Transcatheter Mitral Repair for Functional Mitral Regurgitation According to Left Ventricular Function: A Real-Life Propensity-Score Matched Study

 , , ,
, , ,  , , ,
, , ,  , , , ,
, , , ,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
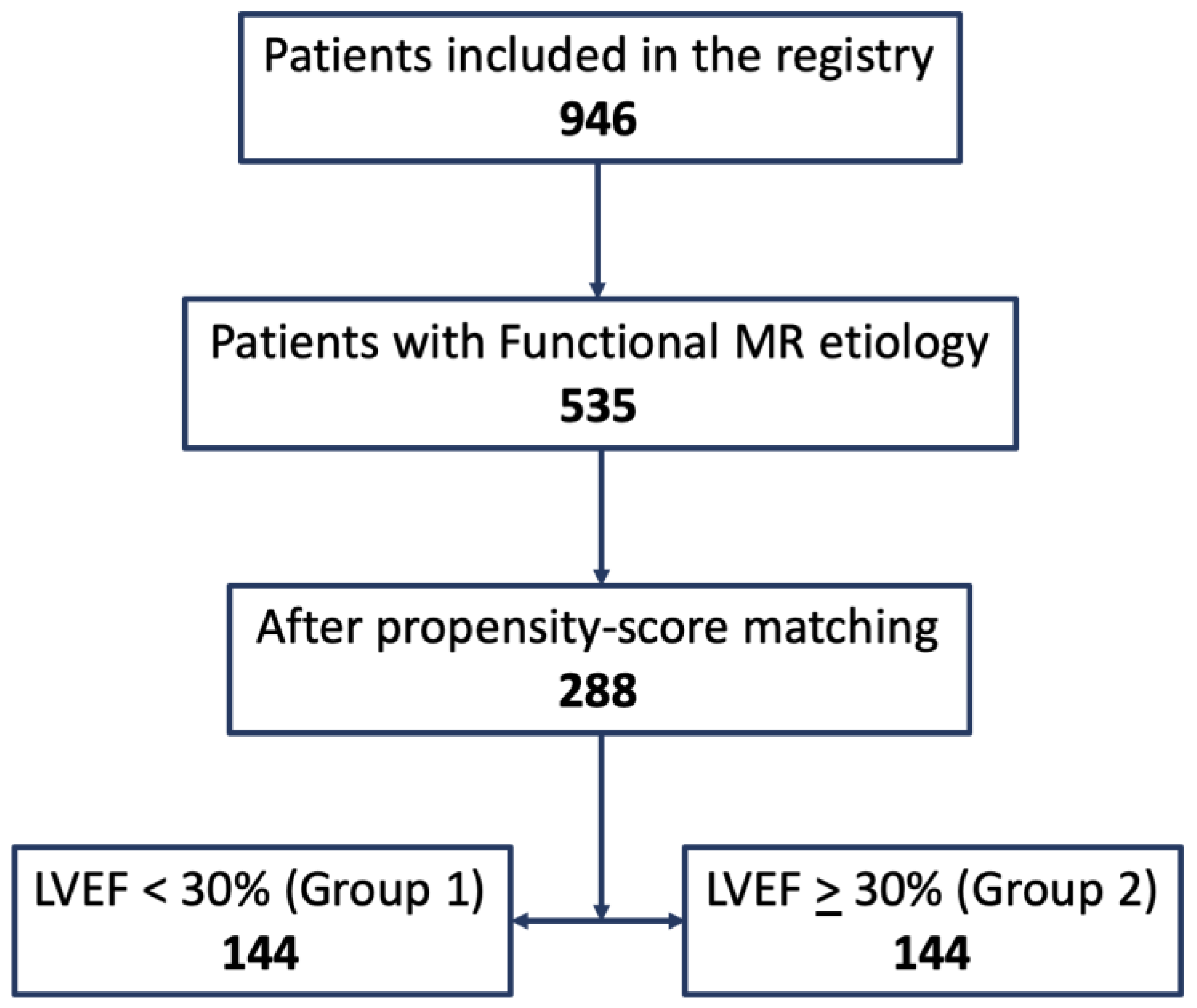
2.1. Study Population
2.2. Variable Definitions
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
Study Population
4. Outcomes
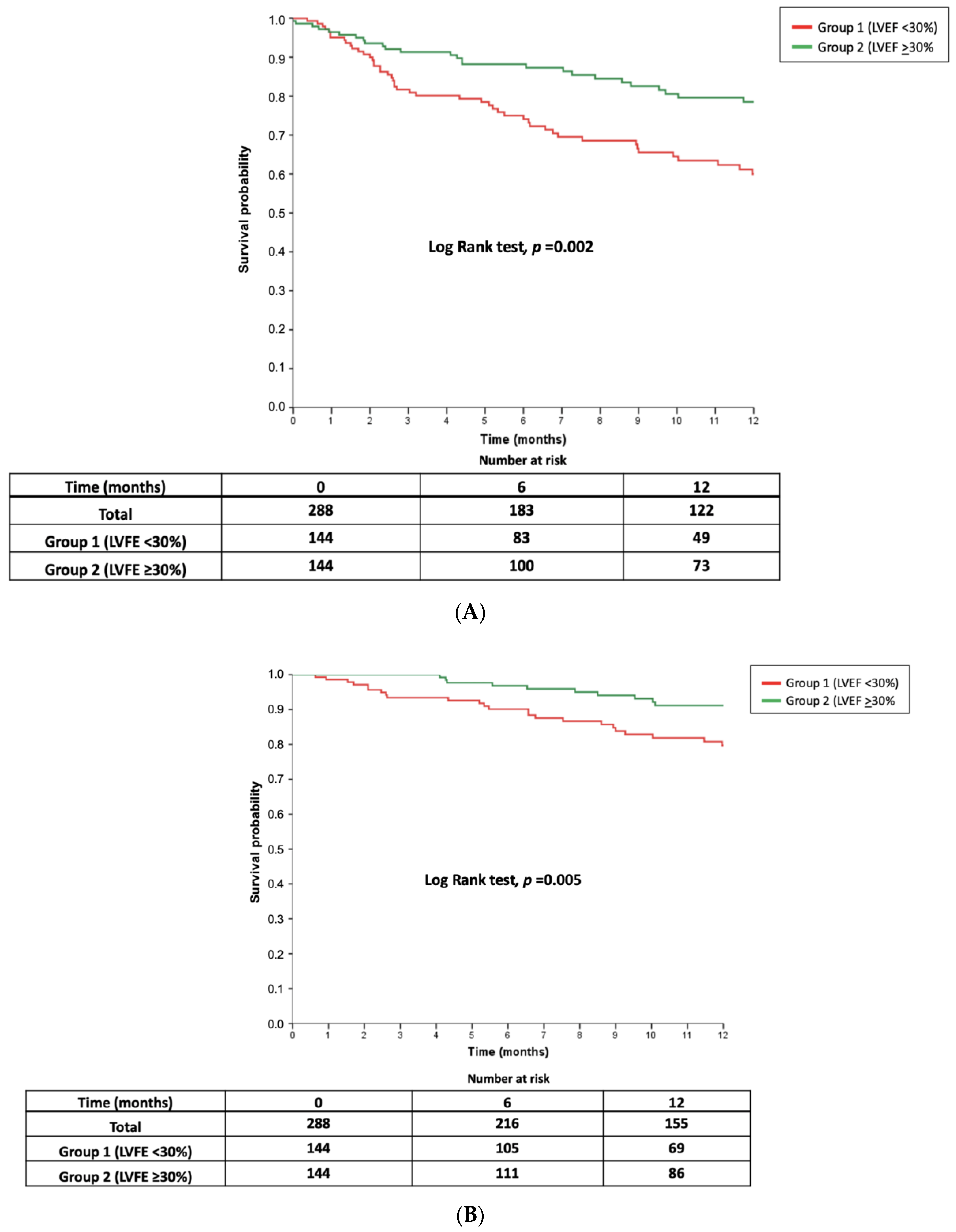
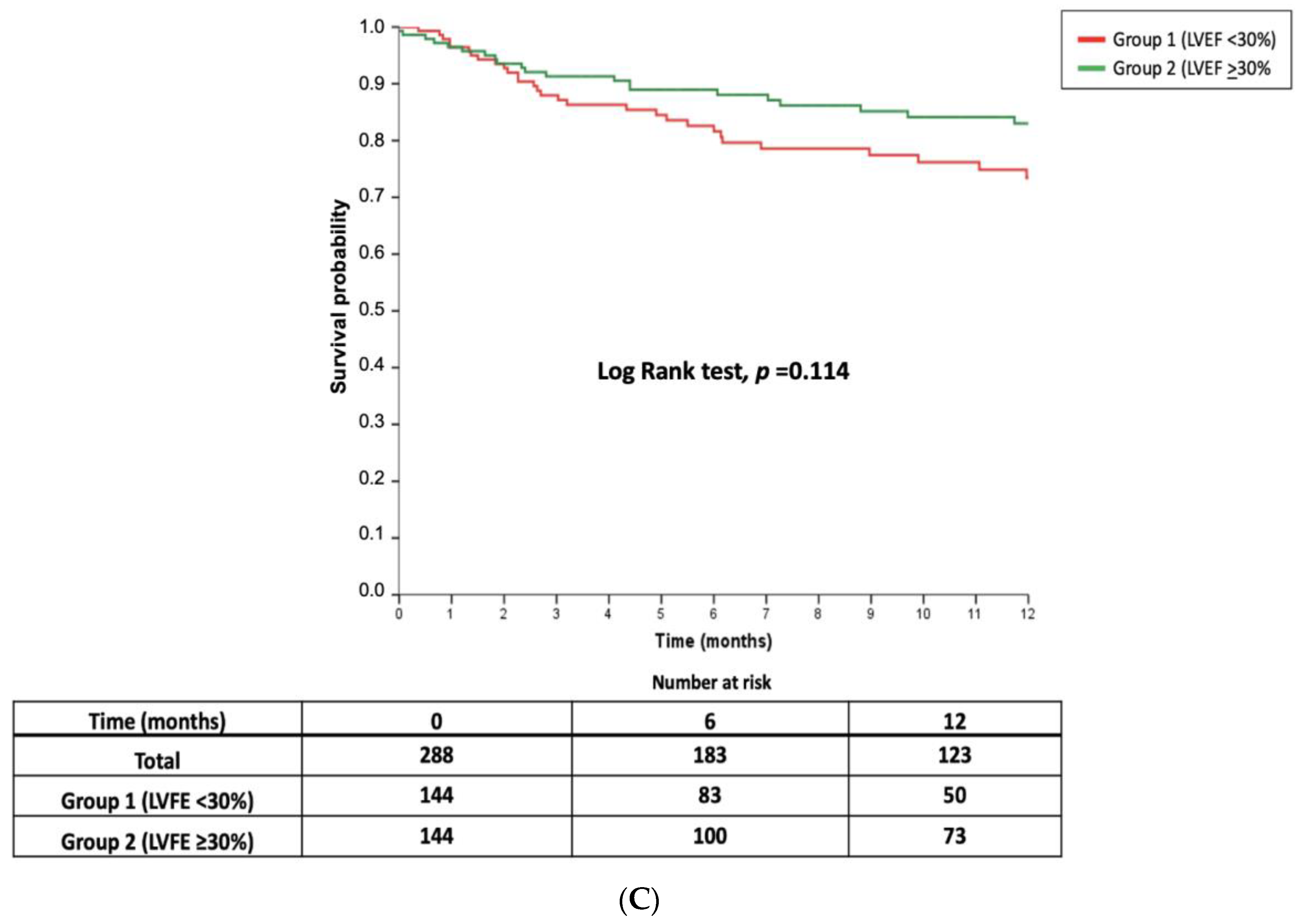
4.1. Primary Endpoint
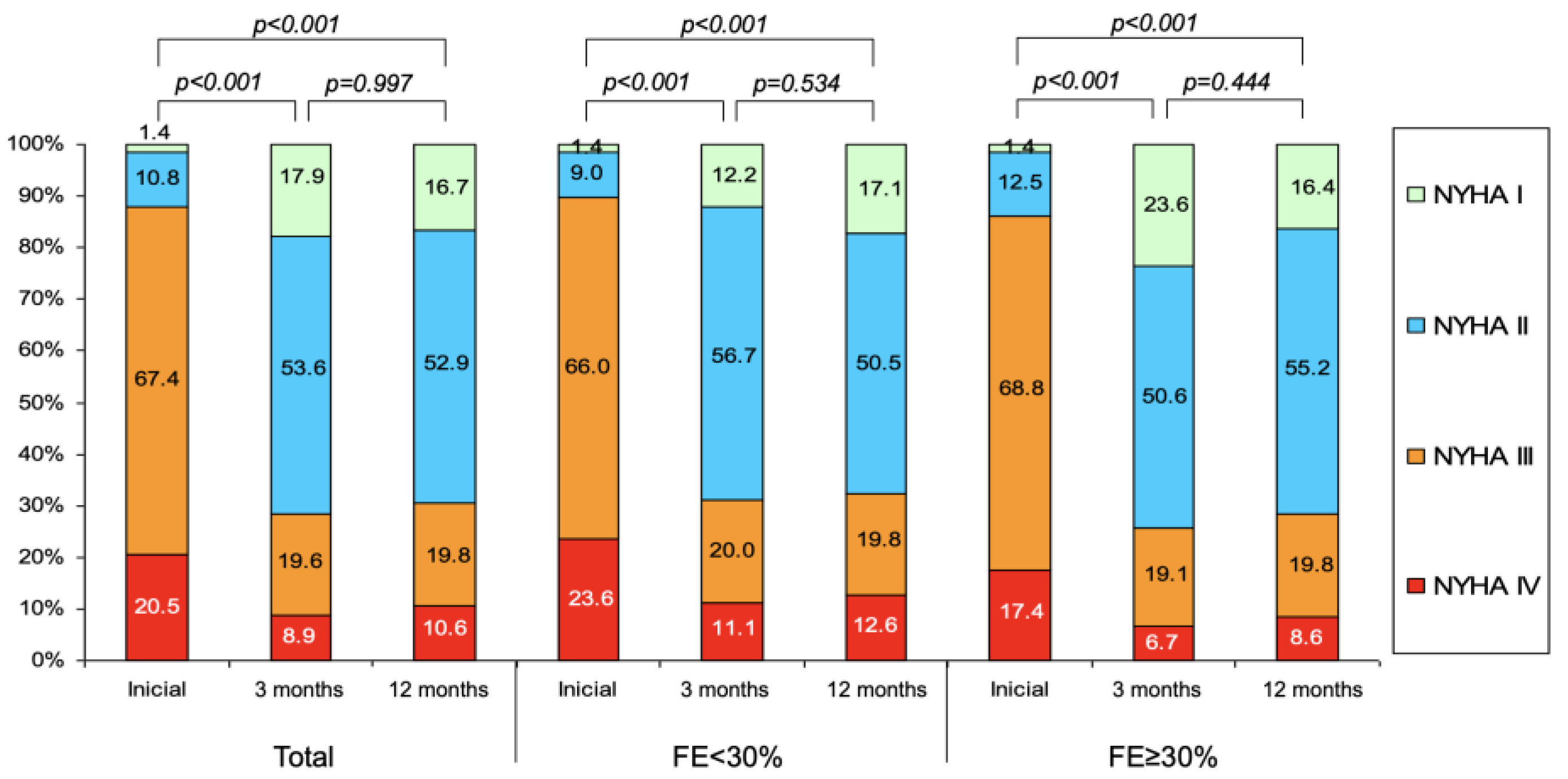
4.2. Secondary Endpoints
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Asgar, A.W.; Mack, M.J.; Stone, G.W. Secondary mitral regurgitation in heart failure: Pathophysiology, prognosis, and therapeutic considerations. J. Am. Coll. Cardiol. 2015, 65, 1231–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef]
- David, T.E.; Armstrong, S.; McCrindle, B.W.; Manlhiot, C. Late outcomes of mitral valve repair for mitral regurgitation due to degenerative disease. Circulation 2013, 127, 1485–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grayburn, P.A.; Carabello, B.; Hung, J.; Gillam, L.D.; Liang, D.; Mack, M.J.; McCarthy, P.M.; Miller, D.C.; Trento, A.; Siegel, R.J. Defining “severe” secondary mitral regurgitation: Emphasizing an integrated approach. J. Am. Coll. Cardiol. 2014, 64, 2792–2801. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2786. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Fleisher, L.A., 3rd; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2017, 70, 252–289. [Google Scholar] [CrossRef]
- Mihaljevic, T.; Lam, B.K.; Rajeswaran, J.; Takagaki, M.; Lauer, M.S.; Gillinov, A.M.; Blackstone, E.H.; Lytle, B.W. Impact of mitral valve annuloplasty combined with revascularization in patients with functional ischemic mitral regurgitation. J. Am. Coll. Cardiol. 2007, 49, 191–2201. [Google Scholar] [CrossRef] [Green Version]
- Diodato, M.D.; Moon, M.R.; Pasque, M.K.; Barner, H.B.; Moazami, N.; Lawton, J.S.; Bailey, M.S.; Guthrie, T.J.; Meyers, B.F.; Damiano, R.J., Jr. Repair of ischemic mitral regurgitation does not increase mortality or improve long-term survival in patients undergoing coronary artery revascularization: A propensity analysis. Ann. Thorac. Surg. 2004, 78, 794–799. [Google Scholar] [CrossRef]
- Maisano, F.; Franzen, O.; Baldus, S.; Schäfer, U.; Hausleiter, J.; Butter, C.; Ussia, G.P.; Sievert, H.; Richardt, G.; Widder, J.D.; et al. Percutaneous mitral valve interventions in the real world: Early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J. Am. Coll. Cardiol. 2013, 62, 1052–1061. [Google Scholar] [CrossRef] [Green Version]
- Nickenig, G.; Estevez-Loureiro, R.; Franzen, O.; Tamburino, C.; Vanderheyden, M.; Lüscher, T.F.; Moat, N.; Price, S.; Dall’Ara, G.; Winter, R.; et al. Percutaneous mitral valve edgeto- edge repair: In-hospital results and 1-year follow-up of 628 patients of the 2011–2012 Pilot European Sentinel Registry. J. Am. Coll. Cardiol. 2014, 64, 875–884. [Google Scholar] [CrossRef] [Green Version]
- Pascual, I.; Arzamendi, D.; Carrasco-Chinchilla, F.; Fernández-Vázquez, F.; Freixa, X.; Nombela-Franco, L.; Avanzas, P.; Serrador Frutos, A.M.; Pan, M.; Cid Álvarez, A.B.; et al. Transcatheter mitral repair according to the cause of mitral regurgitation: Real-life data from the Spanish MitraClip registry. Rev. Esp. Cardiol. (Engl. Ed.) 2019. [Google Scholar] [CrossRef]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter mitral-valve repair in patients with heart failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Obadia, J.F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; et al. Percutaneous repair or medical treatment for secondary mitral regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Cubero-Gallego, H.; Hernandez-Vaquero, D.; Avanzas, P.; Almendarez, M.; Adeba, A.; Lorca, R.; Rozado, J.; Escalera, A.; Silva, J.; Moris, C.; et al. Outcomes with percutaneous mitral repair vs. optimal medical treatment for functional mitral regurgitation: Systematic review. Ann. Transl. Med. 2020. Ahead of print. [Google Scholar]
- Rossi, A.; Dini, F.L.; Faggiano, P.; Agricola, E.; Cicoira, M.; Frattini, S.; Simioniuc, A.; Gullace, M.; Ghio, S.; Enriquez-Sarano, M.; et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart 2011, 97, 1675–1680. [Google Scholar] [CrossRef]
- Garcia-Cosio Carmena, M.A.; Roig Minguell, E.; Ferrero-Gregori, A.; Vazquez Garcia, R.; Delgado Jimenez, J.; Cinca, J. Prognostic implications of functional mitral regurgitation in patients with heart failure and reduced ejection fraction. Rev. Esp. Cardiol. 2017, 70, 785–787. [Google Scholar] [CrossRef]
- Sannino, A.; Smith, R.L., 2nd; Schiattarella, G.G.; Trimarco, B.; Esposito, G.; Grayburn, P.A. Survival and Cardiovascular Outcomes of Patients with Secondary Mitral Regurgitation: A Systematic Review and Meta-analysis. JAMA Cardiol. 2017, 2, 1130–1139. [Google Scholar] [CrossRef]
- Monteagudo Ruiz, J.M.; Zamorano Gomez, J.L. Importance of the Left Ventricle in Secondary Mitral Regurgitation. Hunt with Cats and You Catch Only Rats. Rev. Esp. Cardiol. 2019, 72, 994–997. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Chiarito, M.; Pagnesi, M.; Martino, E.A.; Pighi, M.; Scotti, A.; Biondi-Zoccai, G.; Latib, A.; Landoni, G.; Mario, C.D.; Margonato, A.; et al. Outcome after percutaneous edge-to-edgemitral repair for functional and degenerative mitral regurgitation: A systematicreview and meta-analysis. Heart 2018, 104, 306–312. [Google Scholar] [CrossRef] [Green Version]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous Repair or Surgery for Mitral Regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef] [Green Version]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Deb, S.; Austin, P.C.; Tu, J.V.; Ko, D.T.; Mazer, C.D.; Kiss, A.; Fremes, S.E. A review of propensity-score methods and their use in cardiovascular research. Can. J. Cardiol. 2016, 32, 259–365. [Google Scholar] [CrossRef]
- Kumar, A.; Al-Khafaji, J.; Shariff, M.; Vaz, I.P.; Adalja, D.; Doshi, R. Percutaneous mitral valve repair for secondary mitral valve regurgitation: A systematic review and meta-analysis. Eur. J. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Goel, S.; Pasam, R.T.; Wats, K.; Chava, S.; Gotesman, J.; Sharma, A.; Malik, B.A.; Ayzenberg, S.; Frankel, R.; Shani, J.; et al. Mitraclip Plus Medical Therapy Versus Medical Therapy Alone for Functional Mitral Regurgitation: A Meta-Analysis. Cardiol. Ther. 2019. Ahead of print. [Google Scholar]
- Sanchis, L.; Freixa, X.; Regueiro, A.; Perdomo, J.M.; Sabate, M.; Sitges, M. Safety and outcomes of MitraClip implantation in functional mitral regurgitation according to degree of left ventricular dysfunction. Rev. Esp. Cardiol. (Engl. Ed.) 2019. [Google Scholar] [CrossRef]
- Pascual, I.; Benito-González, T.; Hernandez-Vaquero, D.; Estévez-Loureiro, R.; Lorca, R.; Garrote-Coloma, C.; Avanzas, P.; Gualis, J.; Adeba, A.; Pérez de Prado, A.; et al. Percutaneous treatment with Mitraclip for functional mitral regurgitation: Medium-term follow up according to left ventricular function. Ann. Transl. Med. 2020. Ahead of print. [Google Scholar]
- Bertaina, M.; Galluzzo, A.; D’Ascenzo, F.; Conrotto, F.; Grosso Marra, W.; Frea, S.; Alunni, G.; Crimi, G.; Moretti, C.; Montefusco, A.; et al. Prognostic impact of MitraClip in patients with left ventricular dysfunction and functional mitral valve regurgitation: A comprehensive meta-analysis of RCTs and adjusted observational studies. Int. J. Cardiol. 2019, 290, 70–76. [Google Scholar] [CrossRef]
- Geis, N.A.; Puls, M.; Lubos, E.; Zuern, C.S.; Franke, J.; Schueler, R.; von Bardeleben, R.S.; Boekstegers, P.; Ouarrak, T.; Zahn, R.; et al. Safety and efficacy of MitraClip™ therapy in patients with severely impaired left ventricular ejection fraction: Results from the German transcatheter mitral valve interventions (TRAMI) registry. Eur. J. Heart Fail. 2018, 20, 598–608. [Google Scholar] [CrossRef] [Green Version]
- Arnold, S.V.; Chinnakondepalli, K.M.; Spertus, J.A.; Magnuson, E.A.; Baron, S.J.; Kar, S.; Lim, D.S.; Mishell, J.M.; Abraham, W.T.; Lindenfeld, J.A.; et al. Health Status After Transcatheter Mitral-Valve Repair in Heart Failure and Secondary Mitral Regurgitation: COAPT Trial. J. Am. Coll. Cardiol. 2019, 73, 2123–2132. [Google Scholar] [CrossRef]
- Arnold, S.V.; Li, Z.; Vemulapalli, S.; Baron, S.J.; Mack, M.J.; Kosinski, A.S.; Reynolds, M.R.; Hermiller, J.B.; Rumsfeld, J.S.; Cohen, D.J. Association of transcatheter mitral valve repair with quality of life outcomes at 30 days and 1 year: Analysis of the transcatheter valve therapy registry. JAMA Cardiol. 2018, 3, 1151–1159. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total FMR Group n = 535 | FE < 30% n = 229 (42.8%) | FE ≥ 30% n = 306 (57.2%) | p |
|---|---|---|---|---|
| Age (years) | 71.0 ± 10.8 | 68.1 ± 11.7 | 73.2 ± 9.7 | <0.001 |
| Sex (n (%)) Men Women | 396 (74.0) 139 (26.0) | 174 (76.30) 55 (24.0) | 222 (72.5) 84 (27.5) | 0.370 |
| BSA (m2) | 1.82 ± 0.20 | 1.83 ± 0.23 | 1.76 ± 0.38 | 0.012 |
| BMI (kg/m2) | 27.2 ± 4.5 | 26.6 ± 4.4 | 27.6 ± 4.5 | 0.050 |
| BMI ≥ 30 kg/m2 | 124 (23.2) | 44 (19.2) | 80 (26.1) | 0.060 |
| LVEF, % | 34.3 ± 12.5 | 23.5 ± 6.4 | 42.1 ± 9.9 | - |
| Type 2 Diabetes Mellitus | 189 (35.3) | 79 (34.5) | 110 (35.9) | 0.728 |
| Ischemic Heart Disease | 302 (56.4) | 115 (50.2) | 187 (61.1) | 0.012 |
| Hypertension | 372 (69.5) | 140 (61.1) | 232 (75.8) | <0.001 |
| Previous Cardiac Surgery | 89 (16.6) | 30 (13.1) | 59 (19.3) | 0.058 |
| Hemodyalisis | 9 (1.7) | 3 (1.3) | 6 (2.0) | 0.739 |
| Creatinine (mg/dL) | 1.37 ± 0.57 | 1.34 ± 0.51 | 1.40 ± 0.61 | 0.268 |
| eGFR (mL/min) | 62.2 ± 25.8 | 62.8 ± 23.2 | 61.7 ± 27.6 | 0.763 |
| NYHA Class I II III IV | 12(2.2) 59(11.0) 355 (66.4) 109 (20.4) | 4(1.7) 22(9.6) 149 (65.1) 54 (23.6) | 8(2.6) 37(12.1) 206 (67.3) 55 (18.0) | 0.348 |
| STS Score | 3.7 (1.8–6.7) | 3.2 (1.6–6.4) | 3.6 (2.1–6.8) | 0.135 |
| Active Endocarditis | 4 (0.7) | 1 (0.4) | 3 (1.0) | 0.639 |
| TAPSE | 14.9 ± 6.7 | 15.6 ± 5.5 | 14.4 ± 7.3 | 0.109 |
| Dyslipidemia | 305 (57.0) | 131 (57.2) | 174 (56.9) | 0.937 |
| Critical Preoperative Status | 28 (5.2) | 16 (7.0) | 12 (3.9) | 0.115 |
| Extracardiac Arteriopathy | 73 (13.6) | 32 (14.0) | 41 (13.4) | 0.848 |
| Unstable Angina | 16 (3.0) | 7 (3.1) | 9 (2.9) | 0.938 |
| Permanent Atrial Fibrilation | 313 (58.5) | 123 (53.7) | 190 (62.1) | 0.052 |
| Urgent Cardiac Surgery | 49 (9.2) | 19 (8.3) | 30 (9.8) | 0.550 |
| Smoker | 154 (28.8) | 59 (25.8) | 95 (31.0) | 0.182 |
| COPD | 111 (20.7) | 45 (19.7) | 66 (21.6) | 0.588 |
| Recent Myocardial Infarction | 41 (7.7) | 17 (7.4) | 24 (7.8) | 0.857 |
| Permanent Pacemaker | 74 (13.8) | 32 (14.0) | 42 (13.7) | 0.934 |
| Stroke | 58 (10.8) | 26 (11.4) | 32 (10.5) | 0.741 |
| Percutaneous revacularization | 210 (39.3) | 85 (37.1) | 125 (40.8) | 0.382 |
| CABG | 88 (16.4) | 23 (10.0) | 65 (21.2) | 0.001 |
| Cardiac Resyncronization | 83 (15.5) | 51 (22.3) | 32 (10.5) | <0.001 |
| Autoimplantable cardiodefibrilator | 178 (33.3) | 109 (47.6) | 69 (22.5) | <0.001 |
| Prior TAVI | 13 (2.4) | 7 (3.1) | 6 (2.0) | 0.415 |
| Poor Morbility | 52 (9.7) | 23 (10.0) | 29 (9.5) | 0.827 |
| Previous Heart Transplantation | 29 (5.4) | 14 (6.1) | 15 (4.9) | 0.540 |
| Prior Mitral Annuloplasty | 10 (1.9) | 3 (1.3) | 7 (2.3) | 0.528 |
| Aortic Surgery | 15 (2.8) | 3 (1.2) | 12 (3.9) | 0.070 |
| Technical Procedural Success | 502 (93.8) | 214 (93.4) | 288 (94.1) | 0.751 |
| Matched Group n = 288 | FE < 30% (Group 1) n = 144 | FE ≥ 30% (Group 2) n = 144 | p | |
|---|---|---|---|---|
| Age (years) | 71.5 ± 9.8 | 71.3 ± 10.5 | 71.8 ± 9.1 | 0.676 |
| Sex (n (%)) Men Women | 228 (79.2) 60 (20.8) | 114 (79.2) 30 (20.8) | 114 (79.2) 30 (20.8) | - |
| BSA (m2) | 1.75 ± 0.36 | 1.79 ± 0.19 | 1.71 ± 0.48 | 0.140 |
| BMI (kg/m2) | 26.5 ± 4.2 | 26.4 ± 4.0 | 26.6 ± 4.3 | 0.736 |
| BMI ≥ 30 kg/m2 | 54 (18.8) | 27 (18.8) | 27 (18.8) | - |
| LVEF, % | 32.9 ± 11.8 | 24.2 ± 5.9 | 41.6 ± 9.6 | - |
| Type 2 Diabetes Mellitus | 96 (33.3) | 48 (33.3) | 48 (33.3) | - |
| Ischemic Heart Disease | 186 (64.6) | 93 (64.6) | 93 (64.6) | - |
| Hypertension | 204 (70.8) | 102 (70.8) | 102 (70.8) | - |
| Previous Cardiac Surgery | 53 (18.4) | 25 (17.4) | 28 (19.4) | 0.648 |
| Hemodyalisis | 7 (2.4) | 2 (1.4) | 5 (3.5) | 0.447 |
| Creatinine (mg/dL) | 1.39 ± 0.61 | 1.38 ± 0.49 | 1.41 ± 0.71 | 0.643 |
| eGFR (mL/min) | 65.1 ± 29.0 | 63.0 ± 24.8 | 67.1 ± 32.6 | 0.433 |
| NYHA Class I II III IV | 5 (1.7) 28 (9.7) 190 (66.0) 65 (22.6) | 1 (0.7) 11 (7.6) 93 (64.6) 39 (27.1) | 4 (2.8) 17 (11.8) 97 (67.4) 26 (18.1) | 0.115 |
| STS Score | 3.9 (1.3–6.8) | 3.7 (1.9–7.2) | 3.5 (1.5–6.5) | 0.511 |
| Active Endocarditis | 1 (0.3) | 0 | 1 (0.7) | 1 |
| TAPSE | 14.7 ± 6.8 | 15.1 ± 6.3 | 14.8 ± 7.7 | 0.274 |
| Dyslipidemia | 169 (58.7) | 88 (61.1) | 81 (56.3) | 0.402 |
| Critical Preoperative Status | 13 (4.5) | 8 (5.6) | 5 (3.5) | 0.394 |
| Extracardiac Arteriopathy | 46 (16.0) | 21 (14.6) | 25 (17.4) | 0.520 |
| Unstable Angina | 10 (3.5) | 5 (3.5) | 5 (3.5) | 1 |
| Permanent Atrial Fibrilation | 163 (56.6) | 80 (55.6) | 83 (57.6) | 0.721 |
| Urgent Cardiac Surgery | 22 (7.6) | 9 (6.3) | 13 (9.0) | 0.375 |
| Smoker | 83 (28.8) | 43 (29.9) | 40 (27.8) | 0.696 |
| Chronic obstructive pulmonary disease | 56 (19.4) | 29 (20.1) | 27 (18.8) | 0.766 |
| Recent Myocardial Infarction | 22 (7.6) | 10 (6.9) | 12 (8.3) | 0.825 |
| Permanent Pacemaker | 44 (15.3) | 22 (15.3) | 22 (15.3) | 1 |
| Stroke | 34 (11.8) | 18 (12.5) | 16 (11.1) | 0.715 |
| Percutaneous revacularization | 129 (44.8) | 67 (46.5) | 62 (43.1) | 0.554 |
| CABG | 54 (18.8) | 20 (13.9) | 34 (23.6) | 0.035 |
| Cardiac Resyncronization | 42 (14.6) | 26 (18.1) | 16 (11.1) | 0.095 |
| Autoimplantable Cardiodefibrilator | 91 (31.6) | 61 (42.4) | 30 (20.8) | <0.001 |
| Prior TAVI | 8 (2.8) | 6 (4.2) | 2 (1.4) | 0.282 |
| Poor Morbility | 26 (9.0) | 13 (9.0) | 13 (9.0) | 1 |
| Previous Heart Transplantation | 14 (4.9) | 7 (4.9) | 7 (4.9) | 1 |
| Prior Mitral annuloplasty | 4 (1.4) | 2 (1.4) | 2 (1.4) | 1 |
| Surgery Aorta | 7 (2.4) | 2 (1.4) | 5 (3.5) | 0.447 |
| Technical Procedural Success | 271 (94.1) | 135 (93.8) | 136 (94.4) | 0.803 |
| Matched Group n = 288 | FE < 30% (Group 1) n = 144 | FE ≥ 30% (Group 2) n = 144 | p | |
|---|---|---|---|---|
| Procedural success, n (%) | 271 (94.1) | 135(93.8) | 136 (94.4) | 0.803 |
| Number of clips implanted, n | 1.49 ± 0.64 | 1.48 ± 0.64 | 1.50 ± 0.64 | 0.744 |
| Procedural duration, min | 140 (115–180) | 141 (118–192) | 136 (105–179) | 0.413 |
| Implantation time, min | 80 (60–107) | 82 (59–108) | 70 (60–108) | 0.677 |
| Degree of mitral regurgitation post clip, n (%) 0 I II III IV | 17 (5.9) 176 (61.1) 81 (28.1) 8 (2.8) 6 (2,1) | 9 (6.3) 86 (59.7) 41 (28.5) 5 (3.5) 3 (2.1) | 8 (5.6) 90 (62.5) 40 (27.8) 3 (2.1) 3 (2.1) | 0.955 |
| Transmitral gradient after the clip, mmHg | 3.05 ± 1.68 | 3.06 ± 1.49 | 3.04 ± 1.84 | 0.923 |
| Clip detachment (partial or complete), | 8 (2.8) | 5 (3.5) | 3 (2.1) | 0.723 |
| Catheter thrombosis, n (%) | 2 (0.7) | 1 (0.7) | 1 (0.7) | 1 |
| Subvalvular chordal rupture n (%) | 3 (1.0) | 1 (0.7) | 2 (1.4) | 0.999 |
| Clip entanglement in subvalvular apparatus, n (%) | 0 | 0 | 0 | - |
| Puncture site hematoma, n (%) | 10 (3.5) | 5 (3.5) | 5 (3.5) | 1 |
| Arteriovenous fistula, n (%) | 3 (1.0) | 2 (1.4) | 1 (0.7) | 0.999 |
| Valvular surgery, n (%) | 1 (0.3) | 0 | 1 (0.7) | 0.999 |
| Hemorrhage (BARC criteria) 0 1 2 3a 3b | 250 (86.8) 32 (11.1) 2 (0.7) 1 (0.3) 3 (1.0) | 133 (92.4) 9 (6.3) 1 (0.7) 0 1 (0.7) | 117 (81.3) 23 (16.0) 1 (0.7) 1 (0.7) 2 (1.4) | 0.590 |
| Pericardial leak | 5 (1.7) | 3 (2.1) | 2 (1.4) | 0.685 |
| Urgent indication, n (%) | 19 (6.6) | 10 (6.9) | 9 (6.3) | 0.812 |
| Matched Group n = 288 | FE < 30% (Group 1) n = 144 | FE ≥ 30% (Group 2) n = 144 | p | |
|---|---|---|---|---|
| Deaths | 35 (12.2) | 25 (17.4) | 10 (6.9) | 0.007 |
| Cardiac death | 27 (9.4) | 20 (13.9) | 7 (4.9) | 0.009 |
| Arrhythmic death | 4 (1.4) | 3 (2.1) | 1 (0.7) | 0.622 |
| Non cardiac death | 8 (2.8) | 5 (3.5) | 3 (2.1) | 0.723 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascual, I.; Carrasco-Chinchilla, F.; Benito-Gonzalez, T.; Li, C.H.; Avanzas, P.; Nombela-Franco, L.; Pan, M.; Serrador Frutos, A.; Freixa, X.; Trillo-Nouche, R.; et al. Transcatheter Mitral Repair for Functional Mitral Regurgitation According to Left Ventricular Function: A Real-Life Propensity-Score Matched Study. J. Clin. Med. 2020, 9, 1792. https://doi.org/10.3390/jcm9061792
Pascual I, Carrasco-Chinchilla F, Benito-Gonzalez T, Li CH, Avanzas P, Nombela-Franco L, Pan M, Serrador Frutos A, Freixa X, Trillo-Nouche R, et al. Transcatheter Mitral Repair for Functional Mitral Regurgitation According to Left Ventricular Function: A Real-Life Propensity-Score Matched Study. Journal of Clinical Medicine. 2020; 9(6):1792. https://doi.org/10.3390/jcm9061792
Chicago/Turabian StylePascual, Isaac, Fernando Carrasco-Chinchilla, Tomas Benito-Gonzalez, Chi Hion Li, Pablo Avanzas, Luis Nombela-Franco, Manuel Pan, Ana Serrador Frutos, Xavier Freixa, Ramiro Trillo-Nouche, and et al. 2020. "Transcatheter Mitral Repair for Functional Mitral Regurgitation According to Left Ventricular Function: A Real-Life Propensity-Score Matched Study" Journal of Clinical Medicine 9, no. 6: 1792. https://doi.org/10.3390/jcm9061792