The Frequency of, and Factors Associated with Prolonged Hospitalization: A Multicentre Study in Victoria, Australia


Abstract
:1. Introduction
2. Methods
2.1. Ethics Approval
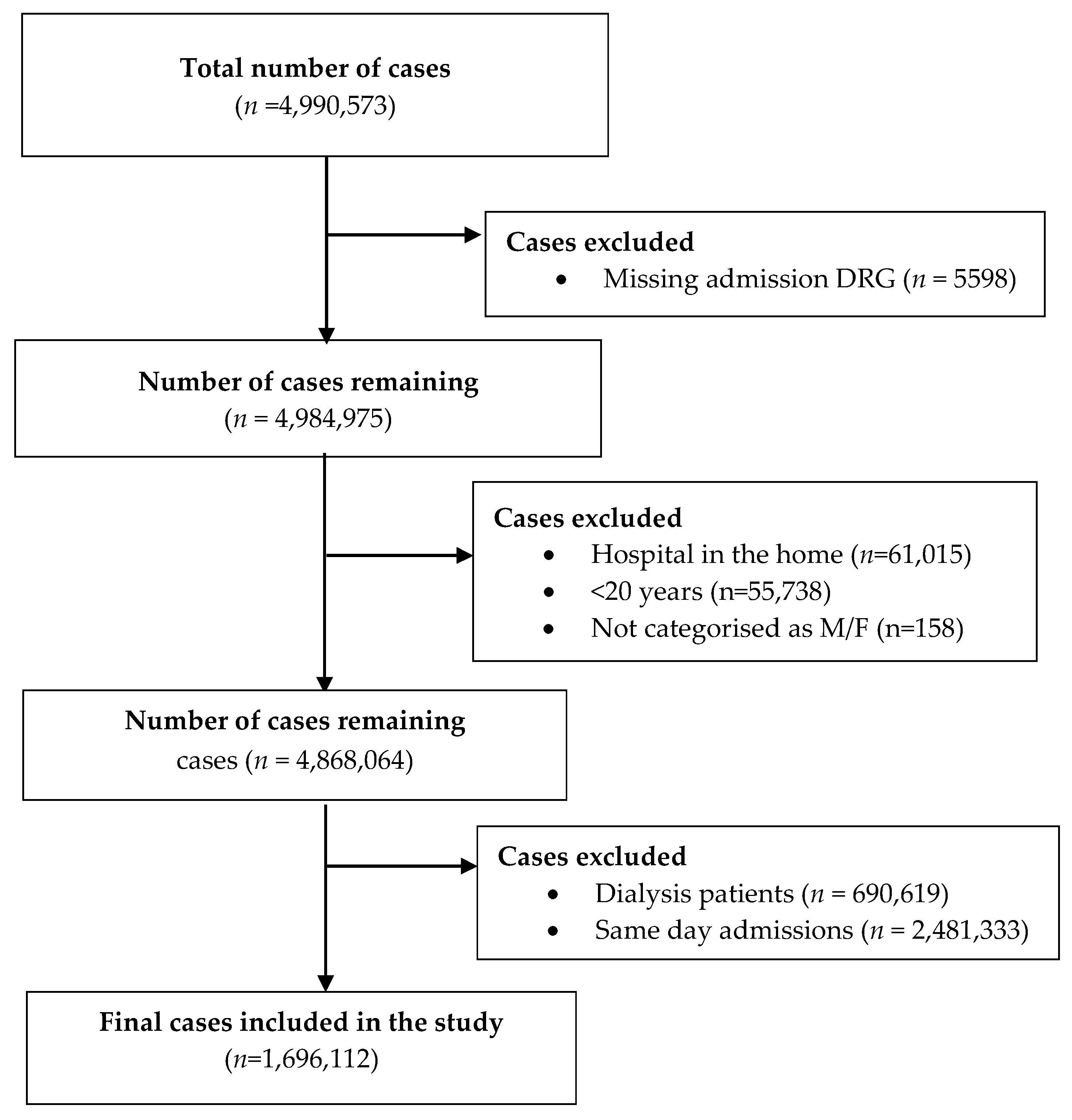
2.2. Study Design and Participants
2.3. Data Sources and Variables Collected
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Details of Study Cohort
3.2. Frequency of Prolonged Hospitalization and Details of Bed Utilisation
3.3. Factors Associated with Prolonged Hospitalization
3.4. Factors Associated with in-Hospital Mortality
3.5. Factors Associated with Hospital Discharge to Home
4. Discussion
4.1. Key Findings
4.2. Comparison with Previous Studies
4.3. Study Strengths and Limitations
4.4. Implications for Clinicians and Policy-Makers
4.5. Areas for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergeron, E.; Lavoie, A.; Moore, L.; Clas, D.; Rossignol, M. Comorbidity and age are both independent predictors of length of hospitalization in trauma patients. Can. J. Surg. 2005, 48, 361–366. [Google Scholar] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [Green Version]
- OECD. Health expenditure in hospitals. In Health at a Glance: Europe 2018; OECD Publishing: Paris, France; European Union: Brussels, Belgium, 2018; pp. 138–139. [Google Scholar] [CrossRef]
- McKee, M. Reducing Hospital Beds. What Are the Lessons to Be Learned? European Observatory Health Systems and Policies: Geneva, Switzerland, 2004; p. 6. [Google Scholar]
- Barisonzo, R.; Wiedermann, W.; Unterhuber, M.; Wiedermann, C.J. Length of stay as risk factor for inappropriate hospital days: Interaction with patient age and co-morbidity. J. Eval. Clin. Pract. 2013, 19, 80–85. [Google Scholar] [CrossRef]
- Celik, Y.; Celik, S.S.; Bulut, H.D.; Khan, M.; Kisa, A. Inappropriate use of hospital beds: A case study of university hospitals in Turkey. World Hosp. Health Serv. 2001, 37, 6–13, 33–34. [Google Scholar]
- Buttigieg, S.C.; Abela, L.; Pace, A. Variables affecting hospital length of stay: A scoping review. J. Health Organ. Manag. 2018, 32, 463–493. [Google Scholar] [CrossRef]
- Chakravarty, A.; Parmar, N.K.; Bhalwar, R. Inappropriate Use of Hospital Beds in a Tertiary Care Service Hospital. Med. J. Armed Forces India 2005, 61, 121–124. [Google Scholar] [CrossRef]
- Agrawal, S.; Chen, L.; Tergas, A.I.; Hou, J.Y.; St Clair, C.M.; Ananth, C.V.; Hershman, D.L.; Wright, J.D. Identifying modifiable and non-modifiable risk factors associated with prolonged length of stay after hysterectomy for uterine cancer. Gynecol. Oncol. 2018, 149, 545–553. [Google Scholar] [CrossRef]
- Agrawal, S.; Chen, L.; Tergas, A.I.; Hou, J.Y.; St Clair, C.M.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L.; Wright, J.D. Characteristics associated with prolonged length of stay after hysterectomy for benign gynecologic conditions. Am. J. Obstet. Gynecol. 2018, 219, 89.e1–89.e15. [Google Scholar] [CrossRef] [Green Version]
- Almogati, J.G.; Ahmed, E.O. Glycated Hemoglobin as a Predictor of the Length of Hospital Stay in Patients Following Coronary Bypass Graft Surgery in the Saudi Population. Braz. J. Cardiovasc. Surg. 2019, 34, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Bateni, S.B.; Bold, R.J.; Meyers, F.J.; Canter, D.J.; Canter, R.J. Comparison of common risk stratification indices to predict outcomes among stage IV cancer patients with bowel obstruction undergoing surgery. J. Surg. Oncol. 2018, 117, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Belkin, N.; Jackson, B.M.; Foley, P.J.; Damrauer, S.M.; Kalapatapu, V.; Golden, M.A.; Fairman, R.M.; Kelz, R.R.; Wang, G.J. Length of Stay after Thoracic Endovascular Aortic Repair Depends on Indication and Acuity. Ann. Vasc. Surg. 2019, 55, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.; Elliott, S.; Kaplan, J.; Lin, M.; Posselt, A.; Rogers, S. Predictors of hospital stay following laparoscopic gastric bypass: Analysis of 9593 patients from the National Surgical Quality Improvement Program. Surg. Obes. Relat. Dis. 2015, 11, 288–294. [Google Scholar] [CrossRef]
- Casillas-Berumen, S.; Rojas-Miguez, F.A.; Farber, A.; Komshian, S.; Kallish, J.A.; Rybin, D.; Goros, G.; Siracuse, J.J. Patient and Aneurysm Characteristics Predicting Prolonged Length of Stay after Elective Open AAA Repair in the Endovascular Era. Vasc. Endovascular. Surg. 2018, 52, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Coelho, R.F.; Cordeiro, M.D.; Padovani, G.P.; Localli, R.; Fonseca, L.; Junior, J.P.; Guglielmetti, G.B.; Sroughi, M.; Naha, W.C. Predictive factors for prolonged hospital stay after retropubic radical prostatectomy in a high-volume teaching center. Int. Braz. J. Urol. 2018, 44, 1089–1105. [Google Scholar] [CrossRef] [Green Version]
- Crisafulli, E.; Ielpo, A.; Barbeta, E.; Ceccato, A.; Huerta, A.; Gabarrus, A.; Soler, N.; Chetta, A.; Torres, A. Clinical variables predicting the risk of a hospital stay for longer than 7 days in patients with severe acute exacerbations of chronic obstructive pulmonary disease: A prospective study. Respir. Res. 2018, 19, 261. [Google Scholar] [CrossRef] [Green Version]
- Dasenbrock, H.H.; Liu, K.X.; Devine, C.A.; Chavakula, V.; Smith, T.R.; Gormley, W.B.; Dunn, I.F. Length of hospital stay after craniotomy for tumor: A National Surgical Quality Improvement Program analysis. Neurosurg. Focus 2015, 39, E12. [Google Scholar] [CrossRef] [Green Version]
- Dunn, J.C.; Lanzi, J.; Kusnezov, N.; Bader, J.; Waterman, B.R.; Belmont, P.J., Jr. Predictors of length of stay after elective total shoulder arthroplasty in the United States. J. Shoulder Elbow Surg. 2015, 24, 754–759. [Google Scholar] [CrossRef]
- Fletcher, R.; Deal, R.; Kubasiak, J.; Torquati, A.; Omotosho, P. Predictors of Increased Length of Hospital Stay Following Laparoscopic Sleeve Gastrectomy from the National Surgical Quality Improvement Program. J. Gastrointest. Surg. 2018, 22, 274–278. [Google Scholar] [CrossRef]
- Goltzman, G.; Perl, S.; Cohen, L.; Avivi, E.; Rapoport, M.J. Single Admission C-reactive protein Levels as a Sole Predictor of Patient Flow and Clinical Course in a General Internal Medicine Department. Isr. Med. Assoc. J. 2019, 21, 686–691. [Google Scholar] [PubMed]
- Inneh, I.A.; Iorio, R.; Slover, J.D.; Bosco, J.A., 3rd. Role of Sociodemographic, Co-morbid and Intraoperative Factors in Length of Stay Following Primary Total Hip Arthroplasty. J. Arthroplast. 2015, 30, 2092–2097. [Google Scholar] [CrossRef] [PubMed]
- Kaoutzanis, C.; Leichtle, S.W.; Mouawad, N.J.; Welch, K.B.; Lampman, R.M.; Wahl, W.L.; Cleary, R.K. Risk factors for postoperative wound infections and prolonged hospitalization after ventral/incisional hernia repair. Hernia 2015, 19, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Lakomkin, N.; Goz, V.; Lajam, C.M.; Iorio, R.; Bosco, J.A., 3rd. Higher Modified Charlson Index Scores Are Associated with Increased Incidence of Complications, Transfusion Events, and Length of Stay Following Revision Hip Arthroplasty. J. Arthroplast. 2017, 32, 1121–1124. [Google Scholar] [CrossRef] [PubMed]
- Lakomkin, N.; Zuckerman, S.L.; Stannard, B.; Montejo, J.; Sussman, E.S.; Virojanapa, J.; Kuzmik, G.; Goz, V.; Hadjipanayis, C.G.; Cheng, J.S. Preoperative Risk Stratification in Spine Tumor Surgery: A Comparison of the Modified Charlson Index, Frailty Index, and ASA Score. Spine 2019, 44, 782–787. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, S.H.; Tan, J.H.H.; Foo, H.S.L.; Phan, P.H.; Kow, A.W.; Lwin, S.; Seah, P.M.; Mordiffi, S.T. Factors associated with prolonged length of stay for elective hepatobiliary and neurosurgery patients: A retrospective medical record review. BMC Health Serv. Res. 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGirt, M.J.; Parker, S.L.; Chotai, S.; Pformiller, D.; Sorenson, J.M.; Foley, K.; Ashler, A.L. Predictors of extended length of stay, discharge to inpatient rehab, and hospital readmission following elective lumbar spine surgery: Introduction of the Carolina-Semmes Grading Scale. J. Neurosurg. Spine 2017, 27, 382–390. [Google Scholar] [CrossRef]
- Menendez, M.E.; Baker, D.K.; Fryberger, C.T.; Ponce, B.A. Predictors of extended length of stay after elective shoulder arthroplasty. J. Shoulder Elbow Surg. 2015, 24, 1527–1533. [Google Scholar] [CrossRef]
- Petis, S.M.; Howard, J.L.; Lanting, B.A.; Somerville, L.E.; Vasarhelyi, E.M. Perioperative Predictors of Length of Stay After Total Hip Arthroplasty. J. Arthroplast. 2016, 31, 1427–1430. [Google Scholar] [CrossRef]
- Quintana, J.M.; Unzurrunzaga, A.; Garcia-Gutierrez, S.; Gonzalez, N.; Lafuente, I.; Bare, M.; de Larrea, N.F.; Esteban, C. Predictors of Hospital Length of Stay in Patients with Exacerbations of COPD: A Cohort Study. J. Gen. Intern. Med. 2015, 30, 824–831. [Google Scholar] [CrossRef]
- Rana, A.; Witte, E.D.; Halazun, K.J.; Sood, G.K.; Mindikoglu, A.L.; Sussmann, N.L.; Vierling, J.M.; Kuet, M.L.; Galvan, N.T.; Cotton, R.T.; et al. Liver transplant length of stay (LOS) index: A novel predictive score for hospital length of stay following liver transplantation. Clin. Transplant. 2017, 31, e13141. [Google Scholar] [CrossRef] [PubMed]
- Thomas, W.W.; Brant, J.; Chen, J.; Coblens, O.; Fischer, J.P.; Newman, J.G.; Chalian, A.A.; Shanti, R.M.; Cannady, S.B. Clinical Factors Associated with Reoperation and Prolonged Length of Stay in Free Tissue Transfer to Oncologic Head and Neck Defects. JAMA Facial Plast. Surg. 2018, 20, 154–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsilimigras, D.I.; Hyer, J.M.; Moris, D.; Sahara, K.; Bagante, F.; Guglielmi, A.; Aldrighetti, A.; Alexandrescu, S.; Marques, H.P.; Shen, F.; et al. Prognostic utility of albumin-bilirubin grade for short- and long-term outcomes following hepatic resection for intrahepatic cholangiocarcinoma: A multi-institutional analysis of 706 patients. J. Surg. Oncol. 2019, 120, 206–213. [Google Scholar] [CrossRef]
- Velagapudi, P.; Kolte, D.; Ather, K.; Khera, S.; Gupta, T.; Gordon, P.C.; Aronow, H.D.; Kirtane, A.J.; Abott, J.D. Temporal Trends and Factors Associated with Prolonged Length of Stay in Patients With ST-Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. Am. J. Cardiol. 2018, 122, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.J.; Jackson, B.M.; Foley, P.J.; Dramrauer, S.M.; Kalapatapu, V.; Golden, M.A.; Fairman, R.M. Treating Peripheral Artery Disease in the Wake of Rising Costs and Protracted Length of Stay. Ann. Vasc. Surg. 2017, 44, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Wasfy, J.H.; Kennedy, K.F.; Masoudi, F.A.; Ferris, T.G.; Arnold, S.V.; Kini, V.; Peterson, P.; Curtis, J.P.; Amin, A.P.; Bradley, S.M.; et al. Predicting Length of Stay and the Need for Postacute Care After Acute Myocardial Infarction to Improve Healthcare Efficiency. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004635. [Google Scholar] [CrossRef]
- Winemaker, M.; Petruccelli, D.; Kabali, C.; de Beer, J. Not all total joint replacement patients are created equal: Preoperative factors and length of stay in hospital. Can. J. Surg. 2015, 58, 160–166. [Google Scholar] [CrossRef] [Green Version]
- Zhan, H.; Guo, R.; Xu, H.; Liu, X.; Yu, X.; Xu, Q.; Chen, H.; Dai, M.; Zhang, B. Hospital length of stay following first-time elective open posterior lumbar fusion in elderly patients: A retrospective analysis of the associated clinical factors. Medicine 2019, 98, e17740. [Google Scholar] [CrossRef]
- Lisk, R.; Uddin, M.; Parbhoo, A.; Yeong, K.; Fluck, D.; Sharma, P.; Lean, M.E.; Shan, T.S. Predictive model of length of stay in hospital among older patients. Aging Clin. Exp. Res. 2019, 31, 993–999. [Google Scholar] [CrossRef] [Green Version]
- Marfil-Garza, B.A.; Belaunzaran-Zamudio, P.F.; Gulias-Herrero, A.; Zuniga, A.C.; Caro-Vega, Y.; Kershenobich-Stalnikowitz, D.; Sifuentes-Osornio, J. Risk factors associated with prolonged hospital length-of-stay: 18-year retrospective study of hospitalizations in a tertiary healthcare center in Mexico. PLoS ONE 2018, 13, e0207203. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, A.T.; Nguyen, T.X.; Nguyen, T.N.; Nguyen, T.H.; Pham, T.; Cumming, R.; Hilmer, S.N.; Vu, H.T. The impact of frailty on prolonged hospitalization and mortality in elderly inpatients in Vietnam: A comparison between the frailty phenotype and the Reported Edmonton Frail Scale. Clin. Interv. Aging 2019, 14, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Sullivan, K.; Martensson, J.; Robbins, R.; Farley, K.J.; Johnson, D.; Jones, D. Epidemiology of long-stay patients in a university teaching hospital. Intern. Med. J. 2017, 47, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.E.; Glasheen, J.J.; Anoff, D.; Pierce, R.; Capp, R.; Jones, C.D. Understanding predictors of prolonged hospitalizations among general medicine patients: A guide and preliminary analysis. J. Hosp. Med. 2015, 10, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Services VSGHaH. Victorian Admitted Episodes Dataset Manual 2019–2020. 2019. Available online: https://www2.health.vic.gov.au/about/publications/policiesandguidelines/Victorian-Admitted-Episodes-Dataset-manual-2019-2020 (accessed on 11 January 2020).
- Services VSGHaH. Victorian Emergency Minimum Dataset (VEMD). 2019. Available online: https://www2.health.vic.gov.au/hospitals-and-health-services/data-reporting/health-data-standards-systems/data-collections/vemd (accessed on 13 January 2020).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- World Health Organization. Proposed Working Definition of an Older Person in Africa for the MDS Project. 2002. Available online: https://www.who.int/healthinfo/survey/ageingdefnolder/en/ (accessed on 11 January 2020).
- Crawford, T.C.; Magruder, J.T.; Grimm, J.C.; Suarez-Pierre, A.; Patel, N.; Sciortino, C.M.; Zehr, K.J.; Mandal, K.; Tedford, R.J.; Russell, S.D.; et al. A Comprehensive Risk Score to Predict Prolonged Hospital Length of Stay After Heart Transplantation. Ann. Thorac. Surg. 2018, 105, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barba, R.; Marco, J.; Canora, J.; Plaza, S.; Juncos, S.N.; Hinojosa, J.; Bailon, M.M.; Zapatero, A. Prolonged length of stay in hospitalized internal medicine patients. Eur. J. Intern. Med. 2015, 26, 772–775. [Google Scholar] [CrossRef]
- Agosti, P.; Tettamanti, M.; Vella, F.S.; Suppressa, P.; Pasina, L.; Franchi, C.; Nobili, A.; Mannucci, P.M.; Sabba, C. REPOSI Investigators. Living alone as an independent predictor of prolonged length of hospital stay and non-home discharge in older patients. Eur. J. Intern. Med. 2018, 57, 25–31. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Overall | Period | |
|---|---|---|---|
| 14 Nov. 2016–13 Nov. 2017 | 14 Nov. 2017–14 Nov. 2018 | ||
| Number of cases (n) | 1,696,112 | 834,045 | 862,067 |
| Female (n, %) | 877,020 (51.7) | 431,543 (51.7) | 445,477 (51.7) |
| Age groups, years. (n, %) | |||
| 20–24 | 61,465 (3.6) | 30,666 (3.7) | 30,799 (3.6) |
| 25–29 | 65,547 (3.9) | 32,465 (3.9) | 33,082 (3.8) |
| 30–34 | 72,766 (4.3) | 35,991 (4.3) | 36,775 (4.3) |
| 35–39 | 75,571 (4.5) | 37,261 (4.5) | 38,310 (4.4) |
| 40–44 | 82,135 (4.8) | 41,519 (5.0) | 40,616 (4.7) |
| 45–49 | 95,566 (5.6) | 47,104 (5.7) | 48,462 (5.6) |
| 50–54 | 103,747 (6.1) | 51,793 (6.2) | 51,954 (6.0) |
| 55–59 | 121,095 (7.1) | 59,470 (7.1) | 61,625 (7.2) |
| 60–64 | 137,130 (8.1) | 67,467 (8.1) | 69,663 (8.1) |
| 65–69 | 163,254 (9.6) | 81,217 (9.7) | 82,037 (9.5) |
| 70–74 | 170,359 (10.0) | 81,641 (9.8) | 88,718 (10.3) |
| 75–79 | 168,124 (9.9) | 82,130 (9.9) | 85,994 (10.0) |
| 80–84 | 158,335 (9.3) | 77,411 (9.3) | 80,924 (9.4) |
| ≥85 | 221,018 (13.0) | 107,910 (12.9) | 113,108 (13.1) |
| Indigenous population (n, %) | 13,888 (0.8) | 6604 (0.8) | 7284 (0.8) |
| Marital Status (n, %) | |||
| Never married | 325,672 (19.2) | 160,081 (19.2) | 165,591 (19.2) |
| Widowed | 244,190 (14.4) | 120,811 (14.5) | 123,379 (14.3) |
| Married or defacto | 955,280 (56.3) | 470,118 (56.4) | 485,162 (56.3) |
| Divorced or separated | 143,222 (8.4) | 69,762 (8.4) | 73,460 (8.5) |
| Other | 27,748 (1.6) | 13,273 (1.6) | 14,475 (1.7) |
| DRG type | |||
| Medical | 1,044,369 (61.6) | 508,577 (61.0) | 535,792 (62.2) |
| Surgical | 571,449 (33.7) | 285,911 (34.3) | 285,538 (33.1) |
| Other | 80,294 (4.7) | 39,557 (4.7) | 40,737 (4.7) |
| Emergency admission (n, %) | 839,360 (49.5) | 405,571 (48.6) | 433,789 (50.3) |
| Admission source (n, %) | |||
| Home | 1,442,065 (85.0) | 710,111 (85.1) | 731,954 (84.9) |
| Aged care residential facility | 11,302 (0.7) | 5234 (0.6) | 6068 (0.7) |
| From another hospital | 195,230 (11.5) | 95,892 (11.5) | 99,338 (11.5) |
| Other | 47,515 (2.8) | 22,808 (2.7) | 24,707 (2.9) |
| ICU stay (n, %) | 79,115 (4.7) | 39,187 (4.7) | 39,928 (4.6) |
| Admitted on weekend (n, %) | 573,292 (33.8) | 282,965 (33.9) | 290,327 (33.7) |
| Season of admission (n, %) | |||
| Spring (Sep-Nov) | 406,209 (24.0) | 204,835 (24.6) | 201,374 (23.4) |
| Summer (Dec-Feb) | 415,172 (24.5) | 203,530 (24.4) | 211,642 (24.6) |
| Autumn (Mar-May) | 433,328 (25.6) | 209,706 (25.1) | 223,622 (25.9) |
| Winter (Jun-Aug) | 441,403 (26.0) | 215,974 (25.9) | 225,429 (26.2) |
| Prior admissions in 12 months | |||
| 0 | 711,166 (41.9) | 411,233 (49.2) | 300,379 (34.8) |
| 1 | 374,576 (22.1) | 186,092 (22.3) | 188,760 (21.9) |
| ≥2 | 610,370 (36.0) | 238,009 (28.5) | 372,928 (43.3) |
| Risk category based on admission unit | |||
| 1 | 659,004 (38.9) | 324,467 (38.8) | 334,991 (38.9) |
| 2 | 503,703 (29.7) | 245,034 (29.3) | 259,133 (30.1) |
| 3 | 387,474 (22.8) | 192,039 (23.0) | 195,701 (22.7) |
| 4 | 145,931 (8.6) | 73,794 (8.8) | 72,242 (8.4) |
| In-hospital mortality (n, %) | 35,287 (2.1) | 17,535 (2.1) | 17,752 (2.1) |
| Length of stay (days), (n, %) | |||
| 1–6 | 1284,508 (75.7) | 629,370 (75.5) | 655,138 (76.0) |
| 7–13 | 248,154 (14.6) | 122,166 (14.7) | 125,988 (14.6) |
| 14–20 | 83,037 (4.9) | 41,317 (5.0) | 41,720 (4.8) |
| 21–27 | 35,457 (2.1) | 17,696 (2.1) | 17,761 (2.1) |
| ≥28 | 44,956 (2.7) | 23,496 (2.8) | 21,460 (2.5) |
| Days of Stay | Hospital Type | Number (%) Admissions * | Number (%) Bed Days |
|---|---|---|---|
| All length of stay | Overall | 1,696,112 (100) | 9,450,306 (100.0) |
| Private | 608,815 (35.9) | 327,285 (34.6) | |
| Regional | 207,938 (12.3) | 1,148,083 (12.1) | |
| Secondary | 382,490 (22.6) | 1,984,477 (21.0) | |
| Tertiary | 378,075 (22.3) | 1,962,871 (20.8) | |
| Other | 118,794 (7.0) | 1,082,050 (11.4) | |
| LOS1–6 days | Overall | 1,284,508 (75.7) | 2,988,383 (31.6) |
| Private | 450,324 (74.0) | 1,047,298 (32.0) | |
| Regional | 160,939 (77.4) | 386,284 (33.6) | |
| Secondary | 302,906 (79.2) | 690,189 (34.8) | |
| Tertiary | 294,359 (77.9) | 678,895 (34.6) | |
| Other | 75,980 (64.0) | 185,717 (17.2) | |
| LOS 7–13 days | Overall | 248,154 (14.6) | 2,285,159 (24.2) |
| Private | 102,152 (16.8) | 945,255 (28.9) | |
| Regional | 27,535 (13.2) | 251,200 (21.9) | |
| Secondary | 48,214 (12.6) | 441,094 (22.2) | |
| Tertiary | 51,832 (13.7) | 475,350 (24.2) | |
| Other | 18,421 (15.5) | 172,260 (15.9) | |
| LOS 14–20 days | Overall | 83,037 (4.9) | 1,354,911 (14.3) |
| Private | 32,485 (5.3) | 524,364 (16.0) | |
| Regional | 9446 (4.5) | 155,169 (13.5) | |
| Secondary | 15,066 (3.9) | 247,272 (12.5) | |
| Tertiary | 16,477 (4.4) | 270,422 (13.8) | |
| Other | 9563 (8.1) | 157,684 (14.6) | |
| LOS 21–27 days | Overall | 35,457 (2.1) | 831,620 (8.8) |
| Private | 11,866 (1.9) | 2,77,342 (8.5) | |
| Regional | 4251 (2.0) | 99,921 (8.7) | |
| Secondary | 6710 (1.8) | 157,566 (7.9) | |
| Tertiary | 7121 (1.9) | 167,133 (8.5) | |
| Other | 5509 (4.6) | 129,658 (12.0) | |
| LOS ≥ 28 days | Overall | 44,956 (2.7) | 1,990,233 (21.1) |
| Private | 11,988 (2.0) | 478,566 (14.6) | |
| Regional | 5767 (2.8) | 255,509 (22.3) | |
| Secondary | 9594 (2.5) | 448,356 (22.6) | |
| Tertiary | 8286 (2.2) | 371,071 (18.9) | |
| Other | 9321 (7.8) | 436,731 (40.4) |
| Variable | Longer LOS (Odds Ratio (OR), 95% CI) | Mortality (Hazard Ratio (HR) 95% CI) |
|---|---|---|
| Age groups, years | ||
| 20–24 | 0.74 (0.71–0.78) | 0.22 (0.18–0.29) |
| 25–29 | 0.85 (0.81–0.88) | 0.26 (0.21–0.32) |
| 30–34 | 0.97 (0.93–1.01) | 0.32 (0.27–0.38) |
| 35–39 | 1.01 (0.97–1.05) | 0.40 (0.35–0.46) |
| 40–44 | 0.97 (0.94–1.01) | 0.56 (0.50–0.63) |
| 45–49 | 0.95 (0.92–0.99) | 0.70 (0.64–0.77) |
| 50–54 | 0.96 (0.93–0.99) | 0.80 (0.74–0.87) |
| 55–59 | 0.95 (0.92–0.98) | 0.91 (0.85–0.97) |
| 60–64 | 1.0 [reference] | 1.0 [reference] |
| 65–69 | 1.03 (1.00–1.06) | 1.08 (1.02–1.14) |
| 70–74 | 1.16 (1.13–1.19) | 1.18 (1.12–1.24) |
| 75–79 | 1.47 (1.43–1.51) | 1.32 (1.25–1.39) |
| 80–84 | 1.80 (1.75–1.85) | 1.62 (1.54–1.71) |
| ≥85 | 2.32 (2.26–2.38) | 2.50 (2.38–2.62) |
| Female gender | 1.09 (1.08–1.11) | 0.90 (0.88–0.92) |
| Indigenous population | ||
| Yes | 0.89 (0.83–0.95) | 1.05 (0.90–1.21) |
| No | 1.0 [reference] | 1.0 [reference] |
| Undefined | 1.13 (1.07–1.19) | 1.34 (1.22–1.47) |
| Charlson co–morbidity Index | ||
| 0 | 1.0 [reference] | 1.0 [reference] |
| 1–2 | 1.44 (1.42–1.46) | 2.74 (2.63–2.85) |
| 3–4 | 2.04 (2.00–2.09) | 4.27 (4.09–4.46) |
| 5–6 | 2.15 (2.07–2.23) | 6.15 (5.81–6.50) |
| >6 | 0.95 (0.93–0.98) | 10.68 (10.24–11.13) |
| Marital Status | ||
| Never married | 1.59 (1.56–1.61) | 0.89 (0.86–0.93) |
| Widowed | 1.26 (1.23–1.28) | 0.95 (0.92–0.97) |
| Married or defacto | 1.0 [reference] | 1.0 [reference] |
| Divorced or separated | 1.37 (1.34–1.40) | 0.86 (0.83–0.90) |
| Other | 1.29 (1.24–1.35) | 1.42 (1.32–1.52) |
| Current smoker | 1.26 (1.24–1.28) | 0.87 (0.83–0.91) |
| DRG type | ||
| Medical | 1.0 [reference] | 1.0 [reference] |
| Surgical | 0.60 (0.59–0.61) | 0.28 (0.26–0.29) |
| Other | 0.79 (0.76–0.82) | 1.09 (1.04–1.14) |
| Emergency (unscheduled) admission | 0.64 (0.63–0.65) | 1.61 (1.56–1.65) |
| Admission source | ||
| Home | 1.0 [reference] | 1.0 [reference] |
| Aged care residential facility | 0.97 (0.90–1.04) | 2.49 (2.33–2.67) |
| From another hospital | 4.12 (4.06–4.18) | 0.90 (0.87–0.93) |
| Other | 4.24 (4.14–4.34) | 1.80 (1.73–1.87) |
| ICU stay | 3.38 (3.31–3.45) | 3.17 (3.06–3.28) |
| Admitted on weekend | 1.07 (1.05–1.08) | 0.94 (0.91–0.96) |
| Season of admission | ||
| Spring (Sep–Nov) | 1.0 [reference] | 1.0 [reference] |
| Summer (Dec–Feb) | 1.17 (1.15–1.19) | 0.96 (0.93–0.99) |
| Autumn (Mar–May) | 1.15 (1.13–1.17) | 0.98 (0.95–1.01) |
| Winter (Jun-Aug) | 1.14 (1.13–1.16) | 0.98 (0.95–1.01) |
| Prior admissions (in 12 months) | ||
| 0 | 1.0 [reference] | 1.0 [reference] |
| 1 | 1.22 (1.19–1.24) | 0.85 (0.81–0.88) |
| ≥2 | 1.32 (1.30–1.35) | 0.98 (0.95–1.01) |
| Risk category based on admission unit | ||
| 1 | 1.0 [reference] | 1.0 [reference] |
| 2 | 1.86 (1.83–1.89) | 0.91 (0.87–0.94) |
| 3 | 2.42 (2.38–2.47) | 1.38 (1.34–1.43) |
| 4 | 8.39 (8.22–8.56) | 2.59 (2.50–2.69) |
| Died in hospital | 0.90 (0.87–0.93) | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ofori-Asenso, R.; Liew, D.; Mårtensson, J.; Jones, D. The Frequency of, and Factors Associated with Prolonged Hospitalization: A Multicentre Study in Victoria, Australia. J. Clin. Med. 2020, 9, 3055. https://doi.org/10.3390/jcm9093055
Ofori-Asenso R, Liew D, Mårtensson J, Jones D. The Frequency of, and Factors Associated with Prolonged Hospitalization: A Multicentre Study in Victoria, Australia. Journal of Clinical Medicine. 2020; 9(9):3055. https://doi.org/10.3390/jcm9093055
Chicago/Turabian StyleOfori-Asenso, Richard, Danny Liew, Johan Mårtensson, and Daryl Jones. 2020. "The Frequency of, and Factors Associated with Prolonged Hospitalization: A Multicentre Study in Victoria, Australia" Journal of Clinical Medicine 9, no. 9: 3055. https://doi.org/10.3390/jcm9093055