
Accuracy of Digital Impression Taking with Intraoral Scanners and Fabrication of CAD/CAM Posts and Cores in a Fully Digital Workflow



Abstract
:1. Introduction
- (1)
- There is no significant difference between the different digital impression methods concerning the deviation from the reference dataset (Part A).
- (2)
- There is no significant difference between the different digital impression methods as well as the materials used about the accuracy of fit of CAD/CAM-P+C (Part B).
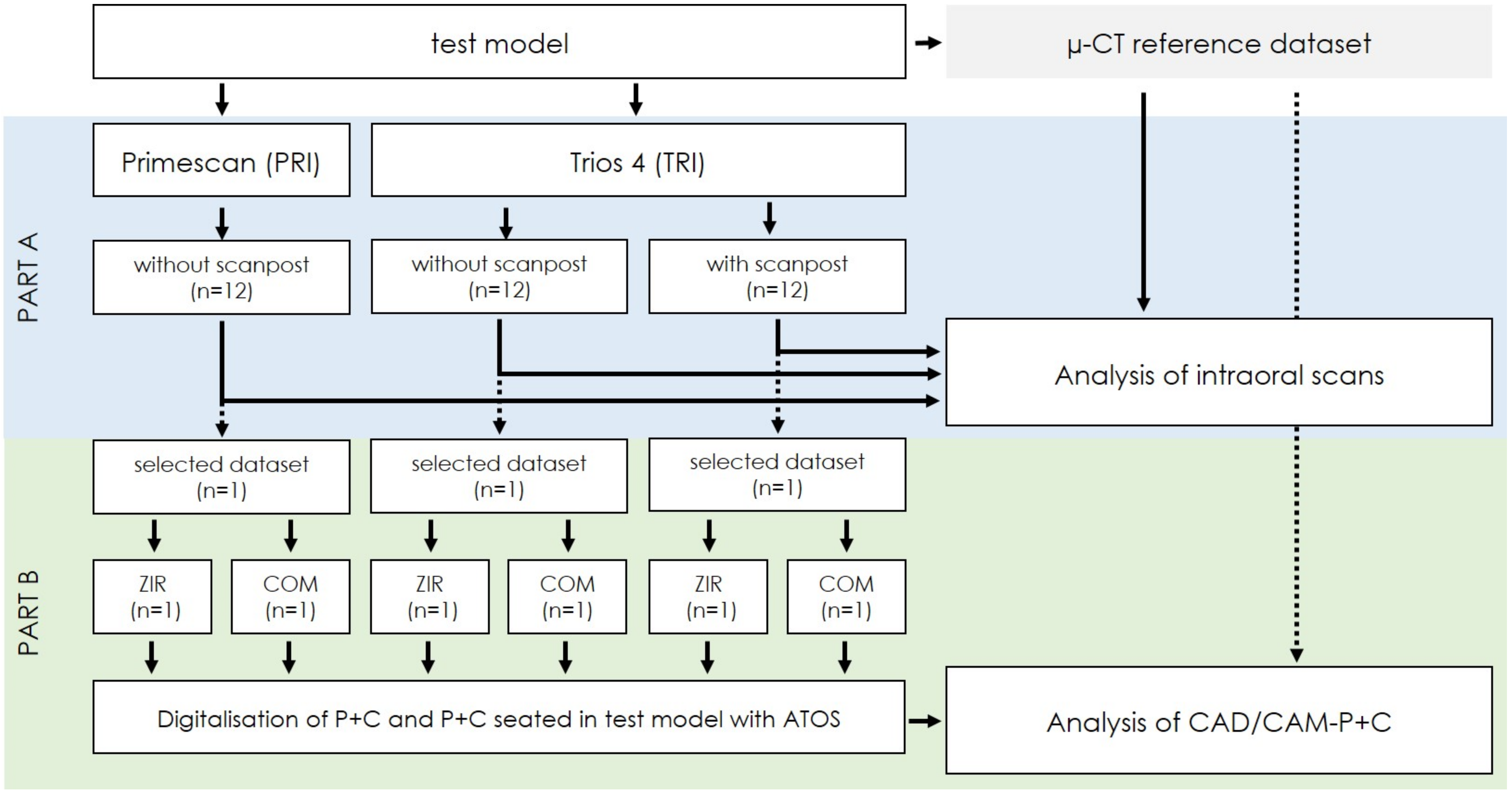
2. Materials and Methods
2.1. Test Models
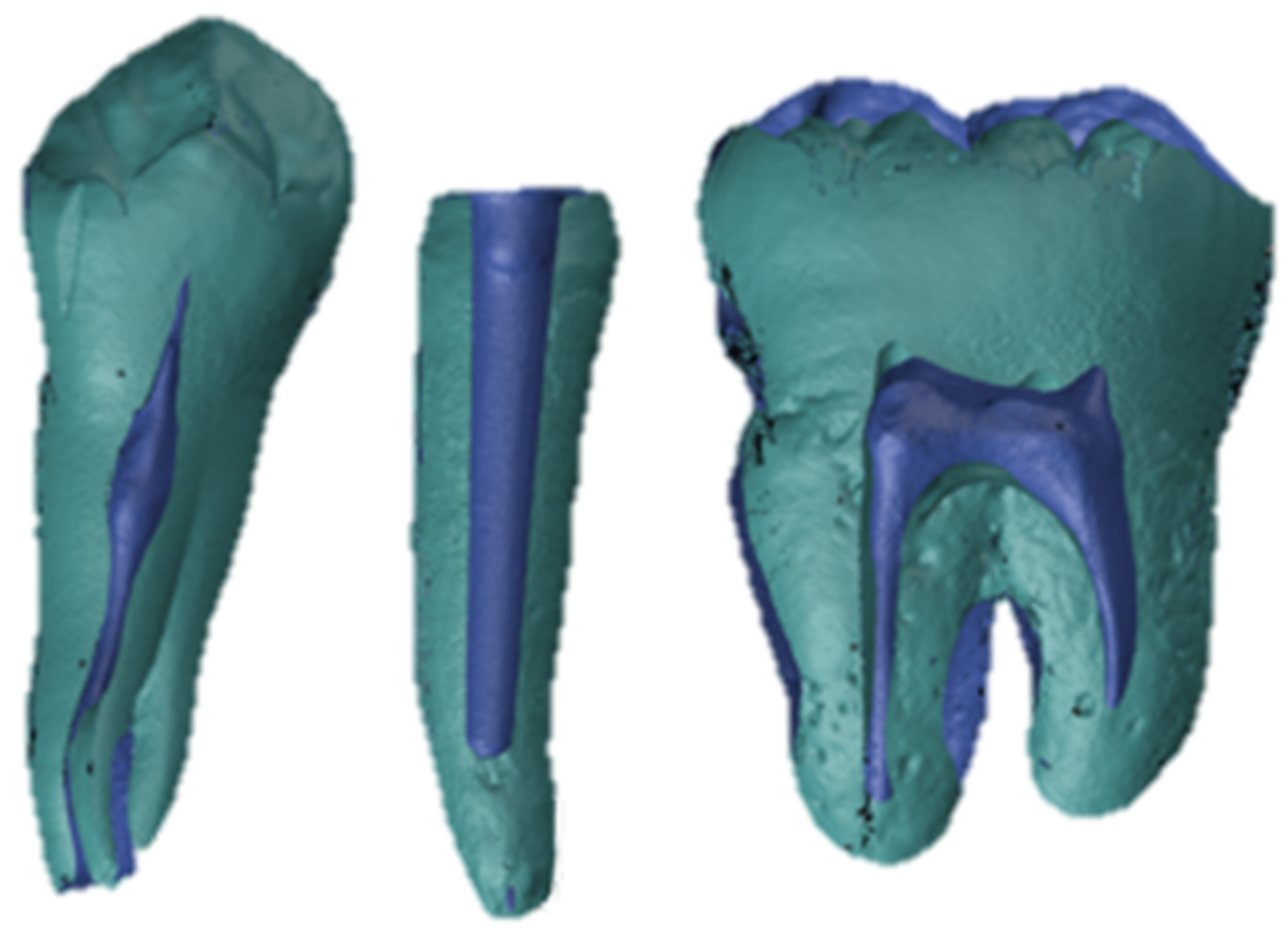
2.2. Reference Dataset
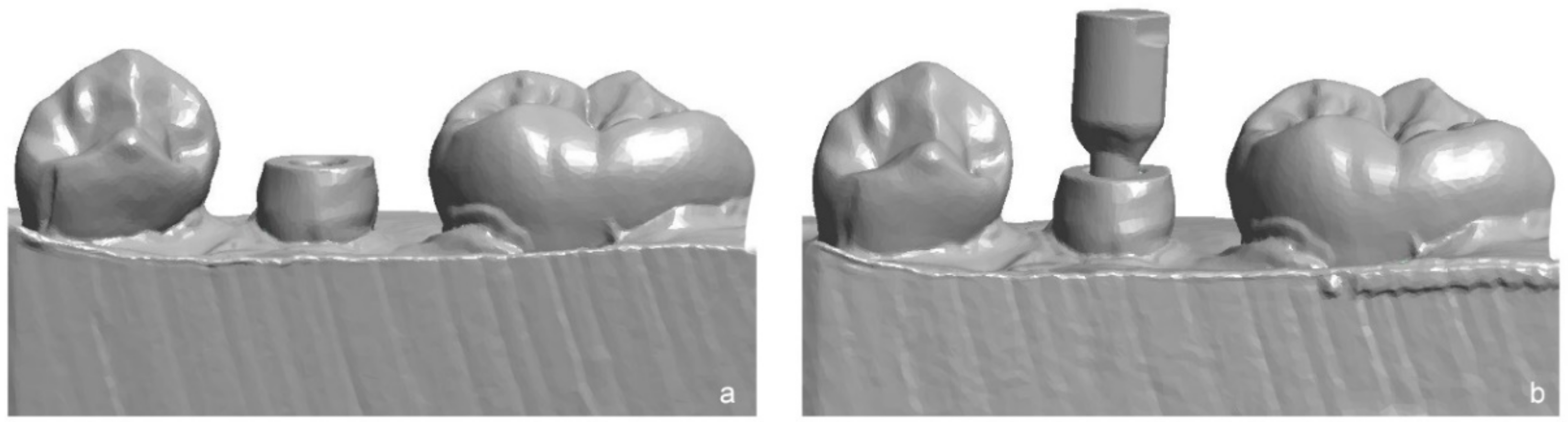
2.3. Impression Taking with IOS
2.4. Fabrication of CAD/CAM-P+C
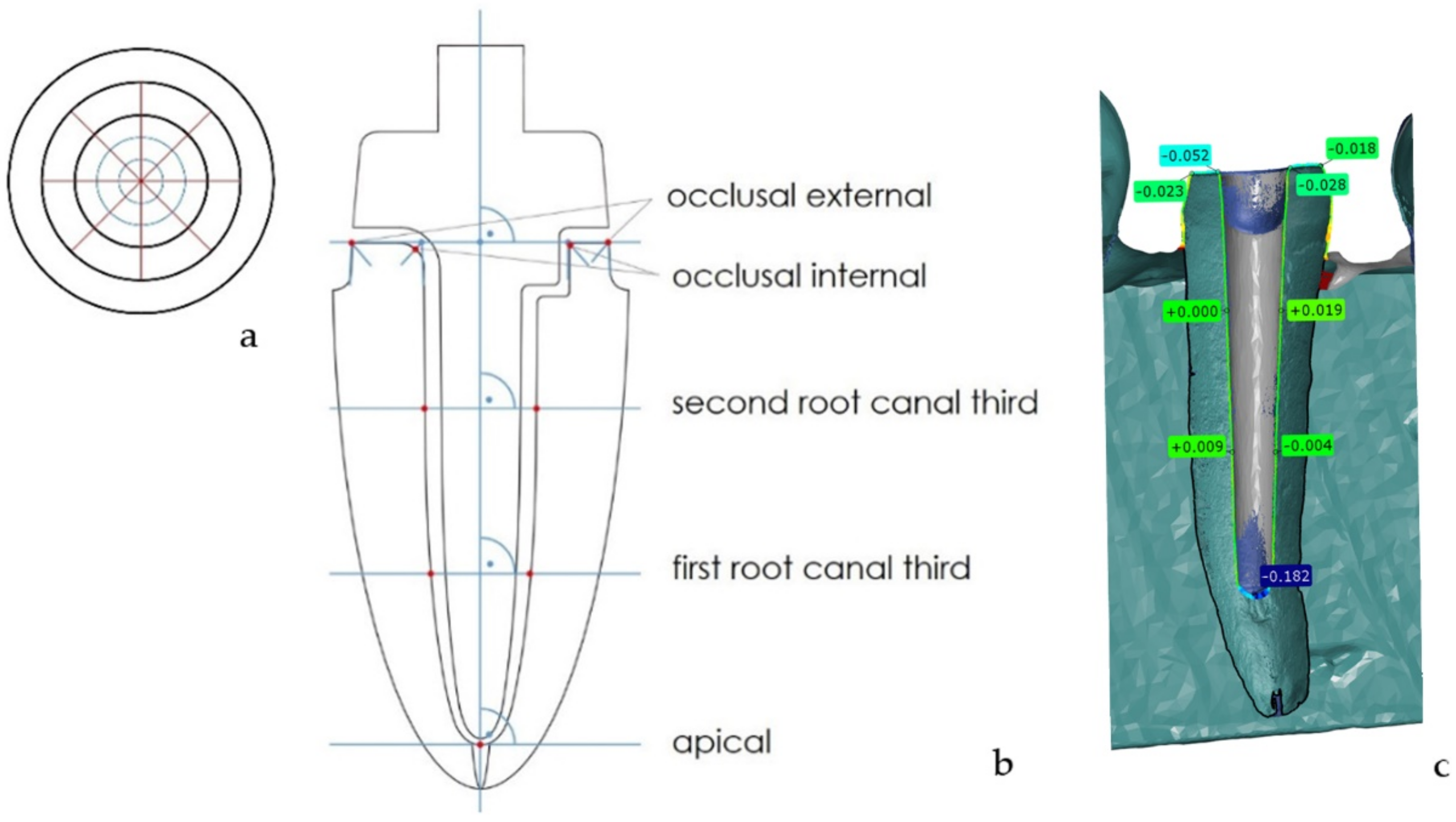
2.5. Analysis of the IOS Datasets (Part A)
2.6. Analysis of the CAD/CAM-P+C (Part B)
2.7. Statistical Analysis
3. Results
3.1. Accuracy of Digital Impression Taking with IOS (Part A)
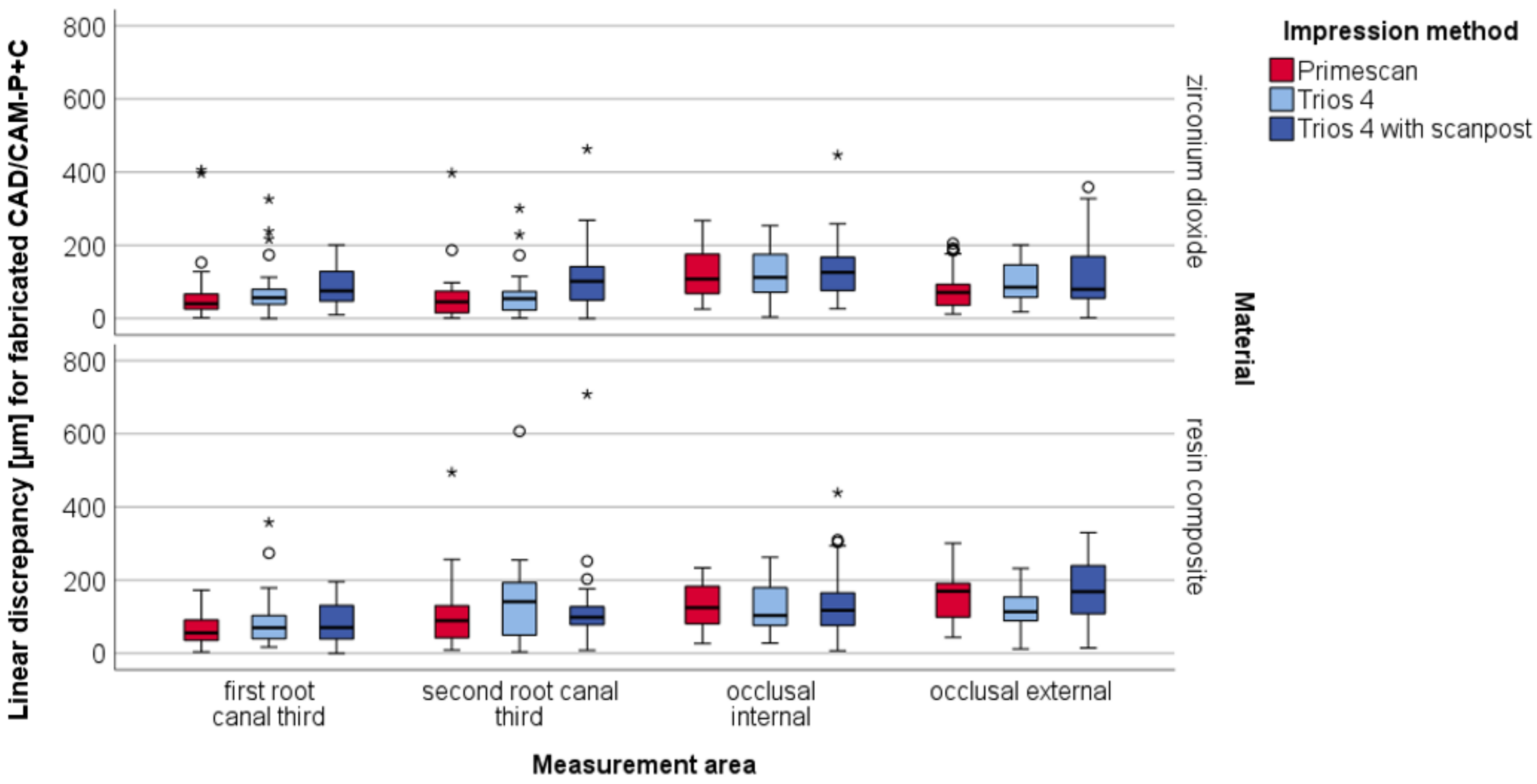
3.2. Accuracy of Fit of CAD/CAM-P+C (Part B)
4. Discussion
4.1. Digital Impression Taking with IOS (Part A)
4.2. Accuracy CAD/CAM-P+C (Part B)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferrini, F.; Sannino, G.; Chiola, C.; Capparé, P.; Gastaldi, G.; Gherlone, E.F. Influence of Intra-Oral Scanner (I.O.S.) on The Marginal Accuracy of CAD/CAM Single Crowns. Int. J. Environ. Res. Public Health 2019, 16, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naumann, M.; Schmitter, M.; Frankenberger, R.; Krastl, G. “Ferrule comes first. post is second!” fake news and alternative facts? A systematic review. J. Endod. 2018, 44, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Zarow, M.; Ramirez-Sebastia, A.; Paolone, G.; de Ribot Porta, J.; Mora, J.; Espona, J.; Duran-Sindreu, F.; Roig, M. A new classification system for the restoration of root filled teeth. Int. Endod. J. 2018, 51, 318–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bittner, N.; Hill, T.; Randi, A. Evaluation of a one-piece milled zirconia post and core with different post-and-core systems: An in vitro study. J. Prosthet. Dent. 2010, 103, 369–379. [Google Scholar] [CrossRef]
- Moustapha, G.; AlShwaimi, E.; Silwadi, M.; Ounsi, H.; Ferrari, M.; Salameh, Z. Marginal and internal fit of CAD/CAM fiber post and cores. Int. J. Comput. Dent. 2019, 22, 45–53. [Google Scholar]
- Theodosopoulou, J.N.; Chochlidakis, K.M. A systematic review of dowel (post) and core materials and systems. J. Prosthodont. Implant Esthet. Reconstr. Dent. 2009, 18, 464–472. [Google Scholar] [CrossRef]
- Alkhatri, R.; Saleh, A.R.M.; Kheder, W. Evaluating fracture resistance and failure modes of root filled teeth restored with CAD/CAM-fabricated post and core. Clin. Cosmet. Investig. Dent. 2019, 11, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Ausiello, P.; Gloria, A.; Maietta, S.; Watts, D.C.; Martorelli, M. Stress Distributions for Hybrid Composite Endodontic Post Designs with and without a Ferrule: FEA Study. Polymers 2020, 12, 1836. [Google Scholar] [CrossRef]
- Awad, M.A.; Marghalani, T.Y. Fabrication of a custom-made ceramic post and core using CAD-CAM technology. J. Prosthet. Dent. 2007, 98, 161–162. [Google Scholar] [CrossRef]
- Sary, S.B.; Samah, M.S.; Walid, A.A. Effect of restoration technique on resistance to fracture of endodontically treated anterior teeth with flared root canals. J. Biomed. Res. 2019, 33, 131–138. [Google Scholar] [CrossRef]
- Guven, M.C.; Dayan, S.C.; Yildirim, G.; Mumcu, E. Custom and prefabricated PolyEtherKetoneKetone (PEKK) post-core systems bond strength: Scanning electron microscopy evaluation. Microsc. Res. Tech. 2020, 83, 804–810. [Google Scholar] [CrossRef]
- Eid, R.Y.; Koken, S.; Baba, N.Z.; Ounsi, H.; Ferrari, M.; Salameh, Z. Effect of fabrication technique and thermal cycling on the bonds trength of CAD/CAM milled custom fit anatomical post and cores: An in vitro study. J. Prosthodont. 2019, 28, 898–905. [Google Scholar] [CrossRef]
- Ozkurt, Z.; Iseri, U.; Kazazoglu, E. Zirconia ceramic post systems: A literature review and a case report. Dent. Mater. J. 2010, 29, 233–245. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Pei, X.; Pei, X.; Wan, Q.; Chen, J.; Wang, J. Success and complication rates of root-filled teeth restored with zirconia posts: A critical review. Int. J. Prosthodont. 2019, 32, 411–419. [Google Scholar] [CrossRef]
- Schriwer, C.; Skjold, A.; Gjerdet, N.R.; Oilo, M. Monolithic zirconia dental crowns. internal fit, margin quality, fracture mode and load at fracture. Dent. Mater. 2017, 33, 1012–1020. [Google Scholar] [CrossRef]
- Sorensen, J.A.; Engelman, M.J. Effect of post adaptation on fracture resistance of endodontically treated teeth. J. Prosthet. Dent. 1990, 64, 419–424. [Google Scholar] [CrossRef]
- Hendi, A.R.; Moharrami, M.; Siadat, H.; Hajmiragha, H.; Alikhasi, M. The effect of conventional, half-digital, and full-digital fabrication techniques on the retention and apical gap of post and core restorations. J. Prosthet. Dent. 2019, 121, 364.e1–364.e6. [Google Scholar] [CrossRef]
- Pinto, A.; Arcuri, L.; Carosi, P.; Nardi, R.; Libonati, A.; Ottria, L.; Campanella, V. In vitro evaluation of the post-space depth reading with an intraoral scanner (IOS) compared to a traditional silicon impression. Oral Implantol. (Rome) 2017, 10, 360–368. [Google Scholar] [CrossRef]
- Jafarian, Z.; Moharrami, M.; Sahebi, M.; Alikhasi, M. Adaptation and retention of conventional and digitally fabricated posts and cores in round and oval-shaped canals. Int. J. Prosthodont. 2020, 33, 91–98. [Google Scholar] [CrossRef]
- Chen, Z.; Li, Y.; Deng, X.; Wang, X. A novel computer-aided method to fabricate a custom one-piece glass fiber dowel-and-core based on digitized impression and crown preparation data. J. Prosthodont. 2014, 23, 276–283. [Google Scholar] [CrossRef]
- Schlenz, M.A.; Schubert, V.; Schmidt, A.; Wöstmann, B.; Ruf, S.; Klaus, K. Digital versus conventional impression taking focusing on interdental areas: A clinical trial. Int. J. Environ. Res. Public Health 2020, 17, 4725. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. Int. J. Comput. Dent. 2019, 22, 11–19. [Google Scholar] [PubMed]
- Schmidt, A.; Klussmann, L.; Wöstmann, B.; Schlenz, M.A. Accuracy of digital and conventional full-arch impressions in patients: An update. J. Clin. Med. 2020, 9, 688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsintsadze, N.; Juloski, J.; Carrabba, M.; Tricarico, M.; Goracci, C.; Vichi, A.; Ferrari, M.; Grandini, S. Performance of CAD/CAM fabricated fiber posts in oval-shaped root canals: An in vitro study. Am. J. Dent. 2017, 30, 248–254. [Google Scholar]
- Pitigoi-Aron, G.; Streacker, A.B.; Schulze, K.A.; Geissberger, M. Accuracy of cast posts and cores using a new investigative method. Gen. Dent. 2012, 60, e153–e157. [Google Scholar]
- De Moraes, A.P.; Poletto Neto, V.; Boscato, N.; Pereira-Cenci, T. Randomized clinical trial of the influence of impression technique on the fabrication of cast metal posts. J. Prosthet. Dent. 2016, 116, 47–51. [Google Scholar] [CrossRef]
- Da Costa, R.G.; Freire, A.; Caregnatto de Morais, E.C.; Machado de Souza, E.; Correr, G.M.; Rached, R.N. Effect of CAD/CAM glass fiber post-core on cement micromorphology and fracture resistance of endodontically treated roots. Am. J. Dent. 2017, 30, 3–8. [Google Scholar]
- 3Shape Germany Trios 4 Handbuch. Available online: https://ww2.3shape.com/de-de/knowledge-center/user-manuals#trios (accessed on 21 April 2020).
- Dentsply Sirona Deutschland Primescan AC Gebrauchsanweisung. Available online: https://manuals.sirona.com/home.HomeDmsDocument.download.html?id=92357 (accessed on 21 April 2020).
- Wesemann, C.; Kienbaum, H.; Thun, M.; Spies, B.C.; Beuer, F.; Bumann, A. Does ambient light affect the accuracy and scanning time of intraoral scans? J. Prosthet. Dent. 2020, 125, 924–931. [Google Scholar] [CrossRef]
- Holst, S.; Karl, M.; Wichmann, M.; Matta, R.E. A new triple-scan protocol for 3D fit assessment of dental restorations. Quintessence Int. 2011, 42, 651–657. [Google Scholar]
- Al-Omari, W.M.; Zagibeh, A.M. The retention of cast metal dowels fabricated by direct and indirect techniques. J. Prosthodont Implant Esthet. Reconstr. Dent. 2010, 19, 58–63. [Google Scholar] [CrossRef]
- Schlenz, M.A.; Vogler, J.; Schmidt, A.; Rehmann, P.; Wöstmann, B. New Intraoral Scanner-Based Chairside Measurement Method to Investigate the Internal Fit of Crowns: A Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 2182. [Google Scholar] [CrossRef] [Green Version]
- Campanella, V.; Carosi, P.; Casella, S.; Pinto, A.; Di Girolamo, M. Clinical fitting of a cast metal post and core obtained by means of an intraoral optical scanning (IOS) and digital workflow. J. Biol. Regul. Homeost. Agents 2019, 33, 43–50. [Google Scholar]
- Libonati, A.; Di Taranto, V.; Gallusi, G.; Montemurro, E.; Campanella, V. CAD/CAM customized glass fiber post and core with digital intraoral impression: A case report. Clin. Cosmet. Investig. Dent. 2020, 12, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, A.; Schlenz, M.A.; Liu, H.; Kämpe, H.S.; Wöstmann, B. The influence of hard- and software improvement of intraoral scanners on the implant transfer accuracy from 2012 to 2021: An in vitro study. Appl. Sci. 2021, 11, 7166. [Google Scholar] [CrossRef]
- Gurpinar, B.; Tak, O. Effect of pulp chamber depth on the accuracy of endocrown scans made with different intraoral scanners versus an industrial scanner: An in vitro study. J. Prosthet. Dent. 2022, 127, 430–437. [Google Scholar] [CrossRef]
- Park, J.M.; Kim, R.J.; Lee, K.W. Comparative reproducibility analysis of 6 intraoral scanners used on complex intracoronal preparations. J. Prosthet. Dent. 2020, 123, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Accuracy of intra-oral scans compared to conventional impression in vitro. Prim. Dent. J. 2019, 8, 34–39. [Google Scholar] [CrossRef]
- Gutmacher, Z.; Kelly, A.; Renne, W.; Hoover, M.; Mennito, A.; Teich, S.; Cayouette, M.; Ludlow, M. Evaluation of the accuracy of multiple digital impression systems on a fully edentulous maxilla. Quintessence Int. 2021, 52, 488–495. [Google Scholar] [CrossRef]
- Zimmermann, M.; Ender, A.; Mehl, A. Local accuracy of actual intraoral scanning systems for single-tooth preparations in vitro. J. Am. Dent. Assoc. 2020, 151, 127–135. [Google Scholar] [CrossRef]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Effect of software version on the accuracy of an intraoral scanning device. Int. J. Prosthodont. 2018, 31, 375–376. [Google Scholar] [CrossRef]
- Schlenz, M.A.; Fiege, C.; Schmidt, A.; Wöstmann, B. Microleakage of thin-walled monolithic zirconia and polymer-containing CAD-CAM crowns. J. Prosthet. Dent. 2021, 125, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Rutkunas, V.; Geciauskaite, A.; Jegelevicius, D.; Vaitiekunas, M. Accuracy of digital implant impressions with intraoral scanners. A systematic review. Eur. J. Oral Implantol. 2017, 10 (Suppl. S1), 101–120. [Google Scholar] [PubMed]
- Tsintsadze, N.; Juloski, J.; Carrabba, M.; Goracci, C.; Vichi, A.; Grandini, S.; Ferrari, M. Effects of scanning technique on in vitro performance of CAD/CAM-fabricated fiber posts. J. Oral Sci. 2018, 60, 262–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanduti, D.; Korat, L.; Kosec, T.; Legat, A.; Ovsenik, M.; Kopač, I. Comparison between accuracy of posts fabricated using a digital CAD/CAM technique and a conventional direct technique. Int. J. Prosthodont. 2021, 34, 212–220. [Google Scholar] [CrossRef]
- Scribante, A.; Vallittu, P.K.; Özcan, M. Fiber-Reinforced Composites for Dental Applications. BioMed Res. Int. 2018, 2018, 4734986. [Google Scholar] [CrossRef]
- Revilla-León, M.; Sadeghpour, M.; Özcan, M. A review of the applications of additive manufacturing technologies used to fabricate metals in implant dentistry. J. Prosthodont. 2020, 29, 579–593. [Google Scholar] [CrossRef]
- Capriotti, L.; Greco, K.; Paolone, G.; Sberna, M.T.; Cantatore, G. Removal of fiber posts during endodontic retreatments using ultrasonic tips: A comparison between two different endodontic fiber posts. G. Ital. Endod. 2018, 32, 47–50. [Google Scholar] [CrossRef]
- Josic, U.; Mazzitelli, C.; Maravic, T.; Comba, A.; Mayer-Santos, E.; Florenzano, F.; Breschi, L.; Mazzoni, A. Evaluation of Fiber Post Adhesion to Root Dentin Achieved with Different Composite Cements: 1-year In Vitro Results. J. Adhes. Dent. 2022, 24, 95–104. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviation | Material | Product Name | Brand | Lot Number | Expiration Date |
|---|---|---|---|---|---|
| ZIR | 3Y-TZP zirconium dioxid | dima Zirconia ST | Kulzer GmbH, Hanau, Germany | 26026 | 2025–07 |
| COM | resin composite | Brilliant Crios | Coltène/Whaledent AG, Altstätten, Switzerland | J72547 | 2022–12 |
| Measurement Area | TRI | TRI + SP | |
|---|---|---|---|
| apical | PRI | NS | NS |
| TRI | / | NS | |
| first root canal third | PRI | NS | p < 0.001 |
| TRI | / | p = 0.021 | |
| second root canal third | PRI | NS | NS |
| TRI | / | NS | |
| occlusal internal | PRI | NS | NS |
| TRI | / | NS | |
| occlusal external | PRI | p < 0.001 | p < 0.001 |
| TRI | / | p = 0.024 |
| Material | Impression Method | Mean ± Standard Deviation (µm) |
|---|---|---|
| zirconium dioxid | PRI | 84.57 ± 76.90 |
| TRI | 95.96 ± 77.08 | |
| TRI + SP | 144.89 ± 125.90 | |
| resin composite | PRI | 267.54 ± 502.35 |
| TRI | 259.59 ± 446.63 | |
| TRI + SP | 320.51 ± 674.87 |
| Material | Measurement Area | TRI | TRI + SP | |
|---|---|---|---|---|
| zirconium dioxid | apical | PRI | NS | p < 0.001 |
| TRI | / | p < 0.001 | ||
| first root canal third | PRI | NS | p = 0.033 | |
| TRI | / | NS | ||
| second root canal third | PRI | NS | p < 0.001 | |
| TRI | / | p = 0.005 | ||
| occlusal internal | PRI | NS | NS | |
| TRI | / | NS | ||
| occlusal external | PRI | NS | NS | |
| TRI | / | NS | ||
| resin composite | apical | PRI | NS | NS |
| TRI | / | NS | ||
| first root canal third | PRI | NS | NS | |
| TRI | / | NS | ||
| second root canal third | PRI | NS | NS | |
| TRI | / | NS | ||
| occlusal internal | PRI | NS | NS | |
| TRI | / | NS | ||
| occlusal external | PRI | p = 0.036 | NS | |
| TRI | / | p = 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leven, R.; Schmidt, A.; Binder, R.; Kampschulte, M.; Vogler, J.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital Impression Taking with Intraoral Scanners and Fabrication of CAD/CAM Posts and Cores in a Fully Digital Workflow. Materials 2022, 15, 4199. https://doi.org/10.3390/ma15124199
Leven R, Schmidt A, Binder R, Kampschulte M, Vogler J, Wöstmann B, Schlenz MA. Accuracy of Digital Impression Taking with Intraoral Scanners and Fabrication of CAD/CAM Posts and Cores in a Fully Digital Workflow. Materials. 2022; 15(12):4199. https://doi.org/10.3390/ma15124199
Chicago/Turabian StyleLeven, Robert, Alexander Schmidt, Roland Binder, Marian Kampschulte, Jonas Vogler, Bernd Wöstmann, and Maximiliane Amelie Schlenz. 2022. "Accuracy of Digital Impression Taking with Intraoral Scanners and Fabrication of CAD/CAM Posts and Cores in a Fully Digital Workflow" Materials 15, no. 12: 4199. https://doi.org/10.3390/ma15124199