther, J.; Geyer, K.; Stecher, L.; Kunath, J.; Meyer, D.; Spies, M.; Rosenfeld, E.; Kick, L.; Rauh, K.; et al. Associations between Prenatal Physical Activity and Neonatal and Obstetric Outcomes-A Secondary Analysis of the Cluster-Randomized GeliS Trial. J. Clin. Med. 2019, 8, 1735. [Google Scholar] [CrossRef] [Green Version]
- Brunner Huber, L.R. Validity of self-reported height and weight in women of reproductive age. Matern. Child Health J. 2007, 11, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S.; Rouse, H.L.; Currie, J. Pregnancy weight gain and childhood body weight: A within-family comparison. PLoS Med. 2013, 10, e1001521. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Control (n = 660) | Exercise (n = 688) | p-Value | |
|---|---|---|---|
| Age (years) | 31 ± 4 | 32 ± 4 | 0.168 |
| SBP (mmHg) | 110 ± 12 | 108 ± 9 | 0.077 |
| DBP (mmHg) | 64 ± 8 | 63 ± 7 | 0.584 |
| Pre-gestational weight (kg) | 63 ± 12 | 64 ± 11 | 0.103 |
| Pre-gestational BMI (kg·m−2) | 23.6 ± 4.0 | 23.5 ± 3.9 | 0.534 |
| Pre-gestational BMI category | 0.349 | ||
| Underweight (<18.5 kg·m−2) | 5% | 4% | |
| Normal weight (18.5–24.9 kg·m−2) | 67% | 69% | |
| Overweight (25–29.9 kg·m−2) | 20% | 21% | |
| Obese (>30 kg·m−2) | 7% | 7% | |
| Smoking during pregnancy | 17% | 15% | 0.353 |
| Occupational activity | <0.001 | ||
| Housewife | 19% | 27% | |
| Sedentary job | 55% | 35% | |
| Active job | 26% | 38% | |
| Educational level | 0.074 | ||
| Primary | 26% | 23% | |
| Higher | 43% | 40% | |
| University | 31% | 37% | |
| Parity | 0.703 | ||
| Nulliparous | 58% | 59% | |
| 1 before | 36% | 34% | |
| 2+ before | 6% | 7% | |
| Previous miscarriage | 0.224 | ||
| No | 73% | 73% | |
| 1 before | 23% | 21% | |
| 2+ before | 4% | 6% | |
| Previous low birthweight | 2% | 2% | 0.361 |
| Previous preterm delivery | 4% | 3% | 0.451 |
| Control (n = 660) | Exercise (n = 688) | p-value | |
|---|---|---|---|
| Gestational age (days) | 277 ± 10 | 277 ± 12 | 0.776 |
| Preterm delivery | 5% | 5% | 0.671 |
| Birthweight (g) | 3265 ± 459 | 3234 ± 457 | 0.232 |
| Apgar score 1 min | 8.7 ± 1.2 | 8.8 ± 1.2 | 0.701 |
| Apgar score 5 min | 9.9 ± 0.7 | 9.8 ± 0.5 | 0.038 |
| Instrumental delivery | 16% | 15% | 0.482 |
| Cesarean delivery | 22% | 19% | 0.288 |
| Duration stage 1 of labor (min) | 430 ± 501 | 382 ± 256 | 0.039 |
| Duration stage 2 of labor (min) | 45 ± 50 | 49 ± 53 | 0.199 |
| Duration stage 3 of labor (min) | 8 ± 7 | 9 ± 11 | 0.060 |
| Outcome | Overall Analysis a | Sub-Group Analysis a | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Control (n = 660) [Reference] | Exercise (n = 688) | Previously Inactive, no Intervention (n = 562) Reference | Previously Active, Intervention (n = 117) | Previously Active, no Intervention (n = 98) | Previously Inactive, Intervention (n = 571) | |||||
| Crude OR (95% CI) | Adjusted OR (95% CI) b | Crude OR (95% CI) | Adjusted OR (95% CI) b | Crude OR (95% CI) | Adjusted OR (95% CI) b | Crude OR (95% CI) | Adjusted OR (95% CI) b | |||
| Mother | ||||||||||
| Gestational hypertension | [1] | 0.43 (0.26–0.71) p = 0.001 | 0.39 (0.23–0.67) p < 0.001 | [1] | 1.40 (0.67–2.92) p = 0.364 | 1.37 (0.63–2.98) p = 0.358 | 2.91 (1.54–5.50) p = 0.001 | 3.00 (1.54–5.83) p = 0.001 | 0.38 (0.20–0.71) p = 0.003 | 0.33 (0.17–0.65) p = 0.001 |
| Gestational diabetes | [1] | 0.53 (0.31–0.89) p = 0.016 | 0.48 (0.28–0.84) p = 0.015 | [1] | 0.42 (0.13–1.40) p = 0.157 | 0.35 (0.10–1.21) p = 0.174 | 1.21 (0.52–2.82) p = 0.657 | 1.06 (0.44–2.55) p = 0.723 | 0.57 (0.32–1.00) p = 0.057 | 0.52 (0.28–0.95) p = 0.042 |
| EGWG | [1] | 0.66 (0.52–0.84) p = 0.001 | 0.60 (0.46–0.79) p = 0.001 | [1] | 0.51 (0.31–0.83) p = 0.007 | 0.50 (0.29–0.87) p = 0.011 | 1.24 (0.80–1.95) p = 0.340 | 1.20 (0.73–1.99) p = 0.403 | 0.72 (0.56–0.94) p = 0.014 | 0.64 (0.48–0.86) p = 0.007 |
| Newborn | ||||||||||
| Low birth weight (<2500 g) | [1] | 0.79 (0.48–1.30) p = 0.413 | 0.80 (0.46–1.37) p = 0.474 | [1] | 0.59 (0.21–1.71) p = 0.362 | 0.58 (0.19–1.73) p = 0.204 | 0.52 (0.16–1.74) p = 0.316 | 0.54 (0.16–1.85) p = 0.226 | 0.76 (0.44–1.30) p = 0.371 | 0.78 (0.44–1.39) p = 0.427 |
| Macrosomia (>4000 g) | [1] | 0.43 (0.25–0.73) p = 0.002 | 0.36 (0.20–0.63) p = 0.007 | [1] | 0.48 (0.17–1.37) p = 0.168 | 0.47 (0.16–1.39) p = 0.204 | 0.88 (0.36–2.13) p = 0.764 | 0.89 (0.35–2.22) p = 0.326 | 0.41 (0.23–0.74) p = 0.003 | 0.33 (0.18–0.62) p = 0.005 |
| Outcome | Overall Analysis a | Sub-Group Analysis a | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control (n = 196) Reference | Exercise (n = 209) | Previously Inactive, no Intervention (n = 165) Reference | Previously Active, Intervention (n = 40) | Previously Active, no Intervention (n = 31) | Previously Inactive, Intervention (n = 169) | |||||||
| Crude OR (95% CI) | Adjusted OR (95% CI) b | Crude OR (95% CI) | Adjusted OR (95%CI) b | Crude OR (95% CI) | Adjusted OR (95% CI) b | Crude OR (95% CI) | Adjusted OR (95% CI) b | |||||
| Mother | ||||||||||||
| Return to pre-pregnancy weight within 6 months | [1] | 1.58 (0.98–2.55) p = 0.059 | 2.37 (1.26–4.54) p = 0.007 | [1] | 1.07 (0.48–2.38) p = 0.875 | 1.37 (0.45–4.11) p = 0.580 | 0.89 (0.32–2.48) p = 0.822 | 0.63 (0.17–2.32) p = 0.483 | 1.71 (1.01–2.89) p = 0.045 | 2.44 (1.25–4.75) p = 0.009 | ||
| Overweight/obesity | [1] | 0.80 (0.53–1.22) p = 0.307 | 0.57 (0.28–1.19) p = 0.136 | [1] | 0.48 (0.21–0.10) p = 0.083 | 0.88 (0.21–3.73) p = 0.862 | 0.92 (0.40–2.10) p = 0.845 | 1.83 (0.54–6.17) p = 0.332 | 0.88 (0.56–1.39) p = 0.585 | 0.67 (0.21–1.35) p = 0.219 | ||
| Hypertension (≥140/90 mmHg) | [1] | 0.44 (0.13–1.51) p = 0.192 | 0.97 (0.12–7.74) p = 0.976 | [1] | − | − | 0.88 (0.10–7.59) p = 0.904 | 4.59 (0.20–108.13) p = 0.345 | 0.54 (0.15–1.90) p = 0.335 | 1.57 (0.15–16.17) p = 0.704 | ||
| Hypertension (≥130/80 mmHg) | [1] | 0.58 (0.32, 1.07) p = 0.083 | 0.75 (0.35, 1.60) p = 0.454 | [1] | 0.25 (0.06, 1.14) p = 0.073 | 0.30 (0.05, 1.72) p = 0.177 | 0.89 (0.27, 2.96) p = 0.848 | 0.67 (0.15, 2.95) p = 0.601 | 0.66 (0.34, 1.26) p = 0.207 | 0.78 (0.35, 1.76) p = 0.551 | ||
| Cardiometabolic conditions | [1] | 0.19 (0.06–0.58) p = 0.003 | 0.27 (0.08–0.95) p = 0.041 | [1] | 0.24 (0.03–1.89) p = 0.177 | 0.64 (0.06–6.47) p = 0.708 | 0.64 (0.14–.93) p = 0.563 | 0.29 (0.03–2.70) p = 0.280 | 0.17 (0.05–0.59) p = 0.005 | 0.19 (0.05–0.76) p = 0.020 | ||
| Child | ||||||||||||
| Overweight/obesity at 1 year | [1] | 0.31 (0.15–0.62) p = 0.001 | 0.20 (0.06–0.63) p = 0.007 | [1] | 0.34 (0.10–1.22) p = 0.099 | 0.37 (0.06–2.13) p = 0.265 | 0.30 (0.07–1.37) p = 0.121 | − | 0.25 (0.12–0.55) p < 0.001 | 0.06 (0.01–0.30) p = 0.001 | ||
| Overweight/obesity at the end of follow-up | [1] | 0.89 (0.50–1.59) p = 0.702 | 0.57 (0.23–1.38) p = 0.210 | [1] | 0.61 (0.20–1.90) p = 0.396 | 0.39 (0.08–1.85) p = 0.235 | 0.56 (0.16–1.99) p = 0.366 | 0.97 (0.17–5.54) p = 0.969 | 0.87 (0.47–1.62) p = 0.667 | 0.61 (0.23–1.59) p = 0.310 | ||
| Low weight at 1 year | [1] | 2.68 (0.28–26.04) p = 0.397 | − | [1] | − | − | − | − | − | − | ||
| Low weight at the end of follow-up | [1] | 1.16 (0.54–2.50) p = 0.702 | 0.41 (0.12–1.44) p = 0.166 | [1] | 0.39 (0.05–3.19) p = 0.383 | 0.22 (0.02–2.63) p = 0.234 | 1.58 (0.40–6.15) p = 0.513 | 1.00 (0.08–12.28) p = 1.000 | 1.49 (0.64–3.44) p = 0.352 | 0.47 (0.12–1.79) p = 0.268 | ||
| Cardiometabolic conditions at the end of follow-up | [1] | 1.11 (0.37–3.36) p = 0.856 | 0.55 (0.11–2.68) p = 0.455 | [1] | 0.86 (0.10–7.58) p = 0.892 | 1.45 (0.09–23.06) p = 0.792 | 1.06 (0.12–9.40) p = 0.958 | − | 1.18 (0.35-3.94) p = 0.790 | 0.39 (0.07–2.23) p = 0.287 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perales, M.; Valenzuela, P.L.; Barakat, R.; Cordero, Y.; Peláez, M.; López, C.; Ruilope, L.M.; Santos-Lozano, A.; Lucia, A. Gestational Exercise and Maternal and Child Health: Effects until Delivery and at Post-Natal Follow-up. J. Clin. Med. 2020, 9, 379. https://doi.org/10.3390/jcm9020379
Perales M, Valenzuela PL, Barakat R, Cordero Y, Peláez M, López C, Ruilope LM, Santos-Lozano A, Lucia A. Gestational Exercise and Maternal and Child Health: Effects until Delivery and at Post-Natal Follow-up. Journal of Clinical Medicine. 2020; 9(2):379. https://doi.org/10.3390/jcm9020379
Chicago/Turabian StylePerales, María, Pedro L. Valenzuela, Ruben Barakat, Yaiza Cordero, Mireia Peláez, Carmen López, Luis M. Ruilope, Alejandro Santos-Lozano, and Alejandro Lucia. 2020. "Gestational Exercise and Maternal and Child Health: Effects until Delivery and at Post-Natal Follow-up" Journal of Clinical Medicine 9, no. 2: 379. https://doi.org/10.3390/jcm9020379