
Untargeted Metabolomics for the Diagnosis of Exocrine Pancreatic Insufficiency in Chronic Pancreatitis

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Diagnosis of Exocrine Pancreatic Insufficiency
2.3. Metabolite Extraction
2.4. HILIC-HRMS Analysis
2.5. Data Set Creation
2.6. Analytical Validation
2.7. Statistical Analysis
2.8. Biomarker Identification
2.9. Biomarker Evaluation
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kleeff, J.; Whitcomb, D.C. Chronic pancreatitis. Nat. Rev. Dis. Primers 2017, 3, 17060. [Google Scholar] [CrossRef] [PubMed]
- Gupte, A.; Goede, D. Chronic pancreatitis. BMJ 2018, 361, k2126. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Munoz, J.E.; Drewes, A.M. Recommendations from the United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis. Pancreatology 2018, 18, 847–854. [Google Scholar] [CrossRef]
- Duggan, S.N.; Ní Chonchubhair, H.M. Chronic pancreatitis: A diagnostic dilemma. World J. Gastroenterol. 2016, 22, 2304–2313. [Google Scholar] [CrossRef]
- Ramsey, M.L.; Conwell, D.L. Complications of Chronic Pancreatitis. Dig. Dis. Sci. 2017, 62, 1745–1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, P.A.; Conwell, D.L. Challenges and Updates in the Management of Exocrine Pancreatic Insufficiency. Pancreas 2016, 45, 1–4. [Google Scholar] [CrossRef]
- de la Iglesia-Garcia, D.; Vallejo-Senra, N. Increased Risk of Mortality Associated with Pancreatic Exocrine Insufficiency in Patients with Chronic Pancreatitis. J. Clin. Gastroenterol. 2018, 52, e63–e72. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Muñoz, J.E. Diagnosis and treatment of pancreatic exocrine insufficiency. Curr. Opin. Gastroenterol. 2018, 34, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Anaizi, A.; Hart, P.A. Diagnosing Chronic Pancreatitis. Dig. Dis. Sci. 2017, 62, 1713–1720. [Google Scholar] [CrossRef]
- González-Sánchez, V.; Amrani, R. Diagnosis of exocrine pancreatic insufficiency in chronic pancreatitis: 13C-Mixed Triglyceride Breath Test versus Fecal Elastase. Pancreatology 2017, 17, 580–585. [Google Scholar] [CrossRef]
- Vanga, R.R.; Tansel, A. Diagnostic Performance of Measurement of Fecal Elastase-1 in Detection of Exocrine Pancreatic Insufficiency: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 1220–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madji Hounoum, B.; Blasco, H. Liquid Chromatography-High-Resolution Mass Spectrometry-Based Cell Metabolomics: Experimental Design, Recommendations, and Applications. Trends Analyt. Chem. 2016, 75, 118–128. [Google Scholar] [CrossRef]
- Guo, H.; Guo, H.; Zhang, L.; Tang, Z.; Yu, X.; Wu, J.; Zeng, F. Metabolome and Transcriptome Association Analysis Reveals Dynamic Regulation of Purine Metabolism and Flavonoid Synthesis in Transdifferentiation during Somatic Embryogenesis in Cotton. Int. J. Mol. Sci. 2019, 20, E2070. [Google Scholar] [CrossRef] [Green Version]
- Zhang, A.; Sun, H. Metabolomics for Biomarker Discovery: Moving to the Clinic. BioMed Res. Int. 2015, 2015, 354671. [Google Scholar] [CrossRef] [PubMed]
- Cajka, T.; Fiehn, O. Toward Merging Untargeted and Targeted Methods in Mass Spectrometry-Based Metabolomics and Lipidomics. Anal. Chem. 2016, 88, 524–545. [Google Scholar] [CrossRef]
- Ríos Peces, S.; Díaz Navarro, C. Untargeted LC-HRMS-Based Metabolomics for Searching New Biomarkers of Pancreatic Ductal Adenocarcinoma: A Pilot Study. SLAS Discov. 2017, 22, 348–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, M.; Patel, B. Exocrine Pancreatic Insufficiency and Malnutrition in Chronic Pancreatitis: Identification, Treatment, and Consequences. Pancreas 2018, 47, 1015–1018. [Google Scholar] [CrossRef]
- de la Iglesia, D.; Vallejo-Senra, N. Pancreatic exocrine insufficiency and cardiovascular risk in patients with chronic pancreatitis: A prospective, longitudinal cohort study. J. Gastroenterol. Hepatol. 2019, 34, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Durie, P.R.; Yung-Jato, L.Y. Bentiromide test using liquid-chromatographic measurement of p-aminobenzoic acid and its metabolites for diagnosing pancreatic insufficiency in childhood. J. Pediatr. 1992, 121, 413–416. [Google Scholar] [CrossRef]
- Kay, J.G.; Fairn, G.D. Distribution, dynamics and functional roles of phosphatidylserine within the cell. Cell Commun. Signal. 2019, 17, 126. [Google Scholar] [CrossRef] [Green Version]
- Sharma, B.; Kanwar, S.S. Phosphatidylserine: A cancer cell targeting biomarker. Semin. Cancer Biol. 2018, 52, 17–25. [Google Scholar] [CrossRef]
- Köninger, J.; Balaz, P. Phosphatidylserine receptor in chronic pancreatitis: Evidence for a macrophage independent role. Ann. Surg. 2005, 241, 144–151. [Google Scholar] [CrossRef] [PubMed]
- N’Guessan, K.F.; Davis, H.W.; Chu, Z.; Vallabhapurapu, S.D.; Lewis, C.S.; Franco, R.S.; Olowokure, O.; Ahmad, S.A.; Yeh, J.J.; Bogdanov, V.Y.; et al. Enhanced Efficacy of Combination of Gemcitabine and Phosphatidylserine-Targeted Nanovesicles against Pancreatic Cancer. Mol. Ther. 2020, 28, 1876–1886. [Google Scholar] [CrossRef]
- Ridgway, N.D. The role of phosphatidylcholine and choline metabolites to cell proliferation and survival. Crit. Rev. Biochem. Mol. Biol. 2013, 48, 20–38. [Google Scholar] [CrossRef] [PubMed]
- Zeman, M.; Macášek, J.; Burda, M.; Tvrzická, E.; Vecka, M.; Krechler, T.; Staňková, B.; Hrabák, P., Jr.; Žák, A. Chronic pancreatitis and the composition of plasma phosphatidylcholine fatty acids. Prostaglandins Leukot. Essent. Fatty Acids 2016, 108, 38–44. [Google Scholar] [CrossRef]
- Osman, M.O.; Jensen, S.L. Acute pancreatitis: The pathophysiological role of cytokines and integrins. New trends for treatment? Dig. Surg. 1999, 16, 347–362. [Google Scholar] [CrossRef]
- Hegyi, P.; Rakonczay, Z., Jr.; Sári, R.; Góg, C.; Lonovics, J.; Takács, T.; Czakó, L. L-arginine-induced experimental pancreatitis. World J. Gastroenterol. 2004, 10, 2003–2009. [Google Scholar] [CrossRef] [PubMed]
- Abdelzaher, W.Y.; Ahmed, S.M.; Welson, N.N.; Marraiki, N.; Batiha, G.E.; Kamel, M.Y. Vinpocetine ameliorates L-arginine induced acute pancreatitis via Sirt1/Nrf2/TNF pathway and inhibition of oxidative stress, inflammation, and apoptosis. Biomed. Pharmacother. 2021, 133, 110976. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Jeppesen, P.B.; Gregersen, S.; Bach Larsen, L.; Hermansen, K. Chronic Exposure to Proline Causes Aminoacidotoxicity and Impaired Beta-Cell Function: Studies In Vitro. Rev. Diabet. Stud. 2016, 13, 66–78. [Google Scholar] [CrossRef] [Green Version]
- Akagawa, M.; Suyama, K. Mechanism of formation of elastin crosslinks. Connect. Tissue Res. 2000, 41, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Kesh, K.; Ganguly, N.; Jana, S.; Swarnakar, S. Matrix metalloproteinases and gastrointestinal cancers: Impacts of dietary antioxidants. World J. Biol. Chem. 2014, 5, 355–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.M.; Kim, J.H.; Choi, E.S.; Kim, E.; Choi, S.K.; Jeon, W.B. RGD-containing elastin-like polypeptide improves islet transplantation outcomes in diabetic mice. Acta Biomater. 2019, 94, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Drake, M.; Dodwad, S.J.; Davis, J.; Kao, L.S.; Cao, Y.; Ko, T.C. Sex-Related Differences of Acute and Chronic Pancreatitis in Adults. J. Clin. Med. 2021, 10, 300. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | CP Patients (%) | EPI (%) | NO-EPI (%) |
|---|---|---|---|
| Number | 53 | 32 (60.4) | 21 (39.6) |
| Age (years) | 55.7 | 56.7 | 54.3 |
| * Sex | |||
| Male | 44 (83) | 30 (93.7) | 14 (66.7) |
| Female | 9 (17) | 2 (6.3) | 7 (33.3) |
| Diagnostic test | |||
| Endoscopic ultrasonography | 38 (71.7) | 21 (65.6) | 17 (81) |
| Computed Tomography | 10 (18.9) | 6 (18.7) | 4 (19) |
| Abdominal ultrasound | 3 (5.6) | 3 (9.4) | 0 (0) |
| Anatomopathological study | 2 (3.8) | 2 (6.3) | 0 (0) |
| * Alcoholic habit | |||
| Yes | 34 (64.2) | 23 (71.9) | 11 (52.4) |
| No | 19 (35.8) | 9 (28.1) | 10 (47.6) |
| Smoking habit | |||
| Yes | 34 (64.2) | 27 (84.4) | 7 (33.3) |
| No | 19 (35.8) | 5 (15.6) | 14 (66.7) |
| Body Mass Index | |||
| Overweight/Obesity (>25) | 24 (45.3) | 10 (31.3) | 14 (66.7) |
| Normal weight (18 > BMI < 25) | 28 (52.8) | 21 (65.6) | 7 (33.3) |
| Underweight (<18) | 1 (1.9) | 1 (3.1) | 0 (0) |
| * Cardiovascular events | |||
| Yes | 4 (7.6) | 2 (6.3) | 2 (9.5) |
| No | 49 (92.4) | 30 (93.7) | 19 (90.5) |
| Abdominal pain | |||
| Yes | 24 (45.3) | 16 (50) | 8 (38.1) |
| No | 29 (54.7) | 16 (50) | 13 (61.9) |
| Diarrhea | |||
| Yes | 12 (22.6) | 10 (31.3) | 2 (9.5) |
| No | 41 (77.4) | 22 (68.7) | 19 (90.5) |
| * Diabetes | |||
| Yes | 26 (49.1) | 20 (62.5) | 6 (28.6) |
| No | 27 (50.9) | 12 (37.5) | 15 (71.4) |
| Complications 1 | |||
| Yes | 31 (58.5) | 19 (59.4) | 12 (57.1) |
| No | 22 (41.5) | 13 (40.6) | 9 (42.9) |
| Hospital readmissions 2 | |||
| Yes | 21 (39.6) | 13 (40.6) | 8 (38.1) |
| No | 32 (60.4) | 19 (59.4) | 13 (61.9) |
| Treatment | |||
| Endoscopic | 8 (15.1) | 6 (18.7) | 2 (9.5) |
| Surgical | 13 (24.5) | 10 (31.3) | 3 (14.3) |
| Analgesic | 30 (56.6) | 21 (65.6) | 9 (42.9) |
| Substitutive enzyme | 29 (54.7) | 22 (68.7) | 7 (33.3) |
| Oral antidiabetics | 26 (49.1) | 20 (62.5) | 6 (28.6) |
| Statins/Fibrates | 16 (30.2) | 11 (34.4) | 5 (23.8) |
| m/z | RT (min) | Tentative Identification | Δppm | Adduct | Fold Change |
|---|---|---|---|---|---|
| 417.2103 | 1 | Arginine-threonine-proline | 0 | +F.A.−H | 1.74 |
| 610.3721 | 1.3 | PC (16:0/5:0(OH)) | 1 | −H | 1.43 |
| 634.3334 | 2.1 | Pentasine | 1 | −H−H2O | 1.29 |
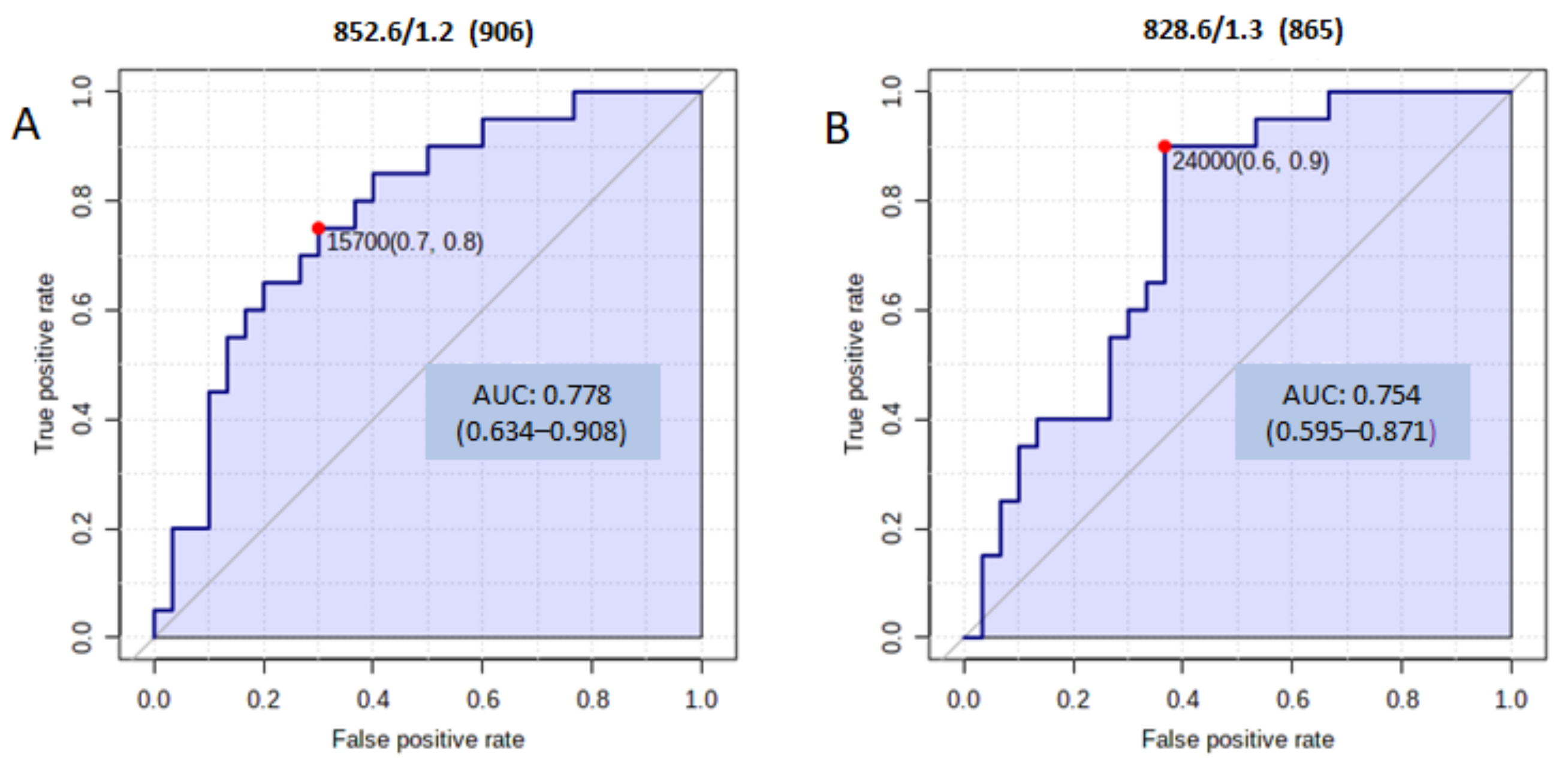
| 828.5726 | 1.3 | PS (R1COOH + R2COOH = 39:2) | 4 | −H | 1.21 |
| 852.5767 | 1.2 | PS (R1COOH + R2COOH = 41:4) | 1 | H | 1.24 |
| 876.5739 | 1.2 | PS (R1COOH + R2COOH = 43:6) | 2 | H | 1.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz, C.; Jiménez-Luna, C.; Diéguez-Castillo, C.; Martín, A.; Prados, J.; Martín-Ruíz, J.L.; Genilloud, O.; Vicente, F.; Pérez del Palacio, J.; Caba, O. Untargeted Metabolomics for the Diagnosis of Exocrine Pancreatic Insufficiency in Chronic Pancreatitis. Medicina 2021, 57, 876. https://doi.org/10.3390/medicina57090876
Díaz C, Jiménez-Luna C, Diéguez-Castillo C, Martín A, Prados J, Martín-Ruíz JL, Genilloud O, Vicente F, Pérez del Palacio J, Caba O. Untargeted Metabolomics for the Diagnosis of Exocrine Pancreatic Insufficiency in Chronic Pancreatitis. Medicina. 2021; 57(9):876. https://doi.org/10.3390/medicina57090876
Chicago/Turabian StyleDíaz, Caridad, Cristina Jiménez-Luna, Carmelo Diéguez-Castillo, Ariadna Martín, José Prados, José Luis Martín-Ruíz, Olga Genilloud, Francisca Vicente, José Pérez del Palacio, and Octavio Caba. 2021. "Untargeted Metabolomics for the Diagnosis of Exocrine Pancreatic Insufficiency in Chronic Pancreatitis" Medicina 57, no. 9: 876. https://doi.org/10.3390/medicina57090876