Abnormalities on Perfusion CT and Intervention for Intracranial Hypertension in Severe Traumatic Brain Injury

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chesnut, R.; Temkin, N.; Carney, N.; Dikmen, S.; Rondina, C.; Videtta, W.; Petroni, G.; Lujan, S.; Pridgeon, J.; Barber, J.; et al. A trial of intracranial-pressure monitoring in traumatic brain injury. N. Engl. J. Med. 2012, 367, 2471–2481. [Google Scholar] [CrossRef] [Green Version]
- Forsyth, R.J.; Raper, J.; Todhunter, E. Routine intracranial pressure monitoring in acute coma. Cochrane Database Syst. Rev. 2015, 11, CD002043. [Google Scholar] [CrossRef]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.J.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the management of severe traumatic brain injury. Neurosurgery 2017, 80, 9. [Google Scholar] [CrossRef]
- Wintermark, M.; Sincic, R.; Sridhar, D.; Chien, J.D. Cerebral perfusion CT: Technique and clinical applicaitons. J. Neuroradiol. 2008, 35, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Bivard, A.; Spratt, N.; Levi, C.; Parsons, M. Perfusion computer tomography: Imaging and clinical validation in acute ischaemic stroke. Brain 2011, 134, 3408–3416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wintermark, M.; Fischbein, N.J.; Smith, W.S.; Ko, N.U.; Quist, M.; Dillon, W.P. Accuracy of dynamic perfusion CT with deconvolution in detecting acute hemispheric stroke. Am. J. Neuroradiol. 2005, 26, 104–112. [Google Scholar]
- Furtado, A.D.; Lau, B.C.; Vittinghoff, E.; Dillon, W.P.; Smith, W.S.; Rigby, T.; Boussel, L.; Wintermark, M. Optimal brain perfusion CT coverage in patients with acute middle cerebral artery stroke. Am. J. Neuroradiol. 2010, 31, 691–695. [Google Scholar] [CrossRef] [Green Version]
- Dorn, F.; Muenzel, D.; Meier, R.; Poppert, H.; Rummeny, E.J.; Huber, A. Brain perfusion CT for acute stroke using 256-slice CT: Improvement in diagnostic information by large volume coverage. Eur. Radiol. 2011, 21, 1803–1810. [Google Scholar] [CrossRef]
- Honda, M.; Ichibayashi, R.; Suzuki, G.; Yokomuro, H.; Seiki, Y.; Sase, S.; Kishi, T. Consideration of the intracranial pressure threshold value for the initiation of traumatic brain injury treatment: A Xenon CT and perfusion CT study. Neurocritical Care 2017, 27, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Wintermark, M.; Chiolero, R.; van Melle, G.; Revelly, J.P.; Porchet, F.; Regali, L.; Meuli, R.; Schnyder, P.; Maeder, P. Relationship between brain perfusion computed tomography variables and cerebral perfusion pressure in severe head trauma patients. Crit. Care Med. 2004, 32, 1579–1587. [Google Scholar] [CrossRef]
- Wintermark, M.; Chiolero, R.; Melle, G.V.; Revelly, J.P.; Porchet, F.; Regli, L.; Maeder, P.; Meuli, R.; Schnyder, P. Cerebral vascular autoregulation assessed by perfusion-CT in severe head trauma patients. J. Neuroradiol. 2006, 33, 27–37. [Google Scholar] [CrossRef]
- Honda, M.; Ichibayashi, R.; Yokomuro, H.; Yoshihara, K.; Masuda, H.; Haga, D.; Seiki, Y.; Kudoh, C.; Kishi, T. Early cerebral circulation disturbance in patients suffering from severe traumatic brain injury: A Xenon CT and perfusion CT study. Neurol. Med. Chir. 2016, 56, 501–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trofimov, A.O.; Kalentiev, G.; Voennov, O.; Grigoryeva, V. Comparison of Cerebral Oxygen Saturation and Cerebral Perfusion Computed Tomography in Cerebral Blood Flow in Patients with Brain Injury. In Oxygen Transport to Tissue XXXVII; Elwell, C.E., Leung, T.S., Harrison, D.K., Eds.; Springer: New York, NY, USA, 2016; pp. 145–149. [Google Scholar]
- Amorim, R.L.; Bor-Seng-Shu, E.; Gattas, G.S.; Paiva, W.; Ferreira de Andrade, A.; Teixeira, M.J. Decompressive craniectomy and cerebral blood flow regulation in head injured patients: A case studied by perfusion CT. J. Neuroradiol. 2012, 39, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Dong, J.; Xia, T.; Zhang, C.; Zhao, W.; Xu, Q.; Cai, X. Changes in cerebral haemodynamics in patients with posttraumatic diffuse brain swelling after external intraventricular drainage. Chin. J. Traumatol. 2015, 18, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.; Lou, H.; Xu, J.; Wang, H.; Huang, X.; Gong, J.; Xiong, B.; Yang, X. The impact of cranioplasty on cerebral blood perfusion in patients treated with decompressive craniectomy for severe traumatic brain injury. Brain Inj. 2015, 29, 1654–1660. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Dai, F.; Li, G.; Dong, J.; Wang, Y. Using computerized tomography perfusion to measure cerebral haemodynamics following treatment of traumatic brain injury in rabbits. Exp. Ther. Med. 2019, 18, 2104–2110. [Google Scholar]
- Wintermark, M.; van Melle, G.; Schnyder, P.; Revelly, J.-P.; Porchet, F.; Regli, L.; Meuli, R.; Maeder, P.; Chioléro, R. Admission perfusion CT: Prognostic value in patients with severe head trauma. Radiology 2004, 232, 211–220. [Google Scholar] [CrossRef]
- Metting, Z.; Rodiger, L.A.; De Jong, B.M.; Stewart, R.E.; Kremer, B.P.; van der Naalt, J. Acute cerebral perfusion CT abnormalities associated with posttraumatic amnesia in mild head injury. J. Neurotrauma 2010, 27, 2183–2189. [Google Scholar] [CrossRef]
- Metting, Z.; Rodiger, L.A.; Stewart, R.E.; Oudkerk, M.; Keyser, J.D.; van der Naalt, J. Perfusion computed tomography in the acute phase of mild head injury: Regional dysfunction and prognostic value. Ann. Neurol. 2009, 66, 809–816. [Google Scholar] [CrossRef]
- Metting, Z.; Spikman, J.M.; Rodiger, L.A.; van der Naalt, J. Cerebral perfusion and neuropsychological follow up in mild traumatic brain injury: Acute versus chronic disturbances? Brain Cogn. 2014, 86, 24–31. [Google Scholar] [CrossRef]
- Bendinelli, C.; Cooper, S.; Evans, T.; Bivard, A.; Pacey, D.; Parsons, M.; Balogh, Z.J. Perfusion abnormalities are frequently detected by early CT perfusion and predict unfavourable outcome following severe traumatic brain injury. World J. Surg. 2017, 41, 2512–2520. [Google Scholar] [CrossRef] [PubMed]
- Bendinelli, C.; Bivard, A.; Nebauer, S.; Parsons, M.W.; Balogh, Z.J. Brain CT perfusion provides additional useful information in severe traumatic brain injury. Inj. Int. J. Care Inj. 2013, 44, 1208–1212. [Google Scholar] [CrossRef] [PubMed]
- Bindu, T.S.; Vyas, S.; Khandelwal, N.; Bhatia, V.; Dhandapani, S.; Kumar, A.; Ahuja, C.K. Role of whole-brain computed tomography perfusion in head injury patients to predict outcome. Indian J. Radiol. Imaging 2017, 27, 268–273. [Google Scholar] [PubMed]
- Patchana, T.; Dorkoski, R.; Zampella, B.; Wiginton, J.G., IV; Sweiss, R.B.; Menoni, R.; Miulli, D.E. The use of computed tomography perfusion on admission to predict outcomes in surgical and nonsurgical traumatic brain injury patients. Cureus 2019, 11, e5007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, J.J.S.; Green, R.; Virani, K.; Wong, H.; Eddy, K.; Vandorpe, R. Admission perfusion CT for classifying early in-hospital mortality of patients with severe traumatic brain injury: A pilot study. Am. J. Roentgenol. 2020, 214, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Brain Trauma Foundation AAoNS; Congress of Neurological Surgeons. Guidelines for the management of severe traumatic brain injury 3rd edition. J. Neurotrauma 2007, 24 (Suppl. S1), 1–106. [Google Scholar]
- Stocchetti, N.; Zanaboni, C.; Colombo, A.; Citerio, G.; Beretta, L.; Ghisoni, L.; Zanier, E.R.; Canavesi, K. Refractory intracranial hypertension and “second tier” therapies in traumatic brain injury. Intensive Care Med. 2008, 34, 461–467. [Google Scholar] [CrossRef]
- Maas, A.I.; Hukkelhoven, C.W.; Marshall, L.F.; Steyerberg, E.W. Prediction of outcome in traumatic brain injury with computed tomographic characteristics: A comparison between the computed tomographic classification and combinations of computed tomographic predictors. Neurosurgery 2005, 57, 1173–1182. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.T.L.; Pettigrew, L.E.L.; Teasdale, G.M. Structured interviews for the Glasgow Outcome Scale and the extended Glasgow Outcome Scale: Guidelines for their use. J. Neurotrauma 1998, 15, 573–585. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Number of Patients | 28 |
|---|---|
| Age (Years): Median (IQR) | 33 (22–53) |
| Male: n (%) | 23 (82%) |
| Clinical Variables | |
| EVD: n (%) | 16 (57%) |
| Pre-Intubation GCS: Median (IQR) | 5 (3–7) |
| ISS: Mean (SD) | 31 (8.2) |
| HNAIS: Median (IQR) | 5 (4–5) |
| Lactate: Median (IQR) | 3 (2–4) |
| BD: Median (IQR) | 3 (2–5) |
| Rotterdam: Median (IQR) | 2 (2–3) |
| Outcome Variables | |
| ICU Days: Mean (SD) | 13 (5.4) |
| Mortality: n (%) | 5 (18%) |
| Favourable GOSE at 6 Months: n (%) | 9 (32%) |
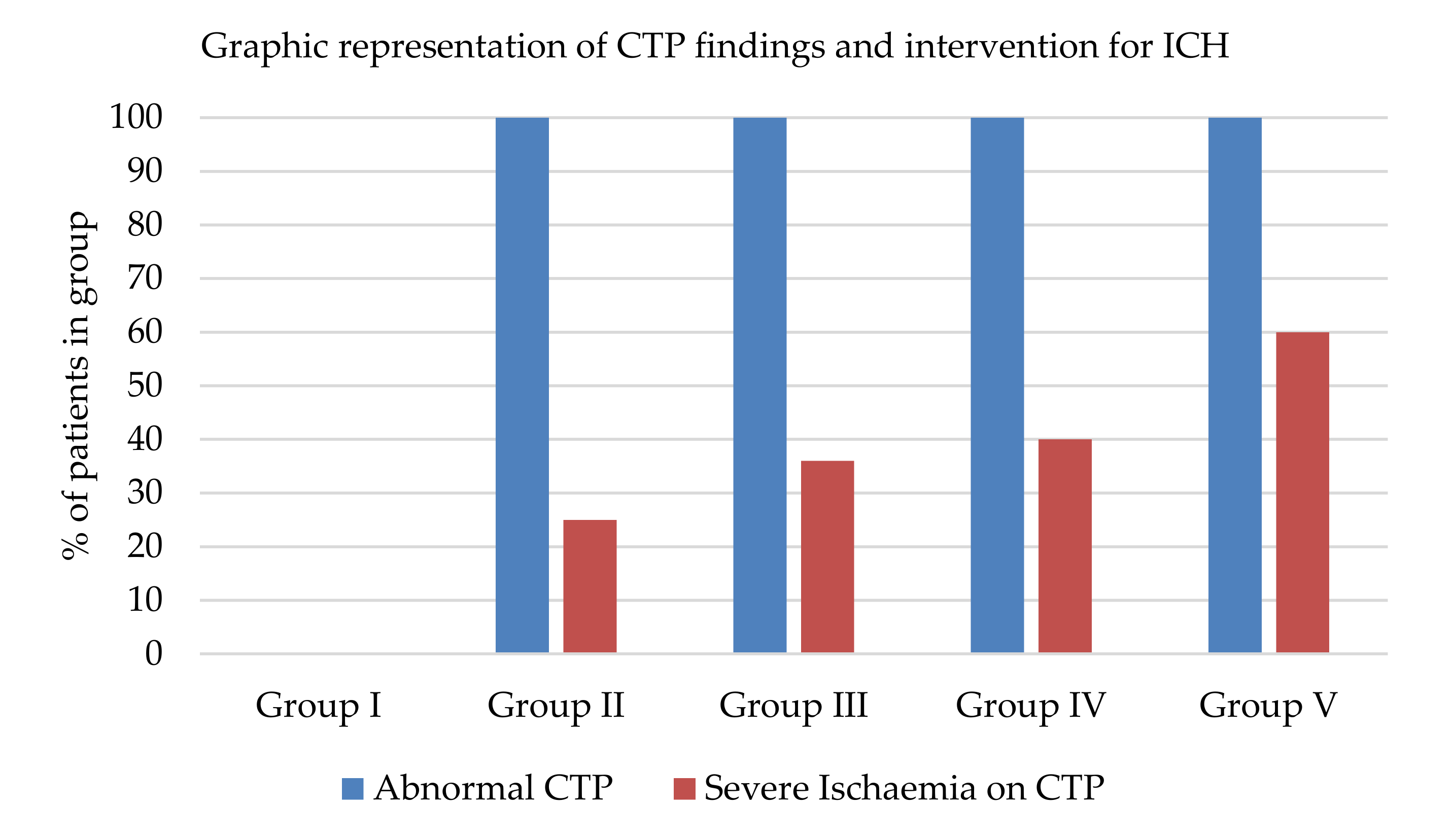
| Group I | Group II | Group III | Group IV | Group V | p-Value | |
|---|---|---|---|---|---|---|
| Number of Patients: n (%) | 2 (7%) | 5 (18%) | 11 (39%) | 5 (18%) | 5 (18%) | |
| Age: Median (IQR) | 23(19–23) | 35 (23–57) | 33 (20–48) | 27 (23–57) | 46 (29–60) | N.S. b |
| Male: n (%) | 2 (100%) | 4 (80%) | 8 (73%) | 4 (80%) | 5 (100%) | N.S. a |
| Clinical Variables | ||||||
| EVD: n (%) | 0 (0%) | 3 (60%) | 5 (46%) | 4 (80%) | 4 (80%) | N.S. a |
| GCS: Median (IQR) | 5 (3–5) | 4 (4–7) | 5 (3–6) | 5 (3–7) | 5 (3–9) | N.S. a |
| ISS: Mean (SD) | 27 (3.5) | 34 (8.8) | 31 (9.8) | 33 (4.8) | 27 (7.8) | N.S. c |
| HNAIS: Median (IQR) | 5 (4–5) | 4 (4–5) | 5 (4–5) | 5 (4–5) | 5 (3–6) | N.S. b |
| Lactate: Median (IQR) | 3 (2–3) | 3 (2–7) | 3(2–4) | 3 (2–4) | 3 (2–4) | N.S. b |
| BD: Median (IQR) | 5 (5–6) | 2 (4–6) | 4 (2–7) | 3 (1–3) | 4 (1–2) | N.S. b |
| Rotterdam: Median (IQR) | 2 (1–2) | 2 (2–3) | 2 (2–3) | 2 (2–2) | 4 (3–4) | 0.046 b |
| Outcome Variables | ||||||
| ICU Days: Mean (SD) | 8 (2.1) | 14 (4.8) | 10 (4.9) | 16 (5.9) | 18 (1.8) | 0.03 c |
| Mortality: n (%) | 0 (0%) | 1 (20%) | 2 (18%) | 1 (20%) | 1 (20%) | N.S. a |
| Favourable GOSE: n (%) | 2 (100%) | 1 (20%) | 3 (27%) | 2 (40%) | 1 (20%) | N.S. b |
| CTP Results | ||||||
| Abnormal: n (%) | 0 (0%) | 5 (100%) | 11 (100%) | 5 (100%) | 5 (100%) | 0.003 a |
| Severe Ischaemia: n (%) | 0 (0%) | 1 (25%) | 4 (36%) | 2 (40%) | 3 (60%) | N.S. a |
| No Intervention | Intervention | p-Value | |
|---|---|---|---|
| Number of Patients: n (%) | 2 (7%) | 26 (93%) | |
| Age: Median (IQR) | 23 (NA) | 33 (18–49) | N.S. c |
| Male: n (%) | 2 (100%) | 21 (81%) | N.S. a |
| Clinical Variables | |||
| EVD: n (%) | 0 (0%) | 16 (62%) | N.S. a |
| Pre-Intubation GCS: Median (IQR) | 5 (NA) | 5 (3–7) | N.S. a |
| ISS: Mean (SD) | 27 (3.5) | 31 (8.1) | N.S. c |
| HNAIS: Median (IQR) | 4.5 (NA) | 5 (4–6) | N.S. b |
| Lactate: Median (IQR) | 2.6 (NA) | 2.8 (2.0–3.6) | N.S. b |
| BD: Median (IQR) | 5 (NA) | 2.3 (0.6–4.2) | N.S. b |
| Rotterdam: Median (IQR) | 2 (NA) | 2 (1–3) | N.S. b |
| Outcome Variables | |||
| ICU Days: Mean (SD) | 8 (2.1) | 13 (5.3) | N.S. c |
| Mortality: n (%) | 0 (0%) | 5 (19%) | N.S. a |
| Favourable Outcome: n (%) | 2 (100%) | 7 (27%) | N.S. a |
| CTP Findings | |||
| Abnormal: n (%) | 0 (0%) | 26 (100%) | 0.003. a |
| Severe Ischaemia: n (%) | 0 (0%) | 10 (38%) | N.S. a |
| No Second-Tier Intervention | Second-Tier Intervention | p-Value | |
|---|---|---|---|
| Number of Patients: n (%) | 18 (64%) | 10 (36%) | |
| Age: Median (IQR) | 30 (22–49) | 45 (25–57) | N.S. b |
| Male: n (%) | 14 (78%) | 9 (90%) | N.S. a |
| Clinical Variables | |||
| EVD: n (%) | 8 (44%) | 8 (80%) | N.S. a |
| Pre-Intubation GCS: Median (IQR) | 5 (3–6) | 5 (3–7) | N.S. a |
| ISS: Mean (SD) | 31 (9.0) | 30 (6.8) | N.S. c |
| HNAIS: Median (IQR) | 5 (4–5) | 5 (4–5) | N.S. b |
| Lactate: Median (IQR) | 3 (2–4) | 2.9 (2–4) | N.S. b |
| BD: Median (IQR) | 4 (1–6) | 3 (1–3) | N.S. b |
| Rotterdam: Median (IQR) | 2 (1–2) | 2 (2–2) | N.S. b |
| Outcome Variables | |||
| ICU Days: Mean (SD) | 11 (4.9) | 17 (4.5) | 0.007 c |
| Mortality: n (%) | 3 (17%) | 2 (20%) | N.S. a |
| Favourable Outcome: n (%) | 6 (64%) | 3 (30%) | N.S. a |
| CTP Findings | |||
| Abnormal: n (%) | 16 (89%) | 10 (100%) | N.S. a |
| Severe Ischaemia: n (%) | 5 (29%) | 5 (50%) | N.S. a |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cooper, S.; Bendinelli, C.; Bivard, A.; Parsons, M.; Balogh, Z.J. Abnormalities on Perfusion CT and Intervention for Intracranial Hypertension in Severe Traumatic Brain Injury. J. Clin. Med. 2020, 9, 2000. https://doi.org/10.3390/jcm9062000
Cooper S, Bendinelli C, Bivard A, Parsons M, Balogh ZJ. Abnormalities on Perfusion CT and Intervention for Intracranial Hypertension in Severe Traumatic Brain Injury. Journal of Clinical Medicine. 2020; 9(6):2000. https://doi.org/10.3390/jcm9062000
Chicago/Turabian StyleCooper, Shannon, Cino Bendinelli, Andrew Bivard, Mark Parsons, and Zsolt J. Balogh. 2020. "Abnormalities on Perfusion CT and Intervention for Intracranial Hypertension in Severe Traumatic Brain Injury" Journal of Clinical Medicine 9, no. 6: 2000. https://doi.org/10.3390/jcm9062000