
Analytical Performance of the Commercial MucorGenius® Assay as Compared to an In-House qPCR Assay to Detect Mucorales DNA in Serum Specimens


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Serum Samples
2.2. Specificity Study Using Spiked Serum Samples
2.3. Statistical Analyses
2.4. Ethical Statement
3. Results
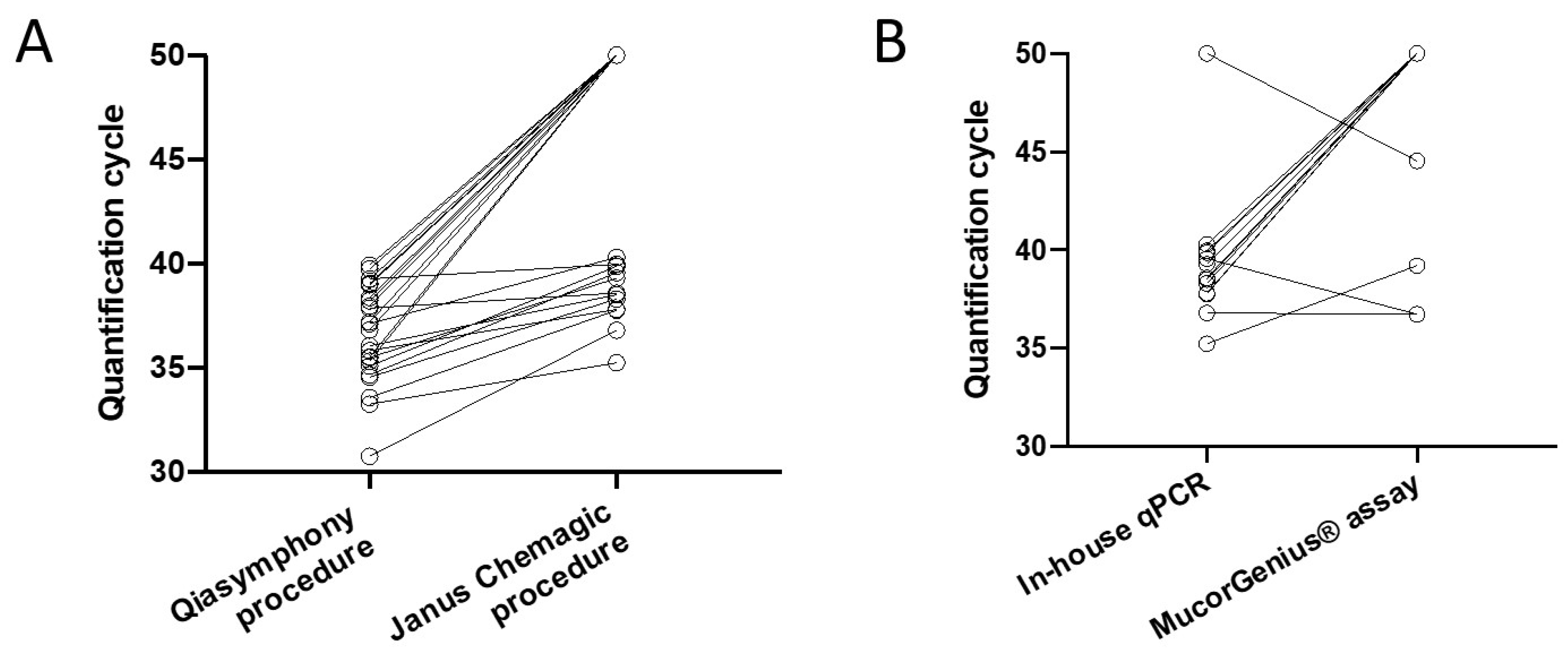
3.1. Comparison of qPCR Assays Based on qPCR Positive Serum Samples from Probable and Proven Mucormycosis Patients
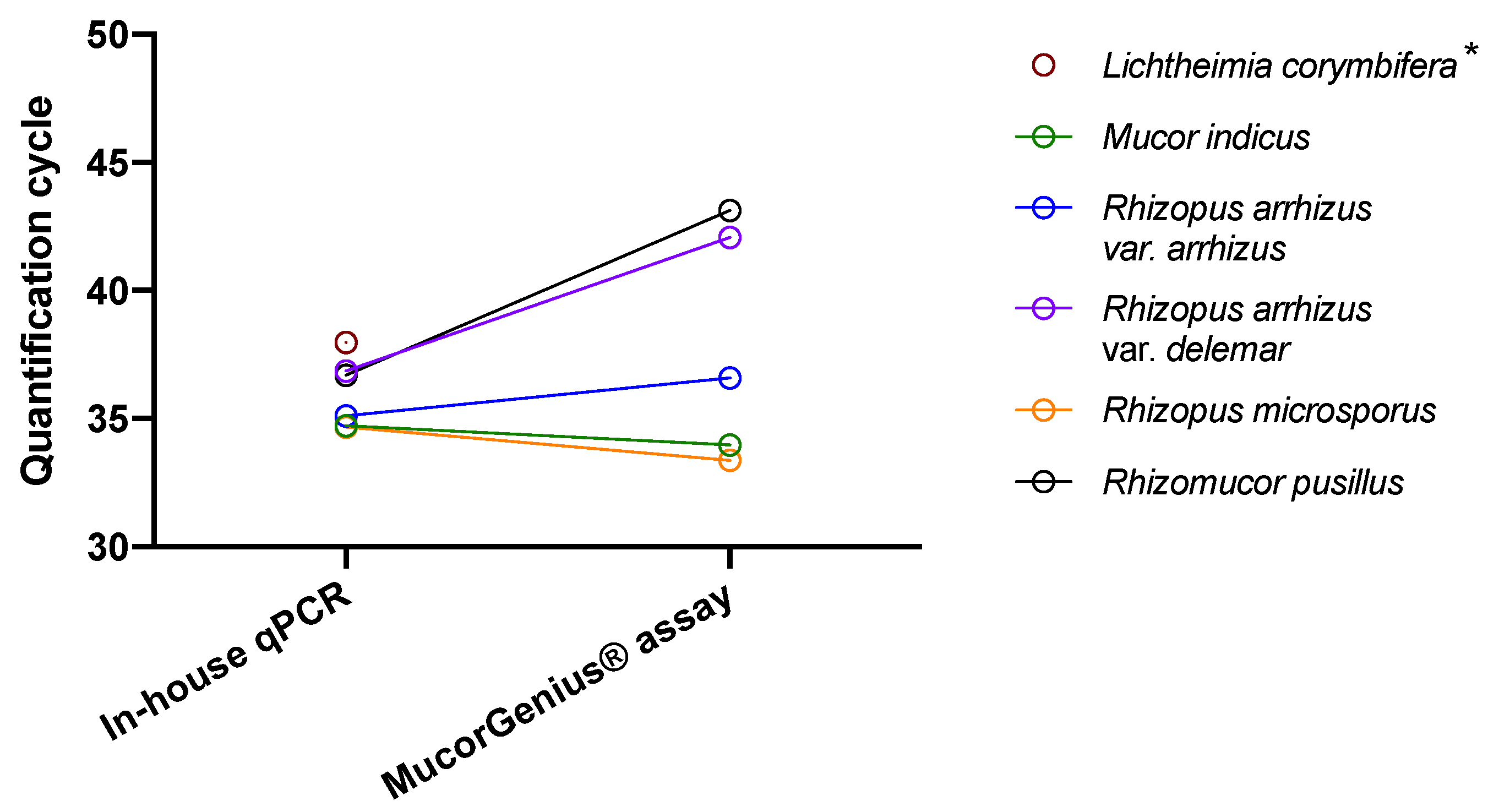
3.2. Comparison of qPCR Assays Based on Spiked Serum
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia-Hermoso, D.; Alanio, A.; Lortholary, O.; Dromer, F. Agents of Systemic and Subcutaneous Mucormycosis and Entomophthoromycosis. In Manual of Clinical Microbiology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2020; pp. 2087–2108. [Google Scholar] [CrossRef]
- Bretagne, S.; Sitbon, K.; Desnos-Ollivier, M.; Garcia-Hermoso, D.; Letscher-Bru, V.; Cassaing, S.; Millon, L.; Morio, F.; Gangneux, J.-P.; Hasseine, L.; et al. Active Surveillance Program to Increase Awareness on Invasive Fungal Diseases: The French RESSIF Network (2012 to 2018). Mbio 2022, 13, e00920-22. [Google Scholar] [CrossRef] [PubMed]
- Chamilos, G.; Lewis, R.E.; Kontoyiannis, D.P. Delaying Amphotericin B–Based Frontline Therapy Significantly Increases Mortality among Patients with Hematologic Malignancy Who Have Zygomycosis. Clin. Infect. Dis. 2008, 47, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Lackner, M.; Caramalho, R.; Lass-Flrl, C. Laboratory Diagnosis of Mucormycosis: Current Status and Future Perspectives. Future Microbiol. 2014, 9, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Pickering, J.W.; Sant, H.W.; Bowles, C.A.P.; Roberts, W.L.; Woods, G.L. Evaluation of a (1→3)-β-d-Glucan Assay for Diagnosis of Invasive Fungal Infections. J. Clin. Microbiol. 2005, 43, 5957–5962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millon, L.; Caillot, D.; Berceanu, A.; Bretagne, S.; Lanternier, F.; Morio, F.; Letscher-Bru, V.; Dalle, F.; Denis, B.; Alanio, A.; et al. Evaluation of Serum Mucorales Polymerase Chain Reaction (PCR) for the Diagnosis of Mucormycoses: The MODIMUCOR Prospective Trial. Clin. Infect. Dis. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Millon, L.; Herbrecht, R.; Grenouillet, F.; Morio, F.; Alanio, A.; Letscher-Bru, V.; Cassaing, S.; Chouaki, T.; Kauffmann-Lacroix, C.; Poirier, P.; et al. Early Diagnosis and Monitoring of Mucormycosis by Detection of Circulating DNA in Serum: Retrospective Analysis of 44 Cases Collected through the French Surveillance Network of Invasive Fungal Infections (RESSIF). Clin. Microbiol. Infect. 2016, 22, 810.e1–810.e8. [Google Scholar] [CrossRef] [Green Version]
- Park, B.J.; Pappas, P.G.; Wannemuehler, K.A.; Alexander, B.D.; Anaissie, E.J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; Brumble, L.M.; Freifeld, A.G.; et al. Invasive Non-Aspergillus Mold Infections in Transplant Recipients, United States, 2001–2006. Emerg. Infect. Dis. 2011, 17, 1855–1864. [Google Scholar] [CrossRef]
- Lanternier, F.; Dannaoui, E.; Morizot, G.; Elie, C.; Garcia-Hermoso, D.; Huerre, M.; Bitar, D.; Dromer, F.; Lortholary, O.; Group, F.M.S. A Global Analysis of Mucormycosis in France: The RetroZygo Study (2005–2007). Clin. Infect. Dis. 2012, 54, S35–S43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legrand, M.; Gits-Muselli, M.; Boutin, L.; Garcia-Hermoso, D.; Maurel, V.; Soussi, S.; Benyamina, M.; Ferry, A.; Chaussard, M.; Hamane, S.; et al. Detection of Circulating Mucorales DNA in Critically Ill Burn Patients: Preliminary Report of a Screening Strategy for Early Diagnosis and Treatment. Clin. Infect. Dis. 2016, 63, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Mercier, T.; Reynders, M.; Beuselinck, K.; Guldentops, E.; Maertens, J.; Lagrou, K. Serial Detection of Circulating Mucorales DNA in Invasive Mucormycosis: A Retrospective Multicenter Evaluation. J. Fungi 2019, 5, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2019, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Alanio, A.; Menotti, J.; Gits-Muselli, M.; Hamane, S.; Denis, B.; Rafoux, E.; de la Tour, R.P.; Touratier, S.; Bergeron, A.; Guigue, N.; et al. Circulating Aspergillus fumigatus DNA Is Quantitatively Correlated to Galactomannan in Serum. Front. Microbiol. 2017, 8, 2040. [Google Scholar] [CrossRef] [Green Version]
- Alanio, A.; Garcia-Hermoso, D.; Mercier-Delarue, S.; Lanternier, F.; Gits-Muselli, M.; Menotti, J.; Denis, B.; Bergeron, A.; Legrand, M.; Lortholary, O.; et al. Molecular Identification of Mucorales in Human Tissues: Contribution of PCR Electrospray-Ionization Mass Spectrometry. Clin. Microbiol. Infect. 2015, 21, 594.e1–594.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guegan, H.; Iriart, X.; Bougnoux, M.-E.; Berry, A.; Robert-Gangneux, F.; Gangneux, J.-P. Evaluation of MucorGenius® Mucorales PCR Assay for the Diagnosis of Pulmonary Mucormycosis. J. Infect. 2020, 81, 311–317. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Barnes, R.A.; Springer, J.; Klingspor, L.; Cuenca-Estrella, M.; Morton, C.O.; Lagrou, K.; Bretagne, S.; Melchers, W.J.G.; Mengoli, C.; et al. Clinical Performance of Aspergillus PCR for Testing Serum and Plasma: A Study by the European Aspergillus PCR Initiative. J. Clin. Microbiol. 2015, 53, 2832–2837. [Google Scholar] [CrossRef] [Green Version]
- Dellière, S.; Gits-Muselli, M.; White, P.L.; Mengoli, C.; Bretagne, S.; Alanio, A. Quantification of Pneumocystis jirovecii: Cross-Platform Comparison of One qPCR Assay with Leading Platforms and Six Master Mixes. J. Fungi 2019, 6, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gits-Muselli, M.; White, P.L.; Mengoli, C.; Chen, S.; Crowley, B.; Dingemans, G.; Fréalle, E.; Gorton, R.L.; Guiver, M.; Hagen, F.; et al. The Fungal PCR Initiative’s Evaluation of in-House and Commercial Pneumocystis Jirovecii QPCR Assays: Toward a Standard for a Diagnostics Assay. Med. Mycol. 2019, 58, 779–788. [Google Scholar] [CrossRef]
- Rocchi, S.; Scherer, E.; Mengoli, C.; Alanio, A.; Botterel, F.; Bougnoux, M.E.; Bretagne, S.; Cogliati, M.; Cornu, M.; Dalle, F.; et al. Interlaboratory Evaluation of Mucorales PCR Assays for Testing Serum Specimens: A Study by the Fungal PCR Initiative and the Modimucor Study Group. Med. Mycol. 2020, 59, 126–138. [Google Scholar] [CrossRef]
- Springer, J.; Goldenberger, D.; Schmidt, F.; Weisser, M.; Wehrle-Wieland, E.; Einsele, H.; Frei, R.; Löffler, J. Development and Application of Two Independent Real-Time PCR Assays to Detect Clinically Relevant Mucorales Species. J. Med. Microbiol. 2016, 65, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Lengerova, M.; Racil, Z.; Hrncirova, K.; Kocmanova, I.; Volfova, P.; Ricna, D.; Bejdak, P.; Moulis, M.; Pavlovsky, Z.; Weinbergerova, B.; et al. Rapid Detection and Identification of Mucormycetes in Bronchoalveolar Lavage Samples from Immunocompromised Patients with Pulmonary Infiltrates by Use of High-Resolution Melt Analysis. J. Clin. Microbiol. 2014, 52, 2824–2828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alanio, A.; Bretagne, S. Difficulties with Molecular Diagnostic Tests for Mould and Yeast Infections: Where Do We Stand? Clin. Microbiol. Infect. 2014, 20 (Suppl. 6), 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghelfenstein-Ferreira, T.; Verdurme, L.; Alanio, A. Analytical Performance of the Commercial MucorGenius® Assay as Compared to an In-House qPCR Assay to Detect Mucorales DNA in Serum Specimens. J. Fungi 2022, 8, 786. https://doi.org/10.3390/jof8080786
Ghelfenstein-Ferreira T, Verdurme L, Alanio A. Analytical Performance of the Commercial MucorGenius® Assay as Compared to an In-House qPCR Assay to Detect Mucorales DNA in Serum Specimens. Journal of Fungi. 2022; 8(8):786. https://doi.org/10.3390/jof8080786
Chicago/Turabian StyleGhelfenstein-Ferreira, Théo, Laura Verdurme, and Alexandre Alanio. 2022. "Analytical Performance of the Commercial MucorGenius® Assay as Compared to an In-House qPCR Assay to Detect Mucorales DNA in Serum Specimens" Journal of Fungi 8, no. 8: 786. https://doi.org/10.3390/jof8080786