Medical Interventions for Patellofemoral Pain and Patellofemoral Osteoarthritis: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
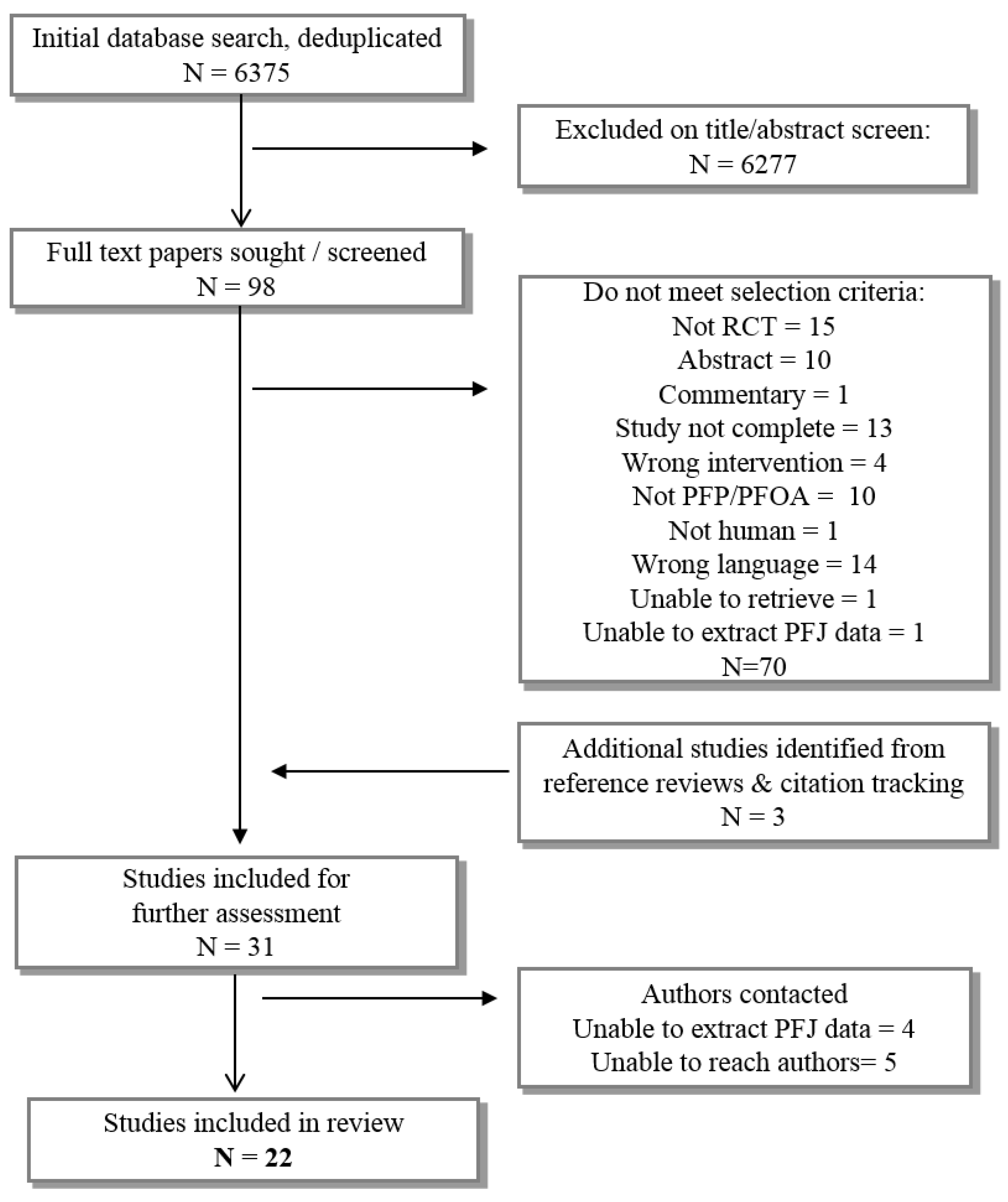
2. Methods
2.1. Study Design
2.2. Study Eligibility and Search Strategy
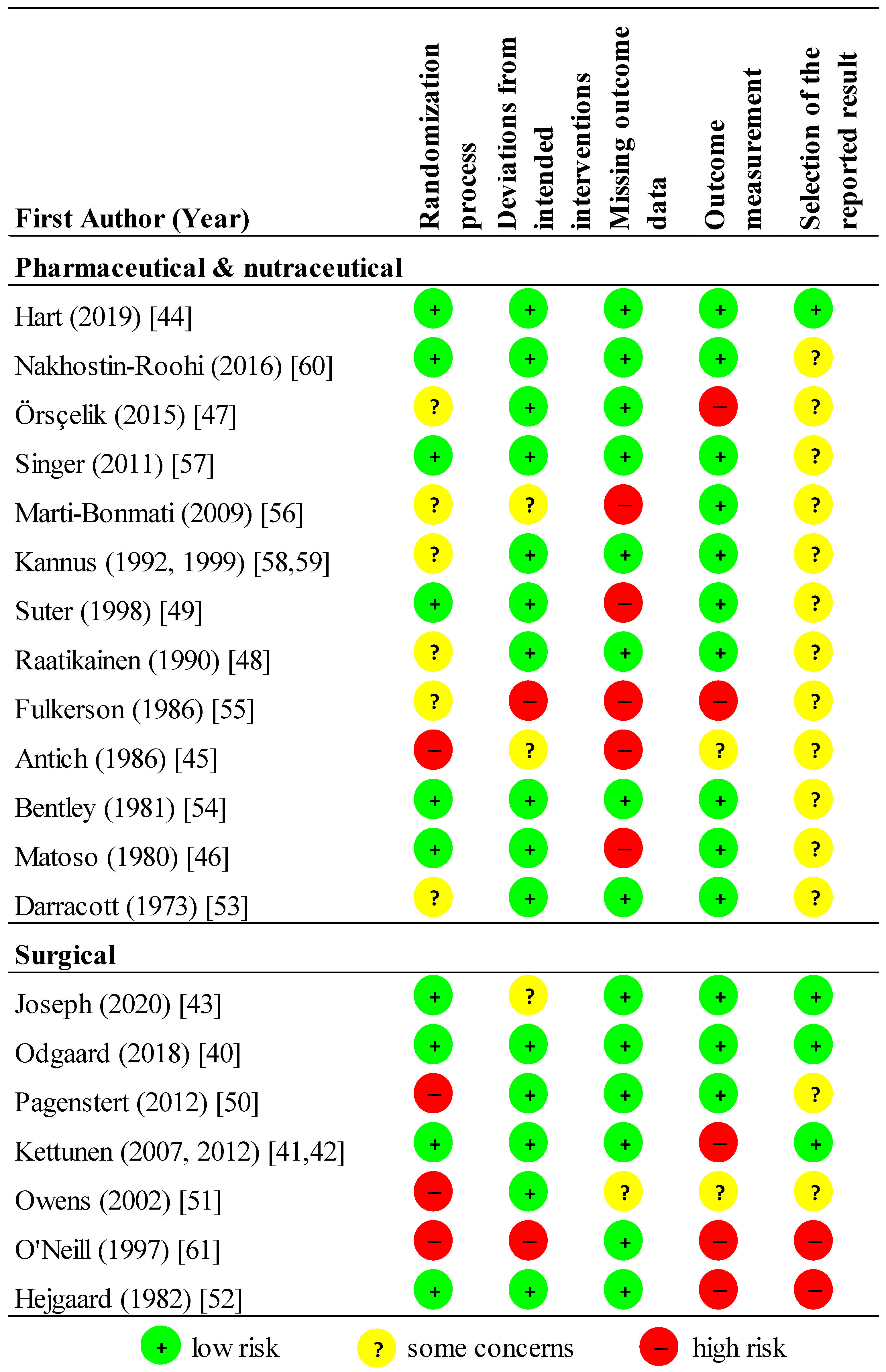
2.3. Risk of Bias
2.4. Data Extraction and Statistical Analyses
3. Results
3.1. Pharmaceutical or Nutraceutical Studies
3.2. Oral Administration
3.2.1. Nonsteroidal antiinflammatories, NSAIDs—Low Certainty of Evidence
3.2.2. Chloroquine—Very Low Certainty of Evidence
3.2.3. Glucosamine—Very Low Certainty of Evidence
3.3. Injections
3.3.1. Glycosaminoglycan Polysulphate (GAGPS)—Very Low Certainty of Evidence
3.3.2. Hyaluronic Acid—Low Certainty of Evidence
3.3.3. Platelet Rich Plasma (PRP)—Very Low Certainty of Evidence
3.3.4. Botox—Low Certainty of Evidence
3.3.5. Anabolic Steroids—Very Low Certainty of Evidence
3.4. Transdermal
3.4.1. NSAIDs (Phonophoresis)—Very Low Certainty of Evidence
3.4.2. Corticosteroid (Iontophoresis or Phonophoresis)—Very Low Certainty of Evidence
3.5. Surgical Studies
3.6. Arthroscopy
3.6.1. Standard Arthroscopy—Very Low Certainty of Evidence
3.6.2. Radiofrequency Debridement—Very Low Certainty of Evidence
3.7. Open Surgeries
3.7.1. Lateral Retinacular Surgery—Very Low Certainty of Evidence
3.7.2. Anterior Tibial Tuberosity Displacement—Very Low Certainty of Evidence
3.7.3. Patellofemoral Arthroplasty—Moderate Certainty of Evidence
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Crossley, K.M.; Stefanik, J.J.; Selfe, J.; Collins, N.J.; Davis, I.S.; Powers, C.M.; McConnell, J.; Vicenzino, B.; Bazett-Jones, D.M.; Esculier, J.F.; et al. 2016 patellofemoral pain consensus statement from the 4th international patellofemoral pain research retreat, manchester. Part 1: Terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br. J. Sports Med. 2016, 50, 839–843. [Google Scholar] [PubMed]
- Glaviano, N.R.; Baellow, A.; Saliba, S. Physical activity levels in individuals with and without patellofemoral pain. Phys. Ther. Sport 2017, 27, 12–16. [Google Scholar] [CrossRef]
- Rathleff, M.S.; Rathleff, C.R.; Olesen, J.L.; Rasmussen, S.; Roos, E.M. Is knee pain during adolescence a self-limiting condition? Prognosis of patellofemoral pain and other types of knee pain. Am. J. Sports Med. 2016, 44, 1165–1171. [Google Scholar] [CrossRef]
- Coburn, S.L.; Barton, C.J.; Filbay, S.R.; Hart, H.F.; Rathleff, M.S.; Crossley, K.M. Quality of life in individuals with patellofemoral pain: A systematic review including meta-analysis. Phys. Ther. Sport 2018, 33, 96–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, N.J.; Crossley, K.M. Young to middle-aged adults with persistent patellofemoral pain demonstrate similar pain, disability and knee-related quality of life as older adults with patellofemoral osteoarthritis. Osteoarthr. Cartil. 2019, 27, S220–S221. [Google Scholar] [CrossRef] [Green Version]
- Maclachlan, L.R.; Collins, N.J.; Matthews, M.L.G.; Hodges, P.W.; Vicenzino, B. The psychological features of patellofemoral pain: A systematic review. Br. J. Sports Med. 2017, 51, 732–742. [Google Scholar] [CrossRef] [Green Version]
- Collins, N.; Vicenzino, B.; Macri, E.; Crossley, K. Prevalence and factors associated with radiographic PFJ OA in young to middle-aged adults with chronic patellofemoral pain. J. Sci. Med. Sport 2015, 19, e85. [Google Scholar] [CrossRef]
- Hinman, R.S.; Lentzos, J.; Vicenzino, B.; Crossley, K.M. Is patellofemoral osteoarthritis common in middle-aged people with chronic patellofemoral pain? Arthritis Care Res. 2014, 66, 1252–1257. [Google Scholar] [CrossRef]
- Macri, E.M.; Neogi, T.; Tolstykh, I.; Widjajahakim, R.; Lewis, C.E.; Torner, J.C.; Nevitt, M.C.; Roux, M.; Stefanik, J.J. Relation of patellofemoral joint alignment, morphology, and radiographic osteoarthritis to frequent anterior knee pain: TheMOST study. Arthritis Care Res. 2019, 72, 1066–1073. [Google Scholar] [CrossRef]
- Smith, B.E.; Selfe, J.; Thacker, D.; Hendrick, P.; Bateman, M.; Moffatt, F.; Rathleff, M.S.; Smith, T.O.; Logan, P. Incidence and prevalence of patellofemoral pain: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0190892. [Google Scholar] [CrossRef] [Green Version]
- Hart, H.F.; Stefanik, J.J.; Wyndow, N.; Machotka, Z.; Crossley, K.M. The prevalence of radiographic and mri-defined patellofemoral osteoarthritis and structural pathology: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1195–1208. [Google Scholar] [CrossRef]
- Van Middelkoop, M.; Van Linschoten, R.; Berger, M.Y.; Koes, B.W.; Bierma-Zeinstra, S.M. Knee complaints seen in general practice: Active sport participants versus non-sport participants. BMC Musculoskelet. Disord. 2008, 9, 36. [Google Scholar] [CrossRef] [Green Version]
- Glaviano, N.R.; Kew, M.; Hart, J.M.; Saliba, S. Demographic and epidemiological trends in patellofemoral pain. Int. J. Sports Phys. 2015, 10, 281–290. [Google Scholar]
- Kastelein, M.; Luijsterburg, P.A.J.; Heintjes, E.M.; van Middelkoop, M.; Verhaar, J.A.N.; Koes, B.W.; Bierma-Zeinstra, S.M.A. The 6-year trajectory of non-traumatic knee symptoms (including patellofemoral pain) in adolescents and young adults in general practice: A study of clinical predictors. Br. J. Sports Med. 2015, 49, 400–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nimon, G.; Murray, D.; Sandow, M.; Goodfellow, J. Natural history of anterior knee pain: A 14-to 20-year follow-up of nonoperative management. J. Pediatric Orthop. 1998, 18, 118–122. [Google Scholar] [CrossRef]
- Thomas, M.J.; Wood, L.; Selfe, J.; Peat, G. Anterior knee pain in younger adults as a precursor to subsequent patellofemoral osteoarthritis: A systematic review. BMC Musculoskelet. Disord. 2010, 11, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utting, M.; Davies, G.; Newman, J. Is anterior knee pain a predisposing factor to patellofemoral osteoarthritis? Knee 2005, 12, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Wyndow, N.; Collins, N.; Vicenzino, B.; Tucker, K.; Crossley, K. Is there a biomechanical link between patellofemoral pain and osteoarthritis? A narrative review. Sports Med. 2016, 46, 1797–1808. [Google Scholar] [CrossRef] [PubMed]
- Duncan, R.; Peat, G.; Thomas, E.; Wood, L.; Hay, E.; Croft, P. How do pain and function vary with compartmental distribution and severity of radiographic knee osteoarthritis? Rheumatology 2008, 47, 1704–1707. [Google Scholar] [CrossRef] [Green Version]
- Hart, H.F.; Filbay, S.R.; Coburn, S.; Charlton, J.M.; Sritharan, P.; Crossley, K.M. Is quality of life reduced in people with patellofemoral osteoarthritis and does it improve with treatment? A systematic review, meta-analysis and regression. Disabil. Rehabil. 2019, 41, 2979–2993. [Google Scholar] [CrossRef]
- Lankhorst, N.; Damen, J.; Oei, E.; Verhaar, J.; Kloppenburg, M.; Bierma-Zeinstra, S.; van Middelkoop, M. Incidence, prevalence, natural course and prognosis of patellofemoral osteoarthritis: The cohort hip and cohort knee study. Osteoarthr. Cartil. 2017, 25, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Brand, C.A.; Harrison, C.; Tropea, J.; Hinman, R.S.; Britt, H.; Bennell, K. Management of osteoarthritis in general practice in australia. Arthritis Care Res. 2014, 66, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Lack, S.; Neal, B.; De Oliveira Silva, D.; Barton, C. How to manage patellofemoral pain—Understanding the multifactorial nature and treatment options. Phys. Ther. Sport 2018, 32, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Crossley, K.M.; Vicenzino, B.; Lentzos, J.; Schache, A.G.; Pandy, M.G.; Ozturk, H.; Hinman, R.S. Exercise, education, manual-therapy and taping compared to education for patellofemoral osteoarthritis: A blinded, randomised clinical trial. Osteoarthr. Cartil. 2015, 23, 1457–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. Oarsi guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- Willy, R.W.; Hoglund, L.T.; Barton, C.J.; Bolgla, L.A.; Scalzitti, D.A.; Logerstedt, D.S.; Lynch, A.D.; Snyder-Mackler, L.; McDonough, C.M.; Altman, R. Patellofemoral pain: Clinical practice guidelines linked to the international classification of functioning, disability and health from the academy of orthopaedic physical therapy of the american physical therapy association. J. Orthop. Sports Phys. Ther. 2019, 49, CPG1–CPG95. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Merchan, E.C. Evidence based conservative management of patello-femoral syndrome. Arch. Bone Jt. Surg. 2014, 2, 4–6. [Google Scholar]
- Castrogiovanni, P.; Trovato, F.M.; Loreto, C.; Nsir, H.; Szychlinska, M.A.; Musumeci, G. Nutraceutical supplements in the management and prevention of osteoarthritis. Int. J. Mol. Sci. 2016, 17, 2042. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C. Surgical treatment of isolated patellofemoral osteoarthritis. HSS J. 2014, 10, 79–82. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Merchan, E.C. The Present Situation of Patellofemoral Arthroplasty in the Management of Solitary Patellofemoral Osteoarthritis. Arch. Bone Jt. Surg. 2020, 8, 325–331. [Google Scholar]
- Barton, C.J.; Lack, S.; Hemmings, S.; Tufail, S.; Morrissey, D. The ’best practice guide to conservative management of patellofemoral pain’: Incorporating level 1 evidence with expert clinical reasoning. Br. J. Sports Med. 2015, 49, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.J.; Barton, C.J.; van Middelkoop, M.; Callaghan, M.J.; Rathleff, M.S.; Vicenzino, B.T.; Davis, I.S.; Powers, C.M.; Macri, E.M.; Hart, H.F.; et al. 2018 consensus statement on exercise therapy and physical interventions (orthoses, taping and manual therapy) to treat patellofemoral pain: Recommendations from the 5th international patellofemoral pain research retreat, gold coast, australia, 2017. Br. J. Sports Med. 2018, 52, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Heintjes, E.M.; Berger, M.; Bierma-Zeinstra, S.M.A.; Bernsen, R.M.D.; Verhaar, J.A.N.; Koes, B.W. Pharmacotherapy for patellofemoral pain syndrome. Cochrane Database Syst. Rev. 2004. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. Open Med. 2009, 3, e123–e130. [Google Scholar] [PubMed]
- Prospero International Prospective Register of Systematic Reviews. Available online: http://www.crd.york.ac.uk/prospero (accessed on 8 December 2017).
- Grelsamer, R.P. Patellar nomenclature: The Tower of Babel revisited. Clin. Orthop. Relat. Res. 2005, 436, 60–65. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Sterne, J.A.C.; Savović, J.; Page, M.J.; Hrobjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S.A. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10 (Suppl 1), 29–31. [Google Scholar]
- Collins, N.J.; Bisset, L.M.; Crossley, K.M.; Vicenzino, B. Efficacy of nonsurgical interventions for anterior knee pain: Systematic review and meta-analysis of randomized trials. Sports Med. 2012, 42, 31–49. [Google Scholar] [CrossRef] [Green Version]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar]
- Odgaard, A.; Madsen, F.; Kristensen, P.W.; Kappel, A.; Fabrin, J. The mark coventry award: Patellofemoral arthroplasty results in better range of movement and early patient-reported outcomes than TKA. Clin. Orthop. Relat. Res. 2018, 476, 87. [Google Scholar] [CrossRef] [Green Version]
- Kettunen, J.A.; Harilainen, A.; Sandelin, J.; Schlenzka, D.; Hietaniemi, K.; Seitsalo, S.; Malmivaara, A.; Kujala, U.M. Knee arthroscopy and exercise versus exercise only for chronic patellofemoral pain syndrome: A randomized controlled trial. BMC Med. 2007, 5, 38. [Google Scholar] [CrossRef] [Green Version]
- Kettunen, J.A.; Harilainen, A.; Sandelin, J.; Schlenzka, D.; Hietaniemi, K.; Seitsalo, S.; Malmivaara, A.; Kujala, U.M. Knee arthroscopy and exercise versus exercise only for chronic patellofemoral pain syndrome: 5-year follow-up. Br. J. Sports Med. 2012, 46, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Joseph, M.; Achten, J.; Parsons, N.; Costa, M. The PAT randomised clinical trial: Total knee arthroplasty versus patellofemoral arthroplasty in patients with severe arthritis of the patellofemoral joint. Bone Joint J. 2020, 102, 310–318. [Google Scholar] [CrossRef]
- Hart, J.M.; Kuenze, C.; Norte, G.; Bodkin, S.; Patrie, J.; Denny, C.; Hart, J.; Diduch, D.R. Prospective, randomized, double-blind evaluation of the efficacy of a single-dose hyaluronic acid for the treatment of patellofemoral chondromalacia. Orthop. J. Sport Med. 2019, 7, 2325967119854192. [Google Scholar] [CrossRef] [PubMed]
- Antich, T.J.; Randall, C.C.; Westbrook, R.A.; Morrissey, M.C.; Brewster, C.E. Physical therapy treatment of knee extensor mechanism disorders: Comparison of four treatment modalities. J. Orthop. Sports Phys. 1986, 8, 255–259. [Google Scholar] [CrossRef]
- Matoso, L.; Schelling, J.L.; Radi, I. Essai clinique contrôlé de la chloroquine dans la chondromalacie rotulienne. Med. Hyg. 1980, 38, 1205–1209. [Google Scholar]
- Örsçelik, A.; Yildiz, Y. Comparison of single and triple platelet rich plasma injections in the treatment of patellofemoral pain syndrome. Turk. Klin. J. Med Sci. 2015, 35, 78–87. [Google Scholar] [CrossRef]
- Raatikainen, T.; Väänänen, K.; Tamelander, G. Effect of glycosaminoglycan polysulfate on chondromalacia patellae: A placebo-controlled 1-year study. Acta Orthop. Scand. 1990, 61, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Suter, E.; Herzog, W.; De Souza, K.; Bray, R. Inhibition of the quadriceps muscles in patients with anterior knee pain. J. Appl. Biomech. 1998, 14, 360–373. [Google Scholar] [CrossRef]
- Pagenstert, G.; Wolf, N.; Bachmann, M.; Gravius, S.; Barg, A.; Hintermann, B.; Wirtz, D.C.; Valderrabano, V.; Leumann, A.G. Open lateral patellar retinacular lengthening versus open retinacular release in lateral patellar hypercompression syndrome: A prospective double-blinded comparative study on complications and outcome. Arthrosc. J. Arthrosc. Relat. Surg. 2012, 28, 788–797. [Google Scholar] [CrossRef]
- Owens, B.D.; Stickles, B.J.; Balikian, P.; Busconi, B.D. Prospective analysis of radiofrequency versus mechanical debridement of isolated patellar chondral lesions. Arthrosc. J. Arthrosc. Relat. Surg. 2002, 18, 151–155. [Google Scholar] [CrossRef]
- Hejgaard, N.; Watt-Boolsen, S. The effect of anterior displacement of the tibial tuberosity in idiopathic chondromalacia patellae: A prospective randomized study. Acta Orthop. Scand. 1982, 53, 135–139. [Google Scholar] [CrossRef]
- Darracott, J. Treatment of the painful knee fulfilling diagnostic criteria for ’chondromalacia patellae’. Curr. Med. Res. Opin. 1973, 1, 412–422. [Google Scholar] [CrossRef]
- Bentley, G.; Leslie, I.J.; Fischer, D. Effect of aspirin treatment on chondromalacia patellae. Ann. Rheum. Dis. 1981, 40, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Fulkerson, J.P.; Folcik, M.A. Comparison of diflunisal and naproxen for relief of anterior knee pain. Clin. Ther. 1986, 9, 59–61. [Google Scholar] [PubMed]
- Martí-Bonmatí, L.; Sanz-Requena, R.; Rodrigo, J.L.; Alberich-Bayarri, Á.; Carot, J.M. Glucosamine sulfate effect on the degenerated patellar cartilage: Preliminary findings by pharmacokinetic magnetic resonance modeling. Eur. Radiol. 2009, 19, 1512–1518. [Google Scholar] [CrossRef]
- Singer, B.J.; Silbert, P.L.; Song, S.; Dunne, J.W.; Singer, K.P. Treatment of refractory anterior knee pain using botulinum toxin type a (dysport) injection to the distal vastus lateralis muscle: A randomised placebo controlled crossover trial. Br. J. Sports Med. 2011, 45, 640–645. [Google Scholar] [CrossRef] [Green Version]
- Kannus, P.; Natri, A.; Niittymäki, S.; Järvinen, M. Effect of intraarticular glycosaminoglycan polysulfate treatment on patellofemoral pain syndrome. A prospective, randomized double-blind trial comparing glycosaminoglycan polysulfate with placebo and quadriceps muscle exercises. Arthritis Rheum. Offic. J. Am. Coll. Rheumatol. 1992, 35, 1053–1061. [Google Scholar] [CrossRef]
- Kannus, P.; Natri, A.; Paakkala, T.; JÄrvinen, M. An outcome study of chronic patellofemoral pain syndrome. Seven-year follow-up of patients in a randomized, controlled trial. J. Bone Joint Surg. 1999, 81, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Nakhostin-Roohi, B.; Khoshkhahesh, F.; Bohlooli, S. Effect of virgin olive oil versus piroxicam phonophoresis on exercise-induced anterior knee pain. Avicenna J. Phytomedicine 2016, 6, 535. [Google Scholar]
- O’Neill, D.B. Open lateral retinacular lengthening compared with arthroscopic release. A prospective, randomized outcome study. J. Bone Joint Surg. 1997, 79, 1759–1769. [Google Scholar]
- Nüesch, E.; Trelle, S.; Reichenbach, S.; Rutjes, A.W.S.; Tschannen, B.; Altman, D.G.; Egger, M.; Jüni, P. Small study effects in meta-analyses of osteoarthritis trials: Meta-epidemiological study. BMJ 2010, 341, c3515. [Google Scholar] [CrossRef] [Green Version]
- Tarassoli, P.; Punwar, S.; Khan, W.; Johnstone, D. Suppl 2: Patellofemoral arthroplasty: A systematic review of the literature. Open Orthop. J. 2012, 6, 340. [Google Scholar] [CrossRef] [Green Version]
- Parratte, S.; Ollivier, M.; Lunebourg, A.; Abdel, M.P.; Argenson, J.N. Long-term results of compartmental arthroplasties of the knee: Long term results of partial knee arthroplasty. Bone Jt. J. 2015, 97, 9–15. [Google Scholar] [CrossRef]
- Bedson, J.; Croft, P.R. The discordance between clinical and radiographic knee osteoarthritis: A systematic search and summary of the literature. BMC Musculoskelet. Disord. 2008, 9, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Heijden, R.A.; de Kanter, J.L.; Bierma-Zeinstra, S.M.; Verhaar, J.A.; van Veldhoven, P.L.; Krestin, G.P.; Oei, E.H.; van Middelkoop, M. Structural abnormalities on magnetic resonance imaging in patients with patellofemoral pain a cross-sectional case-control study. Am. J. Sports Med. 2016, 44, 2339–2346. [Google Scholar] [CrossRef]
- Stefanik, J.J.; Neogi, T.; Niu, J.; Roemer, F.W.; Segal, N.A.; Lewis, C.E.; Nevitt, M.; Guermazi, A.; Felson, D.T. The diagnostic performance of anterior knee pain and activity-related pain in identifying knees with structural damage in the patellofemoral joint: The multicenter osteoarthritis study. J. Rheumatol. 2014, 41, 1695–1702. [Google Scholar] [CrossRef] [Green Version]
- Barton, C.J.; Crossley, K.M.; Macri, E.M. Should we consider changing traditional physiotherapy treatment of patellofemoral pain based on recent insights from the literature? Br. J. Sports Med. 2018, 52, 1546–1547. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Egger, M. Regression methods to detect publication and other bias in meta-analysis. In Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments; Rothstein, H.R., Sutton, A.J., Borenstein, M., Eds.; John Wiley & Sons, Ltd.: West Sussex, UK, 2005; pp. 99–110. [Google Scholar]
- Karlsson, J.; Sward, L.; Lansinger, O. Bad results after anterior advancement of the tibial tubercle for patello-femoral pain syndrome. Arch. Orthop. Trauma Surg. 1992, 111, 195–197. [Google Scholar] [CrossRef]
- Van der Heijden, R.A.; Lankhorst, N.E.; Van Linschoten, R.; Bierma-Zeinstra, S.; Van Middelkoop, M. Exercise for treating patellofemoral pain syndrome. An abridged version of cochrane systematic review. Eur. J. Phys. Rehabil. Med. 2015, 52, 110–133. [Google Scholar]
- Thomson, C.; Krouwel, O.; Kuisma, R.; Hebron, C. The outcome of hip exercise in patellofemoral pain: A systematic review. Man. Ther. 2016, 26, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Lack, S.; Barton, C.; Sohan, O.; Crossley, K.; Morrissey, D. Proximal muscle rehabilitation is effective for patellofemoral pain: A systematic review with meta-analysis. Br. J. Sports Med. 2015, 49, 1365–1376. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| (Patellofemoral Pain Syndrome/OR Chondromalacia Patellae/OR ((Patellofemoral Joint/OR patella/) AND (osteoarthritis/OR osteoarthritis, knee/OR pain/OR Joint Diseases/OR Cartilage Diseases/)) OR Chondromalacia Patellae/OR (((femoropatell* OR patell* OR retropatell*) ADJ6 (pain* OR osteoarthrit* OR osteo-arthrit* OR arthralgi* OR syndrome* OR Chondromalac* OR dysfunction* OR chondropath*)) OR ((femoropatell* OR patell* OR retropatell*) ADJ6 (degenerat*) ADJ6 (arthrit* OR cartilag*)) OR (anter* ADJ3 knee ADJ3 pain*) OR ((lateral* OR odd) ADJ3 (compress* OR facet OR pressure*) ADJ3 syndrome*)).ab,ti,kw) AND (Exp Controlled clinical trial/OR “Double-Blind Method”/OR “Single-Blind Method”/OR “Random Allocation”/OR (random* OR factorial* OR crossover* OR cross over* OR placebo* OR ((doubl* OR singl*) ADJ blind*) OR assign* OR allocat* OR volunteer* OR trial OR groups).ab,ti.) NOT (Animals/NOT Humans/) |
| First Author Year | Sample Randomized n | Sample Completed n | Women % (n) | Age Mean (SD) y | BMI Mean (SD) kg/m2 | Height Mean (SD) cm | Weight Mean (SD) kg | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pharmaceutical and Nutraceutical | Int | Cont | Int | Cont | Int | Cont | Int | Cont | Int | Cont | Int | Cont | |
| Hart 2019 [44] | 86 | 42 | 38 | 76% (34) | 76% (31) | 26.0 (7.0) | 28.1 (8.4) | 26.4 (5.3) | 25.8 (5.1) | 168.9 (9.2) | 168.3 (8.6) | 75.7 (16.6) | 73.5 (17.6) |
| Nakhostin-Roohi 2016 [60] | 93 | 31 | 31 * 31 * | 100% (93) | 26.0 (8.9) | 26.2 (10.0) 27.2 (9.5) | NR | NR NR | 160.7 (11.1) | 164.2 (7.2) 1.6 (8.9) | 59.3 (9.5) | 58.2 (11.1) 61.0 (12.8) | |
| Örsçelik 2015 [47] | 30 | 10 | 20 | 40% (4) | 35% (7) | 28.7 (6.0) | 27.2 (5.7) | 24.2 (3.4) | 24.0 (3.0) | 170.8 (6.6) | 174.5 (7.9) | 71.1 (12.5) | 73.4 (12.8) |
| Singer 2011 [57] | 24 | 14 | 10 | 57% (8) | 90% (9) | 31.5 (r15,48) | 27.4 (r18,44) | NR | NR | NR | NR | NR | NR |
| Marti-Bonmati 2009 [56] | 20 | 10 | 6 | 63% (10) | 39 (18) | NR | NR | NR | NR | NR | NR | ||
| Kannus 1992 [58] and | 5 | 16 | 16 † 17 † | 53% (28) | 27 (9) | NR | NR NR | NR | NR NR | NR | NR NR | ||
| 1999 [59] | As above | 45 | aa | aa | aa | aa | aa | ||||||
| Suter 1998 [49] | 42 | 19 | 17 | 31% (13) | 35.6 (8.4) | NR | NR | NR | NR | NR | NR | ||
| Raitikainen 1990 [48] | 31 | 14 | 15 | 29% (4) | 20% (3) | 29.1 (7.7) | 30.2 (6.6) | 24.6 (3.3) | 25.1 (3.2) | 173.6 (9.0) | 177.0 (8.8) | 74.8 (14.0) | 78.9 (13.9) |
| Fulkerson 1986 [55] | 56 | 20 | 16 | 78% (28) | 32.3 (??) | NR | NR | NR | NR | NR | NR | ||
| Antich 1986 [45] | 64 (86 k) | 9 k | 21 k ‡ 13 k ‡ 16 k ‡ | NR | NR | NR | NR | NR | NR | NR | NR | ||
| Bentley 1981 [54] | 30 | 16 | 13 | 72% (21) | 25 (??) | NR | NR | NR | NR | NR | NR | ||
| Matoso 1980 [46] | 33 | 12 | 10 | 53% (10) | 64% (9) | 28 (r16,50) | 30 (r16,46) | NR | NR | NR | NR | NR | NR |
| Darracott 1973 [53] | 43 | 23 | 20 | 0% (0) | 15% (3) | 22.9 (4.4) | 20.8 (3.3) | NR | NR | NR | NR | NR | NR |
| Surgical | |||||||||||||
| Joseph 2020 [43] | 64 | 31 | 29 | 71% (22) | 90% (26) | 64.7 (10.5) | 64.4 (12.8) | 28.9 (6.7) | 29.2 (4.2) | NR | NR | NR | NR |
| Odgaard 2018 [40] | 100 | 46 | 47 | 77% (77) | 64 (8.9) | NR | NR | NR | |||||
| Pagenstert 2012 [50] | (28) | 14 | 14 | 79% (11) | 71% (10) | 47.6 (9.9) | 48.0 (11.6) | NR | NR | NR | NR | NR | NR |
| Kettunen 2007 [41] | 56 | 27 | 25 | 61% (17) | 64% (18) | 28.4 (7.5) | 28.4 (5.6) | 24.1 (3.3) | 23.8 (3.6) | 171.7 (10.2) | 172.4 (9.6) | 69.0 (19.3) | 71.4 (15.1) |
| 2012 [42] | As above | 24 | 20 | aa | aa | aa | aa | aa | aa | aa | aa | aa | aa |
| Owens 2002 [51] | 48 | 20 | 19 | 100% (20) | 100% (19) | 36.9 (r 30,45) | 37.5 (r 30,45) | NR | NR | NR | NR | NR | NR |
| O’Neill 1997 [61] | 91 | 43 | 43 | 60% (26) | 58% (25) | 27.2 M 18 (r13,56) W 33 (r15,47) | 28.7 M 22 (r13,33) W 34 (r14,59) | NR | NR | NR | NR | NR | NR |
| Hejgaard 1982 [52] | 42 | 20 | 22 | 50% (10) | 59% (13) | 28 (r18,38) | 32 (r19,50) | NR | NR | NR | NR | NR | NR |
| First Author Year | Intervention | Control | Outcome | Short Term * <6 Weeks | Medium Term 7 Weeks–6 Months | Long Term, >6 Months | Adverse Events |
|---|---|---|---|---|---|---|---|
| Pharmaceutical and Nutraceutical | SMD (95% CI) | SMD (95% CI) | SMD (95% CI) | ||||
| Hart 2019 [44] | Hyaluronic acid IA inj | Placebo | VAS single leg squat | −0.3 (−0.7, 0.2) | −0.3 (−0.7, 0.2) | NR | |
| KOOS | −0.9 (−1.3, −0.4) | −0.6 (−1.0,−0.2) | |||||
| AKPS | −0.6 (−1.1, −0.2) | −0.5 (−1.0,−0.1) | |||||
| Tegner | −0.3 (−0.7, 0.1) | −0.2 (−0.6, 0.3) | |||||
| Knee extension | 0.0 (−0.4, 0.4) | −0.1 (−0.6, 0.3) | |||||
| Knee ratio | 0.0 (−0.4, 0.4) | −0.3 (−0.7, 0.2) | |||||
| Nakhostin-Roohi 2016 [60] | Olive oil (phonophoresis) | Piroxicam (phonophoresis) | WOMAC Pain | NR | NR | ||
| WOMAC Stiffness | NR | ||||||
| WOMAC Physical Function | NR | ||||||
| Örsçelik 2015 [47] | PRP, 3 IA inj | PRP, 1 inj | AKPS | 1.1 (0.3, 2.0) | Some localized pain for several weeks after injections (numbers/arm not reported) | ||
| Quadriceps peak torque | 0.1 (−0.7, 0.8) | ||||||
| Singer 2011 [57] | Botox IM inj | Placebo | AKPS | 0.9 (0.1, 1.8) | 6 (43%) slight distal thigh asymmetry; few (numbers and arm NR): temporary bruising or pain last up to several days. | ||
| Pain stairs | 0.3 (−0.5, 1.1) | ||||||
| Pain squat | 1.1 (0.2, 1.9) | ||||||
| Pain kneel | 1.4 (0.5, 2.3) | ||||||
| Pain walk | −0.9 (−1.7, 0.0) | ||||||
| Marti-Bonmati 2009 [56] | Glucosamine | Acetaminophen | AKSS | 2.5 (1.1, 3.9) | NR | ||
| VAS (task not specified) | 4.1 (2.2, 6.0) | ||||||
| Kannus 1992 and 1999 [58,59] | GAGPS IA inj | Placebo | No pain, 1 leg jump | RR 0.9 (0.4, 1.8) | RR 0.8 (0.5, 1.3) | NR | 0 intervention vs. 1 control reactive synovitis to injection (discontinued treatment) |
| No pain, 25 squats | RR 1.1 (0.7, 1.6) | RR 1.1 (0.7, 1.6) | |||||
| Excellent rating | RR 0.9 (0.5, 1.8) | RR 1.4 (0.8, 2.4) | |||||
| Return full activity | RR 1.4 (0.8, 2.4) | RR 1.4 (0.9, 2.0) | |||||
| Lysholm | 0.2 (−0.5,0.8) | 0.2 (−0.5, 0.9) | |||||
| Tegner | 0.4 (−0.3, 1.1) | −0.1 (−0.6, 0.8) | |||||
| Pain with activity | 0.2 (−0.9, 0.5) | 0.0 (−0.7, 0.7) | |||||
| Suter 1998 [49] | Naproxen | Placebo | Pain resisted extension | 0.5 (−0.2, 1.1) | NR | ||
| Raatikainen 1990 [48] | GAGPS IM inj | Placebo | Pain down stairs | −0.1 (−0.6, 0.9) | 0.3 (−0.4, 1.1) | 1.6 (0.8, 2.5) | 1 intervention, sweating and dizziness after 4th injection, resolved and continued |
| Pain squat | 0.3 (−0.4, 1.1) | 0.3 (−0.4, 1.1) | 1.3 (0.5, 2.2) | ||||
| Physician ”Improved” | RR 1.4 (0.6, 3.4) | RR 1.7 (0.5, 6.1) | RR 3.6 (1.2, 10.4) | ||||
| Hindrance—sport | 0.4 (−0.3, 1.2) | 0.5 (−0.3, 1.2) | 0.8 (0.1, 1.6) | ||||
| Hindrance—life | −0.2 (−0.9, 0.6) | 0.3 (−0.4, 1.1) | 0.7 (−0.0, 1.5) | ||||
| Fulkerson 1986 [55] | Diflunisal | Naproxen | Significant pain relief | RR 0.9 (0.5, 1.5) | 11 (55%) diflunisal (headache, gastric distress, etc.) vs. 7 (44%) naproxen (drowsiness, headache, etc.) | ||
| Antich 1986 [45] | Hexadrol (phonophoresis) | Ultrasound plus ice | Subjective improvement | [RR 0.7 (0.2, 2.2)] † | NR | ||
| Bentley 1981 [54] | Palaprin | Placebo | Global improvement | RR 1.2 (0.4, 3.4) | NR | ||
| Matoso 1980 [46] | Chloroquine | Placebo | Spontaneous pain | NR | 15 (79%) intervention (6 discontinued treatment) vs. 4 (29%) controls: visual trouble, digestive trouble, headache, vertigo | ||
| Darracott 1973 [53] | Nandrolone phenylpropionate inj | Placebo | Improved | RR 8.7 (2.3, 32.7) | NR | ||
| Surgical | |||||||
| Joseph 2020 [43] | Patellofemoral arthroplasty | Total knee arthroplasty | WOMAC (1y): | Superficial infections: 4 PFA, 5 TKA—all treated with antibiotics. 4 TKA required further interventions: 1 arthroscopic facetectomy, 1 manipulation under anesthesia, 2 aspiration/steroid injection | |||
| Pain | −0.3 (−0.8, 0.2) | ||||||
| Stiffness | −0.2 (−0.7, 0.3) | ||||||
| Function | −0.1 (−0.6, 0.4) | ||||||
| AKSS (1y): | |||||||
| Knee | 0.1 (−0.5, 0.6) | ||||||
| Function | −0.2 (−0.4, 0.7) | ||||||
| UCLA (1y) | 0.3 (−0.2, 0.8) | ||||||
| EQ5D3L (5y) | 0.2 (−0.4, 0.8) | ||||||
| OKS (5y) | −0.1 (−0.8, 0.5) | ||||||
| Pain-free years (5y) | −0.6 (−1.2, 0.1) | ||||||
| Satisfied (5y) | RR 0.9 (0.6, 1.2) | ||||||
| Odgaard 2018 [40] | Patellofemoral arthroplasty | Total knee arthroplasty | KOOS: | Intervention: 2 deaths unrelated to surgery, 2 revisions (1 of trochlear component, 1 to TKA), 2 other surgical procedures; control: 5 other surgical procedures | |||
| Pain | 0.4 (−0.0, 0.8) ‡ | 0.4 (−0.0, 0.8) | 0.1 (−0.3, 0.5) | ||||
| Symptoms | 0.6 (0.2, 1.0) | 0.8 (0.4, 1.2) | 0.5 (0.1, 0.9) | ||||
| ADL | 0.2 (−0.2, 0.6) | 0.1 (−0.3, 0.5) | −0.1 (−0.6, 0.3) | ||||
| SPR | 0.3 (−0.1, 0.7) | 0.3 (−0.1, 0.7) | 0.3 (−0.2, 0.7) | ||||
| QOL | 0.0 (−0.4, 0.4) | 0.3 (−0.1, 0.7) | 0.1 (−0.4, 0.5) | ||||
| SF-36 Bodily Pain | 0.5 (0.1, 0.9) | 0.4 (0.0, 0.8) | 0.3 (−0.1, 0.7) | ||||
| Pagenstert 2012 [50] | Open lateral retinacular lengthening | Open lateral retinacular release | AKPS | 0.5 (−0.2, 1.3) | 0.8 (0.1, 1.6) | No surgical complications. At 2 years, recurrence of symptoms in 1 lengthening and 2 release; and over-release in 5 release arm | |
| Quadriceps atrophy | 1.2 (0.4, 2.0) | 1.6 (0.7, 2.5) | |||||
| Kettunen 2007 and 2012 [41,42] | Arthroscopy plus exercise | Exercise alone | AKPS | −0.0 (−0.6, 0.5) | Intervention: 1 delayed exercise due to pain, 1 refused exercise after surgery; 3 controls had arthroscopic surgery | ||
| Pain down stairs | −0.1 (−0.7, 0.4) | ||||||
| Pain up stairs | −0.0 (−0.5, 0.5) | ||||||
| Pain sit to stand | 0.2 (−0.3, 0.7) | ||||||
| Owens 2002 [51] | Debridement, radiofrequency probe | Debridement, standard shaver | Fulkerson-Shea | 1.7 (0.9, 2.4) | NR | ||
| O’Neill 1997 [61] | Open lateral retinacular lengthening | Arthroscopic lateral retinacular release | Tegner | RR 1.1 (1.0, 1.2) | Intervention: 1 stitch abscess; 1 skin incision keloid; 1 unable to achieve 90° knee flexion; control: 1 iliotibial band contracture, 1 hematoma, 1 superficial infection, 1 hematoma with infection after self-draining | ||
| Quadriceps open chain strength deficit | RR 1.1 (0.8, 1.6) | ||||||
| Quadriceps atrophy | RR 1.2 (0.9, 1.5) | ||||||
| Knee score (modified Lysholm) | NR | ||||||
| Hejgaard 1982 [52] | Anterior displacement of tibial tuberosity plus debridement | Debridement | Surgeon, Good to Excellent | RR 2.6 (1.2, 5.4) | Intervention: 2 (10%) effusion, 2 (10%) thromboembolism; control: 5 effusion (23%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macri, E.M.; Hart, H.F.; Thwaites, D.; Barton, C.J.; Crossley, K.M.; Bierma-Zeinstra, S.M.A.; van Middelkoop, M. Medical Interventions for Patellofemoral Pain and Patellofemoral Osteoarthritis: A Systematic Review. J. Clin. Med. 2020, 9, 3397. https://doi.org/10.3390/jcm9113397
Macri EM, Hart HF, Thwaites D, Barton CJ, Crossley KM, Bierma-Zeinstra SMA, van Middelkoop M. Medical Interventions for Patellofemoral Pain and Patellofemoral Osteoarthritis: A Systematic Review. Journal of Clinical Medicine. 2020; 9(11):3397. https://doi.org/10.3390/jcm9113397
Chicago/Turabian StyleMacri, Erin M., Harvi F. Hart, David Thwaites, Christian J. Barton, Kay M. Crossley, Sita M.A. Bierma-Zeinstra, and Marienke van Middelkoop. 2020. "Medical Interventions for Patellofemoral Pain and Patellofemoral Osteoarthritis: A Systematic Review" Journal of Clinical Medicine 9, no. 11: 3397. https://doi.org/10.3390/jcm9113397