Adsorption of Blood Components to Extracorporeal Membrane Oxygenation (ECMO) Surfaces in Humans: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Search Strategy and Selection Criteria
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Quality Assessment
3. Results
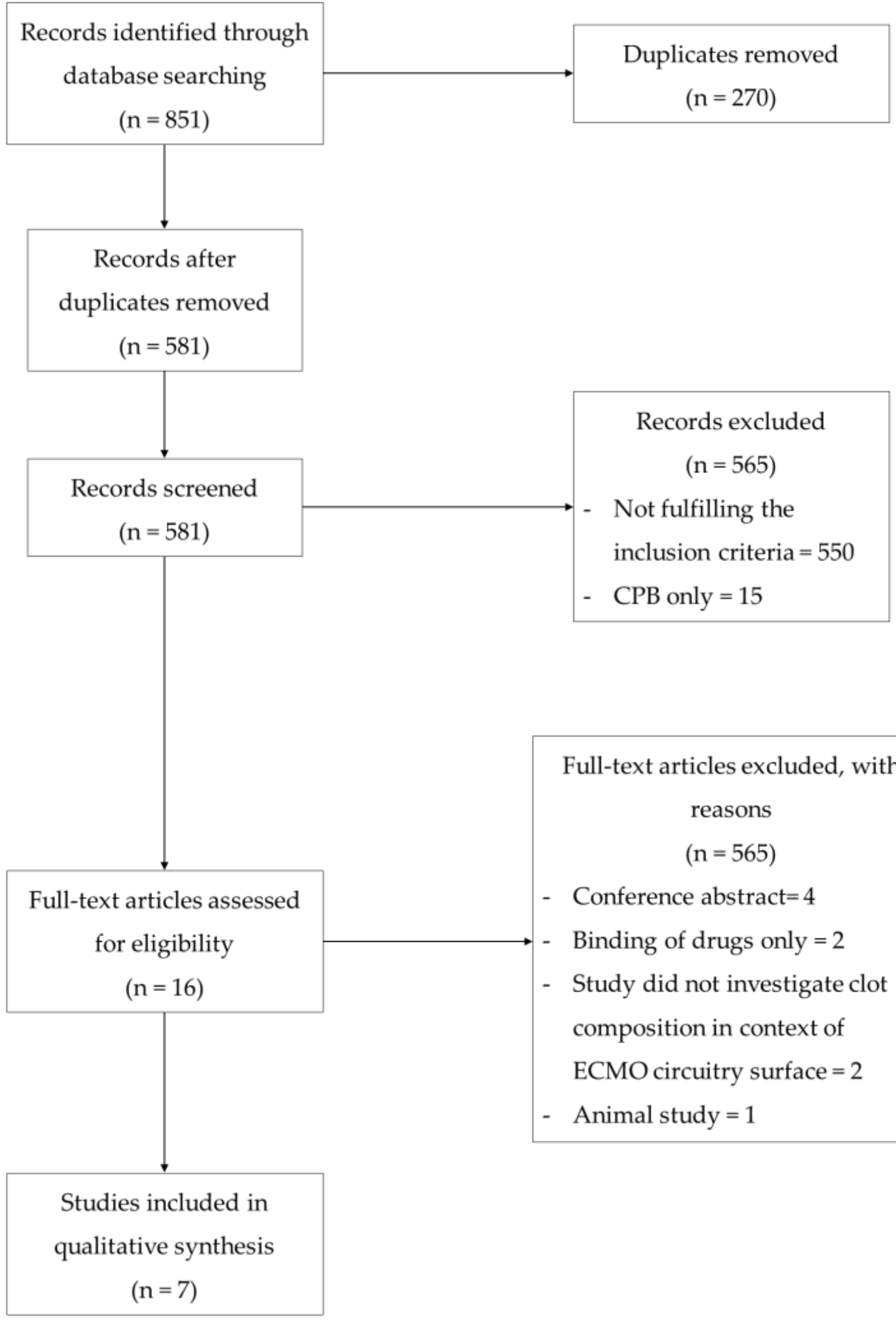
3.1. Description of Included Studies
3.2. Plasma Protein Binding
3.2.1. Fibrin
3.2.2. Von Willebrand Factor
3.2.3. Other Plasma Proteins
3.3. Blood Cell Binding
3.3.1. Erythrocytes
3.3.2. Leukocytes
3.3.3. Platelets
3.3.4. Other Blood Cell Binding
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
Appendix A. Search Strategies
Appendix A.1. Medline Database
- * extracorporeal membrane oxygenation/
- * Oxygenators, Membrane/
- (ecls or ecmo or extracorporeal adj3 life adj3 support * or extracorporeal adj3 membrane adj3 oxygenation *).tw, kf.
- Protein Binding/
- Adsorption/
- Cell Adhesion/
- (bind or binding or adsorption or adhesion or adherence or adhere or accumulation * or deposit * or biomass or thrombosis or coagulat * or clot or clots or clotting or structure or composition).tw, kf.
- Thrombosis/
- exp Blood Proteins/
- exp Endothelial Cells/
- exp Blood Cells/
- (platelet * or erythrocyte * or leukocyte * or vWF or von-willebrand or coagulation-factor *).tw, kf.
- or 2 or * 3) and (4 or 5 or 6 or 7 or 8) and (9 or 10 or 11 or 12).
- exp animals/not human *.sh.
- not 14.
- limit 15 to (english language and yr = “1985-Current”).
Appendix A.2. Embase Database
- * extracorporeal membrane oxygenation device/or * oxygenator/or * extracorporeal oxygenation/
- (ecls or ecmo or extracorporeal adj2 life adj2 support * or extracorporeal adj2 membrane adj2 oxygenation *).tw, kw.
- adsorption/
- bioaccumulation/
- cell adhesion/
- thrombosis/
- protein binding/
- (bind or binding or adsorption or adhesion or adherence or adhere or accumulation * or deposit * or biomass or thrombosis or coagulat * or clot or clots or clotting or structure or composition).tw, kw.
- exp plasma protein/
- leukocyte adherence/
- thrombocyte aggregation/
- endothelium cell/
- exp blood cell/
- (platelet * or erythrocyte * or leukocyte * or vWF or von-willebrand or coagulation-factor *).tw, kw.
- or 2 *) and (3 or 4 or 5 or 6 or 7 or 8) and (9 or 10 or 11 or 12 or 13 or 14)
- exp animals/not human *.sh.
- not 16.
- limit 17 to (english language and yr = “1985-Current”).
Appendix A.3. PubMed Database
Appendix B. Table and Figure

{kind=link}
| Quality Criteria | Study and Scores | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Dimension | Specific Criteria a | Owen et al. [16] | Niimi et al. [13] | Lehle et al. [11] | Dornia et al. [12] | Lehle et al. [17] | Wilm et al. [14] | Steiger et al. [15] | |
| 1 | Clear aims and justification | A. Clear statement of the aims of the research | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| B. Rationale for number of pre- and post-intervention points or adequate baseline measurement | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| C. Explanation for lack of control group | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| D. Appropriateness of qualitative methodology | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| E. Appropriate study design | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| 2 | Managing bias in sampling or between groups | A. Sequence Generation | 0 | 0 | 0 | 0 | 0 | 2 | 0 |
| B. Allocation Concealment | 0 | 0 | 0 | 0 | 0 | 2 | 0 | ||
| C. Justification for sample choice | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| D. Intervention and control group selection designed to protect against systematic difference/selection bias | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| E. Comparability of groups | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| F. Sampling and recruitment | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| 3 | Managing bias in outcome measurements and blinding | A. Blinding | 1 | 1 | 1 | 1 | 1 | 2 | 1 |
| B. Baseline measurement-protection against selection bias | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| C. Protection against contamination | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| D. Protection against secular changes | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| E. Protection against detection bias: blinded assessment of primary outcome measures | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| F. Reliable primary outcome measures | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| G. Comparability of outcomes | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 4 | Managing bias in follow-up | A. Follow-up of subjects (protection against exclusion bias) | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| B. Follow-up of patients or episodes of care | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| C. Incomplete outcome data addressed | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| 5 | Managing bias in other study aspects | A. Protection against detection bias: Intervention unlikely to affect data collection | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| B. Protection against information bias | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| C. Data collection appropriate to address research aims | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| D. Attempts to mitigate effects of no control | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| 6 | Analytical rigor | A. Sufficient data points to enable reliable statistical inference | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| B. Shaping of intervention effect specified | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| C. Analysis sufficiently rigorous/free from bias | 1 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| 7 | Managing bias in reporting/ethical considerations | A. Free of selective outcome reporting | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| B. Limitations addressed | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| C. Conclusions clear and justified | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| D. Free of other bias | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| E. Ethics issues addressed | 2 | 2 | 2 | 2 | 2 | 2 | 2 | ||
| Total score | 42 | 42 | 43 | 42 | 42 | 48 | 43 | ||
| TITLE | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis or both. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary including as applicable background, objectives, data sources, study eligibility criteria, participants and interventions, study appraisal and synthesis methods, results, limitations, conclusions and implications of key findings, systematic review registration number. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 1–2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes and study design (PICOS). | 2 |
| METHODS | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address) and, if available, provide registration information including registration number. | 2 |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 2 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 2 |
| Search | 8 | Present full electronic search strategy for at least one database including any limits used such that it could be repeated. | 7–8 |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review and, if applicable, included in the meta-analysis). | 2 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 2 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 2 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level) and how this information is to be used in any data synthesis. | 2, 11 |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | NA |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | NA |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | 2, 11 |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | NA |
| RESULTS | |||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility and included in the review with reasons for exclusions at each stage, ideally with a flow diagram. | 2–3 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 2, 9 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 10 |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group, (b) effect estimates and confidence intervals, ideally with a forest plot. | 2–6, 9 |
| Synthesis of results | 21 | Present results of each meta-analysis done including confidence intervals and measures of consistency. | NA |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | 11 |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression (see Item 16)). | NA |
| DISCUSSION | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users and policy makers). | 6 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias) and at review level (e.g., incomplete retrieval of identified research, reporting bias). | 6 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence and implications for future research. | 5–6 |
| FUNDING | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 16 |
| Study | Setting | Blood Used | Age | ECMO Mode | Days on ECMO | Sample Size | Reason for ECMO Removal | Sample Type | Surface Coating | Blood Components Analyzed | Analysis Technique/s | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Owen et al. [16], 1985 | Ex vivo | Whole Blood | Neonate | Not specified | 4.8 | n = 1 | Not specified | Oxygenator (Silicone) | Not specified | Albumin, IgG | 2-D Electrophoresis | Analysis of plasma proteins adhering to a neonatal ECMO oxygenator in an ex vivo setting |
| Niimi et al. [13], 1997 | In vitro | Whole Blood | Not specified | Not applicable | 0.125 (in vivo) | n = 3 | Not applicable | Oxygenator (Silicone, double polyolefin, polypropylene) | Not specified | Platelets, Albumin, vWF, Fibronectin, Fibrinogen | SDS-PAGE, Western Blot, Enzyme Immunoassays | Comparison of platelet and protein adsorption to three different types of ECMO oxygenators |
| Lehle et al. [11], 2008 | Ex vivo | Whole Blood | 54 ± 14 | Femoro-jugular VV | 11.0 ± 7 | n = 31 | Reduced CO2 elimination and oxygen transfer capacity | Oxygenator (polymethylpentane) | Heparin | Platelets, Erythrocytes, Fibrin | Fluorescence Microscopy, SEM | SEM and fluorescence microscopy identified fibrous networks on ECMO oxygenators with imbedded platelets and erythrocytes |
| Dornia et al. [12], 2013 | Ex vivo | Whole Blood | Not specified | Femoro-jugular VV | 8 | n = 1 | Patient recovered | Oxygenator (polymethylpentane) | Heparin | Platelets, Erythrocytes, Fibrin | MDCT, SEM | Feasibility study for observing ECMO oxygenator clots using MDCT, implemented SEM to confirm clot formation, revealing adhered platelets and erythrocytes |
| Lehle et al. [17], 2016 | Ex vivo | Whole Blood | Not specified | VV and VA | 6.2 ± 3.3 | n = 16 | 11 due to patient recovered; 5 due to replacement during therapy | Oxygenator (polymethylpentane) | Not specified | Progenitor Cells (Endothelial-like, Mesenchymal-like), Leukocytes | Fluorescence Microscopy, Flow Cytometry, FACS | First report describing the accumulation of endothelial-like and mesenchymal-like cells on ECMO oxygenator surfaces |
| Wilm et al. [14], 2018 | Ex vivo | Whole Blood | 59 (49–71) | VV and VA | 10 (5–21) | n = 41 | 27 due to patient recovered; 5 due to patient death; 7 due to coagulation disorder; 1 due to risk of infection, 1 due to acute thrombosis. | Oxygenator (polymethylpentane) | Not specified | Leukocytes, vWF | Fluorescence Microscopy, Flow Cytometry, DAPI Staining | Immunofluorescence and flow cytometry used to confirm the accumulation of leukocytes on ECMO oxygenators |
| Steiger et al. [15], 2019 | Ex vivo | Whole Blood | 56 (33–68) | VV | Low 13 (8–21) High 8 (6–25) | n = 21 | 13 due to patient recovered; 2 due to patient death; 6 due to replacement during therapy | Oxygenator (polymethylpentane) | Heparin | vWF, Leukocytes, Platelets | Fluorescence Microscopy, DAPI Staining | vWF structures observed to aggregate around crossing points of gas fibers in ECMO oxygenator |
References
- Dalton, H.J.; Garcia-Filion, P.; Holubkov, R.; Moler, F.W.; Shanley, T.; Heidemann, S.; Meert, K.; Berg, R.A.; Berger, J.; Carcillo, J.; et al. Association of bleeding and thrombosis with outcome in extracorporeal life support. Pediatr. Crit. Care Med. 2015, 16, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, G.; Berg, N.; Broman, L.M.; Prahl Wittberg, L. Flow-induced platelet activation in components of the extracorporeal membrane oxygenation circuit. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, A.J.; Hunt, B.J. Current Understanding of How Extracorporeal Membrane Oxygenators Activate Haemostasis and Other Blood Components. Front. Med. 2018, 5, 352. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.A.; Hockings, L.E.; Andrews, R.K.; Aubron, C.; Gardiner, E.E.; Pellegrino, V.A.; Davis, A.K. Extracorporeal membrane oxygenation-hemostatic complications. Transfus. Med. Rev. 2015, 29, 90–101. [Google Scholar] [CrossRef]
- Zangrillo, A.; Landoni, G.; Biondi-Zoccai, G.; Greco, M.; Greco, T.; Frati, G.; Patroniti, N.; Antonelli, M.; Pesenti, A.; Pappalardo, F.J.C.C.; et al. A meta-analysis of complications and mortality of extracorporeal membrane oxygenation. Crit. Care Resusc. 2013, 15, 172. [Google Scholar]
- Van den Goor, J.M.; Van Oeveren, W.; Rutten, P.M.; Tijssen, J.G.; Eijsman, L. Adhesion of thrombotic components to the surface of a clinically used oxygenator is not affected by Trillium coating. Perfusion 2016, 21, 165–172. [Google Scholar] [CrossRef]
- Beely, B.M.; Campbell, J.E.; Meyer, A.; Langer, T.; Negaard, K.; Chung, K.K.; Cap, A.P.; Cancio, L.C.; Batchinsky, A.I. Electron microscopy as a tool for assessment of anticoagulation strategies during extracorporeal life support: The proof is on the membrane. ASAIO J. 2016, 62, 525–532. [Google Scholar] [CrossRef]
- Kundu, S.K.; Klein, M.D.; Whittlesey, G.C.; Barmatoski, S.P.; Salley, S.O. Quantitative scanning electron microscopy for the evaluation of thrombosis in extracorporeal circuits. ASAIO Trans. 1988, 34, 568–572. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Zingg, W.; Castro-Sanchez, E.; Secci, F.V.; Edwards, R.; Drumright, L.N.; Sevdalis, N.; Holmes, A.H. Innovative tools for quality assessment: Integrated quality criteria for review of multiple study designs (ICROMS). Public Health 2016, 133, 19–37. [Google Scholar] [CrossRef]
- Lehle, K.; Philipp, A.; Gleich, O.; Holzamer, A.; Muller, T.; Bein, T.; Schmid, C. Efficiency in extracorporeal membrane oxygenation-cellular deposits on polymethylpentene membranes increase resistance to blood flow and reduce gas exchange capacity. ASAIO J. 2008, 54, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Dornia, C.; Philipp, A.; Bauer, S.; Hoffstetter, P.; Lehle, K.; Schmid, C.; Lubnow, M.; Stroszczynski, C.; Schreyer, A.G. Visualization of thrombotic deposits in extracorporeal membrane oxygenation devices using multidetector computed tomography: A feasibility study. ASAIO J. 2013, 59, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Niimi, Y.; Yamane, S.; Yamaji, K.; Tayama, E.; Sueoka, A.; Nose, Y. Protein adsorption and platelet adhesion on the surface of an oxygenator membrane. ASAIO J. 1997, 43, M706–M710. [Google Scholar] [CrossRef] [PubMed]
- Wilm, J.; Philipp, A.; Muller, T.; Bredthauer, A.; Gleich, O.; Schmid, C.; Lehle, K. Leukocyte Adhesion as an Indicator of Oxygenator Thrombosis During Extracorporeal Membrane Oxygenation Therapy? ASAIO J. 2018, 64, 24–30. [Google Scholar] [CrossRef]
- Steiger, T.; Foltan, M.; Philipp, A.; Mueller, T.; Gruber, M.; Bredthauer, A.; Krenkel, L.; Birkenmaier, C.; Lehle, K. Accumulations of von Willebrand factor within ECMO oxygenators: Potential indicator of coagulation abnormalities in critically ill patients? Artif. Organs 2019, 43, 1065–1076. [Google Scholar] [CrossRef]
- Owen, D.R.; Chen, C.M.; Oschner, J.A.; Zone, R.M. Interactions of plasma proteins with selective artificial surfaces. Trans. Am. Soc. Artif. Intern. Organs 1985, 31, 240–243. [Google Scholar]
- Lehle, K.; Friedl, L.; Wilm, J.; Philipp, A.; Muller, T.; Lubnow, M.; Schmid, C. Accumulation of Multipotent Progenitor Cells on Polymethylpentene Membranes During Extracorporeal Membrane Oxygenation. Artif. Organs 2016, 40, 577–585. [Google Scholar] [CrossRef]
- De Mel, A.; Cousins, B.G.; Seifalian, A.M. Surface modification of biomaterials: A quest for blood compatibility. Int. J. Biomater. 2012, 2012, 707863. [Google Scholar] [CrossRef]
- Turbill, P.; Beugeling, T.; Poot, A.J.B. Proteins involved in the Vroman effect during exposure of human blood plasma to glass and polyethylene. Biomaterials 1996, 17, 1279–1287. [Google Scholar] [CrossRef] [Green Version]
- Kwak, D.; Wu, Y.; Horbett, T.A. Fibrinogen and von Willebrand’s factor adsorption are both required for platelet adhesion from sheared suspensions to polyethylene preadsorbed with blood plasma. J. Biomed. Mater. Res. A 2005, 74, 69–83. [Google Scholar] [CrossRef]
- Tsai, W.B.; Grunkemeier, J.M.; McFarland, C.D.; Horbett, T.A. Platelet adhesion to polystyrene-based surfaces preadsorbed with plasmas selectively depleted in fibrinogen, fibronectin, vitronectin, or von Willebrand’s factor. J. Biomed. Mater. Res. 2002, 60, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.B.; Grunkemeier, J.M.; Horbett, T.A. Human plasma fibrinogen adsorption and platelet adhesion to polystyrene. J. Biomed. Mater. Res. 1999, 44, 130–139. [Google Scholar] [CrossRef]
- Maslach-Hubbard, A.; Bratton, S.L. Extracorporeal membrane oxygenation for pediatric respiratory failure: History, development and current status. World J. Crit. Care Med. 2013, 2, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.W. The history of extracorporeal oxygenators. Anaesthesia 2006, 61, 984–995. [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Callaghan, S.; Cai, T.; McCafferty, C.; Van Den Helm, S.; Horton, S.; MacLaren, G.; Monagle, P.; Ignjatovic, V. Adsorption of Blood Components to Extracorporeal Membrane Oxygenation (ECMO) Surfaces in Humans: A Systematic Review. J. Clin. Med. 2020, 9, 3272. https://doi.org/10.3390/jcm9103272
Callaghan S, Cai T, McCafferty C, Van Den Helm S, Horton S, MacLaren G, Monagle P, Ignjatovic V. Adsorption of Blood Components to Extracorporeal Membrane Oxygenation (ECMO) Surfaces in Humans: A Systematic Review. Journal of Clinical Medicine. 2020; 9(10):3272. https://doi.org/10.3390/jcm9103272
Chicago/Turabian StyleCallaghan, Sam, Tengyi Cai, Conor McCafferty, Suelyn Van Den Helm, Steve Horton, Graeme MacLaren, Paul Monagle, and Vera Ignjatovic. 2020. "Adsorption of Blood Components to Extracorporeal Membrane Oxygenation (ECMO) Surfaces in Humans: A Systematic Review" Journal of Clinical Medicine 9, no. 10: 3272. https://doi.org/10.3390/jcm9103272