“Balancing Expectations with Actual Realities”: Conversations with Clinicians and Scientists in the First Year of a High-Risk Childhood Cancer Precision Medicine Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
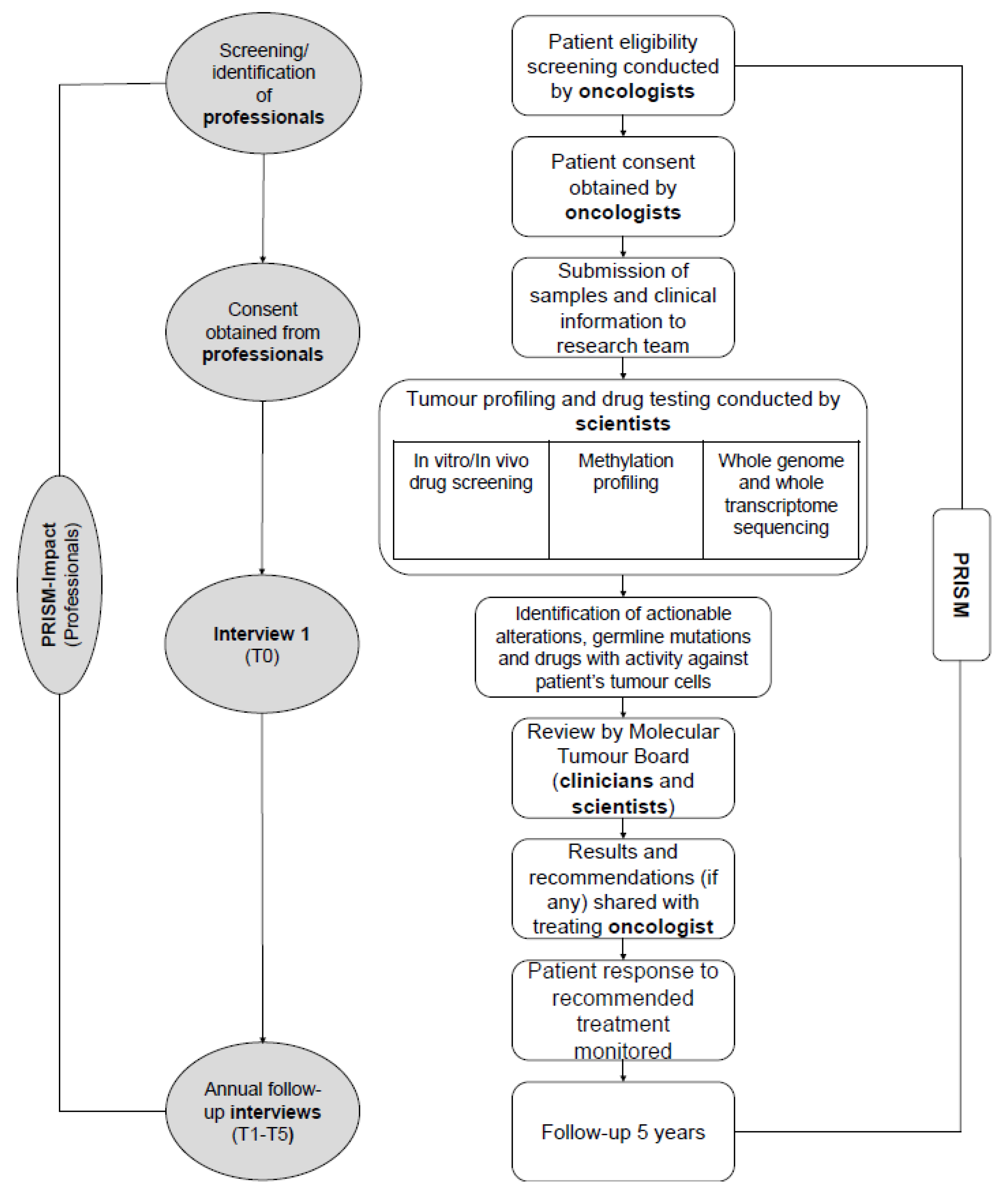
2.1.1. The PRISM Trial
2.1.2. PRISM-Impact
2.2. Procedure
2.3. Data Collection
2.3.1. Measures
2.3.2. Interview
2.4. Data Analysis
3. Results
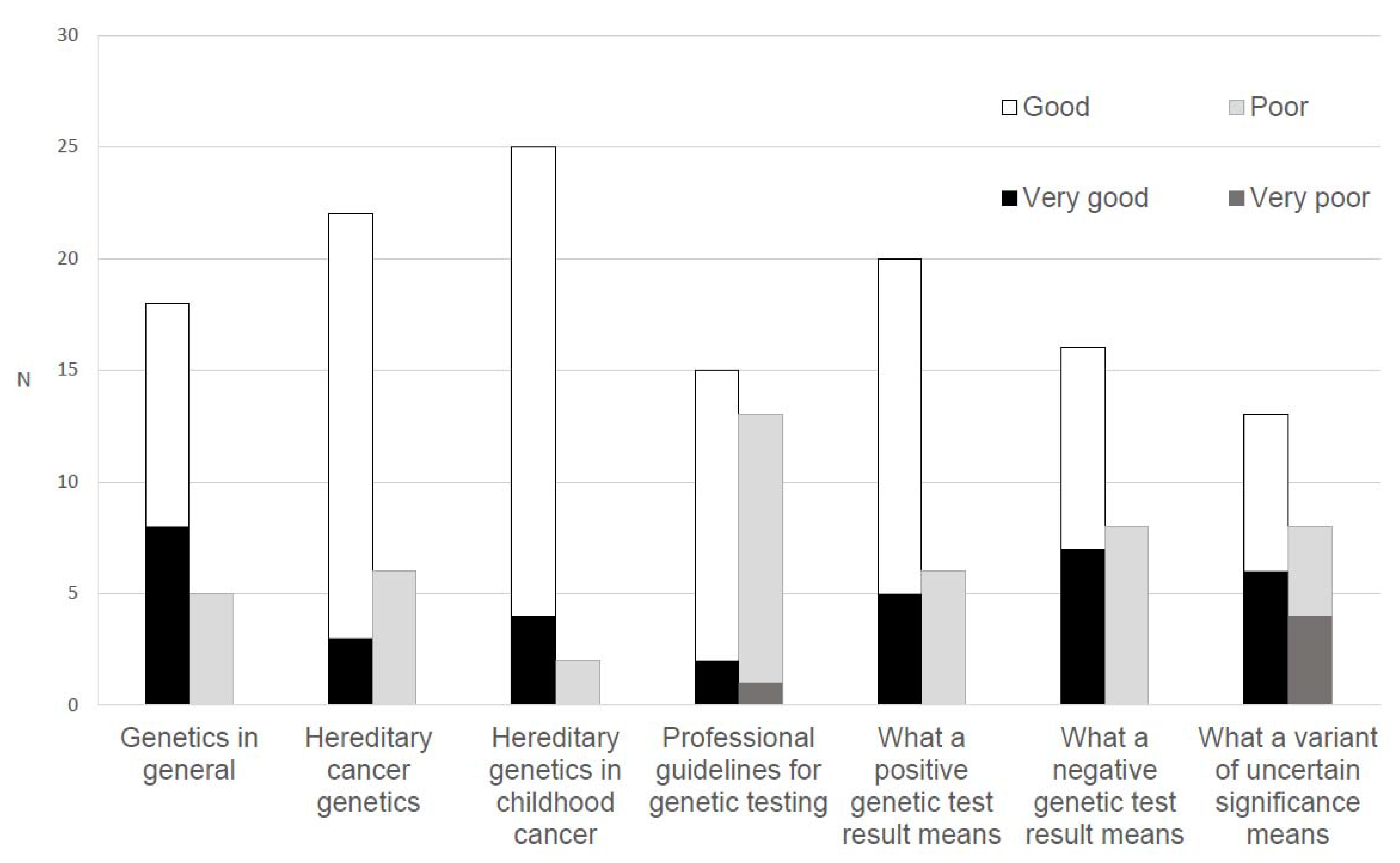
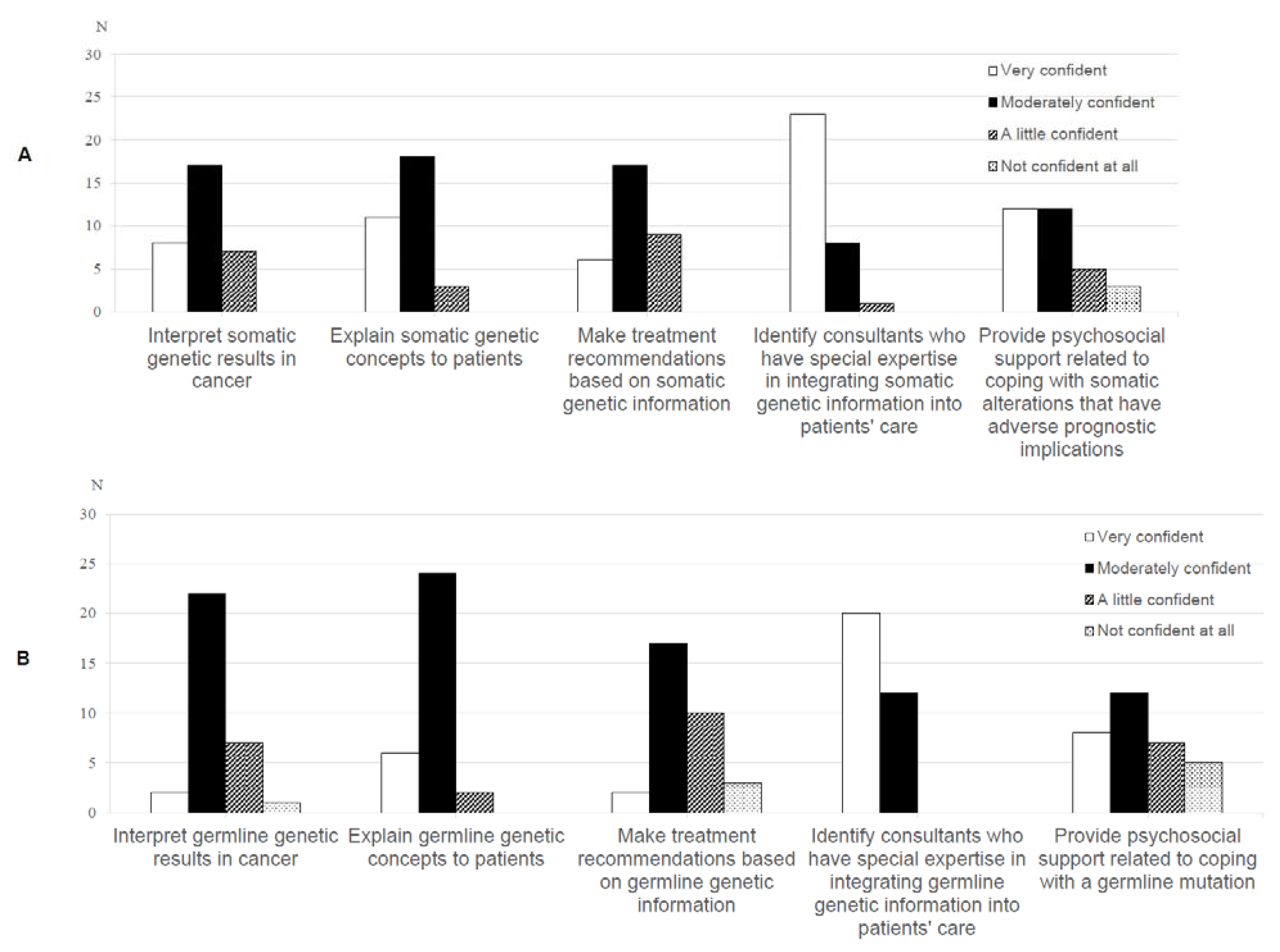
3.1. Knowledge of and Confidence with Genetics
3.2. Interview
3.2.1. Early Experiences with PRISM
I’m not anticipating a whole lot of ‘miracle’ wins to be honest. I think there’ll be the occasional kid who appears to derive clinical benefit…but I think the majority of families will get closure out of it, rather than a miracle.(ID 49, oncologist)
The difficulty is when you have a palliative patient and you’re still giving them access to a phase 1 study their interpretation is that ‘it is going to change things’.(ID 8, oncologist)
PRISM has such a big buzz around it—you know, we had the Prime Minister come here…I think that they think PRISM is the ‘brand new personalised medicine program that will help save lives’, which is what we aim for, but we’re still setting it up.(ID 41, laboratory scientist)
I think it’ll be a little while before we see the bigger changes, but day-to-day I’m seeing the smaller changes. I’m seeing us being able to offer things to families we wouldn’t have otherwise.(ID 7, oncologist)
The basic molecular biology of these things is still over my head. However, being able to learn from the clinician-scientists and all the laboratory staff who are running all the nitty-gritty of these tests really is informative for the clinician.(ID 7, oncologist)
What would be really useful would be to know what happens with a lot of the findings whether recommendations were enacted, or if any child benefited from it. I think that would be useful especially for future patients.(ID 1, clinician-other)
3.2.2. Professional Challenges
There is no knowing whether it will be effective. There is no evidence—not much evidence—you can give to back it up. There is just a lot more uncertainty around the discussion.(ID 7, oncologist)
The difficulty was that the parents found out when the child was very unwell and palliative…so they not only had to deal with that, but also the potential that [the mother] might also be at risk.(ID 1, clinician-other)
Say it was a brain tumour and the surgeon said “Well yes I can get a biopsy but it might cost vision”. Your starting premise has to be that the harm to the child is less than the potential benefits.(ID 20, oncologist)
The big risk is that you find a therapeutic target and yes, there is a drug available, but we cannot get the drug…you build up hope and then take it away.(ID 3, oncologist)
If you see a kid who’s like two months old…you get moved by it quite a lot more than if you see the patient is 25 or 70 years old. That was the big psychological challenge.(ID 42, scientist-other)
As the time gets closer and closer, there may be more hallway talk happening, like ‘what is happening with this patient’ and then things get missed. However, no, stick to the protocol, stick to the protocol.(ID 35, scientist-other)
We need academic output to remain competitive in our careers. However, that is one of the challenges, when you invest so much in each patient. How do you translate that into academic outputs?(ID 43, scientist-other)
You need a champion at every site. It is a very smooth process within [site] but is that process going to be as smooth at the other centres? That takes resources and motivation.(ID 9, oncologist)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Forrest, S.J.; Geoerger, B.; Janeway, K.A. Precision medicine in pediatric oncology. Curr. Opin. Pediatr. 2018, 30, 17. [Google Scholar] [CrossRef] [PubMed]
- Mody, R.J.; Prensner, J.R.; Everett, J.; Parsons, D.W.; Chinnaiyan, A.M. Precision medicine in pediatric oncology: Lessons learned and next steps. Pediatr. Blood Cancer 2017, 64, e26288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsoli, M.; Wadham, C.; Pinese, M.; Failes, T.; Joshi, S.; Mould, E.; Yin, J.X.; Gayevskiy, V.; Kumar, A.; Kaplan, W. Integration of genomics, high throughput drug screening, and personalized xenograft models as a novel precision medicine paradigm for high risk pediatric cancer. Cancer Biol. Ther. 2018, 19, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Worst, B.C.; van Tilburg, C.M.; Balasubramanian, G.P.; Fiesel, P.; Witt, R.; Freitag, A.; Boudalil, M.; Previti, C.; Wolf, S.; Schmidt, S. Next-generation personalised medicine for high-risk paediatric cancer patients–The INFORM pilot study. Eur. J. Cancer 2016, 65, 91–101. [Google Scholar] [CrossRef] [Green Version]
- Granek, L.; Bartels, U.; Scheinemann, K.; Labrecque, M.; Barrera, M. Grief reactions and impact of patient death on pediatric oncologists. Pediatr. Blood Cancer 2015, 62, 134–142. [Google Scholar] [CrossRef]
- Willemsen, A.E.; Krausz, S.; Ligtenberg, M.J.; Grünberg, K.; Groen, H.J.; Voest, E.E.; Cuppen, E.P.; van Laarhoven, H.W.; van Herpen, C.M. Molecular tumour boards and molecular diagnostics for patients with cancer in the Netherlands: Experiences, challenges, and aspirations. Br. J. Cancer 2019, 121, 34–36. [Google Scholar] [CrossRef]
- Bourret, P.; Cambrosio, A. Genomic expertise in action: Molecular tumour boards and decision-making in precision oncology. Sociol Health Illn. 2019, 41, 1568–1584. [Google Scholar] [CrossRef]
- Knepper, T.C.; Bell, G.C.; Hicks, J.K.; Padron, E.; Teer, J.K.; Vo, T.T.; Gillis, N.K.; Mason, N.T.; McLeod, H.L.; Walko, C.M. Key lessons learned from Moffitt’s molecular tumor board: The Clinical Genomics Action Committee experience. Oncologist 2017, 22, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Wright, S.; Porteous, M.; Stirling, D.; Young, O.; Gourley, C.; Hallowell, N. Negotiating jurisdictional boundaries in response to new genetic possibilities in breast cancer care: The creation of an ‘oncogenetic taskscape’. Soc. Sci. Med. 2019, 225, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Hallowell, N.; Wright, S.; Stirling, D.; Gourley, C.; Young, O.; Porteous, M. Moving into the mainstream: Healthcare professionals’ views of implementing treatment focussed genetic testing in breast cancer care. Fam. Cancer 2019, 18, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Vetsch, J.; Wakefield, C.E.; Techakesari, P.; Warby, M.; Ziegler, D.; O’Brien, T.; Drinkwater, C.; Neeman, N.; Tucker, K. Healthcare professionals’ attitudes toward cancer precision medicine: A systematic review. Semin. Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Burton, H.; Cole, T.; Lucassen, A. Genomic medicine: Challenges and opportunities for physicians. Clin. Med. 2012, 12, 416–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, N.S.; Davis, J.K.; Kirby, C.; McGuire, A.L.; Green, R.C.; Blumenthal-Barby, J.; Ubel, P.A.; Project, M. Communication challenges for nongeneticist physicians relaying clinical genomic results. Pers. Med. 2017, 14, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.M.; Valdez, J.M.; Quinn, E.A.; Sykes, A.D.; McGee, R.B.; Nuccio, R.; Hines-Dowell, S.J.; Baker, J.N.; Kesserwan, C.; Nichols, K.E. Integrating next-generation sequencing into pediatric oncology practice: An assessment of physician confidence and understanding of clinical genomics. Cancer 2017, 123, 2352–2359. [Google Scholar] [CrossRef]
- Robertson, E.G.; Mitchell, R.; Wakefield, C.E.; Lewis, P.; Cousens, N.; Marshall, G.M.; Russell, S.J.; Ziegler, D.S.; Anazodo, A.C.; Trahair, T.N. Enrolment in paediatric oncology early-phase clinical trials: The health-care professionals’ perspective. J. Paediatr. Child Health 2019, 55, 561–566. [Google Scholar] [CrossRef]
- Schechter, T.; Grant, R. The complexity of consenting to clinical research in phase I pediatric cancer studies. Paediatr. Drugs 2015, 17, 77–81. [Google Scholar] [CrossRef]
- Cousino, M.K.; Zyzanski, S.J.; Yamokoski, A.D.; Hazen, R.A.; Baker, J.N.; Noll, R.B.; Rheingold, S.R.; Geyer, J.R.; Alexander, S.C.; Drotar, D. Communicating and understanding the purpose of pediatric phase I cancer trials. J. Clin. Oncol. 2012, 30, 4367. [Google Scholar] [CrossRef] [Green Version]
- Oberg, J.A.; Ruiz, J.; Ali-Shaw, T.; Schlechtweg, K.A.; Ricci, A.; Kung, A.L.; Chung, W.K.; Appelbaum, P.S.; Glade Bender, J.L.; Levine, J.M. Whole-genome and whole-exome sequencing in pediatric oncology: An assessment of parent and young adult patient knowledge, attitudes, and expectations. JCO Precis. Oncol. 2018, 2, 1–11. [Google Scholar] [CrossRef]
- Oberg, J.A.; Glade Bender, J.L.; Cohn, E.G.; Morris, M.; Ruiz, J.; Chung, W.K.; Appelbaum, P.S.; Kung, A.L.; Levine, J.M. Overcoming challenges to meaningful informed consent for whole genome sequencing in pediatric cancer research. Pediatr Blood Cancer 2015, 62, 1374–1380. [Google Scholar] [CrossRef]
- Marron, J.M.; Cronin, A.M.; DuBois, S.G.; Glade-Bender, J.; Kim, A.; Crompton, B.D.; Meyer, S.C.; Janeway, K.A.; Mack, J.W. Duality of Purpose: Participant and Parent Understanding of the Purpose of Genomic Tumor Profiling Research Among Children and Young Adults With Solid Tumors. JCO Precis. Oncol. 2019, 3, 1–17. [Google Scholar] [CrossRef]
- Jansen, L.A.; Mahadevan, D.; Appelbaum, P.S.; Klein, W.M.; Weinstein, N.D.; Mori, M.; Daffé, R.; Sulmasy, D.P. Dispositional optimism and therapeutic expectations in early-phase oncology trials. Cancer 2016, 122, 1238–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vetsch, J.; Wakefield, C.E.; Duve, E.; McGill, B.C.; Warby, M.; Tucker, K.M.; Malkin, D.; Lau, L.; Zielger, D.S. Parents’, healthcare professionals’ and scientists’ experiences of a precision medicine pilot trial for high-risk childhood cancer patients: A qualitative study. JCO Precis. Oncol. 2019. [Google Scholar] [CrossRef]
- Johnson, L.-M.; Hamilton, K.V.; Valdez, J.M.; Knapp, E.; Baker, J.N.; Nichols, K.E. Ethical considerations surrounding germline next-generation sequencing of children with cancer. Expert Rev. Mol. Diagn. 2017, 17, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, C.; Manca, P.; Salgado, R.; Van Dam, P.; Dendooven, A.; Coelho, A.M.; Gandia, J.F.; Rutten, A.; Lybaert, W.; Vermeij, J. Multidisciplinary molecular tumour board: A tool to improve clinical practice and selection accrual for clinical trials in patients with cancer. ESMO Open 2018, 3, e000398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, D.A.; Feero, W.G.; Khoury, M.J. Convergence of implementation science, precision medicine, and the learning health care system: A new model for biomedical research. JAMA 2016, 315, 1941–1942. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, D.E.; Moeckel, F.; Villa, M.S.; Housman, L.T.; McCarty, C.A.; McLeod, H.L. Strategies for integrating personalized medicine into healthcare practice. Pers. Med. 2017, 14, 141–152. [Google Scholar] [CrossRef] [Green Version]
- Lau, L.; Byrne, J.; Ekert, P.G.; Failes, T.; Fellowes, A.; Fletcher, J.; Gifford, A.; Haber, M.; Kumar, A.; Lock, R. Pilot study of a comprehensive precision medicine platform for children with high-risk cancer. J. Clin. Oncol. 2017, 35, 10539. [Google Scholar] [CrossRef]
- Douma, K.F.; Smets, E.M.; Allain, D.C. Non-genetic health professionals’ attitude towards, knowledge of and skills in discussing and ordering genetic testing for hereditary cancer. Fam. Cancer 2016, 15, 341–350. [Google Scholar] [CrossRef] [Green Version]
- Klitzman, R.; Chung, W.; Marder, K.; Shanmugham, A.; Chin, L.J.; Stark, M.; Leu, C.-S.; Appelbaum, P.S. Attitudes and practices among internists concerning genetic testing. J. Genet. Couns. 2013, 22, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Miles, M.B.; Huberman, A.M.; Huberman, M.A.; Huberman, M. Qualitative Data Analysis: An Expanded Sourcebook; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- El Saghir, N.S.; Charara, R.N.; Kreidieh, F.Y.; Eaton, V.; Litvin, K.; Farhat, R.A.; Khoury, K.E.; Breidy, J.; Tamim, H.; Eid, T.A. Global practice and efficiency of multidisciplinary tumor boards: Results of an American Society of Clinical Oncology international survey. J. Glob. Oncol. 2015, 1, 57–64. [Google Scholar] [CrossRef]
- Harada, S.; Arend, R.; Dai, Q.; Levesque, J.A.; Winokur, T.S.; Guo, R.; Heslin, M.J.; Nabell, L.; Nabors, L.B.; Limdi, N.A. Implementation and utilization of the molecular tumor board to guide precision medicine. Oncotarget 2017, 8, 57845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaneda, C.; Nalley, K.; Mannion, C.; Bhattacharyya, P.; Blake, P.; Pecora, A.; Goy, A.; Suh, K.S. Clinical decision support systems for improving diagnostic accuracy and achieving precision medicine. J. Clin. Bioinform. 2015, 5, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghavan, S.; Vassy, J.L. Do physicians think genomic medicine will be useful for patient care? Pers. Med. 2014, 11, 425–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, S.; Ghersi, D. Building towards precision medicine: Empowering medical professionals for the next revolution. BMC Med. Genomics 2016, 9, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, K.D.; Vassy, J.L.; Jamal, L.; Lehmann, L.S.; Slashinski, M.J.; Perry, D.L.; Robinson, J.O.; Blumenthal-Barby, J.; Feuerman, L.Z.; Murray, M.F. Are physicians prepared for whole genome sequencing? A qualitative analysis. Clin. Genet. 2016, 89, 228–234. [Google Scholar] [CrossRef]
- Patch, C.; Middleton, A. Genetic counselling in the era of genomic medicine. Br. Med. Bull. 2018, 126, 27–36. [Google Scholar] [CrossRef]
- Jones, D.T.; Banito, A.; Grünewald, T.G.; Haber, M.; Jäger, N.; Kool, M.; Milde, T.; Molenaar, J.J.; Nabbi, A.; Pugh, T.J. Molecular characteristics and therapeutic vulnerabilities across paediatric solid tumours. Nat. Rev. Cancer 2019, 19, 420–438. [Google Scholar] [CrossRef]
- Macklin, S.K.; Jackson, J.L.; Atwal, P.S.; Hines, S.L. Physician interpretation of variants of uncertain significance. Fam. Cancer 2019, 18, 121–126. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Clinicians (n = 39) | Scientists (n = 15) | |
|---|---|---|
| Profession, clinicians, n (%) Oncologist Pathologist Geneticist Genetic counsellor | 35 (90) 2 (4) 1 (3) 1 (3) | |
| Profession, scientists, n (%) Laboratory scientist 1 Bioinformatician Technical support | 11 (73) 3 (20) 1 (7) | |
| Site, n (%) PRISM main site Others | 11 (28) 28 (72) | 11 (73) 4 (27) |
| PRISM investigators 2, n (%) | 31 (79) | 1 (7) |
| PRISM pilot 3, n (%) | 18 (46) | 15 (100) |
| Age, mean (SD), range, y | 47 (9), 30–73 | 36 (9), 25–57 |
| Sex, no. (%) Male Female | 18 (46) 21 (54) | 9 (60) 6 (40) |
| No. years professional practice, mean (SD), range | 20 (12), 5–45 | 7 (5), 1-20 |
| No. years paediatric oncology practice, mean (SD), range | 16 (10), 2–43 | 5 (5), 1–20 |
| Time dedicated to research (%), mean (SD), range | 25 (19), 0–80 | 87 (28), 10–100 |
| Topic | Themes |
|---|---|
| Early experiences with PRISM | Common to both groups • Cautious optimism • Managing expectations • A new way of working • The MTB: a valuable forum, with room for improvement |
| Professional challenges | Clinicians • Difficulty understanding and communicating results • Balancing risk of additional biopsies • Limited drug availability and access Scientists • Greater emotional impact with more awareness of the patient • Resisting urgency • Balancing translational outputs with academic productivity Common to both groups • Logistical challenges of a national trial |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGill, B.C.; Wakefield, C.E.; Hetherington, K.; Munro, L.J.; Warby, M.; Lau, L.; Tyrrell, V.; Ziegler, D.S.; O’Brien, T.A.; Marshall, G.M.; et al. “Balancing Expectations with Actual Realities”: Conversations with Clinicians and Scientists in the First Year of a High-Risk Childhood Cancer Precision Medicine Trial. J. Pers. Med. 2020, 10, 9. https://doi.org/10.3390/jpm10010009
McGill BC, Wakefield CE, Hetherington K, Munro LJ, Warby M, Lau L, Tyrrell V, Ziegler DS, O’Brien TA, Marshall GM, et al. “Balancing Expectations with Actual Realities”: Conversations with Clinicians and Scientists in the First Year of a High-Risk Childhood Cancer Precision Medicine Trial. Journal of Personalized Medicine. 2020; 10(1):9. https://doi.org/10.3390/jpm10010009
Chicago/Turabian StyleMcGill, Brittany C., Claire E. Wakefield, Kate Hetherington, Lachlan J. Munro, Meera Warby, Loretta Lau, Vanessa Tyrrell, David S. Ziegler, Tracey A. O’Brien, Glenn M. Marshall, and et al. 2020. "“Balancing Expectations with Actual Realities”: Conversations with Clinicians and Scientists in the First Year of a High-Risk Childhood Cancer Precision Medicine Trial" Journal of Personalized Medicine 10, no. 1: 9. https://doi.org/10.3390/jpm10010009