Successes and Challenges: Inhaled Treatment Approaches Using Magnetic Nanoparticles in Cystic Fibrosis


1
Department of Pharmacology & Therapeutics, Lung Health Research Centre, School of Biomedical Sciences, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Parkville, VIC 3010, Australia
2
Department of Applied Physics, University of Granada, Av. Fuentenueva s/n, 18071 Granada, Spain
*
Authors to whom correspondence should be addressed.
Magnetochemistry 2020, 6(2), 25; https://doi.org/10.3390/magnetochemistry6020025
Submission received: 13 May 2020
/
Revised: 28 May 2020
/
Accepted: 2 June 2020
/
Published: 4 June 2020
(This article belongs to the Special Issue Magnetic Nanoparticles 2020)
Abstract
:Magnetic nanoparticles have been largely applied to increase the efficacy of antibiotics due to passive accumulation provided by enhancing permeability and retention, which is essential for the treatment of lung infections. Recurring lung infections such as in the life-shortening genetic disease cystic fibrosis (CF) are a major problem. The recent advent of the CF modulator drug ivacaftor, alone or in combination with lumacaftor or tezacaftor, has enabled systemic treatment of the majority of patients. Magnetic nanoparticles (MNPs) show unique properties such as biocompatibility and biodegradability as well as magnetic and heat-medicated characteristics. These properties make them suitable to be used as drug carriers and hyperthermia-based agents. Hyperthermia is a promising approach for the thermal activation therapy of several diseases, including pulmonary diseases. The benefits of delivering CF drugs via inhalation using MNPs as drug carriers afford application of sufficient therapeutic dosages directly to the primary target site, while avoiding potential suboptimal pharmacokinetics/pharmacodynamics and minimizing the risks of systemic toxicity. This review explores the multidisciplinary approach of using MNPs as vehicles of drug delivery. Additionally, we highlight advantages such as increased drug concentration at disease site, minimized drug loss and the possibility of specific cell targeting, while addressing major challenges for this emerging field.
1. Introduction
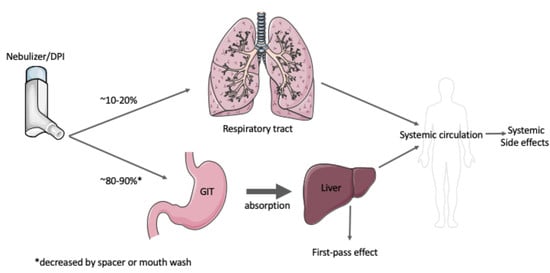
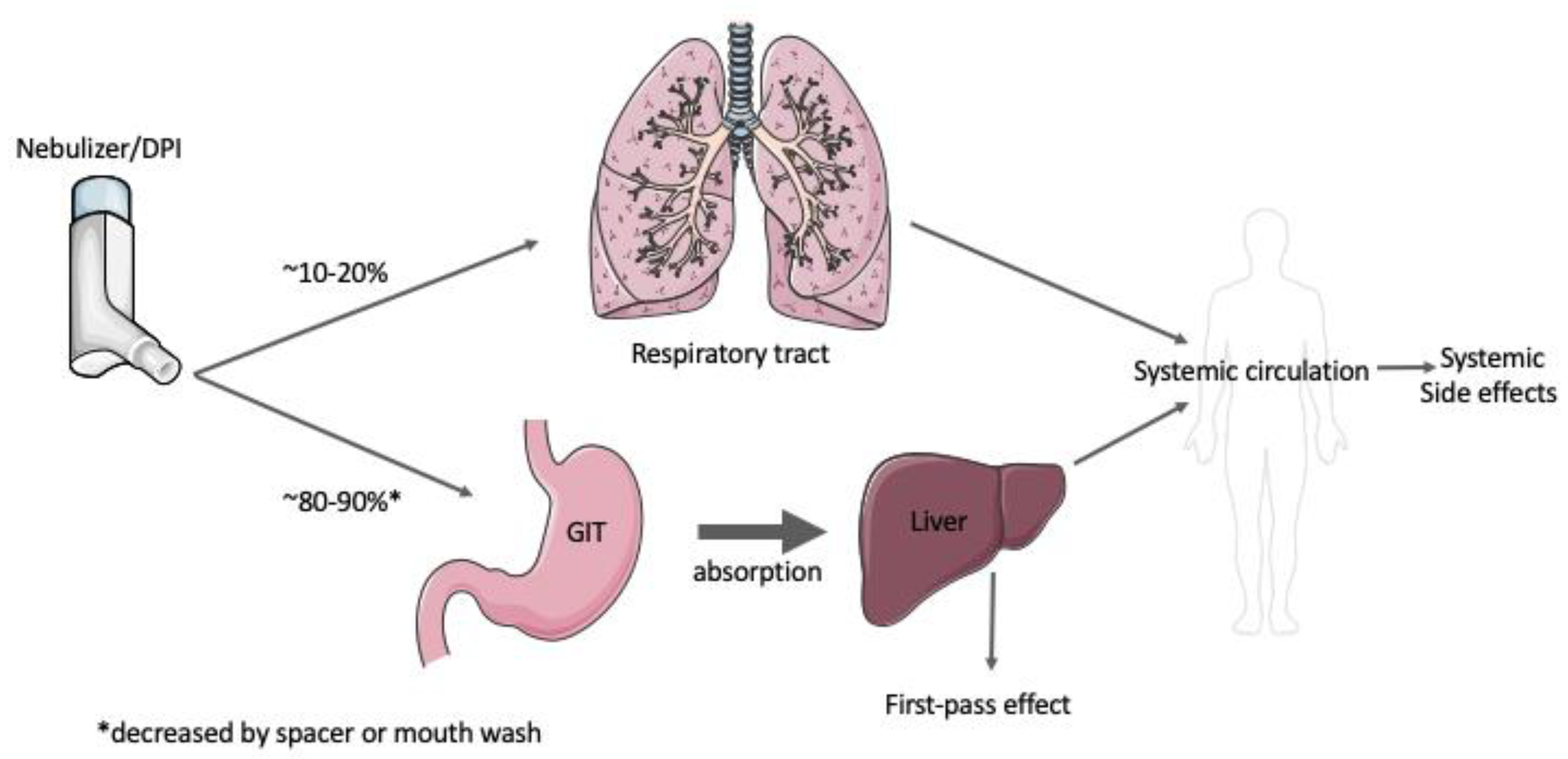
Inhalation of medications for respiratory diseases such as cystic fibrosis, asthma or chronic obstructive pulmonary disease (COPD) play a pivotal role in the prophylaxis and treatment of these common respiratory diseases. The most effective treatments involve aerosolised drug administration delivering corticosteroids in asthma or COPD, or antibiotics in lung infections directly to the respiratory tract, thereby achieving sufficient drug concentrations. A major advantage in delivering drugs directly to the lung is that aerosolised administration significantly decreases potential toxicity associated with systemic exposure (Figure 1).
Ultrasonic systems, jet systems, and other systems using a vibrating mesh/aperture plate are employed as the primary tools for aerosolised pulmonary delivery of drugs via nebulization [1].
1.1. Cystic Fibrosis
1.1.1. An Introduction to the Disease
Cystic fibrosis (CF) is an autosomal recessive genetic disease caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. CF is the most common genetic disease in Caucasian populations [2]. To date, more than 2000 CFTR protein mutations have been identified and categorised into six functional classes I to VI, based on different underlying mutations and disease outcomes (Table 1) [3]. CFTR is a transmembrane protein that is expressed at high levels on apical membrane epithelial cells and regulates the transport of ions such as sodium, chloride and bicarbonate [4]. This disease affects exocrine mucus glands of the lung, pancreas, liver and intestines and is characterised by progressive lung disease and pancreatic insufficiency [3]. Dysfunction in the CFTR results in impaired chloride ion secretion, hyperabsorption of sodium ions and subsequent production of mucus that is thick, viscous and difficult to clear [3]. This is particularly problematic in the respiratory tract where the production of viscous mucus causes a reduction in mucociliary clearance and initiates a vicious cycle of recurrent and persistent bacterial infections [5,6]. These conditions result in a vicious cycle of pulmonary exacerbations, predisposing CF patients to progressive loss of lung function, respiratory failure and consequently death [7].
1.1.2. Current Treatments
Conventional existing CF treatments have predominantly been symptomatic therapy focused on attenuating disease progression and maintaining lung function [5,8]. Antibiotics and anti-inflammatory drugs are administered to control bacterial infections and inflammation [5,8], while bronchodilators, mucolytics and osmotic agents are administered to remove mucus and clear airways [9]. More recently, a large focus has been placed on CFTR modulators designed to target certain biological consequences that are characteristic of CFTR mutation classes or correct specific CFTR gene mutations, and these are discussed below.
CFTR Modulators
Since the development of CFTR modulators, these small therapy treatments have significantly improved the quality of life for CF patients with specific CFTR mutations, namely ivacaftor, lumacaftor, tezacaftor and, recently, elexacaftor. Ivacaftor is the first FDA (Food and Drug Administration )-approved CFTR potentiator drug that addresses the specific G551D gating mutation (class III mutation, affects 4%–6% of CF population) [10]. Ivacaftor monotherapy was later approved for use of additional gating mutations [11]. In 2015, the FDA approved the first combination formulation, combining ivacaftor with the first CFTR corrector, lumacaftor [10]. Subsequently, tezacaftor, a second-generation corrector, gained approval for combination use with the potentiator ivacaftor [12]. This dual combination approach of combining a CFTR corrector, which rescues F508del CFTR to the cell surface, with a CFTR potentiator that potentiates CFTR channel activity, effectively expands the treatment window to the majority of CF; however, some mutations like nonsense mutations remain unrescuable with CFTR modulator treatment [13]. Effort continues to be put into developing next-generation potentiators and correctors with the aim to offer treatment options for all patients with CF [14].
Antibiotics
An essential pillar of pulmonary treatment in CF is the use of antibiotics, which have led to a significant improvement in prognosis since the 1960s [5]. In the CF airway, increased mucus viscosity and impairment of mucociliary clearance promotes bacterial colonization of airways. The most common airway pathogen in the adult CF population is Pseudomonas aeruginosa (P. aeruginosa), and colonisation with P. aeruginosa is directly correlated with a decline in lung function [5]. Other CF relevant organisms include Burkholderia cepacia as well as Haemophilus influenzae and Staphylococcus aureus, which are more commonly found in paediatric CF cohorts [5,15]. Long-term maintenance therapy with inhaled therapeutics is typically used to suppress infection, reduce pulmonary exacerbations and maintain lung function once chronic P. aeruginosa infection occurs [5]. Traditionally, tobramycin, aztreonam and colistin have been used for treatment of chronic P. aeruginosa infection in CF patients [5].
- Tobramycin
Inhaled tobramycin solution (TIS) was the first aerosolised antibiotic to be approved and is clinically available as a pre-mixed 300 mg/5 mL vial for use twice daily for cystic fibrosis patients [5,8]. Since then, new dry powder formulations have been developed and the approval of tobramycin inhalation powder (TIP) was a breakthrough in inhalation therapy for CF. This dry powder formulation has been shown to have a shorter administration time, increased patient adherence and overall satisfaction than TIS [16,17]. Previous studies have shown improved delivery of tobramycin through thick mucus and enhanced treatment of planktonic P. aeruginosa via conjugating its amino groups with carboxyl groups of citric acid-coated magnetic nanoparticles [18,19].
- Aztreonam
Aztreonam is a monocylic β-lactams antibiotic used via intravenous (i.v.) formulation for decades against Gram-negative bacteria [20]. Notably, several side effects including rash, nausea, vomiting and diarrhea have been reported in patients with CF [20]. A potential explanation is that the i.v. formulation contains arginine salt known to cause bronchoconstriction and induce airway inflammation [8,20]. Subsequently, arginine salt has since been substituted with lysine to allow an aerosolised application with less side effects [20].
- Colistinmethate Sodium
Colistin, also known as polymyxin E, is a last-line antibiotic against Gram-negative pathogens and in CF, and is used for treatment of chronic endobronchial P. aeruginosa infection [21]. Historically, colistin has been administered intravenously; however, its use has declined due to neurotoxicity and nephrotoxicity, in addition to less toxic alternatives, e.g., tobramycin [8]. The resurrection of colistin in recent times has been led by the lack of effective treatment options against multi-drug resistant pathogens in addition to the development of newer and safer formulations [8]. In CF, the inactive prodrug colistinmethate sodium (CMS) has been available to the clinic for decades [15,22].
Mucolytics and Osmotic Agents
CFTR dysfunction results in thick viscous mucus that is difficult to clear resulting in recurring lung infections [5]. Furthermore, increased neutrophil degeneration in CF releases large amounts of DNA spiralling down the vicious cycle of further increasing mucus viscosity [23]. Two leading mucoactive agents are N-acetyl cysteine (NAC) and recombinant human deoxyribonuclease I (rhDNase, also knows as dornase alfa) [8,9]. NAC decreases mucus viscosity by disrupting disulphide bonds connecting mucin proteins in mucus [8]. rhDNase enzymatically breaks down DNA in airway secretions, reducing the size of DNA released in sputum [8].
Another therapeutic approach to aid rehydration of airway surfaces and sputum clearance is the use of inhaled hypertonic saline [23]. Beneficially, inhaled hypertonic saline was found to also improve lung function and reduce the number of pulmonary exacerbations [24]. Unfortunately, the use of a nebuliser has proven to be a major obstacle due to logistical difficulties in requiring an electrical supply element, as well as thorough cleaning and disinfection procedures after each single use [25].
1.2. Magnetic Nanoparticles
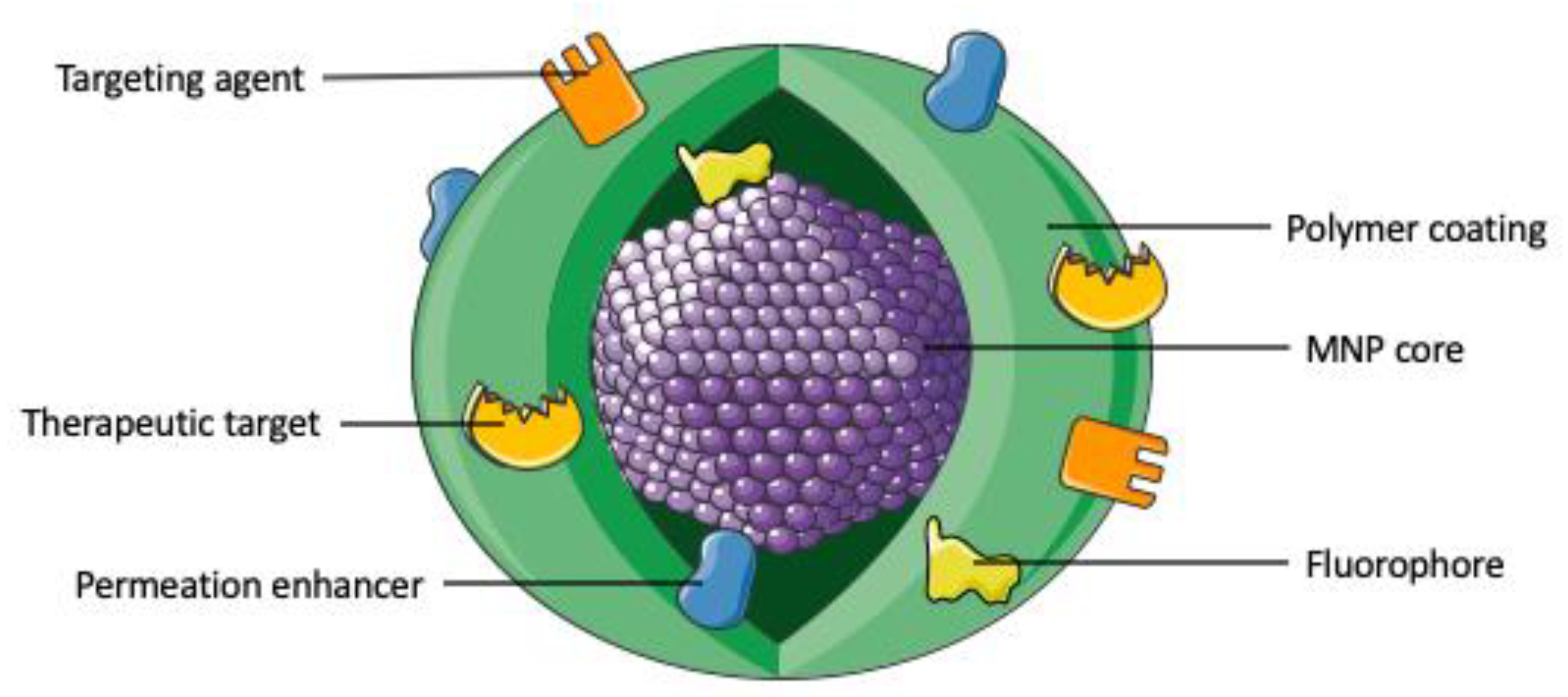
The symbiotic marriage of targeted drug delivery with nanopharmacy has resulted in a number of designs for nanoscale, making magnetic materials ideal for the application as drug delivery carriers (Figure 2, Table 2) [26].
Due to low toxicity, the most commonly used magnetic nanoparticles (MNPs) employ ferromagnetic elements, such as iron, nickel and cobalt, and their compounds, ferrites, magnetite and maghemite [26]. The two main forms of FDA-approved compounds, maghemite (Fe2O3) and magnetite (Fe3O4), can be easily synthesized with controlled size and shape [36,37]. In the past decade, their application in the diagnosis and treatment of various diseases like cancer has grown exponentially; importantly, they offer novel delivery options for respiratory diseases [38,39,40].
MNPs can be synthetised using a great variety of methods, with the most frequently used being co-precipitation, high temperature decomposition of organic precursors, hydrothermal, microemulsions and sol-gel polymerization [41]. They can be easily used as drug carriers since they can modulate the release of different drugs by the application of different frequencies and intensities of an applied external magnetic field. Furthermore, the magnetic properties of these MNPs influence the drug release profile; for example, the specific absorption rate or the saturation of the magnetisation depending on the morphology and anisotropy of the particles [42]. It has been demonstrated that, for example, cubic or octopod iron oxide nanoparticles have superior magnetic heating efficiency as compared to spherical particles of similar sizes [43]. The adsorption of these drugs could be using physical or chemical methods; for example, physical encapsulation using ionic complexation, nanoprecipitation, emulsions, gelations, etc.
MNPs can be used in hyperthermia as heat mediators, which can convert magnetic energy into thermal energy under the influence of external magnetic field. In hyperthermia, upon applying an external magnetic field, the alternative magnetic field (AMF) oscillates. This oscillation is faster than the relaxation time of MNP and thus causes a delay of magnetic moment relaxation resulting in the generation of heat. MNPs mediate heat via the relaxation losses which occur via Neel relaxation and Brownian relaxation. The Neel relaxation is a result of reorientation of magnetic moment in the same direction as the applied magnetic field, and it is size-dependent and prevails in small NPs only. On the other hand, Brownian relaxation is a kind of friction force resulting from the rotation of the NPs in the liquid suspension. Brownian relaxation is both size and viscosity dependent. The amount of released heat is quantified via measuring the specific absorption rate (SAR) [26]. Intensive efforts have focused on developing optimised synthesis protocols for the obtaining of MNPs with reproducible, uniform and well-defined sizes and shapes that also show superparamagnetic behaviour. Superparamagnetism allows MNPs under the control of an external magnetic field to deliver the drug directly to a desired part of the lung while keeping healthy cells away from exposure. In addition, the local hyperthermic effect of MNPs enables magnetically triggered drug release profiles. Most importantly, MNPs play a vital role in the treatment of CF via acting as nano-knives, under the effect of external magnetic field, which can penetrate the thick mucus and biofilm layers to allow the exposure of micro-organisms and inflamed cells to the delivered drugs [44]. It is noteworthy that MNPs can also be employed for other respiratory diseases. Tanmoy Sadhukha et al. (2013) demonstrated that magnetic hyperthermia was particularly suitable for the treatment of lung cancer, where the external AMF can be easily focused [45]. The relatively inert nature of magnetic substances in the absence of magnetic fields and their efficacy in the presence of AMF make this technique highly suitable for achieving an on-demand response. Furthermore, lungs are filled with air, which act as a poor conductor of heat. Thus, the heat generated by the particles in the lungs is less likely to affect the surrounding organs such as the heart. These authors described that instillation or inhalation of iron magnetic nanoparticles results in an effective therapeutic magnetic hyperthermia treatment of in vivo tumor growth in lungs, with minimal exposure to other organs [45].
To display optimal efficiency for biological application, colloidal suspensions of MNPs require long-time stability in aqueous media as well as a magnetic core responsive to an external magnetic field, allowing optimal formation.
1.3. Inhaled Therapeutics
As lung delivery presents itself as the major therapeutic target in CF, inhalation drug delivery offers novel strategies for existing and emerging therapeutic agents [46]. Inhalation administration allows the delivery of high drug doses directly to the site of action while minimising potential side effects and risk of systemic toxicity [5,8]. Additional benefits include fast-acting and non-invasive applications, high compliance and suitability for home therapy [8]. Although the benefits of inhalation therapy are undeniable, the aforementioned lung delivery comes with indisputable drawbacks like large variability in drug absorption, ambiguity regarding target specific concentrations as well as local specific side effects including counterproductive chest tightness and wheezing [7,20]. Furthermore, efficient inhalation delivery is hampered by difficulties in drug formulations including ideal particle size and powder flowability [46].
Magnetic nanoparticles can be useful to overcome all these difficulties since aerosol deposition can be magnetically targeted to a region of interest in the lung via the presence of a target-directed external magnetic field. Using superparamagnetic iron oxide NPs (SPIONs) in aerosol droplets (nanomagnetosol), where the SPIONs are physically connected by a solvent, was shown to increase the magnetic moment and improve the magnetic targeting efficacy [47]. The combination of the direct magnetic field with a simultaneous perpendicular, high frequency alternating magnetic field induced vibrations that caused a local increase in temperature and facilitate NP transport through the mucus. Magnetic hyperthermia was shown to be an effective method for decreasing the viscosity of biofilms and mucus, as well as enhancing drug and immune cell penetration to the affected area. Furthermore, bacterial growth is strongly temperature dependent, so hyperthermia can noticeably reduce the formation and growth of biofilms. Therefore, the disruption of biofilms and the retardation of S. aureus growth can be controlled by the surface coating of SPIONs, such as carboxylate functionalized SPIONs [48].
Current devices for drug delivery via inhalation can be broadly categorized into, firstly, aerosols delivered via nebulizers and, secondly, dry powders for inhalation delivered by dry powder inhalers (DPIs). The characteristics of these devices are summarised in Table 3.
1.4. Approved Inhaled Antibiotics for the Treatment of Lung Infections in CF
An overview of approved inhalation treatment options for CF is summarized in Table 4. Tobramycin (TIP) capsules formulated with low density porous particles have been shown to improve flow and dispersion by inhalation [5]. To date, two phase III studies have investigated the efficacy and safety of this novel and FDA-approved formulation. The EVOLVE study reported the efficacy of TIP-formulated tobramycin in 95 patients over placebo, with significantly improved FEV1 (forced expiratory volume in one second) during treatment for 84 days [50]. The larger scale EAGER study of 553 patients compared the use of 3 treatment cycles of TIP (with TIS) and demonstrated similar efficacy of microbial response with higher treatment satisfaction [17]. In both studies, no severe adverse reactions were reported, with only cough being the most frequently reported adverse reaction related to the dry powder. In this study, the authors concluded that the recommended dose for patients with CF is 112 mg (four 28 mg capsules) inhaled twice daily with alternating 28 day on-treatment and off-treatment cycles [5]. Notably, mild adverse reactions to inhaled tobramycin also include tinnitus and hoarseness; however, prolonged exposure may result in a cumulative effect potentially causing nephrotoxicity and ototoxicity [20].
More recently, lyophilized formulations which increase the product stability of dry powder were developed for unstable antibiotics such as aztreonam and colistin. Aztreonam lysine (AZLI) has been approved for use with a nebulizer [5,51]. It is available to CF patients of 6 years or older, with the recommended dose of 75 mg inhaled thrice daily and with alternating 28 day on-treatment and off-treatment cycles [5]. Importantly, inhaled aztreonam was shown to significantly improve lung function, respiratory symptoms such as cough, sputum production and wheezing, as well as reducing bacterial density in sputum by suppressing chronic P. aeruginosa infections (which has long term effects on patient survival) [5].
Colistimethate sodium salt (CMS) has been approved as a dry powder formulation in Europe for treatment of chronic P. aeruginosa infections in CF patients of 6 years and older. The recommended dose is a 125 mg capsule taken twice daily, administered using a hand-held inhaler [52]. A phase III open-label trial showed that colistimethate sodium DPI was well tolerated and effective [52]. Additionally, patients reported several advantages of using the DPI formulation over the nebulised solution formulation including shorter administration time and enhanced portability [8,52].
1.5. Approved Inhaled Mucolytics and Osmotic Agents
Approved inhaled mucolytics and osmotic agents include inhaled mannitol and hypertonic saline (Table 4). Inhaled mannitol administered as a dry powder formulation has been shown to hydrate airway surfaces and additionally improve mucus clearance [25]. Two phase III studies reported increase in FEV1, albeit no significant improvements were observed in children (6–11 years old) or adolescents (12–17 years old). Furthermore, a 29% reduction of pulmonary exacerbation was reported in patients given 400 mg of inhaled mannitol [53]. Additionally, sustained improvement in lung function over 6 months indicates inhaled mannitol to be an important treatment for CF [53,54]. Inhaled mannitol is administered as a 400 mg dose twice daily, dispensed with an inhaler using 10 individually loaded capsules [53]. Despite no reports of serious respiratory events, patients suffered from cough episodes which led 21.1% in the mannitol group and 16.7% in the control group to the discontinuation of the treatment [53].
1.6. Inhaled Antibiotics in Clinical Trials
In CF, one of the major challenges is the need for alternative antibiotic options as inhaled antibiotics such as tobramycin to be prescribed on an ‘on-off’ regimen (Table 4). The question of what alternate antibiotic to then use can often be very challenging, highlighting the need for more effect treatment options [58]. Fluoroquinolones have traditionally been used in CF due to their large spectrum of bactericidal activity, rapid cellular uptake and excellent bioavailability and tolerance [8]. Inhaled fluoroquinolones, e.g., ciprofloxacin and levofloxacin, are currently in phase III clinical trials (NCT01270347 and NCT01180634) to assess their effect as the second alternate antibiotic during “off” cycles of TIS to avoid drug resistance and improve patient outcomes [8].
Ciprofloxacin is a second generation fluoroquinolone that has been reformulated as a dry powder formulation with low density porous particles for the management of chronic P. aeruginosa infections in CF patients [5]. Phase I studies in paediatric and adult CF patients using single and multiple dose administration showed high concentrations in the lung were achieved with low systemic exposure [5]. A phase II study with the inhaled dry powder ciprofloxacin given at two doses (32.5 mg and 48.75 mg) twice daily for 28 days showed a significant reduction in the density of P. aeruginosa when compared to placebo [55]. Nevertheless, this effect was not sustained to the end of the study where the difference was found to be not significant when compared to placebo [55]. Although a trend in improving the quality of life was reported, the study failed to improve the primary endpoint FEV1. Furthermore, no significant changes were reported for other endpoints such as respiratory symptoms or pulmonary exacerbations [55]. A sunlight sensitivity rash, cartilage toxicity and the emergence of resistance were some of the main side effects [8]. In contrast to the CF study, a separate phase II study using ciprofloxacin DPI has demonstrated a positive effect in patients with bronchiectasis and is currently undergoing phase III trials [58].
Recently, a magnetically triggered release method of ciprofloxacin has been obtained using magnetic poly(lactic-co-glycolic) acid (PLGA) micro/NPs. The attained hyperthermic activity of the developed MNPs upon applying AMF has enhanced the drug release. In particular, the obtained results showed a twofold increase in ciprofloxacin release from MNPs-PLGA NPs as compared with the nonmagnetic PLGA NPs [59].
A phase II study showed inhaled levofloxacin, a third generation fluoroquinolone, was well tolerated, and a reduction in P. aeruginosa density and a dose-dependent increase in FEV1 was observed (in 240 mg given twice daily group) when compared to placebo [60]. Further pharmacokinetic studies highlighted low systemic exposure with high levels in sputum [60]. However, a randomised phase III study with 335 participants given either inhaled levofloxacin (n = 220, solution) or placebo (n = 110) did not demonstrate a clear benefit in reducing or delaying pulmonary exacerbations [56]. Treatment-related dysgeusia was reported in 35.2% of the inhaled levofloxacin group during treatment duration, with other reported side effects in both treatment groups being cough, nausea, pyrexia and haemoptysis [56]. Similar reasons such as disease progression and dysgeusia were reported for the discontinuation of the study in both groups [56]. Another phase III study comprising of 282 CF patients evaluated the safety and efficacy of inhaled levofloxacin (n = 189) to TIS (n = 93) [57]. Inhaled levofloxacin was well tolerated and demonstrated non-inferiority to TIS [57]. Treatment-related side effects were reported by 22% of the inhaled levofloxacin group and 32.2% of the TIS group [57]. Discontinuation and occurrence of side effects were similar between both groups, with dysgeusia being reported as the most frequent adverse event [57].
Taken together, new methods of drug delivery and technology are needed to address issues of antibiotic resistance, adverse treatment-related side effects and improved therapeutics for the CF population.
1.7. Gene Delivery
The successful cloning of the CFTR gene in 1989 marks a major breakthrough in the recent development of gene therapy in cystic fibrosis [61,62,63]. Unfortunately, current efforts have only been partially successful as, firstly, lung gene transfer proves to be inefficient and, secondly, a complete understanding of gene transfer agents is crucial [64]. A major conceptual advantage of gene therapy over small molecules such as CFTR modulators is that gene therapy could potentially treat all classes of CF [12]. To date, the most challenging hurdle for CF gene therapy remains drug delivery.
1.7.1. Barriers to Gene Delivery
Lung delivery continues to prove a difficult target due to effective intra- and extracellular barriers shielding the lung from inhaled material. Additionally, extracellular barriers include mucociliary clearance and immune response mechanisms [65,66,67,68]. Amongst typical biological barriers to lung drug delivery, the CF lung proves to be an added challenge in the form of a thick mucus layer blocking access to epithelial lung cells.
1.7.2. Mucus-Penetrating Magnetic Nanoparticles (MNPs)
To date, one of the greatest challenges in treating CF with MNPs is the successful penetration of the thick, sticky mucus that is characteristic of CF disease. The CF mucus architecture sterically hinders drug delivery to the lung and reduces drug delivery efficacy [9]. Due to their small size, MNPs have emerged as promising vehicles to package drugs and transport through the mucus, with increasing penetration resulting in higher delivery rates. Magnetite (Fe3O4) is preferred over maghemite (Fe2O3) as core material since Fe3+ is naturally internalized by many pathogenic bacteria and triggers targeting [69]. One example is the study carried out by Scherer et al. (2002) that describes the use of poly(ethylene imine)-coated MNPs as a gene vector [70]. The magnetic field was applied to these MNPs in an in vitro study and showed a significant improvement in the rapid accumulation of gene vector in the targeted cells.
The use of MNPs in combination with gene therapy also includes the attachment of viruses to the surface of MNPs to enhance the transfection efficiency. Morishita et al. (2005) attached HVJ-E virus loaded with the gene vector to the surface of protamine sulfate (PS)-coated MNPs [71]. This study was implemented using the EGFP (Ehhanced Green Fluorescent Protein) gene and FITC-oligodeoxynucleotide for baby hamster kidney cells and examined the luciferase gene in COS7 cells, obtaining a significant enhancement in the transfection efficiency in a dose-dependent manner.
In summary, the efficient penetration of MNPs into the mucus phase can be achieved by eliminating potential electrostatic interactions of MNPs with mucus by coating MNPs with electrostatically neutral molecules such as polyethylenglycol (PEG) or increasing mucus penetration by mucus-inert add-ons or mycolytics attached to the MNP [72,73]. Notably, MNPs offer the potential to deliver not only antibiotics directly to the lung, but also the aforementioned gene therapy approach. Suk et al. (2011) compared the diffusivity, displacement and transport rates of uncoated NPs with PEGylated NPs of 100, 200 and 500 nm [73]. The study concluded that coating of 200 nm PEGylation was optimal in regard to mucus penetration compared with uncoated, smaller and larger coated NPs. The PEG chain conformation and resulting effect of PEGylation degree was further investigated by Craparo et al. (2016), delivering nonsteroidal anti-inflammatory ibuprofen as a newly synthesised mucus-penetrating fluorescent NP [74]. To form grafted co-polymers with an average NP size <200 nm, the authors employed α,β-Poly(N-2-hydroxyethyl)-d,l-aspartamide (PHEA), thatwas covalently bound to rhodamine B (RhB) and polylactic acid (PLA), and further coated with 0%, 2% or 8.5% PEGylation. PEG density increases were reported to be directly correlated with increases of the penetrating ability of PHEA-RhB-PLA-PEG NPs, suggesting the PEG chain to be an important property for the activity of NPs.
Direct delivery of CFTR modulators to the lung offers potential benefits of correcting the CFTR at a major target side or contributing to the eradication of lung infections [15,75]. Porsio et al. (2018) developed an ~70 nm PEG-coated NP containing a transactivating transcriptional activator peptide (Tat) that was loaded with ivacaftor [75]. The authors reported that faster penetration and higher rates of ivacaftor release (12%) were achieved by their ivacaftor-loaded NP compared to free ivacaftor (6% release). This approach offers great potential for delivering CFTR modulators directly to the lung, although clinical trials are needed to confirm these findings in the clinic.
1.7.3. Non-Viral Vectors for Gene Delivery
For a comprehensive overview on viral vectors refer to the review by Griesenbach and Alton et al. (2013) [62] and Schneider-Futschik (2019) [12]. Non-viral vectors such as NPs have the potential to circumvent some of the viral vector-induced problems, such as limited packaging capacity or immune response [76]. Non-viral approaches include cationic liposomes, DNA nanoparticles/polymers and naked DNA. NPs can be developed with a variety of materials including several shapes and sizes, different surface charges and with specific targeting moieties (Table 5). In the past, the aforementioned mucolytics such as NAC and rhDNase were used to improve the delivery of non-viral gene carriers, albeit with varying outcomes.
MNPs can be used to transfer different genes, providing protection and stability to DNA and increasing the transformation efficiency and safety, namely magnetofection. The mechanism of magnetofection is similar to using transfection reagents with the only difference that the plasmids form complexes with cationic polymer-coated MNPs, for example poly(ethylenimine) (PEI)-coated MNPs [77]. Furthermore, MNPs display advantageous properties as they are not subjected to microbial interactions due to the inorganic nature of the metallic core. In addition, these nanoparticles can be functionalised with different functionalised groups, e.g., carboxyl, amines, biotin, polyethyleneimine and antibodies, allowing several methods of DNA or RNA attachment and, furthermore, suitable delivery of small interfering RNA or oligonucleotides under in vitro and in vivo conditions. One study carried out by Tang et al. (2014) describes the preparation of magnetic calcium phosphate nano-formulations that were used for transfection of DNA [78]. In the same way, any other divalent metal cations, such as Mg+2, Mn+2 and Ba+2 can form ionic complexes with the DNA (similar to Ca+2), providing stabilization to DNA structures.
Gold MNPs are very attractive as non-viral vectors due to their low chemical reactivity, stability easy preparation and gene transfection efficacy. Likewise, SPIONS have been described as gene delivery systems, especially as pulmonary gene delivery agents. Nguyen et al. (2009) described how to prepare SPIONS coated with PEG or branched with biodegradable polyesthers that maintained their transfection ability at in vivo condition after nebulization [79]. Furthermore, Dames et al. (2007) described the preparation of SPIONs used as magnetic aerosol droplets for the treatment of lung disorders such as cystic fibrosis and asthma [80]. Recent studies have combined MNP-heating properties and MNP-transfection characteristics, in order to develop both a hyperthermia and gene delivery system [81]. The development of a novel and synergic methodology of magnetofection using oscillating MNPs is a future field to be explored.
1.7.4. Clinical Trials in CF Using NPs
The UK Gene Therapy Consortium developed a cationic NP lipid formulation, namely, GL67A [85]; however, the immune-stimulatory CpG dinucleotides which caused mild flu-like symptoms have since been removed [86]. The subsequent plasmid, pGM169, encompasses a novel regulatory element, hCEFI, comprising of the elongation factor 1 α promotor coupled to the human CMV enhancer [87]. In 2015, a phase I/IIa study showed acceptable safety and efficacy using nebulised liposome-mediated gene therapy for CF patients [88]. Subsequently, a prolonged multi-dose study was undertaken, administering either 5 mL of nebulised pGM169/GL67A or 0.9% saline every month for 12 months. The 140 patients were randomly assigned to receive a placebo (n = 62) or pGM169/GL67A (n = 78) [89]. A modest, albeit significant, effect in the pGM169/GL67A group was observed at 12 months follow-up (3.7%, 95% CI 0.1–7.3; p = 0.046) which was linked to a stabilisation of lung function in the pGM169/GL67A group. However, the study did not proceed to substantive phase III studies despite reaching primary endpoints.
1.8. Future Directions
In the past decade, remarkable progress has been accomplished in the treating CF. CFTR modulation has been demonstrated to be effective in increasing the quality of life and life expectancy in a select number of patients. This review underscores the importance of the inhaled delivery of CF drugs to improve the efficacy of current systemic treatments. The main advantage of inhalation use is high drug exposure at the primary target site, while avoiding unfavourable pharmacokinetic/pharmacodynamic interactions associated with systemic use, as well as reducing the risks of potential systemic toxicity. Employing MNPs through lung delivery is a currently untapped therapeutic approach in CF modulator administration. The application of MNPs in CF still needs more experimental and clinical studies to introduce a superparamagnetism high enough to control drug delivery without the cytotoxic effects of the metal oxides. Encouraging results in the application of MNPs for CF have established the potential utility of new technologies for CFTR modulators, mucolytics or antibiotics. Proof-of-concept studies of effective MNP lung delivery will pave the way for future CFTR inhalation strategies to improve clinical outcomes in patients with CF, as well as comprehensive study of its pharmacokinetic and pharmacodynamics. Furthermore, rigorous testing of toxicity related to MNPs on the lung tissues is required. Therefore, more effort and work is still required to optimize the targeted delivery of MNPs in CF.
Author Contributions
M.T., F.R.-O. and E.K.S.-F.: data analysis, data interpretation, visualization, manuscript preparation and editorial review. All authors have read and agreed to the published version of the manuscript.
Funding
E.K.S.-F. is supported by a research grant from The University of Melbourne and the Australian National Health and Medical Research Council (NHMRC) as Biomedical Research Fellow. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Australian National Health and Medical Research Council.
Conflicts of Interest
MT, FR-O and EKS-F have nothing to disclose.
References
- Andrade, F.; Rafael, D.; Videira, M.; Ferreira, D.; Sosnik, A.; Sarmento, B. Nanotechnology and pulmonary delivery to overcome resistance in infectious diseases. Adv. Drug Deliv. Rev. 2013, 65, 1816–1827. [Google Scholar] [CrossRef] [PubMed]
- Worldwide CF. 2018. Available online: https://www.cfww.org (accessed on 23 April 2020).
- De Boeck, K.; Amaral, M.D. Progress in therapies for cystic fibrosis. Lancet Respir. Med. 2016, 4, 662–674. [Google Scholar] [CrossRef]
- Saint-Criq, V.; Gray, M.A. Role of CFTR in epithelial physiology. Cell Mol. Life Sci. 2017, 74, 93–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Döring, G.; Flume, P.; Heijerman, H.; Elborn, J.S. Treatment of lung infection in patients with cystic fibrosis: Current and future strategies. J. Cyst. Fibros. 2012, 11, 461–479. [Google Scholar] [CrossRef] [Green Version]
- Schneider-Futschik, E.K.; Paulin, O.K.A.; Hoyer, D.; Roberts, K.D.; Ziogas, J.; Baker, M.A.; Karas, J.; Li, J.; Velkov, T. Sputum Active Polymyxin Lipopeptides: Activity against Cystic Fibrosis Pseudomonas aeruginosa Isolates and Their Interactions with Sputum Biomolecules. ACS Infect. Dis. 2018, 4, 646–655. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, I.; Conte, C.; La Rotonda, M.I.; Miro, A.; Quaglia, F.; Ungaro, F. Improving the efficacy of inhaled drugs in cystic fibrosis: Challenges and emerging drug delivery strategies. Adv. Drug Deliv. Rev. 2014, 75, 92–111. [Google Scholar] [CrossRef]
- Velino, C.; Carella, F.; Adamiano, A.; Sanguinetti, M.; Vitali, A.; Catalucci, D.; Bugli, F.; Iafisco, M. Nanomedicine Approaches for the Pulmonary Treatment of Cystic Fibrosis. Front. Bioeng. Biotechnol. 2019, 7, 406. [Google Scholar] [CrossRef] [Green Version]
- Ong, V.; Mei, V.; Cao, L.; Lee, K.; Chung, E.J. Nanomedicine for Cystic Fibrosis. Slas Technol. 2019, 24, 169–180. [Google Scholar] [CrossRef]
- Schneider, E.K.; Reyes-Ortega, F.; Li, J.; Velkov, T. Can Cystic Fibrosis Patients Finally Catch a Breath with Lumacaftor/Ivacaftor? Clin. Pharmacol. Ther. 2017, 101, 130–141. [Google Scholar] [CrossRef] [Green Version]
- Davies, J.C.; Cunningham, S.; Harris, W.T.; Lapey, A.; Regelmann, W.E.; Sawicki, G.S.; Southern, K.W.; Robertson, S.; Green, Y.; Cooke, J.; et al. Safety, pharmacokinetics, and pharmacodynamics of ivacaftor in patients aged 2-5 years with cystic fibrosis and a CFTR gating mutation (KIWI): An open-label, single-arm study. Lancet Respir. Med. 2016, 4, 107–115. [Google Scholar] [CrossRef]
- Schneider-Futschik, E.K. Beyond cystic fibrosis transmembrane conductance regulator therapy: A perspective on gene therapy and small molecule treatment for cystic fibrosis. Gene 2019, 26, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, C.E.; Elborn, J.S.; Ramsey, B.W.; Marigowda, G.; Huang, X.; Cipolli, M.; Colombo, C.; Davies, J.C.; De Boeck, K.; Flume, P.A.; et al. Lumacaftor-Ivacaftor in Patients with Cystic Fibrosis Homozygous for Phe508del CFTR. N. Engl. J. Med. 2015, 373, 220–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghelani, D.P.; Schneider-Futschik, E.K. Emerging Cystic Fibrosis Transmembrane Conductance Regulator Modulators as New Drugs for Cystic Fibrosis: A Portrait of in Vitro Pharmacology and Clinical Translation. ACS Pharmacol. Transl. Sci. 2020, 3, 4–10. [Google Scholar] [CrossRef]
- Schneider, E.K.; Azad, M.A.; Han, M.L.; Tony Zhou, Q.; Wang, J.; Huang, J.X.; Cooper, M.A.; Doi, Y.; Baker, M.A.; Bergen, P.J.; et al. An "Unlikely" Pair: The Antimicrobial Synergy of Polymyxin B in Combination with the Cystic Fibrosis Transmembrane Conductance Regulator Drugs KALYDECO and ORKAMBI. ACS Infect. Dis. 2016, 2, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Hamed, K.; Conti, V.; Tian, H.; Loefroth, E. Adherence to tobramycin inhaled powder vs inhaled solution in patients with cystic fibrosis: Analysis of US insurance claims data. Patient Prefer. Adherence 2017, 11, 831–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstan, M.W.; Flume, P.A.; Kappler, M.; Chiron, R.; Higgins, M.; Brockhaus, F.; Zhang, J.; Angyalosi, G.; He, E.; Geller, D.E. Safety, efficacy and convenience of tobramycin inhalation powder in cystic fibrosis patients: The EAGER trial. J. Cyst. Fibros. 2011, 10, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Brandt, Y.I.; Armijo, L.M.; Rivera, A.C.; Plumley, J.B.; Cook, N.C.; Smolyakov, G.A.; Smyth, H.D.; Osiński, M. Effectiveness of Tobramycin Conjugated to Iron Oxide Nanoparticles in Treating Infection in Cystic Fibrosis. In Proceedings of the SPIE BiOS, San Francisco, CA, USA, 2–3 February 2013. [Google Scholar]
- Armijo, L.; Kopciuch, M.; Olszόwka, Z.; Wawrzyniec, S.; Rivera, A.; Plumley, J.; Cook, N.; Brandt, Y.; Huber, D.; Smolyakov, G.; et al. Delivery of Tobramycin Coupled to Iron Oxide Nanoparticles Across the Biofilm of Mucoidal Pseudonomas aeruginosa and Investigation of its Efficacy; SPIE: Bellingham, WA, USA, 2014; Volume 8955. [Google Scholar]
- Kirkby, S.; Novak, K.; McCoy, K. Aztreonam (for inhalation solution) for the treatment of chronic lung infections in patients with cystic fibrosis: An evidence-based review. Core Evid. 2011, 6, 59–66. [Google Scholar] [CrossRef] [Green Version]
- Koerner-Rettberg, C.; Ballmann, M. Colistimethate sodium for the treatment of chronic pulmonary infection in cystic fibrosis: An evidence-based review of its place in therapy. Core Evid. 2014, 9, 99–112. [Google Scholar] [CrossRef] [Green Version]
- Velkov, T.; Abdul Rahim, N.; Zhou, Q.T.; Chan, H.K.; Li, J. Inhaled anti-infective chemotherapy for respiratory tract infections: Successes, challenges and the road ahead. Adv. Drug Deliv. Rev. 2015, 85, 65–82. [Google Scholar] [CrossRef]
- Rogers, D.F. Mucoactive agents for airway mucus hypersecretory diseases. Respir. Care 2007, 52, 1176–1193; discussion 1193–1197. [Google Scholar]
- Elkins, M.R.; Robinson, M.; Rose, B.R.; Harbour, C.; Moriarty, C.P.; Marks, G.B.; Belousova, E.G.; Xuan, W.; Bye, P.T. A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis. N. Engl. J. Med. 2006, 354, 229–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burness, C.B.; Keating, G.M. Mannitol dry powder for inhalation: In patients with cystic fibrosis. Drugs 2012, 72, 1411–1421. [Google Scholar] [CrossRef]
- Reyes-Ortega, F.; Delgado, A.V.; Schneider, E.K.; Checa Fernandez, B.L.; Iglesias, G.R. Magnetic Nanoparticles Coated with a Thermosensitive Polymer with Hyperthermia Properties. Polymer 2017, 10, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manfredi, C.; Tindall, J.M.; Hong, J.S.; Sorscher, E.J. Making precision medicine personal for cystic fibrosis. Science 2019, 365, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Boyle, M.P.; De Boeck, K. A new era in the treatment of cystic fibrosis: Correction of the underlying CFTR defect. Lancet Respir. Med. 2013, 1, 158–163. [Google Scholar] [CrossRef]
- Brogden, R.N.; Heel, R.C. Aztreonam. A review of its antibacterial activity, pharmacokinetic properties and therapeutic use. Drugs 1986, 31, 96–130. [Google Scholar] [CrossRef]
- Allobawi, R.; Ghelani, D.P.; Schneider-Futschik, E.K. Metabolomic description of ivacaftor elevating polymyxin B mediated antibacterial activity in cystic fibrosis Pseudomonas aeruginosa. ACS Pharmacol. Transl. Sci. 2020. [Google Scholar] [CrossRef]
- Jiang, L.; Patel, D.J. Solution structure of the tobramycin-RNA aptamer complex. Nat. Struct. Biol. 1998, 5, 769–774. [Google Scholar] [CrossRef]
- LeBel, M. Ciprofloxacin: Chemistry, mechanism of action, resistance, antimicrobial spectrum, pharmacokinetics, clinical trials, and adverse reactions. Pharmacotherapy 1988, 8, 3–33. [Google Scholar] [CrossRef]
- Croom, K.F.; Goa, K.L. Levofloxacin: A review of its use in the treatment of bacterial infections in the United States. Drugs 2003, 63, 2769–2802. [Google Scholar] [CrossRef]
- Tardiolo, G.; Bramanti, P.; Mazzon, E. Overview on the Effects of N-Acetylcysteine in Neurodegenerative Diseases. Molecules 2018, 23, 3305. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.A.; Wagener, J.S. Recombinant Human Deoxyribonuclease I. In Pharmaceutical Biotechnology; Crommelin, D., Sindelar, R., Meibohm, B., Eds.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Moreno, R.; Poyser, S.; Meilak, D.; Meo, A.; Jenkins, S.; Lazarov, V.K.; Vallejo-Fernandez, G.; Majetich, S.; Evans, R.F.L. The role of faceting and elongation on the magnetic anisotropy of magnetite Fe3O4 nanocrystals. Sci. Rep. 2020, 10, 2722. [Google Scholar] [CrossRef]
- Issa, B.; Obaidat, I.M.; Albiss, B.A.; Haik, Y. Magnetic nanoparticles: Surface effects and properties related to biomedicine applications. Int. J. Mol. Sci. 2013, 14, 21266–21305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez-Sotomayor, R.; Ahualli, S.; Viota, J.L.; Rudzka, K.; Delgado, A.V. Iron/Magnetite Nanoparticles as Magnetic Delivery Systems for Antitumor Drugs. J. Nanosci. Nanotechnol. 2015, 15, 3507–3514. [Google Scholar] [CrossRef] [PubMed]
- Roca, X.; Karginov, F.V. RNA biology in a test tube—An overview of in vitro systems/assays. Wiley Interdiscip. Rev. RNA 2012, 3, 509–527. [Google Scholar] [CrossRef] [PubMed]
- McBain, S.C.; Yiu, H.H.; Dobson, J. Magnetic nanoparticles for gene and drug delivery. Int. J. Nanomed. 2008, 3, 169–180. [Google Scholar] [CrossRef] [Green Version]
- Ansari, S.; Ficiara, E.; Ruffinatti, F.A.; Stura, I.; Argenziano, M.; Abollino, O.; Cavalli, R.; Guiot, C.; D’Agata, F. Magnetic Iron Oxide Nanoparticles: Synthesis, Characterization and Functionalization for Biomedical Applications in the Central Nervous System. Material 2019, 12, 465. [Google Scholar] [CrossRef] [Green Version]
- Reyes-Ortega, F.; Checa Fernandez, B.L.; Delgado, A.V.; Iglesias, G.R. Hyperthermia-Triggered Doxorubicin Release from Polymer-Coated Magnetic Nanorods. Pharmaceutics 2019, 11, 517. [Google Scholar] [CrossRef] [Green Version]
- Nemati, Z.; Alonso, J.; Martinez, L.M.; Khurshid, H.; Garaio, E.; Garcia, J.A.; Srikanth, H. Enhanced Magnetic Hyperthermia in Iron Oxide Nano-Octopods: Size and Anisotropy Effects. J. Phys. Chem. C 2016, 120, 8370–8379. [Google Scholar] [CrossRef]
- El-Sherbiny, I.M.; Elbaz, N.M.; Sedki, M.; Elgammal, A.; Yacoub, M.H. Magnetic nanoparticles-based drug and gene delivery systems for the treatment of pulmonary diseases. Nanomedicine 2017, 12, 387–402. [Google Scholar] [CrossRef]
- Sadhukha, T.; Wiedmann, T.S.; Panyam, J. Inhalable magnetic nanoparticles for targeted hyperthermia in lung cancer therapy. Biomaterials 2013, 34, 5163–5171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristallini, C.; Barbani, N.; Ventrelli, L.; Summa, C.; Filippi, S.; Capelôa, T.; Vitale, E.; Albera, C.; Messore, B.; Giachino, C. Biodegradable microparticles designed to efficiently reach and act on cystic fibrosis mucus barrier. Mater. Sci. Eng. C 2018, 95. [Google Scholar] [CrossRef] [PubMed]
- Klinger-Strobel, M.; Lautenschlager, C.; Fischer, D.; Mainz, J.G.; Bruns, T.; Tuchscherr, L.; Pletz, M.W.; Makarewicz, O. Aspects of pulmonary drug delivery strategies for infections in cystic fibrosis—where do we stand? Expert Opin. Drug Deliv. 2015, 12, 1351–1374. [Google Scholar] [CrossRef] [PubMed]
- Leuba, K.D.; Durmus, N.G.; Taylor, E.N.; Webster, T.J. Short communication: Carboxylate functionalized superparamagnetic iron oxide nanoparticles (SPION) for the reduction of S. aureus growth post biofilm formation. Int. J. Nanomed. 2013, 8, 731–736. [Google Scholar] [CrossRef] [Green Version]
- Usmani, O.S. Choosing the right inhaler for your asthma or COPD patient. Clin. Risk Manag. 2019, 15, 461–472. [Google Scholar] [CrossRef] [Green Version]
- Konstan, M.W.; Geller, D.E.; Minic, P.; Brockhaus, F.; Zhang, J.; Angyalosi, G. Tobramycin inhalation powder for P. aeruginosa infection in cystic fibrosis: The EVOLVE trial. Pediatr. Pulmonol. 2011, 46, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Elson, E.C.; Mermis, J.; Polineni, D.; Oermann, C.M. Aztreonam Lysine Inhalation Solution in Cystic Fibrosis. Clin. Med. Insights Circ. Respir. Pulm. Med. 2019, 13. [Google Scholar] [CrossRef]
- Schuster, A.; Haliburn, C.; Doring, G.; Goldman, M.H.; Freedom Study, G. Safety, efficacy and convenience of colistimethate sodium dry powder for inhalation (Colobreathe DPI) in patients with cystic fibrosis: A randomised study. Thorax 2013, 68, 344–350. [Google Scholar] [CrossRef] [Green Version]
- Bilton, D.; Bellon, G.; Charlton, B.; Cooper, P.; De Boeck, K.; Flume, P.A.; Fox, H.G.; Gallagher, C.G.; Geller, D.E.; Haarman, E.G.; et al. Pooled analysis of two large randomised phase III inhaled mannitol studies in cystic fibrosis. J. Cyst. Fibros. 2013, 12, 367–376. [Google Scholar] [CrossRef] [Green Version]
- Aitken, M.L.; Bellon, G.; De Boeck, K.; Flume, P.A.; Fox, H.G.; Geller, D.E.; Haarman, E.G.; Hebestreit, H.U.; Lapey, A.; Schou, I.M.; et al. Long-Term Inhaled Dry Powder Mannitol in Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2012, 185, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Dorkin, H.L.; Staab, D.; Operschall, E.; Alder, J.; Criollo, M. Ciprofloxacin DPI: A randomised, placebo-controlled, phase IIb efficacy and safety study on cystic fibrosis. BMJ Open Respir. Res. 2015, 2, e000100. [Google Scholar] [CrossRef] [PubMed]
- Flume, P.A.; VanDevanter, D.R.; Morgan, E.E.; Dudley, M.N.; Loutit, J.S.; Bell, S.C.; Kerem, E.; Fischer, R.; Smyth, A.R.; Aaron, S.D.; et al. A phase 3, multi-center, multinational, randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of levofloxacin inhalation solution (APT-1026) in stable cystic fibrosis patients. J. Cyst. Fibros. 2016, 15, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Stuart Elborn, J.; Geller, D.E.; Conrad, D.; Aaron, S.D.; Smyth, A.R.; Fischer, R.; Kerem, E.; Bell, S.C.; Loutit, J.S.; Dudley, M.N.; et al. A phase 3, open-label, randomized trial to evaluate the safety and efficacy of levofloxacin inhalation solution (APT-1026) versus tobramycin inhalation solution in stable cystic fibrosis patients. J. Cyst. Fibros. 2015, 14, 507–514. [Google Scholar] [CrossRef]
- Elborn, J.S. Ciprofloxacin dry powder inhaler in cystic fibrosis. BMJ Open Respir. Res. 2016, 3, e000125. [Google Scholar] [CrossRef] [Green Version]
- Hua, X.; Tan, S.; Bandara, H.M.; Fu, Y.; Liu, S.; Smyth, H.D. Externally controlled triggered-release of drug from PLGA micro and nanoparticles. PLoS ONE 2014, 9, e114271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geller, D.E.; Flume, P.A.; Staab, D.; Fischer, R.; Loutit, J.S.; Conrad, D.J.; Mpex 204 Study, G. Levofloxacin inhalation solution (MP-376) in patients with cystic fibrosis with Pseudomonas aeruginosa. Am. J. Respir. Crit. Care Med. 2011, 183, 1510–1516. [Google Scholar] [CrossRef]
- Griesenbach, U.; Pytel, K.M.; Alton, E.W. Cystic Fibrosis Gene Therapy in the UK and Elsewhere. Hum. Gene 2015, 26, 266–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griesenbach, U.; Alton, E.W. Moving forward: Cystic fibrosis gene therapy. Hum. Mol. Genet. 2013, 22, R52–R58. [Google Scholar] [CrossRef] [Green Version]
- Griesenbach, U.; Alton, E.W. Current status and future directions of gene and cell therapy for cystic fibrosis. BioDrugs 2011, 25, 77–88. [Google Scholar] [CrossRef]
- Griesenbach, U.; Geddes, D.M.; Alton, E.W. Advances in cystic fibrosis gene therapy. Curr. Opin. Pulm. Med. 2004, 10, 542–546. [Google Scholar] [CrossRef]
- Stern, M.; Ulrich, K.; Geddes, D.M.; Alton, E.W. Poly (D, L-lactide-co-glycolide)/DNA microspheres to facilitate prolonged transgene expression in airway epithelium in vitro, ex vivo and in vivo. Gene 2003, 10, 1282–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuster, B.S.; Kim, A.J.; Kays, J.C.; Kanzawa, M.M.; Guggino, W.B.; Boyle, M.P.; Rowe, S.M.; Muzyczka, N.; Suk, J.S.; Hanes, J. Overcoming the cystic fibrosis sputum barrier to leading adeno-associated virus gene therapy vectors. Mol. Ther. 2014, 22, 1484–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, E.; Munegowda, M.A.; Cao, H.; Hu, J. Lung gene therapy-How to capture illumination from the light already present in the tunnel. Genes Dis. 2014, 1, 40–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonemitsu, Y.; Kitson, C.; Ferrari, S.; Farley, R.; Griesenbach, U.; Judd, D.; Steel, R.; Scheid, P.; Zhu, J.; Jeffery, P.K.; et al. Efficient gene transfer to airway epithelium using recombinant Sendai virus. Nat. Biotechnol. 2000, 18, 970–973. [Google Scholar] [CrossRef]
- Wilson, B.R.; Bogdan, A.R.; Miyazawa, M.; Hashimoto, K.; Tsuji, Y. Siderophores in Iron Metabolism: From Mechanism to Therapy Potential. Trends Mol. Med. 2016, 22, 1077–1090. [Google Scholar] [CrossRef] [Green Version]
- Scherer, F.; Anton, M.; Schillinger, U.; Henke, J.; Bergemann, C.; Kruger, A.; Gansbacher, B.; Plank, C. Magnetofection: Enhancing and targeting gene delivery by magnetic force in vitro and in vivo. Gene 2002, 9, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Morishita, N.; Nakagami, H.; Morishita, R.; Takeda, S.; Mishima, F.; Terazono, B.; Nishijima, S.; Kaneda, Y.; Tanaka, N. Magnetic nanoparticles with surface modification enhanced gene delivery of HVJ-E vector. Biochem. Biophys. Res. Commun. 2005, 334, 1121–1126. [Google Scholar] [CrossRef] [Green Version]
- Abdulkarim, M.; Agullo, N.; Cattoz, B.; Griffiths, P.; Bernkop-Schnurch, A.; Borros, S.G.; Gumbleton, M. Nanoparticle diffusion within intestinal mucus: Three-dimensional response analysis dissecting the impact of particle surface charge, size and heterogeneity across polyelectrolyte, pegylated and viral particles. Eur. J. Pharm. Biopharm. 2015, 97 Pt A, 230–238. [Google Scholar] [CrossRef]
- Suk, J.S.; Lai, S.K.; Boylan, N.J.; Dawson, M.R.; Boyle, M.P.; Hanes, J. Rapid transport of muco-inert nanoparticles in cystic fibrosis sputum treated with N-acetyl cysteine. Nanomedecine 2011, 6, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Craparo, E.F.; Porsio, B.; Sardo, C.; Giammona, G.; Cavallaro, G. Pegylated Polyaspartamide-Polylactide-Based Nanoparticles Penetrating Cystic Fibrosis Artificial Mucus. Biomacromolecules 2016, 17, 767–777. [Google Scholar] [CrossRef]
- Porsio, B.; Craparo, E.F.; Mauro, N.; Giammona, G.; Cavallaro, G. Mucus and Cell-Penetrating Nanoparticles Embedded in Nano-into-Micro Formulations for Pulmonary Delivery of Ivacaftor in Patients with Cystic Fibrosis. ACS Appl. Mater. Interfaces 2018, 10, 165–181. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.W.; Matthews, D.A.; Blair, G.E. Novel molecular approaches to cystic fibrosis gene therapy. Biochem. J. 2005, 387 Pt 1, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Xenariou, S.; Griesenbach, U.; Ferrari, S.; Dean, P.; Scheule, R.K.; Cheng, S.H.; Geddes, D.M.; Plank, C.; Alton, E.W. Using magnetic forces to enhance non-viral gene transfer to airway epithelium in vivo. Gene 2006, 13, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Zhou, Y.; Sun, H.; Li, D.; Zhou, S. Biodegradable magnetic calcium phosphate nanoformulation for cancer therapy. Eur. J. Pharm. Biopharm. 2014, 87, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.; Reul, R.; Betz, T.; Dayyoub, E.; Schmehl, T.; Gessler, T.; Bakowsky, U.; Seeger, W.; Kissel, T. Nanocomposites of lung surfactant and biodegradable cationic nanoparticles improve transfection efficiency to lung cells. J. Control. Release 2009, 140, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Dames, P.; Gleich, B.; Flemmer, A.; Hajek, K.; Seidl, N.; Wiekhorst, F.; Eberbeck, D.; Bittmann, I.; Bergemann, C.; Weyh, T.; et al. Targeted delivery of magnetic aerosol droplets to the lung. Nat. Nanotechnol. 2007, 2, 495–499. [Google Scholar] [CrossRef]
- Yuan, C.; An, Y.; Zhang, J.; Li, H.; Zhang, H.; Wang, L.; Zhang, D. Magnetic nanoparticles for targeted therapeutic gene delivery and magnetic-inducing heating on hepatoma. Nanotechnology 2014, 25, 345101. [Google Scholar] [CrossRef] [Green Version]
- Deacon, J.; Abdelghany, S.M.; Quinn, D.J.; Schmid, D.; Megaw, J.; Donnelly, R.F.; Jones, D.S.; Kissenpfennig, A.; Elborn, J.S.; Gilmore, B.F.; et al. Antimicrobial efficacy of tobramycin polymeric nanoparticles for Pseudomonas aeruginosa infections in cystic fibrosis: Formulation, characterisation and functionalisation with dornase alfa (DNase). J. Control. Release 2015, 198, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.Z.J.; Shan, W. Developments of Mucus Penetrating Nanoparticles. Asian J. Pharm. Sci. 2015, 10, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Jasim, R.; Schneider, E.K.; Han, M.; Azad, M.A.K.; Hussein, M.; Nowell, C.; Baker, M.A.; Wang, J.; Li, J.; Velkov, T. A Fresh Shine onCystic Fibrosis Inhalation Therapy: Antimicrobial Synergy of Polymyxin B in Combination with Silver Nanoparticles. J. Biomed. Nanotechnol. 2017, 13, 447–457. [Google Scholar] [CrossRef]
- Maclachlan, T.K.; Lukason, M.; Collins, M.; Munger, R.; Isenberger, E.; Rogers, C.; Malatos, S.; Dufresne, E.; Morris, J.; Calcedo, R.; et al. Preclinical safety evaluation of AAV2-sFLT01- a gene therapy for age-related macular degeneration. Mol. Ther. 2011, 19, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, F.E.; Clancy, J.P.; Perricone, M.A.; Bebok, Z.; Hong, J.S.; Cheng, S.H.; Meeker, D.P.; Young, K.R.; Schoumacher, R.A.; Weatherly, M.R.; et al. A clinical inflammatory syndrome attributable to aerosolized lipid-DNA administration in cystic fibrosis. Hum. Gene 2001, 12, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Hyde, S.C.; Pringle, I.A.; Abdullah, S.; Lawton, A.E.; Davies, L.A.; Varathalingam, A.; Nunez-Alonso, G.; Green, A.M.; Bazzani, R.P.; Sumner-Jones, S.G.; et al. CpG-free plasmids confer reduced inflammation and sustained pulmonary gene expression. Nat. Biotechnol. 2008, 26, 549–551. [Google Scholar] [CrossRef] [PubMed]
- Alton, E.W.; Boyd, A.C.; Porteous, D.J.; Davies, G.; Davies, J.C.; Griesenbach, U.; Higgins, T.E.; Gill, D.R.; Hyde, S.C.; Innes, J.A.; et al. A Phase I/IIa Safety and Efficacy Study of Nebulized Liposome-mediated Gene Therapy for Cystic Fibrosis Supports a Multidose Trial. Am. J. Respir. Crit. Care Med. 2015, 192, 1389–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alton, E.; Armstrong, D.K.; Ashby, D.; Bayfield, K.J.; Bilton, D.; Bloomfield, E.V.; Boyd, A.C.; Brand, J.; Buchan, R.; Calcedo, R.; et al. Repeated nebulisation of non-viral CFTR gene therapy in patients with cystic fibrosis: A randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Respir. Med. 2015, 3, 684–691. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Schematic overview of pharmacokinetics of inhaled drugs.

Figure 2.
Magnetic nanoparticle coated with a surface coating and functional groups chosen for specific uses, e.g., targeting agents, permeation enhancers or fluorophores.
Figure 2.
Magnetic nanoparticle coated with a surface coating and functional groups chosen for specific uses, e.g., targeting agents, permeation enhancers or fluorophores.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Classification of cystic fibrosis transmembrane conductance regulator (CFTR) mutations and therapeutic strategies.
Table 1.
Classification of cystic fibrosis transmembrane conductance regulator (CFTR) mutations and therapeutic strategies.
| CFTR Class | I | II | III | IV | V | VI |
|---|---|---|---|---|---|---|
| CFTR defect | Protein synthesis | Maturation processing | Ion channel gating | Ion channel conductance | Reduced protein | Reduced membrane stability |
| Type of mutations | Nonsense; frameshift; canonical splice | Missense; amino acid deletion | Missense; amino acid change | Missense; amino acid change | Splicing defect; missense | Missense; amino acid change |
| CFTR protein effect | Complete loss of protein function | Defective regulation processing | Defective protein regulation | Defective protein conductance | Reduced protein synthesis | Impacted surface retention |
| Cellular compartment where defect occurs | Ribosome | Golgi/endoplasmic reticulum | Plasma membrane CFTR | Plasma membrane CFTR | Plasma membrane, spliceosome | Plasma membrane, post-endoplasmic reticulum compartments |
| Example mutations | 3659delC; 621 + 1G→T 1078delT; 1717-1G→A; | R560T, N1303K G85E, F508del, I507del | G551S, G970R, G1244E, S1251N, G178R, S549N, S549R, G551D, S1255P, G1349D | R347P, R334W, R117H | A455E, 2789 + 5G→A, 3849 + 10KbC→T | 120del23, N287Y |
| Prevalence within CF cohort * | 22% | 88% | 6% | 6% | 5% | 0.5% |
| Patients with modulator approved genotype | <0.5% | 39.2% | 4.6% | 2.6% | 3.5% | - |
| Therapeutic strategies | Read-through synthesis | Correctors and potentiators | Potentiators | Potentiators | Amplifiers, splicing modulators, potentiators | Stabilizers |
Table 2.
Structure of CF therapies.
| Name | Mode of Action | Structure | Ref. |
|---|---|---|---|
| CFTR modulator | |||
| Ivacaftor | Potentiator |  | [14] |
| Lumacaftor | Corrector |  | [14] |
| Tezacaftor | Corrector |  | [14] |
| Elexacaftor | Corrector |  | [14] |
| Inhaled Antibiotics | |||
| Aztreonam lysine | β-lactam |  | [29] |
| Colistin | Lipopeptide |  | [30] |
| Tobramycin | Aminoglycoside |  | [31] |
| Ciprofloxacin | Fluoroquinolone |  | [32] |
| Levofloxacin | Fluoroquinolone |  | [33] |
| Mucolytics | |||
| N-acetyl cysteine (NAC) and | reduces disulphide bonds |  | [34] |
| Recombinant human deoxyribonuclease I (rhDNase) | Cleaves extracellular DNA |  | [35] |
Table 3.
Characteristics of inhalation devices commonly used for pulmonary delivery.
| Inhalation Device | ||
|---|---|---|
| Nebuliser | Dry Powder Inhaler (DPI) | |
| Mechanism | Nebulisation by air-jet | Dry powder |
| Characteristics | Vibrating mesh technology or aerosol droplets generated from liquids | High stability and sterility |
| Advantages | Little training for correct use required Ability to deliver large dosages Usage is independent on age | Short administration Small and portable Breath-actuated Little coordination required |
| Disadvantages | Requires regular maintenance Frequent administration Long inhalation times | Use in children limited Efficiency requires high inspiratory effort Optimal dosage requires proper dose preparation and loading |
Adapted from [49].
Table 4.
Inhaled therapies currently used for treatment of CF.
| Inhaled Therapy | Status | Dosage | Delivery Method | Target | Potential Side Effects | Reference |
|---|---|---|---|---|---|---|
| Mucociliary clearance | ||||||
| Mannitol | Phase III completed | 400 mg (in 10 capsules), twice daily | Dry powder | Thick viscous mucous | Cough | [53,54] |
| Hypertonic saline | - | 7% saline (active), twice daily | Nebuliser | Increase hydration of airway surface liquid | Cough | [24] |
| Anti-infective | ||||||
| Aztreonam Lysine | FDA approved | 75 mg, thrice daily | Nebuliser | P. aeruginosa colonization | Fever Cough Bronchospasm Throat and chest discomfort Nasal congestion Headache | [51] |
| Ciprofloxacin | Phase II completed | 32.5 mg twice daily | Dry powder | P. aeruginosa colonization | Sunlight sensitivity rash Cartilage toxicity Emergence of antibiotic resistance | [8,55] |
| Colistimethate sodium salt | Phase III completed | 125 mg, twice daily | Dry powder | P. aeruginosa colonization | Cough Throat irritation Chest tightness Bronchospasm | [52] |
| Levofloxacin (approved for use in Europe & Canada) | Phase III completed in USA; | 240 mg, twice daily | Nebuliser | P. aeruginosa colonization | Dysgeusia Cough Nausea Pyrexia Hemoptysis | [56,57] |
| Tobramycin (TIS) | FDA approved | 300 mg/5 mL vial, twice daily | Nebuliser | P. aeruginosa colonization | Cough Bronchospasm Dyspnoea Dysphonia Haemoptysis Transient tinnitus Voice alteration | [17,50] |
| Tobramycin (TIP) | FDA approved | 112 mg, twice daily | Dry powder | |||
Table 5.
Characteristics of magnetic nanoparticles (MNPs) for CF.
| Size | Surface Charge | Material | Composition | ||||
|---|---|---|---|---|---|---|---|
| MNP | 100–200 nm | Positive Charge e.g., Chitosan | Neutral Charge, e.g., Low Molecular Weight PEG | Lipophilic Material, e.g., PGLA | PGLA *, Chitosan | Silver | Alginate |
| Benefit | Epithelial cell uptake | Targets negatively charged mucus | Reduced electrostatic hindrance resulting in improved epithelial cell penetration PEG coating allows longer circulation | Penetration reduced by hydrophobic mucus | Biocompatible, low toxicity | Antimicrobial properties | High loading efficiency due to negative charge |
| Reference | [73] | [82] | [83] | [83] | [82] | [84] | [82] |
* PGLA = poly(lactic-co-glycolic acid); adapted from Ong et al. [9].
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tan, M.; Reyes-Ortega, F.; Schneider-Futschik, E.K. Successes and Challenges: Inhaled Treatment Approaches Using Magnetic Nanoparticles in Cystic Fibrosis. Magnetochemistry 2020, 6, 25. https://doi.org/10.3390/magnetochemistry6020025
AMA Style
Tan M, Reyes-Ortega F, Schneider-Futschik EK. Successes and Challenges: Inhaled Treatment Approaches Using Magnetic Nanoparticles in Cystic Fibrosis. Magnetochemistry. 2020; 6(2):25. https://doi.org/10.3390/magnetochemistry6020025
Chicago/Turabian StyleTan, Marsha, Felisa Reyes-Ortega, and Elena K. Schneider-Futschik. 2020. "Successes and Challenges: Inhaled Treatment Approaches Using Magnetic Nanoparticles in Cystic Fibrosis" Magnetochemistry 6, no. 2: 25. https://doi.org/10.3390/magnetochemistry6020025
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.