
Sexual Dysfunction and Atopic Dermatitis: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
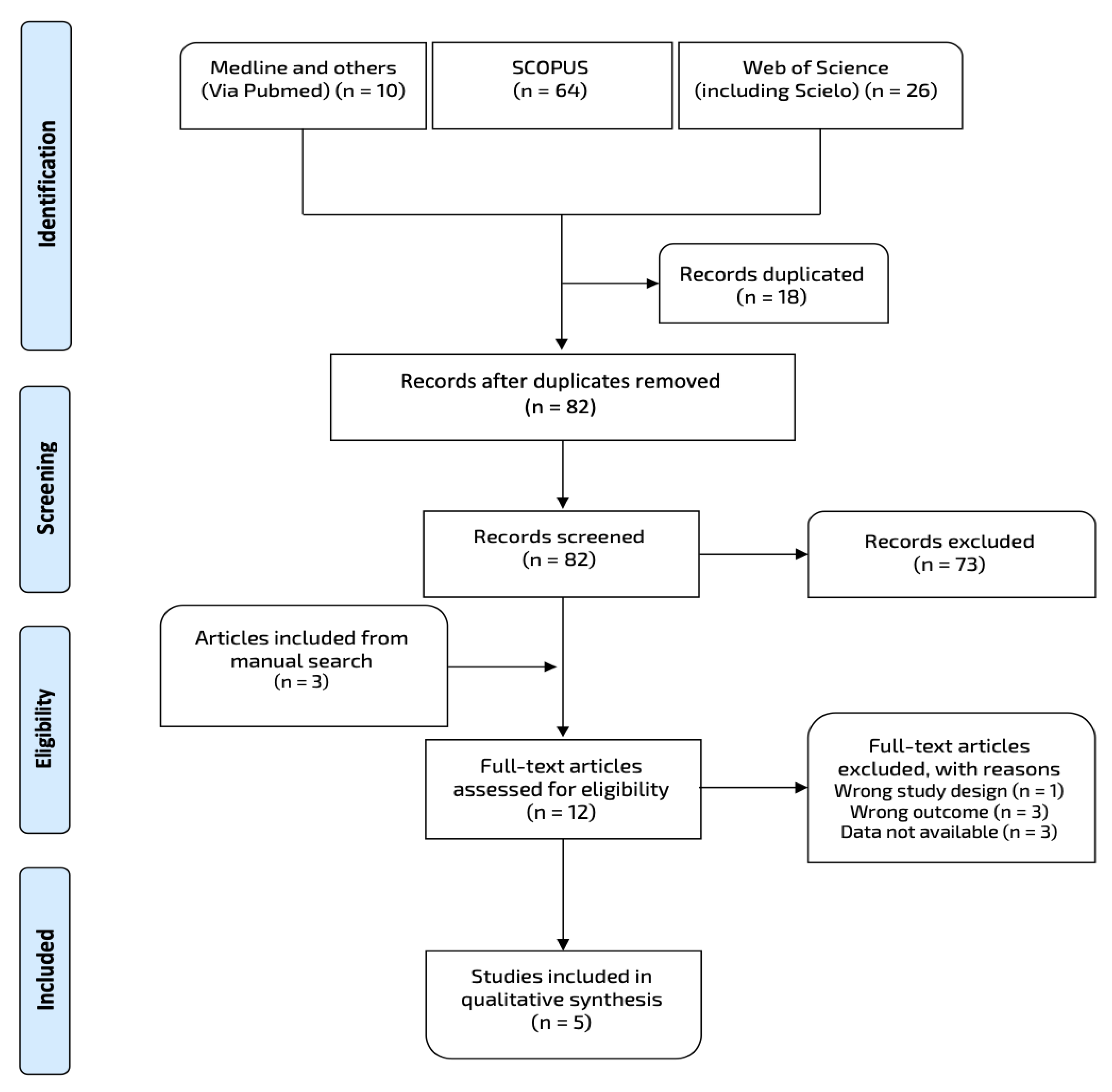
2.1. Data Sources and Search Strategy
2.2. Study Selection and Data Extraction
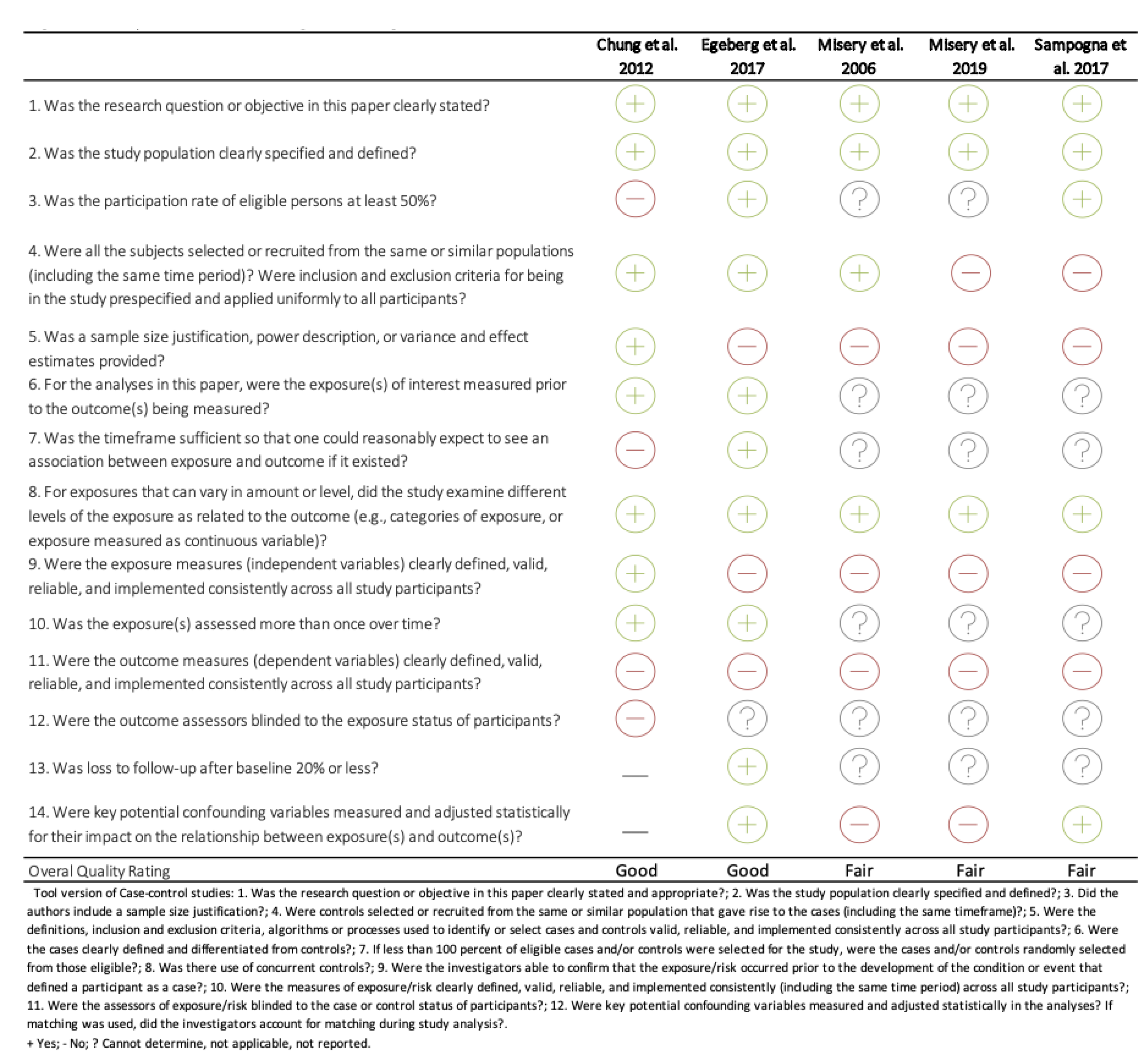
2.3. Quality Assessment: Risk of Bias Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Silverberg, J.I. Public Health Burden and Epidemiology of Atopic Dermatitis. Dermatol. Clin. 2017, 35, 283–289. [Google Scholar] [CrossRef]
- Muraro, A.; Lemanske, R.F.; Hellings, P.W.; Akdis, C.A.; Bieber, T.; Casale, T.B.; Jutel, M.; Ong, P.Y.; Poulsen, L.K.; Schmid-Grendelmeier, P.; et al. Precision medicine in patients with allergic diseases: Airway diseases and atopic dermatitis—PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2016, 137, 1347–1358. [Google Scholar]
- Sicras-Mainar, A.; Navarro-Artieda, R.; Armario-Hita, J.C. Severe Atopic Dermatitis In Spain: A Real-Life Observational Study. Ther. Clin. Risk Manag. 2019, 15, 1393–1401. [Google Scholar] [CrossRef] [Green Version]
- Sicras-Mainar, A.; Navarro-Artieda, R.; Sánchez, L.; Sastre, J. Prevalence of severe atopic dermatitis in adults in 3 areas of spain. J. Investig. Allergol. Clin. Immunol. 2018, 28, 195–197. [Google Scholar] [CrossRef]
- Nettis, E.; Ortoncelli, M.; Pellacani, G.; Foti, C.; Di Leo, E.; Patruno, C.; Rongioletti, F.; Argenziano, G.; Ferrucci, S.M.; Macchia, L.; et al. A Multicenter Study on the Prevalence of Clinical Patterns and Clinical Phenotypes in Adult Atopic Dermatitis. J. Investig. Allergol. Clin. Immunol. 2020, 30, 448–450. [Google Scholar] [CrossRef]
- Dattola, A.; Bennardo, L.; Silvestri, M.; Nisticò, S.P. What’s new in the treatment of atopic dermatitis? Dermatol. Ther. 2019, 32, e12787. [Google Scholar] [CrossRef] [PubMed]
- Koszorú, K.; Borza, J.; Gulácsi, L.; Sárdy, M. Quality of life in patients with atopic dermatitis. Cutis 2019, 104, 174–177. [Google Scholar] [PubMed]
- Silverberg, J.I.; Gelfand, J.M.; Margolis, D.J.; Boguniewicz, M.; Fonacier, L.; Grayson, M.H.; Simpson, E.L.; Ong, P.Y.; Chiesa Fuxench, Z.C. Patient burden and quality of life in atopic dermatitis in US adults: A population-based cross-sectional study. Ann. Allergy Asthma Immunol. 2018, 121, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, J.I. Comorbidities and the impact of atopic dermatitis. Ann. Allergy Asthma Immunol. 2019, 123, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Rønnstad, A.T.M.; Halling-Overgaard, A.S.; Hamann, C.R.; Skov, L.; Egeberg, A.; Thyssen, J.P. Association of atopic dermatitis with depression, anxiety, and suicidal ideation in children and adults: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2018, 79, 448–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brew, B.K.; Lundholm, C.; Gong, T.; Larsson, H.; Almqvist, C. The familial aggregation of atopic diseases and depression or anxiety in children. Clin. Exp. Allergy 2018, 48, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Lim, V.Z.Y.; Ho, R.C.M.; Tee, S.I.; Ho, M.S.L.; Pan, J.Y.; Lim, Y.L.; Tang, M.B.Y.; Chan, K.L.; Giam, Y.C. Anxiety and depression in patients with atopic dermatitis in a Southeast Asian tertiary dermatological centre. Ann. Acad. Med. Singap. 2016, 45, 451–455. [Google Scholar] [PubMed]
- Wespes, E.; Amar, E.; Eardley, I.; Giuliano, F.; Hatzichristou, D.; Hatzimouratidis, K.; Montorsi, F.; Vardi, Y. Guía clínica sobre la disfunción sexual masculina: Disfunción eréctil y eyaculación precoz. Eur. Assoc. Urol. 2010, 2010, 842–899. [Google Scholar]
- Blümel, M.J.E.; Binfa, E.L.; Cataldo, A.P.; Carrasco, V.A.; Izaguirre, L.H.; Sarrá, C.S. Índice De Función Sexual Femenina: Un Test Para Evaluar La Sexualidad De La Mujer. Rev. Chil. Obstet. Ginecol. 2004, 69, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Clayton, A.H.; Valladares Juarez, E.M. Female Sexual Dysfunction. Med. Clin. N. Am. 2019, 103, 681–698. [Google Scholar] [CrossRef]
- Palacios, S.; Castaño, R.; Grazziotin, A. Epidemiology of female sexual dysfunction. Maturitas 2009, 63, 119–123. [Google Scholar] [CrossRef]
- Egeberg, A.; Hansen, P.R.; Gislason, G.H.; Skov, L.; Thyssen, J.P. Erectile Dysfunction in Male Adults With Atopic Dermatitis and Psoriasis. J. Sex. Med. 2017, 14, 380–386. [Google Scholar] [CrossRef]
- Chung, S.D.; Keller, J.J.; Lin, H.C. Association of erectile dysfunction with atopic dermatitis: A population-based case-control study. J. Sex. Med. 2012, 9, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Canguven, O. The role of low testosterone associated with erectile dysfunction with atopic dermatitis. J. Sex. Med. 2013, 10, 618. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Covidence Systematic Review Software. Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 29 September 2021).
- National Institutes of Health. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 2014. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 29 September 2021).
- Misery, L.; Finlay, A.Y.; Martin, N.; Boussetta, S.; Nguyen, C.; Myon, E.; Taieb, C. Atopic dermatitis: Impact on the quality of life of patients and their partners. Dermatology 2007, 215, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Sampogna, F.; Abeni, D.; Gieler, U.; Tomas-Aragones, L.; Lien, L.; Titeca, G.; Jemec, G.B.; Misery, L.; Szabó, C.; Linder, M.D.; et al. Impairment of Sexual Life in 3485 Dermatological Outpatients From a Multicentre Study in 13 European Countries. Acta Derm.-Venereol. 2016, 96, 128–129. [Google Scholar]
- Misery, L.; Seneschal, J.; Reguiai, Z.; Merhand, S.; Héas, S.; Huet, F.; Taieb, C.; Ezzedine, K. The impact of atopic dermatitis on sexual health. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 428–432. [Google Scholar] [CrossRef]
- Picardi, A.; Abeni, D.; Renzi, C.; Braga, M.; Melchi, C.F.; Pasquini, P. Treatment outcome and incidence of psychiatric disorders in dermatological out-patients. J. Eur. Acad. Dermatol. Venereol. 2003, 17, 155–159. [Google Scholar] [CrossRef]
- Cheng, C.M.; Hsu, J.W.; Huang, K.L.; Bai, Y.M.; Su, T.P.; Li, C.T.; Yang, A.C.; Chang, W.-H.; Chen, T.-J.; Tsai, S.-J.; et al. Risk of developing major depressive disorder and anxiety disorders among adolescents and adults with atopic dermatitis: A nationwide longitudinal study. J. Affect. Disord. 2015, 178, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Ronaldson, A.; Arias de la Torre, J.; Sima, R.M.; Hatch, S.; Hotopf, M.; Dregan, A. Depressive and anxiety symptomatology among people with asthma or atopic dermatitis: A population-based investigation using the UK Biobank data. Brain Behav. Immun. 2020, 90, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, J.K.; Wu, K.K.; Bui, T.L.; Armstrong, A.W. Association Between Atopic Dermatitis and Suicidality: A Systematic Review and Meta-analysis. JAMA Dermatol. 2019, 155, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Li, J.C.; Fishbein, A.; Singam, V.; Patel, K.R.; Zee, P.C.; Attarian, H.; Cella, D.; Silverberg, J.I. Sleep Disturbance and Sleep-Related Impairment in Adults With Atopic Dermatitis: A Cross-sectional Study. Dermatitis 2018, 29, 270–277. [Google Scholar] [CrossRef]
- Fishbein, A.B.; Mueller, K.; Kruse, L.; Boor, P.; Sheldon, S.; Zee, P.; Paller, A.S. Sleep disturbance in children with moderate/severe atopic dermatitis: A case-control study. J. Am. Acad. Dermatol. 2018, 78, 336–341. [Google Scholar] [CrossRef]
- Ermertcan, A.T. Sexual dysfunction in dermatological diseases. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 999–1007. [Google Scholar] [CrossRef]
- Latif, E.Z.; Diamond, M.P. Arriving at the diagnosis of female sexual dysfunction. Fertil. Steril. 2013, 100, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, C.M.; Fernandez, J.M.; Hsiao, J.L.; Shi, V.Y. The Interplay of Atopic Dermatitis and Sexual Health. Dermatitis 2020, 31, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Hatzichristou, D.; Kirana, P.S.; Banner, L.; Althof, S.E.; Lonnee-Hoffmann, R.A.; Dennerstein, L.; Rossen, R.C. Diagnosing Sexual Dysfunction in Men and Women: Sexual History Taking and the Role of Symptom Scales and Questionnaires. J. Sex. Med. 2016, 13, 1166–1182. [Google Scholar] [CrossRef] [PubMed]
- Giraldi, A.; Rellini, A.; Pfaus, J.G.; Bitzer, J.; Laan, E.; Jannini, E.A.; Fugl-Meyer, A.R. Questionnaires for assessment of female sexual dysfunction: A review and proposal for a standardized screener. J. Sex. Med. 2011, 8, 2681–2706. [Google Scholar] [CrossRef]
- Long, C.C.; Funnell, C.M.; Collard, R.; Finlay, A.Y. What do members of the National Eczema Society really want? Clin. Exp. Dermatol. 1993, 18, 516–522. [Google Scholar] [CrossRef]
- Ebata, T.; Itamura, R.; Aizawa, H.; Niimura, M. Serum sex hormone levels in adult patients with atopic dermatitis. J. Dermatol. 1996, 23, 603–605. [Google Scholar] [CrossRef]
- Ramsay, B.; O’Reagan, M. A survey of the social and psychological effects of psoriasis. Br. J. Dermatol. 1988, 118, 195–201. [Google Scholar] [CrossRef]
- Tasliyurt, T.; Bilir, Y.; Sahin, S.; Seckin, H.Y.; Kaya, S.U.; Sivgin, H.; Demir, A.K.; Erdemir, F. Erectile dysfunction in patients with psoriasis: Potential impact of the metabolic syndrome. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 581–586. [Google Scholar]
- Cabete, J.; Torres, T.; Vilarinho, T.; Ferreira, A.; Selores, M. Erectile dysfunction in psoriasis patients. Eur. J. Dermatol. 2014, 24, 482–486. [Google Scholar] [CrossRef]
- Molina-Leyva, A.; Molina-Leyva, I.; Almodovar-Real, A.; Ruiz-Carrascosa, J.C.; Naranjo-Sintes, R.; Jimenez-Moleon, J.J. Prevalence and Associated Factors of Erectile Dysfunction in Patients With Moderate to Severe Psoriasis and Healthy Population: A Comparative Study Considering Physical and Psychological Factors. Arch. Sex. Behav. 2016, 45, 2047–2055. [Google Scholar] [CrossRef]
- Zhao, S.; Wang, J.; Xie, Q.; Liu, Y.; Luo, L.; Zhu, Z.; Li, E.; Zhao, Z. High prevalence of erectile dysfunction in men with psoriasis: Evidence from a systematic review and meta-analysis. Int. J. Impot. Res. 2019, 31, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Duan, X.; Chen, S.; Chen, X.; Yu, R.; Yu, X. Association Between Psoriasis and Erectile Dysfunction: A Meta-Analysis. J. Sex. Med. 2018, 15, 839–847. [Google Scholar] [CrossRef]
- Kurizky, P.; Martins, G.; Carneiro, J.; Gomes, C.; da Mota, L. Evaluation of the occurrence of sexual dysfunction and general quality of life in female patients with psoriasis. An. Bras. Dermatol. 2018, 93, 801–806. [Google Scholar] [CrossRef] [Green Version]
- Alavi, A.; Farzanfar, D.; Rogalska, T.; Lowes, M.A.; Chavoshi, S. Quality of life and sexual health in patients with hidradenitis suppurativa. Int. J. Womens Dermatol. 2018, 4, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Janse, I.C.; Deckers, I.E.; van der Maten, A.D.; Evers, A.W.M.; Boer, J.; van der Zee, H.H.; Prens, E.P.; Horváth, B. Sexual health and quality of life are impaired in hidradenitis suppurativa: A multicentre cross-sectional study. Br. J. Dermatol. 2017, 176, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Slyper, M.; Strunk, A.; Garg, A. Incidence of sexual dysfunction among patients with hidradenitis suppurativa: A population-based retrospective analysis. Br. J. Dermatol. 2018, 179, 502–503. [Google Scholar] [CrossRef]
- Cuenca-Barrales, C.; Ruiz-Villaverde, R.; Molina-Leyva, A. Sexual Distress in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study. J. Clin. Med. 2019, 8, 532. [Google Scholar] [CrossRef] [Green Version]
- Cuenca-Barrales, C.; Molina-Leyva, A. Risk Factors of Sexual Dysfunction in Patients with Hidradenitis Suppurativa: A Cross-Sectional Study. Dermatology 2020, 236, 37–45. [Google Scholar] [CrossRef]
- Cuenca-Barrales, C.; Montero-Vílchez, T.; Szepietowski, J.C.; Matusiak, L.; Molina-Leyva, A. Sexual impairment in patients with hidradenitis suppurativa: A systematic review. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 345–352. [Google Scholar] [CrossRef]
- Juan, C.K.; Chen, H.J.; Shen, J.L.; Kao, C.H. Lichen Simplex Chronicus Associated With Erectile Dysfunction: A Population-Based Retrospective Cohort Study. PLoS ONE 2015, 10, e0128869. [Google Scholar] [CrossRef]
- Sukan, M.; Maner, F. The problems in sexual functions of vitiligo and chronic urticaria patients. J. Sex Marital Ther. 2007, 33, 55–64. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Country | Design | Gender/Age (x ± sd, Years) | Sample Size Cases (AD), N | Atopic Dermatitis Severity, N | Sample Size Controls, N | Sexual Dysfunction Assessment Tool | Prevalence SD in Cases, No (%) | Prevalence SD in Controls, No (%) |
|---|---|---|---|---|---|---|---|---|---|
| Chung et al., 2012 [18] | Taiwan | Case-Control | All Men/50.6 ± 15.0 | 3,997 | Not reported | Healthy controls, 19,985 | Erectile dysfunction (impotence, organic (International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) | 425 (10.6) | Healthy controls 1333 (6.7) |
| Egeberg et al., 2017 [17] | Denmark | Cohort Study | All men/53.0 ± 14.6, 46.7 ± 12.0, 56.3 ± 13.8, for general population, AD and psoriasis respectively | 2,373 | Mild AD, 1072 Severe AD, 1301 | Healthy controls, 1,727,770 Psoriasis, 26,536 | Erectile Dysfunction (patients’ first claimed prescription for drugs used in treatment of male ED (i.e., sildenafil, ATC code G04BE03; tadalafil, ATC code G04BE08; vardenafil, ATC code G04BE09; or avanafil, ATC code G04BE10). | 112 (10.65) * | Healthy controls, 79,374 (10.79) * Psoriasis, 1533 (14.56) * |
| Misery et al., 2006 [24] | United Kingdom | Cross-sectional | 91 males and 175 females/32.7 ± 12.7 | 266 | Mild AD,4 Moderate AD, 114 Severe AD, 148 | No controls | Sexual questionnaire from the CHOQ, which include 7 items for the patients and 6 for their partners. DLQI | 153 (57.5) | - |
| Misery et al., 2019 [26] | France | Cross-sectional | 427 males and 596 women | 1022 | Mild AD, 283 Moderate AD, 414 Severe AD, 327 | No controls | Item nine from the DLQI | 483 (57.9) | - |
| Sampogna et al., 2017 [25] | Multicenter Study from 13 European Countries; main author from Italy. | Cross-sectional | 1524 males and 1950 females/38.3% <39 years; 34.2% from 40 to 59 years; 27.5% > 60 years. | 448 | Not reported | Psoriasis, 537 Acne, 202 Blistering disorders, 53 Other dermatological conditions +, 2245 | Item nine from the DLQI | 130 (29.0) | Psoriasis, 187 (34.8) Blistering disorders, 18 (34.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linares-Gonzalez, L.; Lozano-Lozano, I.; Gutierrez-Rojas, L.; Lozano-Lozano, M.; Rodenas-Herranz, T.; Ruiz-Villaverde, R. Sexual Dysfunction and Atopic Dermatitis: A Systematic Review. Life 2021, 11, 1314. https://doi.org/10.3390/life11121314
Linares-Gonzalez L, Lozano-Lozano I, Gutierrez-Rojas L, Lozano-Lozano M, Rodenas-Herranz T, Ruiz-Villaverde R. Sexual Dysfunction and Atopic Dermatitis: A Systematic Review. Life. 2021; 11(12):1314. https://doi.org/10.3390/life11121314
Chicago/Turabian StyleLinares-Gonzalez, Laura, Ignacio Lozano-Lozano, Luis Gutierrez-Rojas, Mario Lozano-Lozano, Teresa Rodenas-Herranz, and Ricardo Ruiz-Villaverde. 2021. "Sexual Dysfunction and Atopic Dermatitis: A Systematic Review" Life 11, no. 12: 1314. https://doi.org/10.3390/life11121314