Short-Term Effects of Comprehensive Pulmonary Rehabilitation and its Maintenance in Patients with Idiopathic Pulmonary Fibrosis: A Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
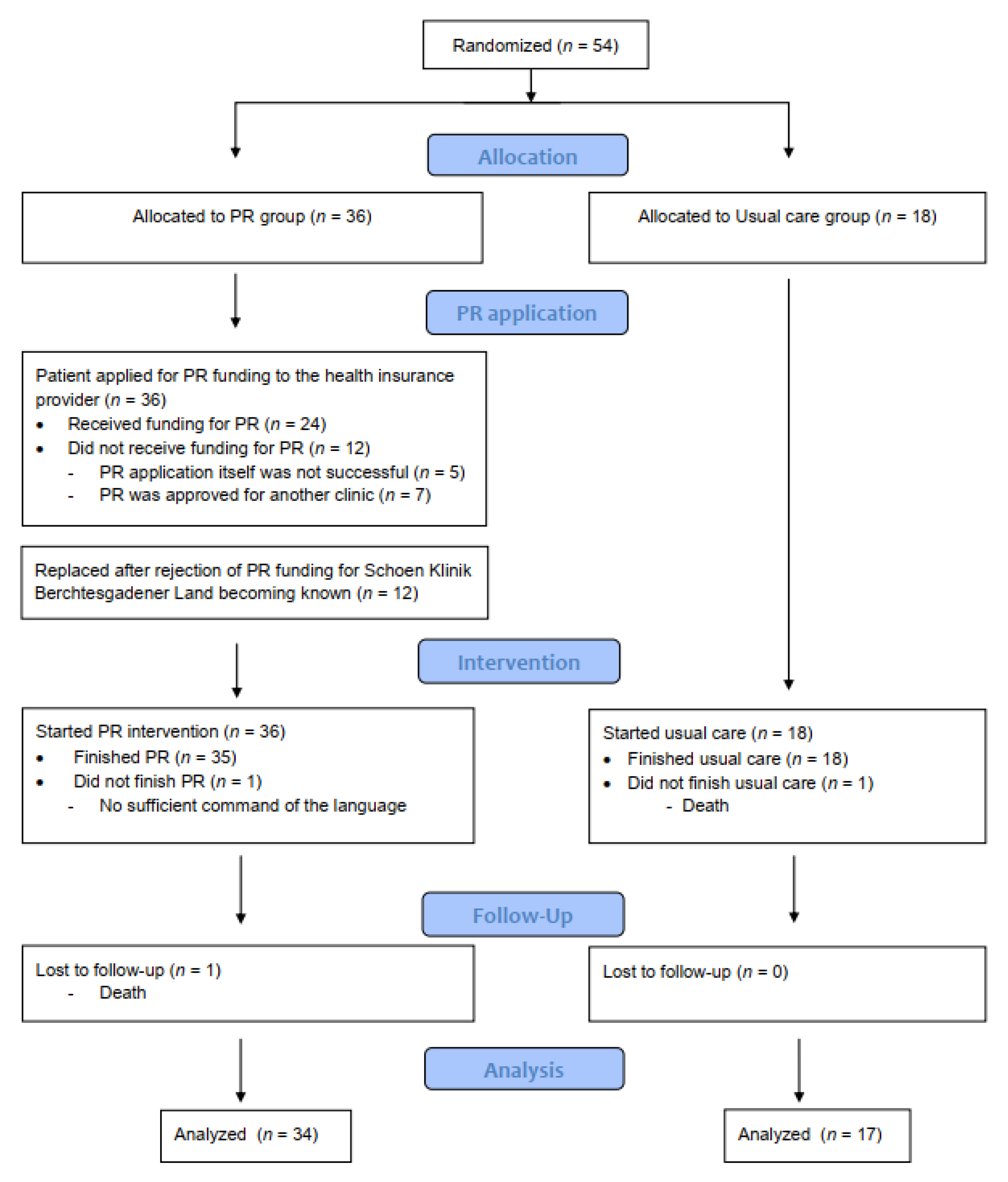
2.1. Study Population
2.2. Study Design
2.3. Assessment
2.4. Statistical Methods
3. Results
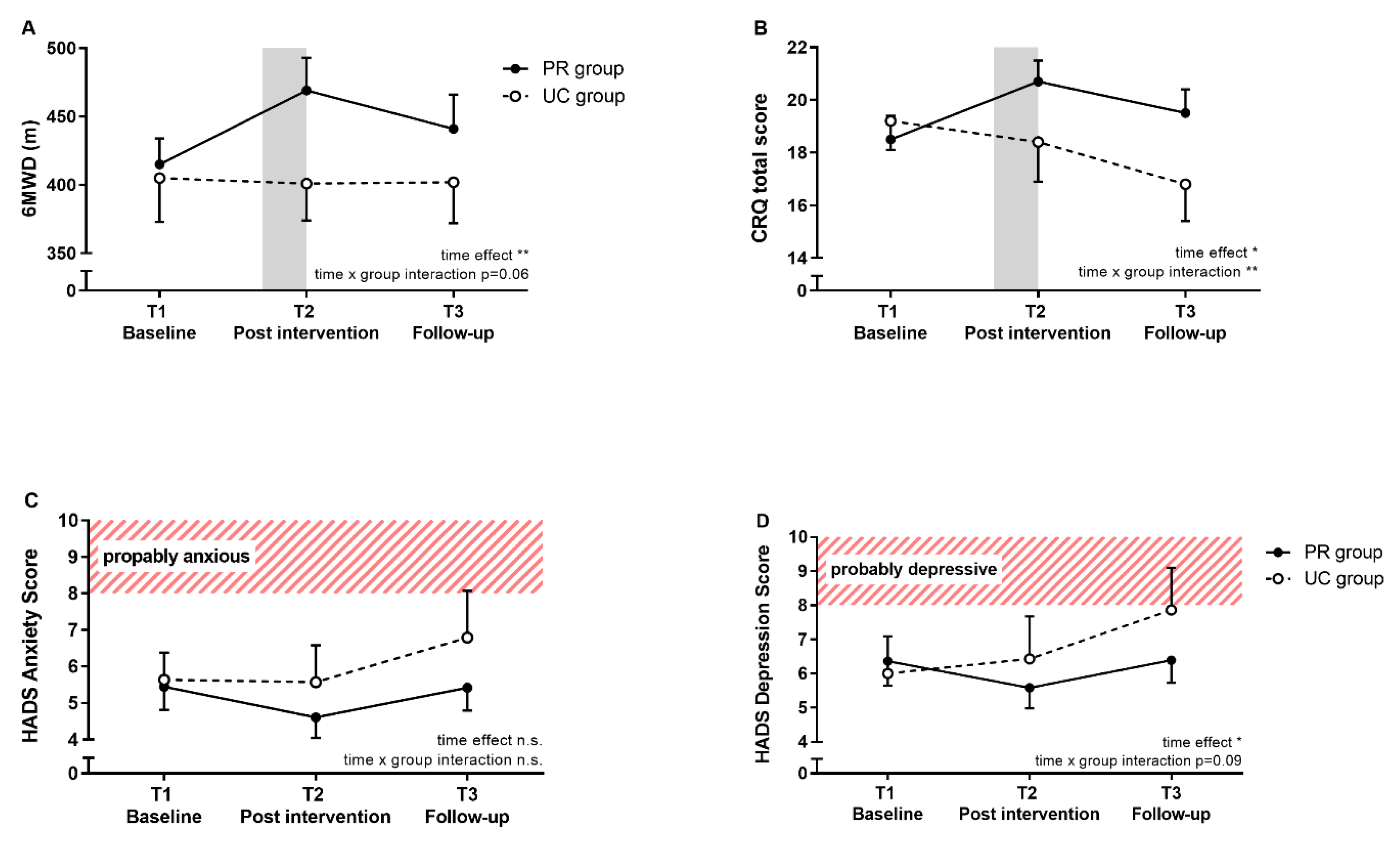
3.1. Primary Outcome
3.2. Secondary Outcomes
4. Discussion
4.1. Short-Term PR Effects
4.2. Maintenance of PR Effects
4.3. Determinants of Short-Term PR Success
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| 6MWD | 6-min walk distance |
| 6MWT | 6-min walk test |
| ATS | American Thoracic Society |
| BMI | Body mass index |
| CRQ | Chronic Respiratory disease Questionnaire |
| DLCO | Diffusion capacity of the lung for carbon monoxide |
| ERS | European Respiratory Society |
| FEV1 | Forced expiratory volume in 1 s |
| FVC | Forced vital capacity |
| GAP index | Gender, age and physiologic variables index |
| HADS | Hospital Anxiety and Depression Scale |
| HRCT | High-resolution computed tomography |
| HRQL | Health-related quality of life |
| ILD | Interstitial lung disease |
| IPF | Idiopathic pulmonary fibrosis |
| LTOT | Long term oxygen therapy |
| PaO2 | Partial pressure of oxygen by breathing room air |
| PaCO2 | Partial pressure of carbon dioxide by breathing room air |
| PR | Pulmonary Rehabilitation |
| SF36 | Short-form 36 |
| T1 | Baseline |
| T2 | Post pulmonary rehabilitation (Pulmonary rehabilitation group) or after 9 weeks from baseline (Usual care group) |
| T3 | at 3 months follow-up |
| TLC | Total lung capacity |
| UC | Usual care. |
References
- Lederer, D.J.; Martinez, F.J. Idiopathic Pulmonary Fibrosis. N. Engl. J. Med. 2018, 378, 1811–1823. [Google Scholar] [CrossRef]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Lynch, D.A. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef]
- Kreuter, M.; Swigris, J.; Pittrow, D.; Geier, S.; Klotsche, J.; Prasse, A.; Grohé, C. The clinical course of idiopathic pulmonary fibrosis and its association to quality of life over time: Longitudinal data from the INSIGHTS-IPF registry. Respir. Res. 2019, 20, 59. [Google Scholar] [CrossRef] [PubMed]
- Bahmer, T.; Kirsten, A.M.; Waschki, B.; Rabe, K.F.; Magnussen, H.; Kirsten, D.; Watz, H. Prognosis and longitudinal changes of physical activity in idiopathic pulmonary fibrosis. BMC Pulm. Med. 2017, 17, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Pitta, F. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Dowman, L.; Hill, C.J.; Holland, A.E. Pulmonary rehabilitation for interstitial lung disease. Cochrane Database Syst. Rev. 2014, 10, CD006322. [Google Scholar] [CrossRef]
- Huppmann, P.; Sczepanski, B.; Boensch, M.; Winterkamp, S.; Schönheit-Kenn, U.; Neurohr, C.; Kenn, K. Effects of inpatient pulmonary rehabilitation in patients with interstitial lung disease. Eur. Respir. J. 2013, 42, 444–453. [Google Scholar] [CrossRef] [Green Version]
- Holland, A.E.; Hill, C.J.; Conron, M.; Munro, P.; McDonald, C.F. Short term improvement in exercise capacity and symptoms following exercise training in interstitial lung disease. Thorax 2008, 63, 549–554. [Google Scholar] [CrossRef] [Green Version]
- Dowman, L.M.; McDonald, C.F.; Hill, C.J.; Lee, A.L.; Barker, K.; Boote, C.; Gillies, R. The evidence of benefits of exercise training in interstitial lung disease: A randomised controlled trial. Thorax 2017, 72, 610–619. [Google Scholar] [CrossRef] [Green Version]
- Perez-Bogerd, S.; Wuyts, W.; Barbier, V.; Demeyer, H.; Van Muylem, A.; Janssens, W.; Troosters, T. Short and long-term effects of pulmonary rehabilitation in interstitial lung diseases: A randomised controlled trial. Respir Res 2018, 19, 182. [Google Scholar] [CrossRef]
- Sharp, C.; McCabe, M.; Hussain, M.J.; Dodd, J.W.; Lamb, H.; Adamali, H.; Smith, D. Duration of benefit following completion of pulmonary rehabilitation in interstitial lung disease-an observational study. QJM Mon. J. Assoc. Phys. 2017, 110, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Hill , C.J.; Glaspole , I.; Goh , N.; McDonald , C.F. Predictors of benefit following pulmonary rehabilitation for interstitial lung disease. Respir. Med. 2012, 106, 429–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gloeckl, R.; Heinzelmann, I.; Baeuerle, S.; Damm, E.; Schwedhelm, A.L.; Diril, M.; Kenn, K. Effects of whole body vibration in patients with chronic obstructive pulmonary disease—A randomized controlled trial. Respir. Med. 2012, 106, 75–83. [Google Scholar] [CrossRef] [Green Version]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Choi, S.M.; Lee, J.; Park, Y.S.; Lee, C.H.; Yim, J.J.; Lee, S.M. Validation of the GAP score in Korean patients with idiopathic pulmonary fibrosis. Chest 2015, 147, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Ley, B.; Ryerson, C.J.; Vittinghoff, E.; Ryu, J.H.; Tomassetti, S.; Lee, J.S.; King, T.E. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann. Intern. Med. 2012, 156, 684–691. [Google Scholar] [CrossRef]
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, V.; Hernandes, N.A.; Mitchell, K.E.; Hill, C.J.; Carlin, B.W. An official systematic review of the European Respiratory Society/American Thoracic Society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef]
- Puhan, M.A.; Frey, M.; Büchi, S.; Schünemann, H.J. The minimal important difference of the hospital anxiety and depression scale in patients with chronic obstructive pulmonary disease. Health Qual. Life Outcomes 2008, 6, 46. [Google Scholar] [CrossRef] [Green Version]
- Arizono, S.; Taniguchi, H.; Sakamoto, K.; Kondoh, Y.; Kimura, T.; Kataoka, K.; Kozu, R. Endurance time is the most responsive exercise measurement in idiopathic pulmonary fibrosis. Respir. Care 2014, 59, 1108–1115. [Google Scholar] [CrossRef] [Green Version]
- Vainshelboim, B.; Oliveira, J.; Fox, B.D.; Soreck, Y.; Fruchter, O.; Kramer, M.R. Long-term effects of a 12-week exercise training program on clinical outcomes in idiopathic pulmonary fibrosis. Lung 2015, 193, 345–354. [Google Scholar] [CrossRef]
- Ryerson, C.J.; Cayou, C.; Topp, F.; Hilling, L.; Camp, P.G.; Wilcox, P.G.; Garvey, C. Pulmonary rehabilitation improves long-term outcomes in interstitial lung disease: A prospective cohort study. Respir. Med. 2014, 108, 203–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; Wanger, J. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, R.; Vanfleteren, L.E.; Franssen, F.M.; Sarv, J.; Taib, Z.; Groenen, M.T.; Spruit, M.A. Objectively identified comorbidities in COPD: Impact on pulmonary rehabilitation outcomes. Eur. Respir. J. 2015, 46, 545–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssens, T.; De Peuter, S.; Stans, L.; Verleden, G.; Troosters, T.; Decramer, M.; Van den Bergh, O. Dyspnea perception in COPD: Association between anxiety, dyspnea-related fear, and dyspnea in a pulmonary rehabilitation program. Chest 2011, 140, 618–625. [Google Scholar] [CrossRef]
- Maurer, J.; Rebbapragada, V.; Borson, S.; Goldstein, R.; Kunik, M.E.; Yohannes, A.M.; Hanania, N.A. Anxiety and depression in COPD: Current understanding, unanswered questions, and research needs. Chest 2008, 134 (Suppl. 4), 43S–56S. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.H.; Mak, Y.W. Psycho-Physiological Associates of Dyspnea in Hospitalized Patients with Interstitial Lung Diseases: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 1277. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| UC Group (n = 17) | PR Group (n = 34) | |
|---|---|---|
| Gender, m (%) | 13 (81) | 25 (76) |
| Age, y | 65 (10) | 68 (9) |
| BMI, kg/m2 | 27.8 (5.1) | 27.2 (4.4) |
| FVC, % pred. | 72 (20) | 74 (19) |
| TLC, % pred. | 70 (17) | 71 (14) |
| DLCO, % pred. | 36.6 (18.8) | 44.1 (15.4) |
| PaO2, mmHg | 61.1 (15.0) | 72.8 (13.3) |
| PaCO2, mmHg | 37.5 (4.6) | 38.8 (4.1) |
| Time between T1 and T2 (days) | 65 (26) | 77 (37) |
| 6MWD, m | 405 (109) | 415 (101) |
| GAP index | ||
| Stage I, n (%) | 6 (35) | 18 (53) |
| Stage II, n (%) | 8 (47) | 11 (32) |
| Stage III, n (%) | 3 (18) | 5 (15) |
| CRQ scores | ||
| dyspnea | 4.5 (1.4) | 4.7 (1.7) |
| fatigue | 4.4 (1.1) | 4.4 (1.2) |
| emotional function | 4.7 (0.9) | 4.7 (1.2) |
| mastery | 5.0 (1.2) | 4.8 (1.5) |
| total | 18.7 (3.8) | 18.6 (5.0) |
| SF36 summary scores | ||
| physical component | 39.9 (10.0) | 41.4 (9.9) |
| mental component | 45.3 (13.3) | 44.6 (12.9) |
| HADS scores | ||
| anxiety | 5.4 (2.8) | 5.5 (3.7) |
| depression | 5.9 (3.9) | 6.4 (4.1) |
| LTOT, n | 6 (38) | 7 (22) |
| Between-Group Difference (Mean Difference (95% CI)) | p-Value | |
|---|---|---|
| CRQ total | ||
| T1 to T2 | 3.0 (0.7–5.3) | 0.011 |
| T1 to T3 | 3.5 (1.5–5.4) | 0.001 |
| CRQ dyspnea | ||
| T1 to T2 | 0.9 (0.2–1.6) | 0.013 |
| T1 to T3 | 1.3 (0.5–2.1) | 0.002 |
| CRQ fatigue | ||
| T1 to T2 | 0.7 (0.0–1.4) | 0.059 |
| T1 to T3 | 0.7 (0.2–1.1) | 0.003 |
| CRQ emotional function | ||
| T1 to T2 | 0.8 (0.2–1.4) | 0.008 |
| T1 to T3 | 0.7 (0.2–1.2) | 0.009 |
| CRQ mastery | ||
| T1 to T2 | 0.6 (0.1–1.1) | 0.019 |
| T1 to T3 | 0.8 (0.1–1.4) | 0.018 |
| SF-36 physical component summary score | ||
| T1 to T2 | 2.8 (1.6–7.2) | 0.213 |
| T1 to T3 | 2.1 (4.3–8.6) | 0.504 |
| SF-36 mental component summary score | ||
| T1 to T2 | 7.1 (1.9–12.3) | 0.008 |
| T1 to T3 | 6.1 (–3.9–16) | 0.222 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarosch, I.; Schneeberger, T.; Gloeckl, R.; Kreuter, M.; Frankenberger, M.; Neurohr, C.; Prasse, A.; Freise, J.; Behr, J.; Hitzl, W.; et al. Short-Term Effects of Comprehensive Pulmonary Rehabilitation and its Maintenance in Patients with Idiopathic Pulmonary Fibrosis: A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1567. https://doi.org/10.3390/jcm9051567
Jarosch I, Schneeberger T, Gloeckl R, Kreuter M, Frankenberger M, Neurohr C, Prasse A, Freise J, Behr J, Hitzl W, et al. Short-Term Effects of Comprehensive Pulmonary Rehabilitation and its Maintenance in Patients with Idiopathic Pulmonary Fibrosis: A Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(5):1567. https://doi.org/10.3390/jcm9051567
Chicago/Turabian StyleJarosch, Inga, Tessa Schneeberger, Rainer Gloeckl, Michael Kreuter, Marion Frankenberger, Claus Neurohr, Antje Prasse, Julia Freise, Juergen Behr, Wolfgang Hitzl, and et al. 2020. "Short-Term Effects of Comprehensive Pulmonary Rehabilitation and its Maintenance in Patients with Idiopathic Pulmonary Fibrosis: A Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 5: 1567. https://doi.org/10.3390/jcm9051567