The Long-Term Outcomes of Intensive Combined Therapy of Adult Patients with Localised Synovial Sarcoma

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patients and Treatment
3.2. Local and Distant Recurrence
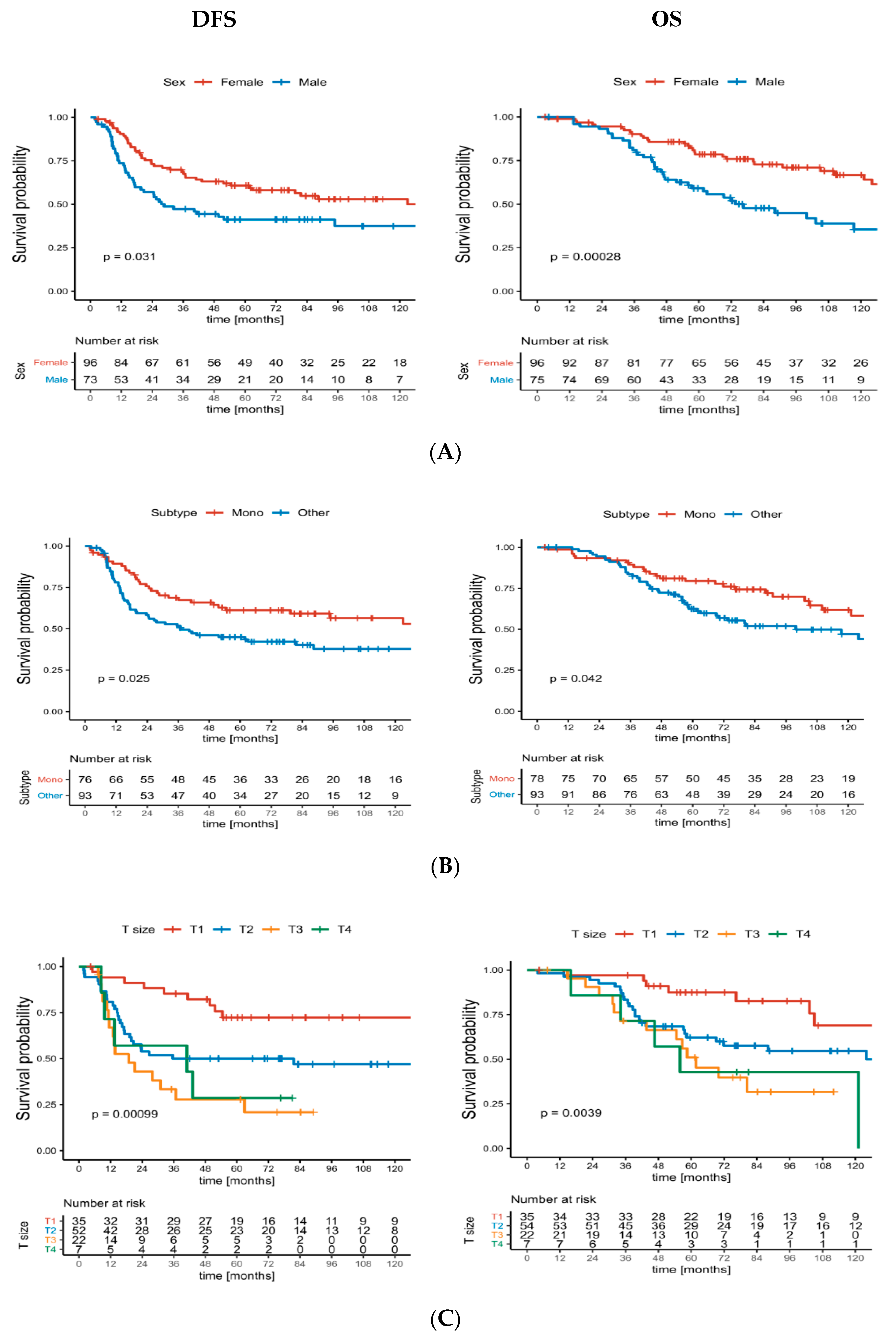
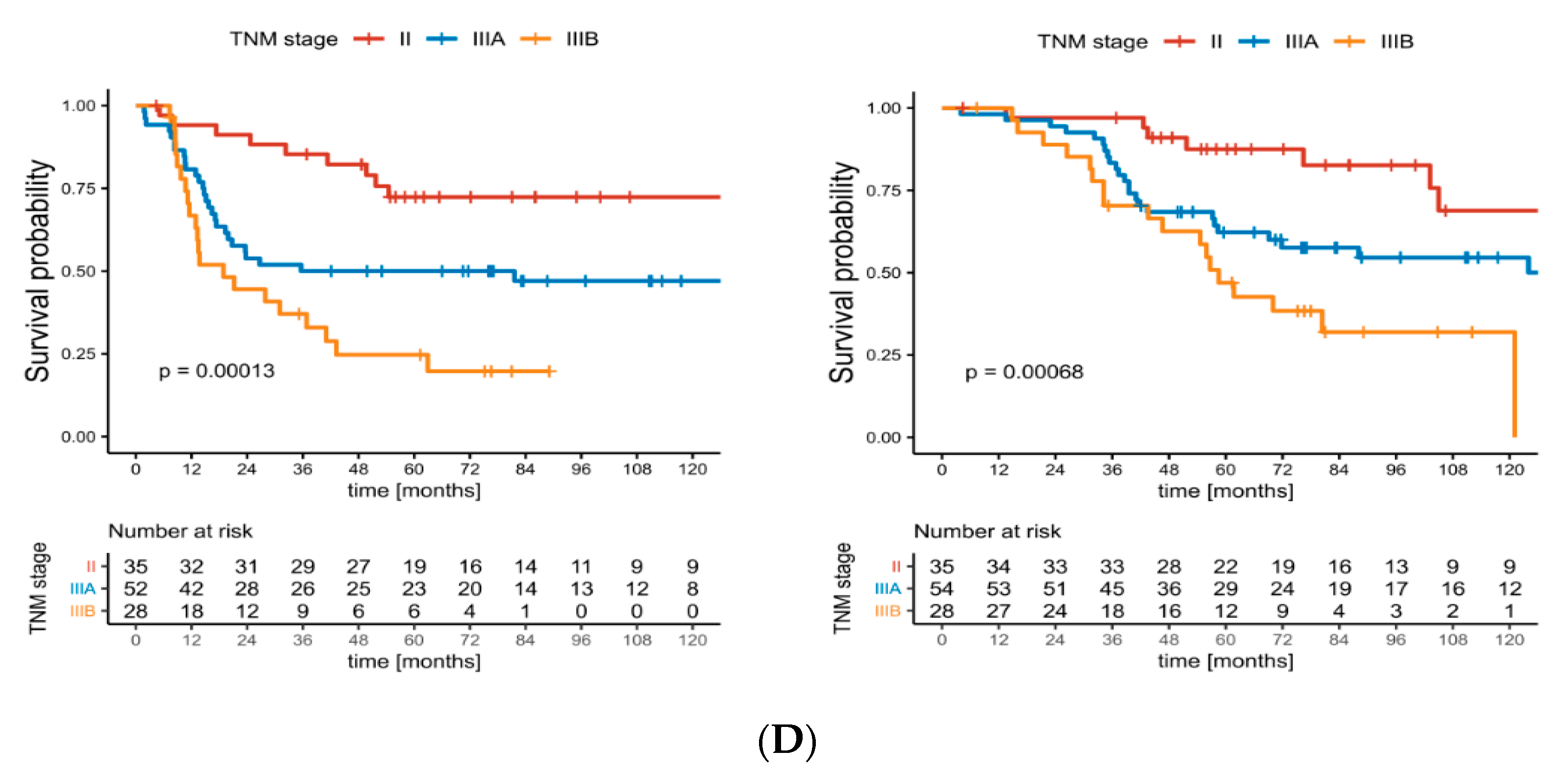
3.3. Disease-Free Survival
3.4. Overall Survival
3.5. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brennan, M.F.; Antonescu, C.R.; Alektiar, K.M.; Maki, R.G. Management of Soft Tissue Sarcoma; Springer: New York, NY, USA, 2013. [Google Scholar]
- Palmerini, E.; Staals, E.L.; Alberghini, M.; Zanella, L.; Ferrari, C.; Benassi, M.S.; Picci, P.; Mercuri, M.; Bacci, G.; Ferrari, S. Synovial sarcoma: Retrospective analysis of 250 patients treated at a single institution. Cancer 2009, 115, 2988–2998. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Penel, N.; Robin, Y.M.; Bui, B.; Le Cesne, A.; Piperno-Neumann, S.; Tubiana-Hulin, M.; Bompas, E.; Chevreau, C.; Isambert, N.; et al. Neo/adjuvant chemotherapy does not improve outcome in resected primary synovial sarcoma: A study of the French Sarcoma Group. Ann. Oncol. 2009, 20, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Eilber, F.C.; Dry, S.M. Diagnosis and management of synovial sarcoma. J. Surg. Oncol. 2008, 97, 314–320. [Google Scholar] [CrossRef]
- Lewis, J.J.; Antonescu, C.R.; Leung, D.H.; Blumberg, D.; Healey, J.H.; Woodruff, J.M.; Brennan, M.F. Synovial sarcoma: A multivariate analysis of prognostic factors in 112 patients with primary localized tumors of the extremity. J. Clin. Oncol. 2000, 18, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Spillane, A.J.; A’Hern, R.; Judson, I.R.; Fisher, C.; Thomas, J.M. Synovial sarcoma: A clinicopathologic, staging, and prognostic assessment. J. Clin. Oncol. 2000, 18, 3794–3803. [Google Scholar] [CrossRef] [PubMed]
- Trassard, M.; Le Doussal, V.; Hacene, K.; Terrier, P.; Ranchere, D.; Guillou, L.; Fiche, M.; Collin, F.; Vilain, M.O.; Bertrand, G.; et al. Prognostic factors in localized primary synovial sarcoma: A multicenter study of 128 adult patients. J. Clin. Oncol. 2001, 19, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulos, I.; Mertens, F.; Isaksson, M.; Limon, J.; Gustafson, P.; Skytting, B.; Akerman, M.; Sciot, R.; Dal Cin, P.; Samson, I.; et al. Clinical impact of molecular and cytogenetic findings in synovial sarcoma. Genes Chromosomes. Cancer 2001, 31, 362–372. [Google Scholar] [CrossRef]
- Carmody Soni, E.E.; Schlottman, S.; Erkizan, H.V.; Uren, A.; Toretsky, J.A. Loss of SS18-SSX1 inhibits viability and induces apoptosis in synovial sarcoma. Clin. Orthop. Relat. Res. 2014, 472, 874–882. [Google Scholar] [CrossRef] [Green Version]
- Ladanyi, M.; Antonescu, C.R.; Leung, D.H.; Woodruff, J.M.; Kawai, A.; Healey, J.H.; Brennan, M.F.; Bridge, J.A.; Neff, J.R.; Barr, F.G.; et al. Impact of SYT-SSX fusion type on the clinical behavior of synovial sarcoma: A multi-institutional retrospective study of 243 patients. Cancer Res. 2002, 62, 135–140. [Google Scholar]
- Ferrari, A.; Gronchi, A.; Casanova, M.; Meazza, C.; Gandola, L.; Collini, P.; Lozza, L.; Bertulli, R.; Olmi, P.; Casali, P.G. Synovial sarcoma: A retrospective analysis of 271 patients of all ages treated at a single institution. Cancer 2004, 101, 627–634. [Google Scholar] [CrossRef]
- Gronchi, A.; Ferrari, S.; Quagliuolo, V.; Broto, J.M.; Pousa, A.L.; Grignani, G.; Basso, U.; Blay, J.-Y.; Tendero, O.; Diaz, R.; et al. Histotype-tailored neoadjuvant chemotherapy versus standard chemotherapy in patients with high-risk soft-tissue sarcomas (ISG-STS 1001): An international, open-label, randomised, controlled, phase 3, multicentre trial. Lancet Oncol. 2017, 18, 812–822. [Google Scholar] [CrossRef]
- Kawai, A.; Woodruff, J.; Healey, J.H.; Brennan, M.F.; Antonescu, C.R.; Ladanyi, M. SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. N. Engl. J. Med. 1998, 338, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, H.; Nagasaka, T.; Otsuka, T.; Sugiura, E.; Nakashima, N.; Eimoto, T. Association of SYT-SSX fusion types with proliferative activity and prognosis in synovial sarcoma. Mod. Pathol. 2000, 13, 482–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Outani, H.; Nakamura, T.; Murata, H.; Stevenson, J.; Parry, M.; Gregory, J.; Tillman, R.; Jeys, L.; Abudu, A. Localized synovial sarcoma: A single institutional study of 191 patients with a minimum follow-up of 5 years for survivors. J. Surg. Oncol. 2019, 119, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Singer, S.; Baldini, E.H.; Demetri, G.D.; Fletcher, J.A.; Corson, J.M. Synovial sarcoma: Prognostic significance of tumor size, margin of resection, and mitotic activity for survival. J. Clin. Oncol. 1996, 14, 1201–1208. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, Y.; Wang, C.; Shi, Y. Adjuvant chemotherapy decreases and postpones distant metastasis in extremity stage IIB/III synovial sarcoma patients. J. Surg. Oncol. 2012, 106, 162–168. [Google Scholar] [CrossRef]
- Canter, R.J.; Qin, L.X.; Maki, R.G.; Brennan, M.F.; Ladanyi, M.; Singer, S. A synovial sarcoma-specific preoperative nomogram supports a survival benefit to ifosfamide-based chemotherapy and improves risk stratification for patients. Clin. Cancer Res. 2008, 14, 8191–8197. [Google Scholar] [CrossRef] [Green Version]
- Von Mehren, M.; Benjamin, R.S. Soft Tissue Sarcoma, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. Available online: https://www.nccn.org/professionals/physician_gls/PDF/sarcoma.pdf (accessed on 27 September 2020).
- Casali, P.G.; Abecassis, N.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brodowicz, T.; Broto, J.M.; et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv51–iv67. [Google Scholar] [CrossRef]
- Krieg, A.H.; Hefti, F.; Speth, B.M.; Jundt, G.; Guillou, L.; Exner, U.G.; von Hochstetter, A.R.; Cserhati, M.D.; Fuchs, B.; Mouhsine, E.; et al. Synovial sarcomas usually metastasize after >5 years: A multicenter retrospective analysis with minimum follow-up of 10 years for survivors. Ann. Oncol. 2011, 22, 458–467. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0; National Cancer Institute: Bethesda, MD, USA, 2009.
- Team R Core. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Wickham, H. Tidyverse: Easily Install and Load “Tidyverse” Packages. 2017. Available online: https://tidyverse.tidyverse.org/ (accessed on 22 September 2020).
- Vlenterie, M.; Litiere, S.; Rizzo, E.; Marreaud, S.; Judson, I.; Gelderblom, H.; Le Cesne, A.; Wardelmann, E.; Messiou, C.; Gronchi, A.; et al. Outcome of chemotherapy in advanced synovial sarcoma patients: Review of 15 clinical trials from the European Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group; setting a new landmark for studies in this entity. Eur. J. Cancer 2016, 58, 62–72. [Google Scholar] [CrossRef]
- Eilber, F.C.; Brennan, M.F.; Eilber, F.R.; Eckardt, J.J.; Grobmyer, S.R.; Riedel, E.; Forscher, C.; Maki, R.G.; Singer, S. Chemotherapy is associated with improved survival in adult patients with primary extremity synovial sarcoma. Ann. Surg. 2007, 246, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Vining, C.C.; Sinnamon, A.J.; Ecker, B.L.; Kelz, R.R.; Fraker, D.L.; Roses, R.E.; Karakousis, G.C. Adjuvant chemotherapy in resectable synovial sarcoma. J. Surg. Oncol. 2017, 116, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Naing, K.W.; Monjazeb, A.M.; Li, C.S.; Lee, L.Y.; Yang, A.; Borys, D.; Canter, R.J. Perioperative radiotherapy is associated with improved survival among patients with synovial sarcoma: A SEER analysis. J. Surg. Oncol. 2015, 111, 158–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gingrich, A.A.; Marrufo, A.S.; Liu, Y.; Li, C.S.; Darrow, M.A.; Monjazeb, A.M.; Thorpe, S.W.; Canter, R.J. Radiotherapy is Associated With Improved Survival in Patients With Synovial Sarcoma Undergoing Surgery: A National Cancer Database Analysis. J. Surg. Res. 2020, 255, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Park, J.; Kim, H.J.; Kim, I.H.; Han, I.; Kim, H.S.; Kim, S. Effects of Adjuvant Radiotherapy in Patients With Synovial Sarcoma. Am. J. Clin. Oncol. 2017, 40, 306–311. [Google Scholar] [CrossRef]
- Eilber, F.; Eckardt, J.; Rosen, G.; Forscher, C.; Selch, M.; Fu, Y.S. Preoperative therapy for soft tissue sarcoma. Hematol. Oncol. Clin. N. Am. 1995, 9, 817–823. [Google Scholar] [CrossRef]
- Blay, J.Y.; Papai, Z.; Tolcher, A.W.; Italiano, A.; Cupissol, D.; López-Pousa, A.; Chawla, S.P.; Bompas, E.; Babovic, N.; Penel, N.; et al. Ombrabulin plus cisplatin versus placebo plus cisplatin in patients with advanced soft-tissue sarcomas after failure of anthracycline and ifosfamide chemotherapy: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015, 16, 531–540. [Google Scholar] [CrossRef]
- Jelic, S.; Kovcin, V.; Milanovic, N.; Babovic, N.; Kreacic, M.; Ristovic, Z.; Vlajic, M.; Filipovic-Ljeskovic, I. Randomized study of high-dose epirubicin versus high-dose epirubicin and cisplatin chemotherapy for advanced soft tissue sarcoma. Eur. J. Cancer 1997, 33, 220–225. [Google Scholar] [CrossRef]
- Ferrari, A.; Sultan, I.; Huang, T.T.; Rodriguez-Galindo, C.; Shehadeh, A.; Meazza, C.; Ness, K.K.; Casanova, M.; Spunt, S.L. Soft tissue sarcoma across the age spectrum: A population-based study from the Surveillance Epidemiology and End Results database. Pediatr. Blood Cancer 2011, 57, 943–949. [Google Scholar] [CrossRef] [Green Version]
- Guillou, L.; Benhattar, J.; Bonichon, F.; Gallagher, G.; Terrier, P.; Stauffer, E.; de Saint Aubain Somerhausen, N.; Michels, J.J.; Jundt, G.; Vince, D.R.; et al. Histologic grade, but not SYT-SSX fusion type, is an important prognostic factor in patients with synovial sarcoma: A multicenter, retrospective analysis. J. Clin. Oncol. 2004, 22, 4040–4050. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, F.; Brookland, D.R.; Washington, R.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Gustafson, P.; Dreinhofer, K.E.; Rydholm, A. Soft tissue sarcoma should be treated at a tumor center. A comparison of quality of surgery in 375 patients. Acta Orthop. Scand. 1994, 65, 47–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | n | % |
|---|---|---|
| Age | ||
| ≤35 | 102 | 60 |
| >35 | 69 | 40 |
| Sex | ||
| Female | 96 | 56 |
| Male | 75 | 44 |
| Histological subtype a | ||
| Monophasic | 78 | 59 |
| Biphasic | 44 | 33 |
| Poorly differentiated | 11 | 8 |
| Localisation of primary tumour | ||
| Upper limb | 32 | 19 |
| Lower limb | 121 | 71 |
| Trunk wall | 15 | 9 |
| Retroperitoneal space and head and neck | 3 | 2 |
| Size of primary tumour, cm b | ||
| ≤5 | 35 | 30 |
| >5 | 83 | 70 |
| Disease stage according to AJCC b | ||
| II | 35 | 30 |
| IIIA | 55 | 47 |
| IIIB | 28 | 24 |
| Status at initiation of treatment in MSCNRIO | ||
| Patients previously untreated (primary tumour) | 77 | 45 |
| Patients after surgical treatment without prior diagnostic biopsy | 64 | 37 |
| Clinical local recurrence | 30 | 18 |
| Type of surgical treatment for localisation in an extremity | ||
| Limb-sparing surgery | 136 | 89 |
| Amputation | 17 | 11 |
| Surgical margins | ||
| R0 | 149 | 87 |
| R1 | 22 | 13 |
| Preoperative radiotherapy | 154 | |
| 5 × 4 Gy | 84 | 55 |
| 5 × 5 Gy | 69 | 45 |
| 28 × 1.8 Gy | 1 | 1 |
| Number of cycles of perioperative adjuvant chemotherapy | ||
| six | 149 | 87 |
| five | 6 | 4 |
| four | 7 | 4 |
| three | 6 | 4 |
| two | 3 | 2 |
| Variable | 5-Year LRFS | 95% CI | p | 5-Year MFS | 95% CI | p | 5-Year OS | 95% CI | p |
|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||
| ≤35 | 80% | 0.72–0.89 | 0.82 | 66% | 0.58–0.76 | 0.0051 | 81% | 0.73–0.88 | 0.014 |
| >35 | 81% | 0.70–0.93 | 52% | 0.41–0.66 | 67% | 0.57–0.80 | |||
| Sex | |||||||||
| Female | 88% | 0.81–0.95 | 0.02 | 70% | 0.62–0.81 | 0.0068 | 84% | 0.76–0.92 | <0.001 |
| Male | 70% | 0.59–0.83 | 48% | 0.37–0.61 | 64% | 0.54–0.76 | |||
| Histological subtype | |||||||||
| Monophasic | 78% | 0.69–0.89 | 0.39 | 74% | 0.64–0.49 | 0.08 | 79% | 0.71–0.89 | 0.2 |
| Biphasic | 84% | 0.73–0.96 | 44% | 0.32–0.62 | 60% | 0.47–0.77 | |||
| Poorly differentiated | 100% | 1.00–1.00 | 50% | 0.27–0.92 | 54% | 0.26–1.00 | |||
| Not specified | 76% | 0.63–0.93 | 58% | 0.44–0.76 | 65% | 0.51–0.82 | |||
| T stage | |||||||||
| T1 | 84% | 0.71–0.98 | 0.97 | 85% | 0.74–0.98 | <0.001 | 88% | 0.77–0.99 | 0.0039 |
| T2 | 88% | 0.79–0.98 | 53% | 0.41–0.69 | 62% | 0.50–0.77 | |||
| T3 | 85% | 0.71–1.00 | 32% | 0.17–0.61 | 51% | 0.33–0.78 | |||
| T4 | 86% | 0.63–1.00 | 29% | 0.09–0.92 | 43% | 0.18–1.00 | |||
| TNM stage | |||||||||
| II | 84% | 0.71–0.98 | 0.86 | 85% | 0.74–0.98 | <0.001 | 88% | 0.77–0.99 | <0.001 |
| IIIA | 88% | 0.79–0.98 | 53% | 0.41–0.69 | 62% | 0.50–0.77 | |||
| IIIB | 85% | 0.72–1.00 | 28% | 0.15–0.52 | 47% | 0.31–0.71 | |||
| Surgical margins | |||||||||
| R0 | 82% | 0.76–0.89 | 0.048 | 62% | 0.55–0.71 | 0.57 | 73% | 0.66–0.81 | 0.25 |
| R1 | 69% | 0.51–0.93 | 50% | 0.33–0.76 | 53% | 0.35–0.80 |
| Variables | MFS HR (95% CI), p | DFS HR (95% CI), p | OS HR (95% CI), p |
|---|---|---|---|
| Male sex | 1.53 (0.90–2.60), p = 0.117 | 1.60 (0.97–2.64), p = 0.067 | 2.18 (1.25–3.78), p = 0.006 |
| Age > 35 years | 2.53 (1.48–4.34), p = 0.001 | 2.39 (1.44–3.96), p = 0.001 | 2.03 (1.17–3.52), p = 0.012 |
| Histologic subtype other than monophasic | 1.95 (1.11–3.44), p = 0.021 | 1.97 (1.15–3.35), p = 0.013 | 1.94 (1.09–3.44), p = 0.025 |
| Tumour size (continuous variable) | 1.10 (1.05–1.16), p < 0.001 | 1.09 (1.04–1.14), p < 0.001 | 1.09 (1.04–1.14), p < 0.001 |
| Study | Number of Patients | Size of Primary Tumour (%) | Median Follow-Up Time (Months) | R1 Resection (%) | RT Periop (%) | CHT (%) | 5-Year LRFs (%) | 5-Year MFS (%) | 5-Year OS (%) |
|---|---|---|---|---|---|---|---|---|---|
| Canter et al. (2008) [18] | 255 | ≥5 cm | 72 | - | 63 | 39 | - | 55 | 72 |
| 56 | |||||||||
| Chen et al. (2012) [17] | 76 | ≥5 cm | 68 | 32 | 75 | 68 | - | 48 | 59 |
| 100 | |||||||||
| Italiano et al. (2009) [3] | 237 | - | 58 | 15 | 76 | 60 | 70 | 57 | 64 |
| Lewis et al. (2000) [5] | 112 | ≥5 cm | 72 | 14 | 46 | 37 | 78 | 61 | 75 |
| 45 | |||||||||
| Palmerini et al. (2009) [2] | 204 | >5 cm | 66 | 12 | 52 | 52 | 81 | - | 76 |
| 49 | |||||||||
| Trassard et al. (2001) [7] | 128 | ≥5 cm | 37 | 24 | 80 | 57 | - | - | 63 |
| 70 | |||||||||
| This study (2020) | 171 | ≥5 cm | 114 | 13 | 90 | 100 | 80 | 60 | 75 |
| 73 | |||||||||
| Ferrari et al. * (2004) [11] | 215 | >5 cm | 65 | - | 50 | 28 | 63 | 51 | 71 |
| 64 | |||||||||
| Outani et al. * (2019) [15] | 191 | ≥5 cm | 68 | 7 | 55 | 30 | 89 | 66 | 76 |
| 63 | |||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozak, K.; Teterycz, P.; Świtaj, T.; Koseła-Paterczyk, H.; Falkowski, S.; Morysiński, T.; Bartnik, E.; Czarnecka, A.M.; Wągrodzki, M.; Ługowska, I.; et al. The Long-Term Outcomes of Intensive Combined Therapy of Adult Patients with Localised Synovial Sarcoma. J. Clin. Med. 2020, 9, 3129. https://doi.org/10.3390/jcm9103129
Kozak K, Teterycz P, Świtaj T, Koseła-Paterczyk H, Falkowski S, Morysiński T, Bartnik E, Czarnecka AM, Wągrodzki M, Ługowska I, et al. The Long-Term Outcomes of Intensive Combined Therapy of Adult Patients with Localised Synovial Sarcoma. Journal of Clinical Medicine. 2020; 9(10):3129. https://doi.org/10.3390/jcm9103129
Chicago/Turabian StyleKozak, Katarzyna, Paweł Teterycz, Tomasz Świtaj, Hanna Koseła-Paterczyk, Sławomir Falkowski, Tadeusz Morysiński, Ewa Bartnik, Anna M. Czarnecka, Michał Wągrodzki, Iwona Ługowska, and et al. 2020. "The Long-Term Outcomes of Intensive Combined Therapy of Adult Patients with Localised Synovial Sarcoma" Journal of Clinical Medicine 9, no. 10: 3129. https://doi.org/10.3390/jcm9103129