
Multi-Omic Admission-Based Prognostic Biomarkers Identified by Machine Learning Algorithms Predict Patient Recovery and 30-Day Survival in Trauma Patients

 , , ,
, , ,
Abstract
:
1. Introduction
2. Methods
2.1. Patient Enrollment
2.2. IRB Approval
2.3. Untargeted Metabolomic and Lipidomic Assays
2.4. Multiplexed Proteomics Assay
2.5. Data Normalization, Noise Reduction, and Scaling
2.6. Feature Selection and Regression Analysis
2.7. Gene Set Enrichment Analysis
2.8. Predictive Modeling at Admission
2.9. Cross-Prediction Validation across Two Trials
3. Results
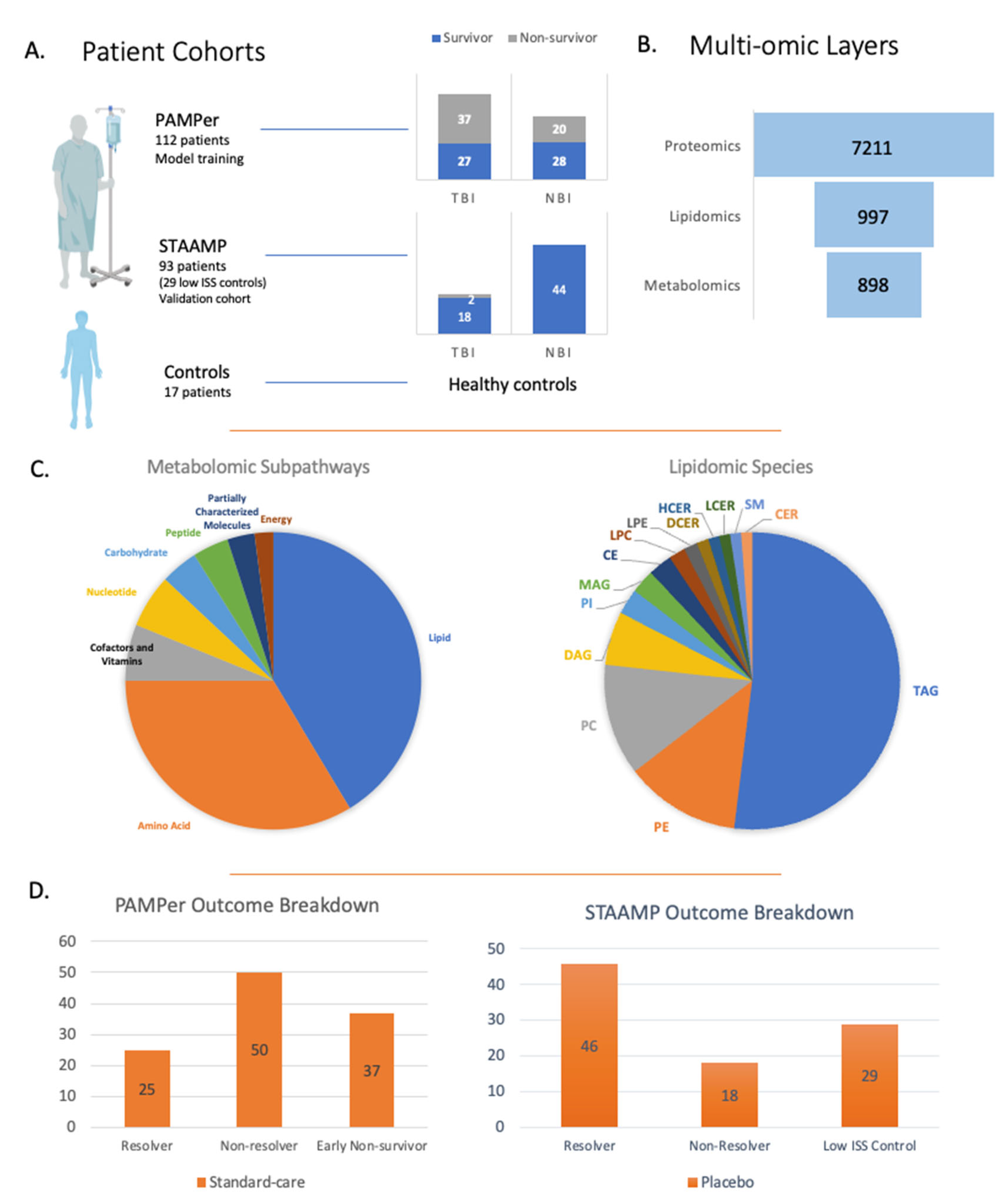
3.1. Overview of Study Design, Details, and Multi-Omic Layers
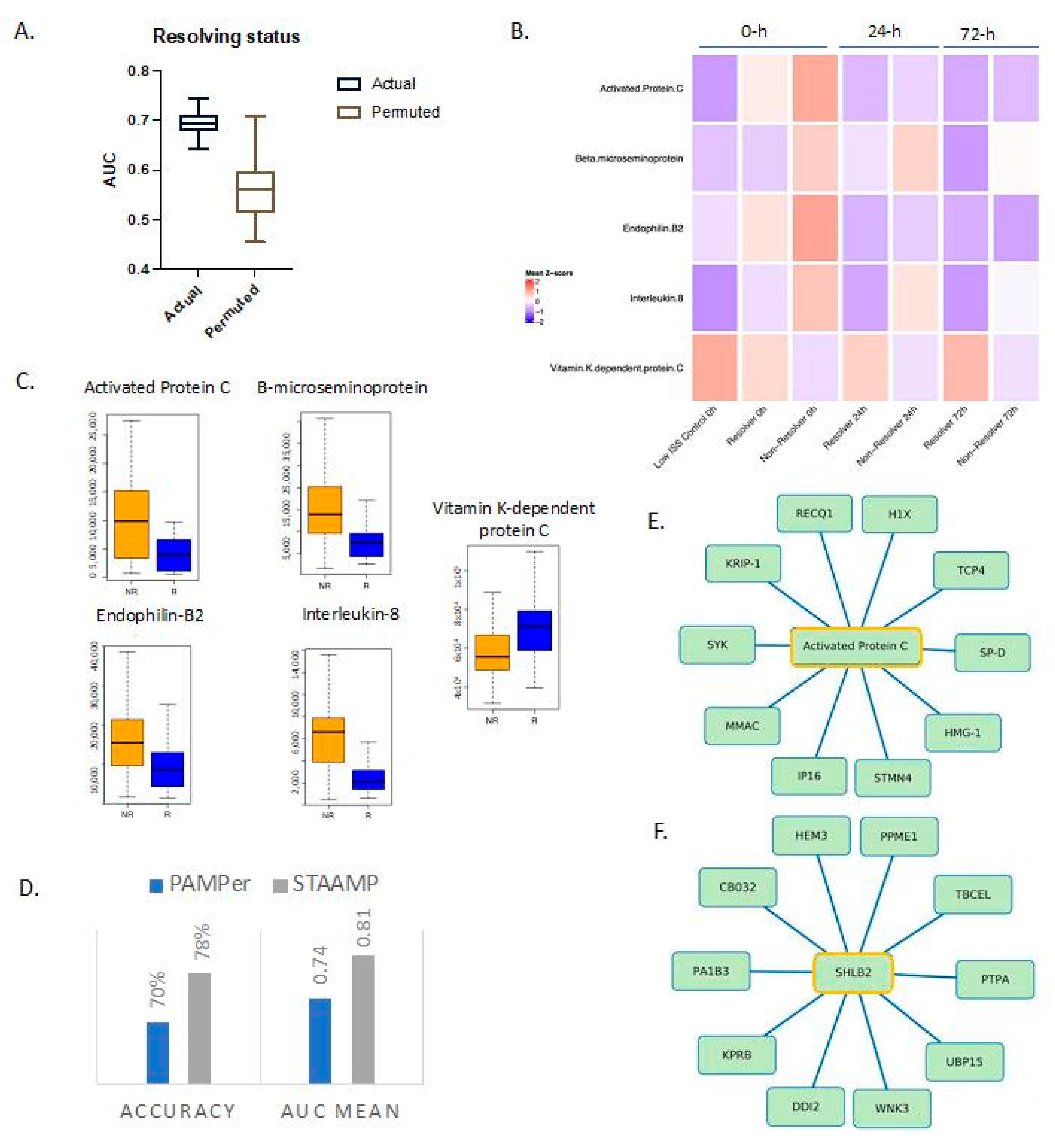
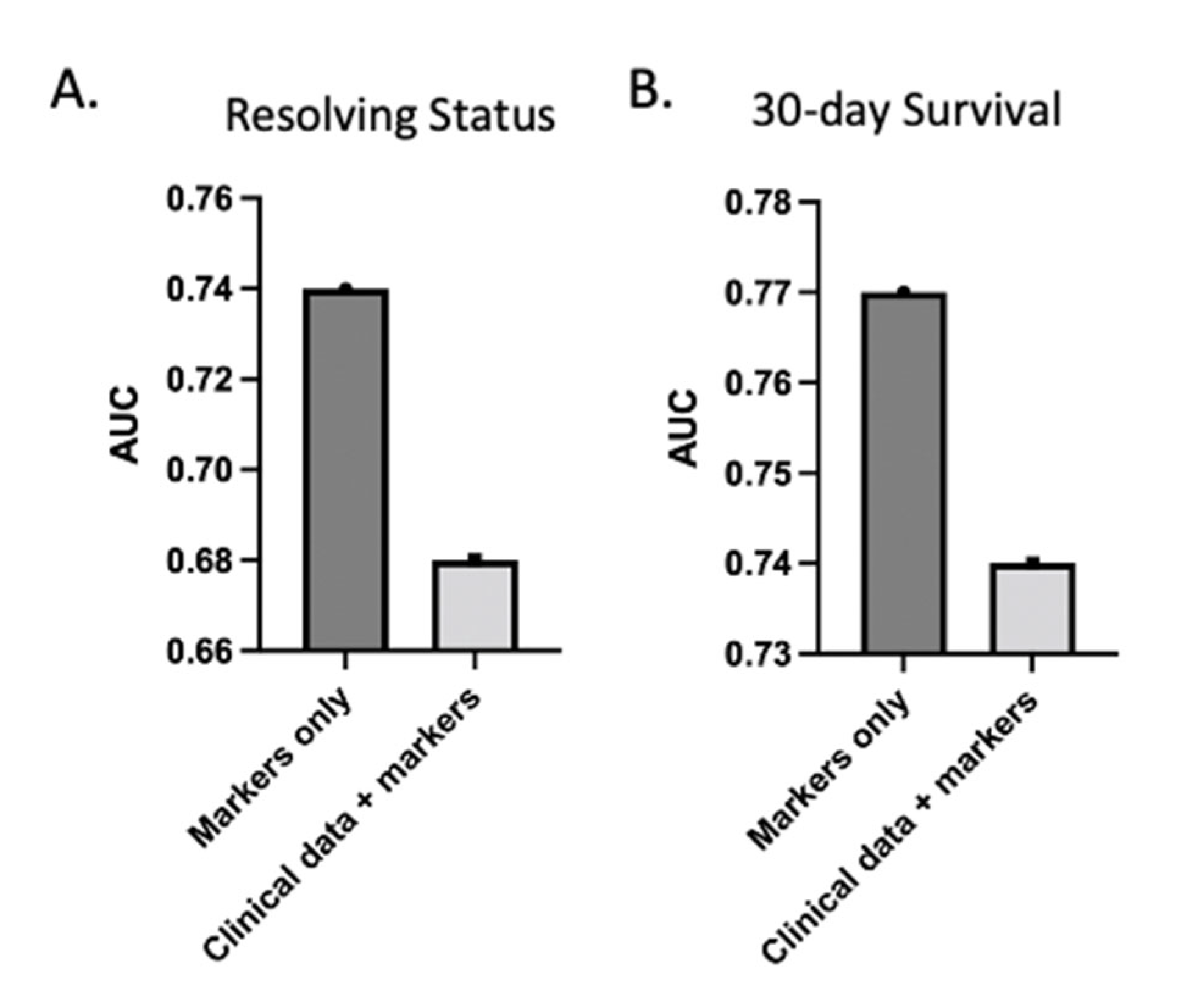
3.2. Proteomics Predicts Resolution from Critical Illness
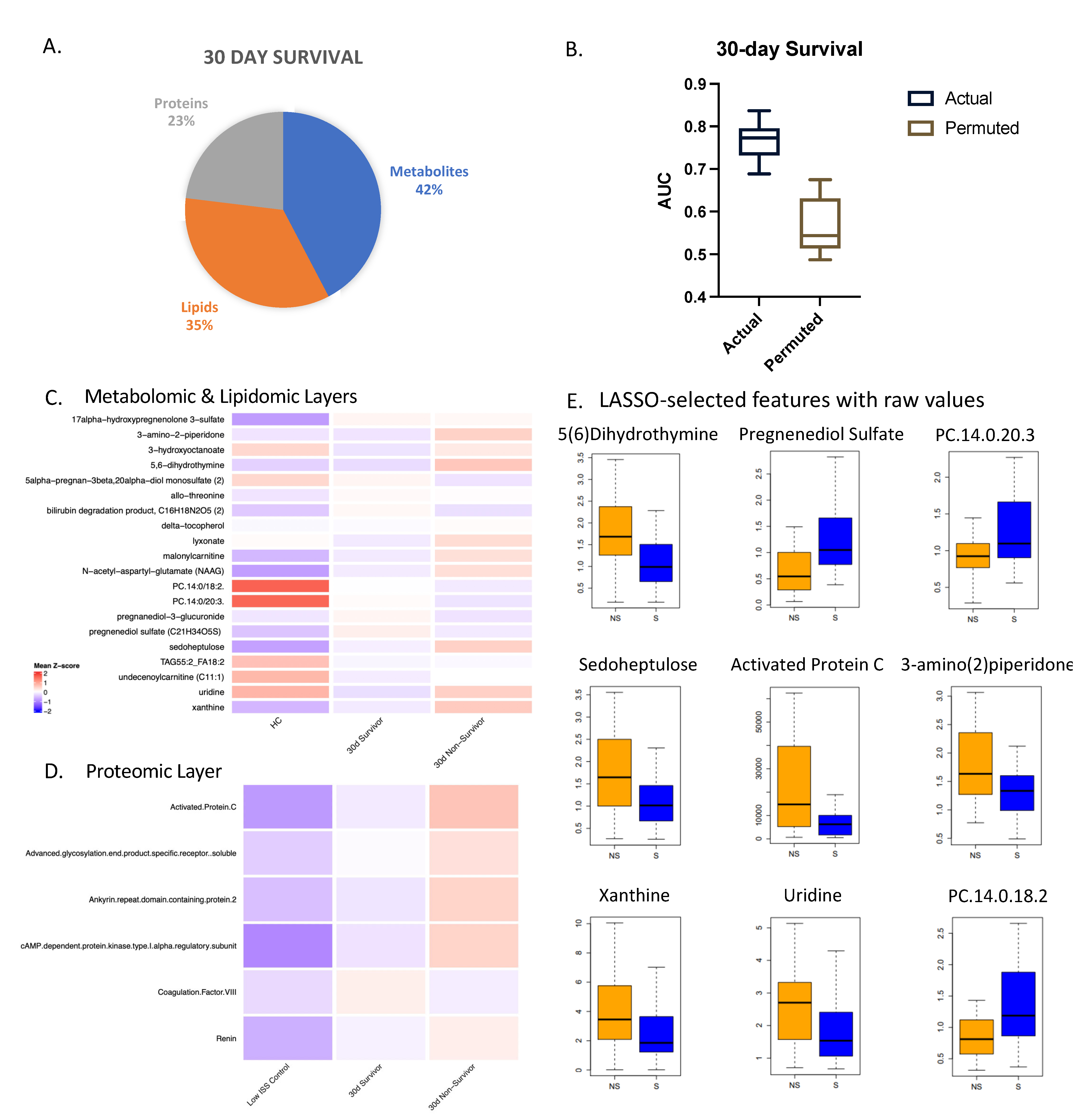
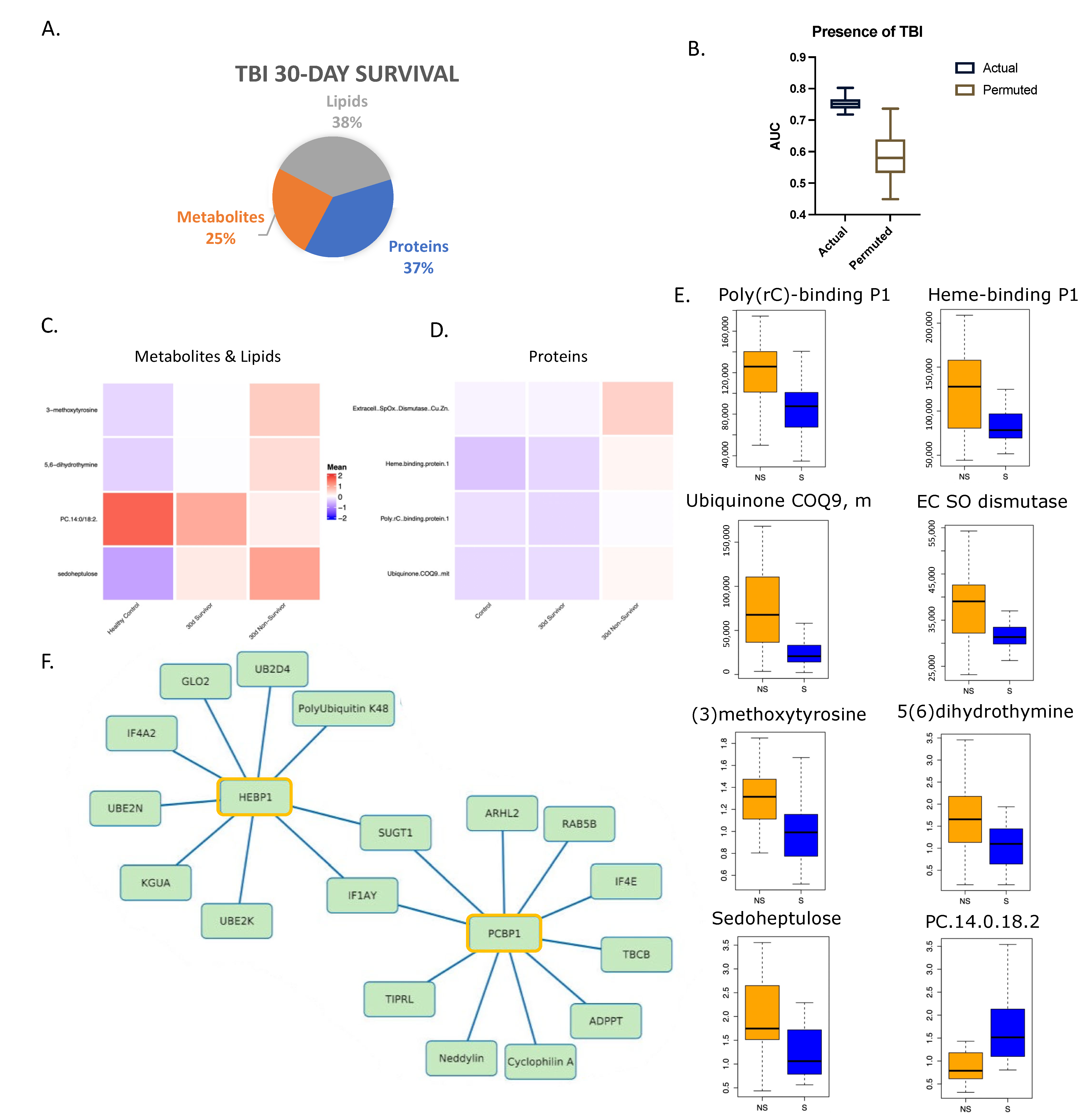
3.3. Multi-Omic Markers from Three Omic Data Layers Predict 30-Day Survival
3.4. Unique Admission Multi-Omic Markers Predict 30-Day Survival in Patients with Traumatic Brain Injury
3.5. Gene Set Enrichment Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. Underlying Cause of Death, 1999–2020 Results Form 2020. Available online: https://wonder.cdc.gov/controller/datarequest/D76;jsessionid=2F705A64B38A54BD2E3C93BE1C4F (accessed on 16 March 2022).
- Stoecklein, V.M.; Osuka, A.; Lederer, J.A. Trauma equals danger--damage control by the immune system. J. Leukoc. Biol. 2012, 92, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Asehnoune, K.; Roquilly, A.; Abraham, E.; Riou, B. Innate Immune Dysfunction in Trauma Patients: From pathophysiology to treatment. Anesthesiology 2012, 117, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Mondello, S.; Cantrell, A.; Italiano, D.; Fodale, V.; Mondello, P.; Ang, D. Complications of Trauma Patients Admitted to the ICU in Level I Academic Trauma Centers in the United States. BioMed Res. Int. 2014, 2014, 473419. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, J.; Johnson, J.L.; Sperry, J.; A West, M.; Moore, E.E.; Minei, J.P.; Bankey, P.E.; Nathens, A.B.; Cuenca, A.G.; Efron, P.A.; et al. Benchmarking Outcomes in the Critically Injured Trauma Patient and the Effect of Implementing Standard Operating Procedures. Ann. Surg. 2012, 255, 993–999. [Google Scholar] [CrossRef]
- Glance, L.G.; Osler, T.M.; Mukamel, D.B.; Dick, A.W. Outcomes of Adult Trauma Patients Admitted to Trauma Centers in Pennsylvania, 2000–2009. Arch. Surg. 2012, 147, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Chrysos, E.; Lilitsis, E.; Xenaki, S.; Athanasakis, E.; Papadakis, E.; Syrogianni, P.; Chalkiadakis, G. Guiding management in severe trauma: Reviewing factors predicting outcome in vastly injured patients. J. Emerg. Trauma Shock. 2018, 11, 80–87. [Google Scholar] [CrossRef]
- Bonaroti, J.; Li, S.; Abdelhamid, S.; Billiar, T. Prognostic Biomarkers to Predict Outcomes in Trauma. In Biomarkers in Trauma, Injury and Critical Care; Rajendram, R., Preedy, V.R., Patel, V.B., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 1–25. [Google Scholar] [CrossRef]
- Sperry, J.L.; Guyette, F.X.; Brown, J.B.; Yazer, M.H.; Triulzi, D.J.; Early-Young, B.J.; Adams, P.W.; Daley, B.J.; Miller, R.S.; Harbrecht, B.G.; et al. Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock. N. Engl. J. Med. 2018, 379, 315–326. [Google Scholar] [CrossRef]
- Wu, J.; Vodovotz, Y.; Abdelhamid, S.; Guyette, F.X.; Yaffe, M.B.; Gruen, D.S.; Cyr, A.; Okonkwo, D.O.; Kar, U.K.; Krishnamoorthi, N.; et al. Multi-omic analysis in injured humans: Patterns align with outcomes and treatment responses. Cell Rep. Med. 2021, 2, 100478. [Google Scholar] [CrossRef]
- Wu, J.; Cyr, A.; Gruen, D.; Lovelace, T.; Benos, P.; Chen, T.; Guyette, F.X.; Yazer, M.H.; Daley, B.J.; Miller, R.S.; et al. Lipidomic Signatures Align with Inflammatory Patterns and Outcomes in Critical Illness. Res. Sq. 2021. preprint. [Google Scholar] [CrossRef]
- Cyr, A.; Zhong, Y.; Reis, S.E.; Namas, R.A.; Amoscato, A.; Zuckerbraun, B.; Sperry, J.; Zamora, R.; Vodovotz, Y.; Billiar, T.R. Analysis of the Plasma Metabolome after Trauma, Novel Circulating Sphingolipid Signatures, and In-Hospital Outcomes. J. Am. Coll. Surg. 2021, 232, 276–287.e1. [Google Scholar] [CrossRef]
- Guyette, F.X.; Brown, J.B.; Zenati, M.S.; Early-Young, B.J.; Adams, P.W.; Eastridge, B.J.; Nirula, R.; Vercruysse, G.A.; O’Keeffe, T.; Joseph, B.; et al. Tranexamic Acid During Prehospital Transport in Patients at Risk for Hemorrhage After Injury: A Double-blind, Placebo-Controlled, Randomized Clinical Trial. JAMA Surg. 2020, 156, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Gruen, D.S.; Brown, J.B.; Guyette, F.X.; Vodovotz, Y.; Johansson, P.I.; Stensballe, J.; Barclay, D.A.; Yin, J.; Daley, B.J.; Miller, R.S.; et al. Prehospital plasma is associated with distinct biomarker expression following injury. JCI Insight 2020, 5, e135350. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Moheimani, H.; Li, S.; Kar, U.K.; Bonaroti, J.; Miller, R.S.; Daley, B.J.; Harbrecht, B.G.; Claridge, J.A.; Gruen, D.S.; et al. High Dimensional Multiomics Reveals Unique Characteristics of Early Plasma Administration in Polytrauma Patients with TBI. Ann. Surg. 2022. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Wu, J. Metabolomic and Proteomic Dataset of Trauma Patients in PAMPer Trial. Mendeley 2021. Available online: https://doi.org/10.17632/vt8nhp2y2t.1 (accessed on 1 June 2022).
- Ackerman, M.E.; Das, J.; Pittala, S.; Broge, T.; Linde, C.; Suscovich, T.J.; Brown, E.P.; Bradley, T.; Natarajan, H.; Lin, S.; et al. Route of immunization defines multiple mechanisms of vaccine-mediated protection against SIV. Nat. Med. 2018, 24, 1590–1598. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Devadhasan, A.; Linde, C.; Broge, T.; Sassic, J.; Mangano, M.; O′Keefe, S.; Suscovich, T.; Streeck, H.; Irrinki, A.; et al. Mining for humoral correlates of HIV control and latent reservoir size. PLoS Pathog. 2020, 16, e1008868. [Google Scholar] [CrossRef]
- Suscovich, T.J.; Fallon, J.K.; Das, J.; Demas, A.R.; Crain, J.; Linde, C.H.; Michell, A.; Natarajan, H.; Arevalo, C.; Broge, T.; et al. Mapping functional humoral correlates of protection against malaria challenge following RTS,S/AS01 vaccination. Sci. Transl. Med. 2020, 12, eabb4757. [Google Scholar] [CrossRef] [PubMed]
- Serfass, J.M.; Takahashi, Y.; Zhou, Z.; Kawasawa, Y.I.; Liu, Y.; Tsotakos, N.; Young, M.; Tang, Z.; Yang, L.; Atkinson, J.M.; et al. Endophilin B2 facilitates endosome maturation in response to growth factor stimulation, autophagy induction, and influenza A virus infection. J. Biol. Chem. 2017, 292, 10097–10111. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Wang, J.-Q.; Wang, Q.; Wang, Y.; Guo, C.; Chen, Q.; Chai, T.; Tang, T.-S. Endophilin B2 promotes inner mitochondrial membrane degradation by forming heterodimers with Endophilin B1 during mitophagy. Sci. Rep. 2016, 6, 25153. [Google Scholar] [CrossRef]
- Neyrinck, A.P.; Liu, K.D.; Howard, J.P.; Matthay, M.A. Protective mechanisms of activated protein C in severe inflammatory disorders. Br. J. Pharmacol. 2009, 158, 1034–1047. [Google Scholar] [CrossRef]
- The UniProt Consortium. UniProt: The universal protein knowledgebase in 2021. Nucleic Acids Res. 2021, 49, D480–D489. [Google Scholar] [CrossRef]
- Yang, H.; Zeng, Q.; Silverman, H.A.; Gunasekaran, M.; George, S.J.; Devarajan, A.; Addorisio, M.E.; Li, J.; Tsaava, T.; Shah, V.; et al. HMGB1 released from nociceptors mediates inflammation. Proc. Natl. Acad. Sci. USA 2021, 118, e2102034118. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.M.; Mollen, K.; Prince, J.M.; Kaczorowski, D.J.; Vallabhaneni, R.; Liu, S.; Tracey, K.J.; Lotze, M.T.; Hackam, D.J.; Fink, M.P.; et al. Systemic inflammation and remote organ injury following trauma require HMGB1. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 293, R1538–R1544. [Google Scholar] [CrossRef] [PubMed]
- Devosse, T.; Dutoit, R.; Migeotte, I.; De Nadai, P.; Imbault, V.; Communi, D.; Salmon, I.; Parmentier, M. Processing of HEBP1 by Cathepsin D Gives Rise to F2L, the Agonist of Formyl Peptide Receptor 3. J. Immunol. 2011, 187, 1475–1485. [Google Scholar] [CrossRef]
- Yagensky, O.; Kohansal-Nodehi, M.; Gunaseelan, S.; Rabe, T.; Zafar, S.; Zerr, I.; Härtig, W.; Urlaub, H.; Chua, J.J. Increased expression of heme-binding protein 1 early in Alzheimer’s disease is linked to neurotoxicity. eLife 2019, 8, e47498. [Google Scholar] [CrossRef]
- Gene Cards. HEBP1 Gene—GeneCards|HEBP1 Protein|HEBP1 Antibody 2022. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=HEBP1 (accessed on 16 April 2022).
- Safran, M.; Rosen, N.; Twik, M.; BarShir, R.; Stein, T.I.; Dahary, D.; Fishilevich, S.; Lancet, D. The GeneCards Suite. In Practical Guide to Life Science Databases; Abugessaisa, I., Kasukawa, T., Eds.; Springer: Singapore, 2021; pp. 27–56. [Google Scholar] [CrossRef]
- GSEA. HALLMARK_COAGULATION 2022. Available online: https://www.gsea-msigdb.org/gsea/msigdb/cards/HALLMARK_COAGULATION (accessed on 17 March 2022).
- GSEA. HALLMARK_INTERFERON_ALPHA_RESPONSE 2022. Available online: https://www.gsea-msigdb.org/gsea/msigdb/cards/HALLMARK_INTERFERON_ALPHA_RESPONSE (accessed on 18 March 2022).
- Gwinnutt, C.L.; Driscoll, P.A. Advanced trauma life support. Eur. J. Anaesthesiol. 1996, 13, 95–101. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guidelines for Essential Trauma Care; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Kieffer, W.K.M.; Michalik, D.V.; Gallagher, K.; McFadyen, I.; Bernard, J.; Rogers, B.A. Temporal variation in major trauma admissions. Ann. R. Coll. Surg. Engl. 2016, 98, 128–137. [Google Scholar] [CrossRef]
- Moran, C.G.; Lecky, F.; Bouamra, O.; Lawrence, T.; Edwards, A.; Woodford, M.; Willett, K.; Coats, T.J. Changing the System—Major Trauma Patients and Their Outcomes in the NHS (England) 2008–2017. eClinicalMedicine 2018, 2–3, 13–21. [Google Scholar] [CrossRef]
- Bayissa, B.B.; Alemu, S. Pattern of trauma admission and outcome among patients presented to Jimma University Specialized Hospital, south-western Ethiopia. Trauma Surg. Acute Care Open 2021, 6, e000609. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Delano, M.J.; Chen, K.; Sperry, J.L.; Namas, R.A.; Lamparello, A.J.; Deng, M.; Conroy, J.; Moldawer, L.L.; Efron, P.A.; et al. A road map from single-cell transcriptome to patient classification for the immune response to trauma. JCI Insight 2021, 6, e145108. [Google Scholar] [CrossRef]
- Raymond, S.L.; Hawkins, R.B.; Wang, Z.; Mira, J.C.; Stortz, J.A.; Han, F.; Lanz, J.D.; Hennessy, L.V.; Brumback, B.A.; Baker, H.V.; et al. Prospective Validation of a Transcriptomic Metric in Severe Trauma. Ann. Surg. 2020, 271, 802–810. [Google Scholar] [CrossRef]
- Salvo, F.; Luppi, F.; Lucchesi, D.M.; Canovi, S.; Franchini, S.; Polese, A.; Santi, F.; Trabucco, L.; Fasano, T.; Ferrari, A.M. Serum Copeptin levels in the emergency department predict major clinical outcomes in adult trauma patients. BMC Emerg. Med. 2020, 20, 14. [Google Scholar] [CrossRef]
- Paladino, L.; Sinert, R.; Wallace, D.; Anderson, T.; Yadav, K.; Zehtabchi, S. The utility of base deficit and arterial lactate in differentiating major from minor injury in trauma patients with normal vital signs. Resuscitation 2008, 77, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Régnier, M.-A.; Raux, M.; Le Manach, Y.; Asencio, Y.; Gaillard, J.; Devilliers, C.; Langeron, O.; Riou, B. Prognostic Significance of Blood Lactate and Lactate Clearance in Trauma Patients. Anesthesiology 2012, 117, 1276–1288. [Google Scholar] [CrossRef] [PubMed]
- Yakulov, T.A.; Todkar, A.P.; Slanchev, K.; Wiegel, J.; Bona, A.; Groß, M.; Scholz, A.; Hess, I.; Wurditsch, A.; Grahammer, F.; et al. CXCL12 and MYC control energy metabolism to support adaptive responses after kidney injury. Nat. Commun. 2018, 9, 3660. [Google Scholar] [CrossRef] [PubMed]
- Nagy, C.; Haschemi, A. Sedoheptulose kinase regulates cellular carbohydrate metabolism by sedoheptulose 7-phosphate supply. Biochem. Soc. Trans. 2013, 41, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.F.; Claus, C.P.; Vreman, H.J.; Wong, R.J.; Noble-Haeusslein, L.J. Heme Regulation in Traumatic Brain Injury: Relevance to the Adult and Developing Brain. J. Cereb. Blood Flow Metab. 2005, 25, 1401–1417. [Google Scholar] [CrossRef] [PubMed]
- Shinotsuka, C.; Bozza, F. Analysis of cytokine profile and heme metabolism byproducts after hemorrhagic stroke. Crit. Care 2013, 17 (Suppl. 3), P31. [Google Scholar] [CrossRef]
- Kourula, S.; Wong, R.J.; Jang, K.Y.; Kalish, F.; Chisholm, K.; Zhao, H.; Vreman, H.J.; Sylvester, K.G.; Stevenson, D.K. Heme oxygenase-1 deficiency promotes the development of necrotizing enterocolitis-like intestinal injury in a newborn mouse model. Am. J. Physiol. Gastrointest. Liver Physiol. 2013, 304, G991–G1001. [Google Scholar] [CrossRef]
- West, S.D.; Mold, C. Monocyte Deactivation Correlates with Injury Severity Score, But Not with Heme Oxygenase-1 Levels in Trauma Patients. J. Surg. Res. 2012, 172, 5–10. [Google Scholar] [CrossRef]
- Barrett, J.P.; Henry, R.; Shirey, K.A.; Doran, S.J.; Makarevich, O.D.; Ritzel, R.; Meadows, V.A.; Vogel, S.N.; Faden, A.I.; Stoica, B.A.; et al. Interferon-β Plays a Detrimental Role in Experimental Traumatic Brain Injury by Enhancing Neuroinflammation That Drives Chronic Neurodegeneration. J. Neurosci. 2020, 40, 2357–2370. [Google Scholar] [CrossRef]
- Roselli, F.; Chandrasekar, A.; Morganti-Kossmann, M.C. Interferons in Traumatic Brain and Spinal Cord Injury: Current Evidence for Translational Application. Front. Neurol. 2018, 9, 458. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PAMPer Cohort | TBI | No TBI | p-Value |
|---|---|---|---|
| N | 64 | 48 | |
| Age (Average) | 45.9 | 46.2 | |
| Gender | >0.05 | ||
| Males | 53 | 35 | |
| Females | 11 | 13 | |
| Outcome | <0.05 | ||
| Resolver | 8 | 17 | |
| Non-resolver | 34 | 16 | |
| Early non-survivor | 22 | 15 | |
| ISS | <0.05 | ||
| Mild (ISS < 15) | 4 | 13 | |
| Moderate (ISS 16–25) | 12 | 17 | |
| Severe (ISS > 25) | 48 | 18 | |
| Treatment | <0.05 | ||
| Standard of care | 49 | 35 | |
| Experimental | 38 | 27 | |
| Type of Injury | <0.05 | ||
| Blunt | 64 | 36 | |
| Penetrating | 0 | 11 | |
| Both | 0 | 1 | |
| 30-day Survival | >0.05 | ||
| Yes | 27 | 28 | |
| No | 37 | 20 | |
| Shock | 0.29 | ||
| Yes | 34 | 26 | |
| No | 30 | 22 |
| LASSO MODEL | AREA UNDER THE ROC CURVE | ACCURACY |
|---|---|---|
| 30-DAY SURVIVAL | 0.77 | 70% |
| RESOLVING STATUS | 0.74 | 70% |
| VALIDATION COHORT FOR RESOLVING STATUS | 0.81 | 78% |
| 30-DAY SURVIVAL IN TBI PATIENTS | 0.75 | 76% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelhamid, S.S.; Scioscia, J.; Vodovotz, Y.; Wu, J.; Rosengart, A.; Sung, E.; Rahman, S.; Voinchet, R.; Bonaroti, J.; Li, S.; et al. Multi-Omic Admission-Based Prognostic Biomarkers Identified by Machine Learning Algorithms Predict Patient Recovery and 30-Day Survival in Trauma Patients. Metabolites 2022, 12, 774. https://doi.org/10.3390/metabo12090774
Abdelhamid SS, Scioscia J, Vodovotz Y, Wu J, Rosengart A, Sung E, Rahman S, Voinchet R, Bonaroti J, Li S, et al. Multi-Omic Admission-Based Prognostic Biomarkers Identified by Machine Learning Algorithms Predict Patient Recovery and 30-Day Survival in Trauma Patients. Metabolites. 2022; 12(9):774. https://doi.org/10.3390/metabo12090774
Chicago/Turabian StyleAbdelhamid, Sultan S., Jacob Scioscia, Yoram Vodovotz, Junru Wu, Anna Rosengart, Eunseo Sung, Syed Rahman, Robert Voinchet, Jillian Bonaroti, Shimena Li, and et al. 2022. "Multi-Omic Admission-Based Prognostic Biomarkers Identified by Machine Learning Algorithms Predict Patient Recovery and 30-Day Survival in Trauma Patients" Metabolites 12, no. 9: 774. https://doi.org/10.3390/metabo12090774