The Oral Bacterial Microbiome of Interdental Surfaces in Adolescents According to Carious Risk

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
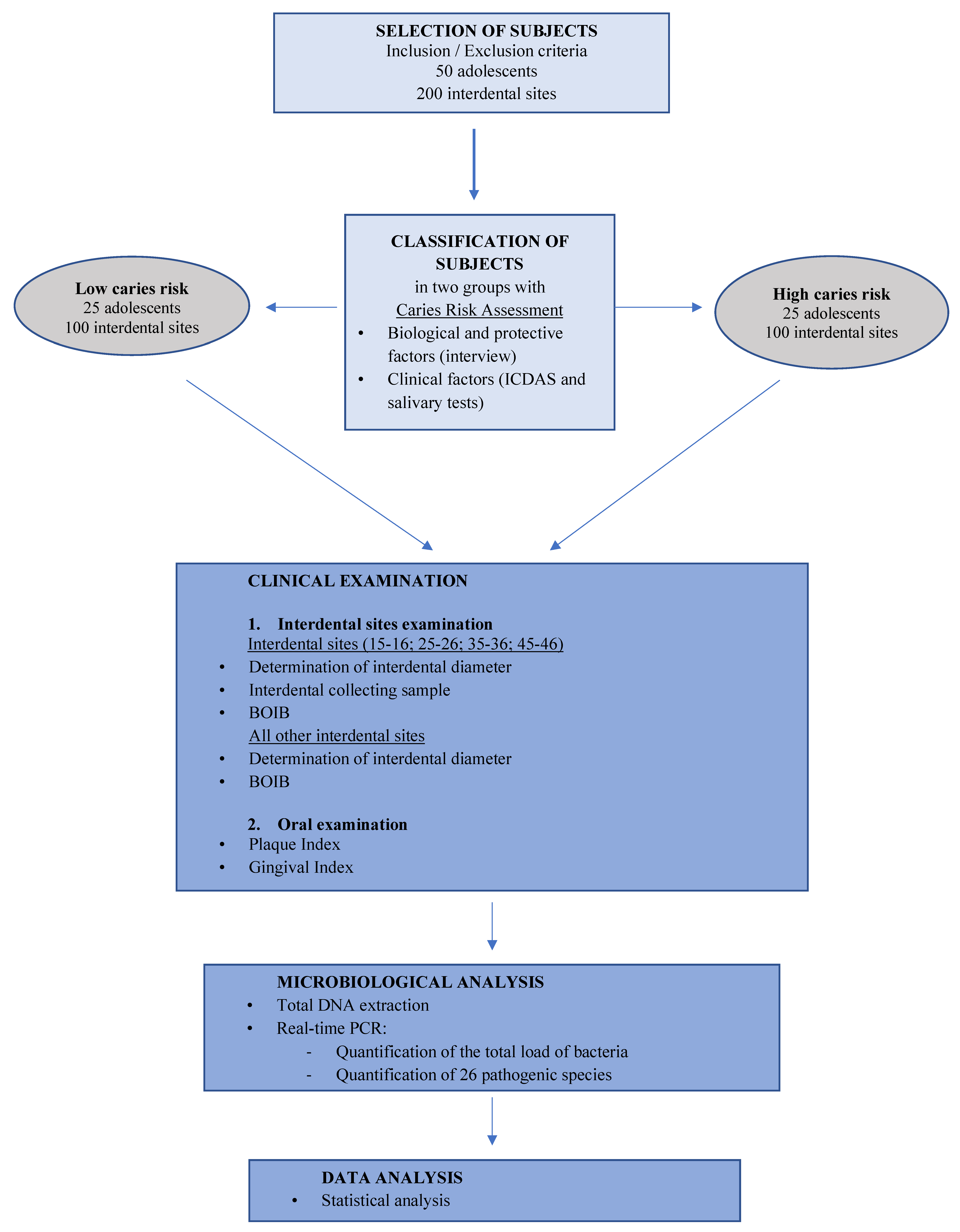
2.1. Study Population
2.2. Ethical Approval and Informed Consent
2.3. Classification of Subjects According to Carious Risk
2.4. Clinical Examination and Interdental Sample Collection
2.5. Microbiological Analysis
2.5.1. Total Deoxyribonucleic Acid (DNA) Extraction
2.5.2. Quantitative Real-Time PCR Assays
2.6. Statistical Analysis
2.6.1. Sample Size
2.6.2. Statistical Tests
3. Results
3.1. Age, Gender, and Clinical Characteristics in the Two Carious Risk Groups
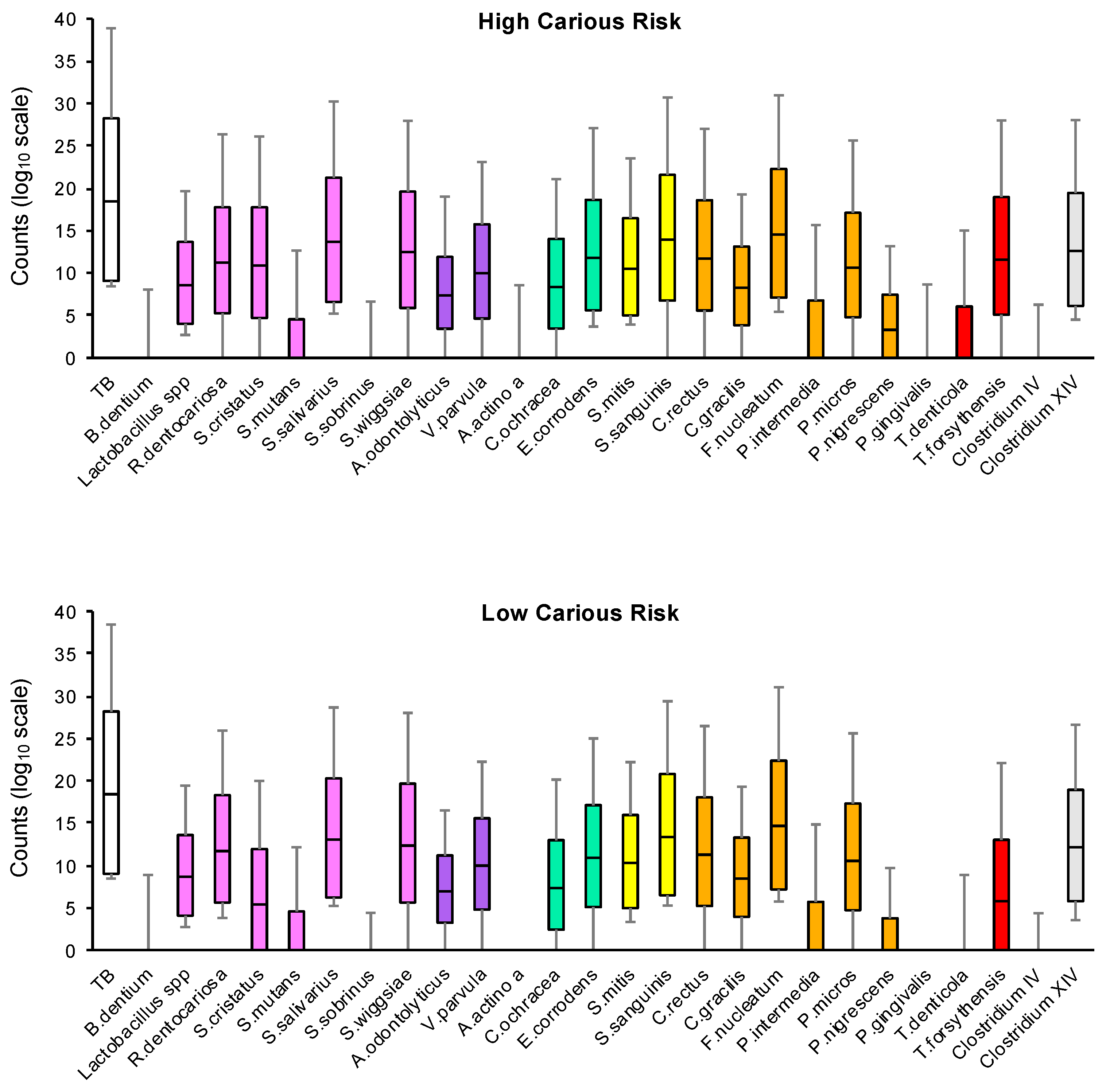
3.2. Quantification of the Total Genome Count and Bacteria Count According to Carious Risk
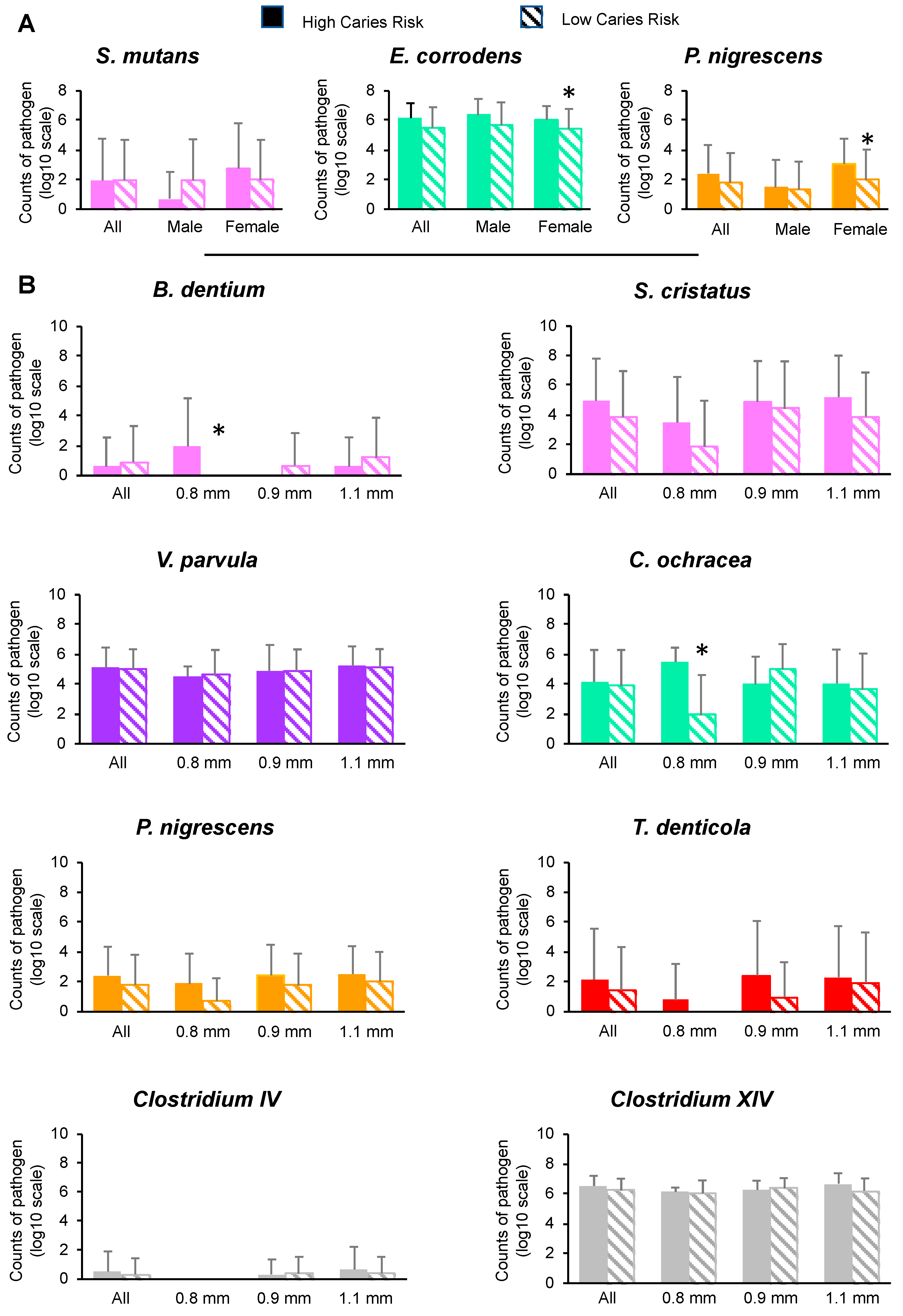
3.3. Effects of Gender, Interdental Diameter and BOIB on the Total Genome Count and Bacteria Count
3.4. Pathogen Correlations According to Carious Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Study 2017 (GBD 2017) Data Resources|GHDx. Available online: http://ghdx.healthdata.org/gbd-2017 (accessed on 14 December 2018).
- Valm, A.M. The structure of dental plaque microbial communities in the transition from health to dental caries and periodontal disease. J. Mol. Biol. 2019, 431, 2957–2969. [Google Scholar] [CrossRef]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primer 2017, 3, 17030. [Google Scholar] [CrossRef]
- Abou Neel, E.A.; Aljabo, A.; Strange, A.; Ibrahim, S.; Coathup, M.; Young, A.M.; Bozec, L.; Mudera, V. Demineralization–remineralization dynamics in teeth and bone. Int. J. Nanomed. 2016, 11, 4743–4763. [Google Scholar] [CrossRef]
- Chenicheri, S.R.U.; Ramachandran, R.; Thomas, V.; Wood, A. Insight into oral biofilm: Primary, secondary and residual caries and phyto-challenged solutions. Open Dent. J. 2017, 11. [Google Scholar] [CrossRef]
- Ribeiro, A.A.; Azcarate-Peril, M.A.; Cadenas, M.B.; Butz, N.; Paster, B.J.; Chen, T.; Bair, E.; Arnold, R.R. The oral bacterial microbiome of occlusal surfaces in children and its association with diet and caries. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Zaura, E.; Brandt, B.W.; Prodan, A.; Teixeira de Mattos, M.J.; Imangaliyev, S.; Kool, J.; Buijs, M.J.; Jagers, F.L.; Hennequin-Hoenderdos, N.L.; Slot, D.E.; et al. On the ecosystemic network of saliva in healthy young adults. ISME J. 2017, 11, 1218–1231. [Google Scholar] [CrossRef]
- Takahashi, N.; Nyvad, B. The role of bacteria in the caries process: Ecological perspectives. J. Dent. Res. 2011, 90, 294–303. [Google Scholar] [CrossRef]
- Mosaddad; Tahmasebi, E.; Yazdanian, A.; Rezvani, M.B.; Seifalian, A.; Yazdanian, M.; Tebyanian, H. Oral microbial biofilms: An update. Eur. J. Clin. Microbiol. Infect. Dis. 2019. [Google Scholar] [CrossRef]
- Carrouel, F.; Llodra, J.C.; Viennot, S.; Santamaria, J.; Bravo, M.; Bourgeois, D. Access to interdental brushing in periodontal healthy young adults: A cross-sectional Study. PLoS ONE 2016, 11, e0155467. [Google Scholar] [CrossRef]
- Ng, E.; Lim, L.P. An Overview of different interdental cleaning aids and their effectiveness. Dent. J. 2019, 7, 56. [Google Scholar] [CrossRef]
- Maheswari, S.U.; Raja, J.; Kumar, A.; Seelan, R.G. Caries management by risk assessment: A review on current strategies for caries prevention and management. J. Pharm. Bioallied Sci. 2015, 7, S320–S324. [Google Scholar]
- Worthington, H.V.; MacDonald, L.; Poklepovic Pericic, T.; Sambunjak, D.; Johnson, T.M.; Imai, P.; Clarkson, J.E. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst. Rev. 2019, 4, CD012018. [Google Scholar] [CrossRef]
- Slot, D.E.; Wiggelinkhuizen, L.; Rosema, N.A.M.; Van der Weijden, G.A. The efficacy of manual toothbrushes following a brushing exercise: A systematic review. Int. J. Dent. Hyg. 2012, 10, 187–197. [Google Scholar] [CrossRef]
- Dye, B.A.; Thornton-Evans, G.; Li, X.; Iafolla, T.J. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. NCHS Data Brief 2015, 1–8. [Google Scholar]
- Schwendicke, F.; Paris, S.; Stolpe, M. Detection and treatment of proximal caries lesions: Milieu-specific cost-effectiveness analysis. J. Dent. 2015, 43, 647–655. [Google Scholar] [CrossRef]
- Mejàre, I.; Källest l, C.; Stenlund, H. Incidence and progression of approximal caries from 11 to 22 years of age in Sweden: A prospective radiographic study. Caries Res. 1999, 33, 93–100. [Google Scholar] [CrossRef]
- Alm, A.; Wendt, L.K.; Koch, G.; Birkhed, D. Prevalence of approximal caries in posterior teeth in 15-year-old Swedish teenagers in relation to their caries experience at 3 years of age. Caries Res. 2007, 41, 392–398. [Google Scholar] [CrossRef]
- Lussi, A.; João-Souza, S.H.; Megert, B.; Carvalho, T.S.; Baumann, T. The erosive potential of different drinks, foodstuffs and medicines—a vade mecum. Swiss Dent. J. 2019, 129, 479–487. [Google Scholar]
- Nihtila, A.; West, N.; Lussi, A.; Bouchard, P.; Ottolenghi, L.; Senekola, E.; Llodra, J.C.; Viennot, S.; Bourgeois, D. Oral health behavior and lifestyle factors among overweight and non-overweight young adults in europe: A cross-sectional questionnaire study. Healthc. Basel Switz. 2016, 4, 21. [Google Scholar] [CrossRef]
- Featherstone, J.D.B.; Chaffee, B.W. The evidence for caries management by risk assessment (CAMBRA®). Adv. Dent. Res. 2018, 29, 9–14. [Google Scholar] [CrossRef]
- Kasmaei, P.; Amin Shokravi, F.; Hidarnia, A.; Hajizadeh, E.; Atrkar-Roushan, Z.; Karimzadeh Shirazi, K.; Montazeri, A. Brushing behavior among young adolescents: Does perceived severity matter. BMC Public Health 2014, 14, 8. [Google Scholar] [CrossRef]
- Erbe, C.; Klees, V.; Ferrari-Peron, P.; Ccahuana-Vasquez, R.A.; Timm, H.; Grender, J.; Cunningham, P.; Adam, R.; Farrell, S.; Wehrbein, H. A comparative assessment of plaque removal and toothbrushing compliance between a manual and an interactive power toothbrush among adolescents: A single-center, single-blind randomized controlled trial. BMC Oral Health 2018, 18, 130. [Google Scholar] [CrossRef]
- De Silva, A.M.; Hegde, S.; Akudo Nwagbara, B.; Calache, H.; Gussy, M.G.; Nasser, M.; Morrice, H.R.; Riggs, E.; Leong, P.M.; Meyenn, L.K.; et al. Community-based population-level interventions for promoting child oral health. Cochrane Database Syst. Rev. 2016, 9, CD009837. [Google Scholar] [Green Version]
- Huang, Y.K.; Lee, W.F.; Wang, M.J.; Chang, Y.H.S.; Tchaou, W.S.; Chang, W.J.; Lee, S.Y.; Sheu, J.R.; Teng, N.C. Chair-side quantitative oral-microflora screening for assessing familial correlation of periodontal status and caries prevalence. PLoS ONE 2014, 9, e87100. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentisty. Guideline on Caries-Risk Assessment and Management for Infants, Children, and Adolescents. 2010. Available online: http://www.aapd.org/media/Policies_Guidelines/G_CariesRiskAssessment.pdf (accessed on 15 March 2013).
- Clinical Affairs Committee, American Academy of Pediatric Dentistry Guideline on Adolescent Oral Health Care. Pediatr. Dent. 2015, 37, 49–56.
- Pitts, N.B.; Ekstrand, K.R. ICDAS Foundation International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef]
- Rosenauer, T.; Wagenschwanz, C.; Kuhn, M.; Kensche, A.; Stiehl, S.; Hannig, C. The bleeding on brushing index: A novel index in preventive dentistry. Int. Dent. J. 2017, 67, 299–307. [Google Scholar] [CrossRef]
- Löe, H. The gingival index, the plaque index and the retention index systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Kralik, P.; Ricchi, M. A basic guide to real time PCR in microbial diagnostics: Definitions, parameters, and everything. Front. Microbiol. 2017, 8, 108. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Paolantonio, M.; Festa, F.; di Placido, G.; D’Attilio, M.; Catamo, G.; Piccolomini, R. Site-specific subgingival colonization by Actinobacillus actinomycetemcomitans in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 423–428. [Google Scholar] [CrossRef]
- Ristic, M.; Vlahovic Svabic, M.; Sasic, M.; Zelic, O. Clinical and microbiological effects of fixed orthodontic appliances on periodontal tissues in adolescents. Orthod. Craniofac. Res. 2007, 10, 187–195. [Google Scholar] [CrossRef]
- Pan, S.; Liu, Y.; Zhang, L.; Li, S.; Zhang, Y.; Liu, J.; Wang, C.; Xiao, S. Profiling of subgingival plaque biofilm microbiota in adolescents after completion of orthodontic therapy. PLoS ONE 2017, 12, e0171550. [Google Scholar] [CrossRef]
- Zaura, E.; Keijser, B.J.F.; Huse, S.M.; Crielaard, W. Defining the healthy “core microbiome” of oral microbial communities. BMC Microbiol. 2009, 9, 259. [Google Scholar] [CrossRef]
- Gomez, A.; Nelson, K.E. The oral microbiome of children: Development, disease, and implications beyond oral health. Microb. Ecol. 2017, 73, 492–503. [Google Scholar] [CrossRef]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.R.; Yu, W.H.; Lakshmanan, A.; Wade, W.G. The human oral microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef]
- Wade, W.G. The oral microbiome in health and disease. Pharmacol. Res. 2013, 69, 137–143. [Google Scholar] [CrossRef]
- Carrouel, F.; Viennot, S.; Santamaria, J.; Veber, P.; Bourgeois, D. Quantitative molecular detection of 19 major pathogens in the interdental biofilm of periodontally healthy young adults. Front. Microbiol. 2016, 7. [Google Scholar] [CrossRef]
- Iwano, Y.; Sugano, N.; Matsumoto, K.; Nishihara, R.; Iizuka, T.; Yoshinuma, N.I.K. Salivary microbial levels in relation to periodontal status and caries development. J. Periodontal Res. 2010, 45, 165–169. [Google Scholar] [CrossRef]
- Sewón, L.A.; Parvinen, T.H.; Sinisalo, T.V.; Larmas, M.A.; Alanen, P.J. Dental status of adults with and without periodontitis. J. Periodontol. 1988, 59, 595–598. [Google Scholar] [CrossRef]
- Sioson, P.B.; Furgang, D.; Steinberg, L.M.; Fine, D.H. Proximal caries in juvenile periodontitis patients. J. Periodontol. 2000, 71, 710–716. [Google Scholar] [CrossRef]
- Durand, R.; Roufegarinejad, A.; Chandad, F.; Rompré, P.H.; Voyer, R.; Michalowicz, B.S.; Emami, E. Dental caries are positively associated with periodontal disease severity. Clin. Oral Investig. 2019, 1–9. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Featherstone, J.D.B.; Gansky, S.A.; Cheng, J.; Zhan, L. Caries risk assessment item importance. JDR Clin. Transl. Res. 2016, 1, 131–142. [Google Scholar] [CrossRef]
- Rindal, D.B.; Rush, W.A.; Perrin, N.A.; Maupomé, G.; Bader, J.D. Outcomes associated with dentists’ risk assessment. Community Dent. Oral Epidemiol. 2006, 34, 381–386. [Google Scholar] [CrossRef]
- The American Academy of Pediatric Dentistry. Caries-Risk Assessment and Management for Infants, Children, and Adolescents. 2014. Available online: https://www.aapd.org/media/Policies_Guidelines/BP_CariesRiskAssessment.pdf (accessed on 5 November 2018).
- Guo, L.; Shi, W. Salivary biomarkers for caries risk assessment. J. Calif. Dent. Assoc. 2013, 41, 107–109. [Google Scholar]
- Krasse, B.; Fure, S. Root surface caries: A problem for periodontally compromised patients. Periodontol. 2000 1994, 4, 139–147. [Google Scholar] [CrossRef]
- Gross, E.L.; Beall, C.J.; Kutsch, S.R.; Firestone, N.D.; Leys, E.J.; Griffen, A.L. Beyond Streptococcus mutans: Dental caries onset linked to multiple species by 16S rRNA community analysis. PLoS ONE 2012, 7, e47722. [Google Scholar] [CrossRef]
- Thenisch, N.L.; Bachmann, L.M.; Imfeld, T.; Leisebach Minder, T.; Steurer, J. Are mutans streptococci detected in preschool children a reliable predictive factor for dental caries risk? A systematic review. Caries Res. 2006, 40, 366–374. [Google Scholar] [CrossRef]
- Beighton, D. The complex oral microflora of high-risk individuals and groups and its role in the caries process. Community Dent. Oral Epidemiol. 2005, 33, 248–255. [Google Scholar] [CrossRef]
- Johansson, I.; Witkowska, E.; Kaveh, B.; Lif Holgerson, P.; Tanner, A.C.R. The microbiome in populations with a low and high prevalence of caries. J. Dent. Res. 2016, 95, 80–86. [Google Scholar] [CrossRef]
- Eriksson, L.; Lif Holgerson, P.; Esberg, A.; Johansson, I. Microbial Complexes and Caries in 17-Year-Olds with and without Streptococcus mutans. J. Dent. Res. 2018, 97, 275–282. [Google Scholar] [CrossRef]
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of dental caries in primary and permanent teeth in children and young adults. J. Clin. Microbiol. 2008, 46, 1407–1417. [Google Scholar] [CrossRef]
- Gross, E.L.; Leys, E.J.; Gasparovich, S.R.; Firestone, N.D.; Schwartzbaum, J.A.; Janies, D.A.; Asnani, K.; Griffen, A.L. Bacterial 16S sequence analysis of severe caries in young permanent teeth. J. Clin. Microbiol. 2010, 48, 4121–4128. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Mathney, J.M.J.; Kent, R.L.; Chalmers, N.I.; Hughes, C.V.; Loo, C.Y.; Pradhan, N.; Kanasi, E.; Hwang, J.; Dahlan, M.A.; et al. Cultivable anaerobic microbiota of severe early childhood caries. J. Clin. Microbiol. 2011, 49, 1464–1474. [Google Scholar] [CrossRef]
- Conrads, G.; de Soet, J.J.; Song, L.; Henne, K.; Sztajer, H.; Wagner-Döbler, I.; Zeng, A.P. Comparing the cariogenic species Streptococcus sobrinus and S. mutans on whole genome level. J. Oral Microbiol. 2014, 6, 26189. [Google Scholar] [CrossRef]
- Drucker, D.B.; Shakespeare, A.P.; Green, R.M. The production of dental plaque and caries by the bacterium Streptococcus salivarius in gnotobiotic WAG/RIJ rats. Arch. Oral Biol. 1984, 29, 437–443. [Google Scholar] [CrossRef]
- Burton, J.P.; Drummond, B.K.; Chilcott, C.N.; Tagg, J.R.; Thomson, W.M.; Hale, J.D.F.; Wescombe, P.A. Influence of the probiotic Streptococcus salivarius strain M18 on indices of dental health in children: A randomized double-blind, placebo-controlled trial. J. Med. Microbiol. 2013, 62, 875–884. [Google Scholar] [CrossRef]
- Kressirer, C.A.; Smith, D.J.; King, W.F.; Dobeck, J.M.; Starr, J.R.; Tanner, A.C.R. Scardovia wiggsiae and its potential role as a caries pathogen. J. Oral Biosci. 2017, 59, 135–141. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Sonis, A.L.; Lif Holgerson, P.; Starr, J.R.; Nunez, Y.; Kressirer, C.A.; Paster, B.J.; Johansson, I. White-spot lesions and gingivitis microbiotas in orthodontic patients. J. Dent. Res. 2012, 91, 853–858. [Google Scholar] [CrossRef]
- Dzidic, M.; Collado, M.C.; Abrahamsson, T.; Artacho, A.; Stensson, M.; Jenmalm, M.C.; Mira, A. Oral microbiome development during childhood: An ecological succession influenced by postnatal factors and associated with tooth decay. ISME J. 2018, 12, 2292–2306. [Google Scholar] [CrossRef]
- Ho, M.H.; Lamont, R.J.; Xie, H. Identification of streptococcus cristatus peptides that repress expression of virulence genes in porphyromonas gingivalis. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Teanpaisan, R.; Thitasomakul, S.; Piwat, S.; Thearmontree, A.; Pithpornchaiyakul, W.; Chankanka, O. Longitudinal study of the presence of mutans streptococci and lactobacilli in relation to dental caries development in 3–24 month old Thai children. Int. Dent. J. 2007, 57, 445–451. [Google Scholar] [CrossRef]
- Piwat, S.; Teanpaisan, R.; Thitasomakul, S.; Thearmontree, A.; Dahlén, G. Lactobacillus species and genotypes associated with dental caries in Thai preschool children. Mol. Oral Microbiol. 2010, 25, 157–164. [Google Scholar] [CrossRef]
- Hamada, S.; Slade, H.D. Biology, immunology, and cariogenicity of streptococcus mutans. Microbiol. Rev. 1980, 44, 331–384. [Google Scholar]
- Corby, P.M.; Lyons-Weiler, J.; Bretz, W.A.; Hart, T.C.; Aas, J.A.; Boumenna, T.; Goss, J.; Corby, A.L.; Junior, H.M.; Weyant, R.J.; et al. Microbial risk indicators of early childhood caries. J. Clin. Microbiol. 2005, 43, 5753–5759. [Google Scholar] [CrossRef]
- Caufield, P.W.; Schön, C.N.; Saraithong, P.; Li, Y.; Argimón, S. Oral lactobacilli and dental caries: A model for niche adaptation in humans. J. Dent. Res. 2015, 94, 110S–118S. [Google Scholar] [CrossRef]
- Modesto, M.; Biavati, B.; Mattarelli, P. Occurrence of the family bifidobacteriaceae in human dental caries and plaque. Caries Res. 2006, 40, 271–276. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Kent, R.L.; Holgerson, P.L.; Hughes, C.V.; Loo, C.Y.; Kanasi, E.; Chalmers, N.I.; Johansson, I. Microbiota of severe early childhood caries before and after therapy. J. Dent. Res. 2011, 90, 1298–1305. [Google Scholar] [CrossRef]
- Nair, S.; Kumar, V.S.; Krishnan, R.; Rajan, P. A comparative evaluation of bifidobacteria levels in early childhood caries and severe early childhood caries. J. Pharm. Bioallied Sci. 2017, 9, S82–S84. [Google Scholar] [CrossRef]
- Manome, A.; Abiko, Y.; Kawashima, J.; Washio, J.; Fukumoto, S.; Takahashi, N. Acidogenic potential of oral bifidobacterium and its high fluoride tolerance. Front. Microbiol. 2019, 10, 1099. [Google Scholar] [CrossRef]
- Jiang, S.; Gao, X.; Jin, L.; Lo, E.C.M. Salivary microbiome diversity in caries-free and caries-affected children. Int. J. Mol. Sci. 2016, 17, 1978. [Google Scholar] [CrossRef]
- Ferrazzano, G.F.; Scioscia, E.; Sateriale, D.; Pastore, G.; Colicchio, R.; Pagliuca, C.; Cantile, T.; Alcidi, B.; Coda, M.; Ingenito, A.; et al. In vitro antibacterial activity of pomegranate juice and peel extracts on cariogenic bacteria. BioMed Res. Int. 2017, 2017, 2152749. [Google Scholar] [CrossRef]
- Hajishengallis, E.; Parsaei, Y.; Klein, M.I.; Koo, H. Advances in the microbial etiology and pathogenesis of early childhood caries. Mol. Oral Microbiol. 2017, 32, 24–34. [Google Scholar] [CrossRef]
- Xu, H.; Tian, J.; Hao, W.; Zhang, Q.; Zhou, Q.; Shi, W.; Qin, M.; He, X.; Chen, F. Oral microbiome shifts from caries-free to caries-affected status in 3-year-old chinese children: A longitudinal study. Front. Microbiol. 2018, 9, 2009. [Google Scholar] [CrossRef]
- Hajishengallis, G. Immunomicrobial pathogenesis of periodontitis: Keystones, pathobionts, and host response. Trends Immunol. 2014, 35, 3–11. [Google Scholar] [CrossRef]
- Tu, Y.; Ling, X.; Chen, Y.; Wang, Y.; Zhou, N.; Chen, H. Effect of S. Mutans and S. Sanguinis on growth and adhesion of P. Gingivalis and their ability to adhere to different dental materials. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 4539–5445. [Google Scholar] [CrossRef]
- Hua, X.; Guy, S.; Cook, J.; William, C.; Greg, B.; Timothy, M.; Richard, J.; Lamont, R.J. Intergeneric communication in dental plaque biofilms. J. Bacteriol. 2000, 128, 7067–7069. [Google Scholar]
- Zhu, Y.; Dashper, S.G.; Chen, Y.Y.; Crawford, S.; Slakeski, N.; Reynolds, E.C. Porphyromonas gingivalis and Treponema denticola synergistic polymicrobial biofilm development. PLoS ONE 2013, 8, e71727. [Google Scholar] [CrossRef]
- Cogoni, V.; Morgan-Smith, A.; Fenno, J.C.; Jenkinson, H.F.; Dymock, D. Treponema denticola chymotrypsin-like proteinase (CTLP) integrates spirochaetes within oral microbial communities. Microbiol. Read. Engl. 2012, 158, 759–770. [Google Scholar] [CrossRef] [Green Version]
- Peterson, S.N.; Snesrud, E.; Liu, J.; Ong, A.C.; Kilian, M.; Schork, N.J.; Bretz, W. The dental plaque microbiome in health and disease. PLoS ONE 2013, 8, e58487. [Google Scholar] [CrossRef]
- Sharma, A.; Inagaki, S.; Sigurdson, W.; Kuramitsu, H.K. Synergy between Tannerella forsythia and Fusobacterium nucleatum in biofilm formation. Oral Microbiol. Immunol. 2005, 20, 39–42. [Google Scholar] [CrossRef]
- Nath, S.G.; Raveendran, R. Microbial dysbiosis in periodontitis. J. Indian Soc. Periodontol. 2013, 17, 543–545. [Google Scholar] [CrossRef]
- Kanasi, E.; Johansson, I.; Lu, S.C.; Kressin, N.R.; Nunn, M.E.; Kent, R.; Tanner, A.C.R. Microbial risk markers for childhood caries in pediatricians’ offices. J. Dent. Res. 2010, 89, 378–383. [Google Scholar] [CrossRef]
- Nakagawa, S.; Fujii, H.; Machida, Y.; Okuda, K. A longitudinal study from prepuberty to puberty of gingivitis. Correlation between the occurrence of Prevotella intermedia and sex hormones. J. Clin. Periodontol. 1994, 21, 658–665. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, J.K.; Cho, J.Y.; Lee, J.M.; Hong, S.H. Quantification of subgingival bacterial pathogens at different stages of periodontal diseases. Curr. Microbiol. 2012, 65, 22–27. [Google Scholar] [CrossRef]
- Becker, M.R.; Paster, B.J.; Leys, E.J.; Moeschberger, M.L.; Kenyon, S.G.; Galvin, J.L.; Boches, S.K.; Dewhirst, F.E.; Griffen, A.L. Molecular analysis of bacterial species associated with childhood caries. J. Clin. Microbiol. 2002, 40, 1001–1009. [Google Scholar] [CrossRef]
- Belda-Ferre, P.; Alcaraz, L.D.; Cabrera-Rubio, R.; Romero, H.; Simón-Soro, A.; Pignatelli, M.; Mira, A. The oral metagenome in health and disease. ISME J. 2012, 6, 46–56. [Google Scholar] [CrossRef]
- Bik, E.M.; Long, C.D.; Armitage, G.C.; Loomer, P.; Emerson, J.; Mongodin, E.F.; Nelson, K.E.; Gill, S.R.; Fraser-Liggett, C.M.; Relman, D.A. Bacterial diversity in the oral cavity of 10 healthy individuals. ISME J. 2010, 4, 962–974. [Google Scholar] [CrossRef]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the normal bacterial flora of the oral cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef]
- Abusleme, L.; Dupuy, A.K.; Dutzan, N.; Silva, N.; Burleson, J.A.; Strausbaugh, L.D.; Gamonal, J.; Diaz, P.I. The subgingival microbiome in health and periodontitis and its relationship with community biomass and inflammation. ISME J. 2013, 7, 1016–1025. [Google Scholar] [CrossRef] [Green Version]
- Ge, Y.; Caufield, P.W.; Fisch, G.S.; Li, Y. Streptococcus mutans and Streptococcus sanguinis colonization correlated with caries experience in children. Caries Res. 2008, 42, 444–448. [Google Scholar] [CrossRef]
- Choi, H.; Kim, E.; Kang, J.; Kim, H.J.; Lee, J.Y.; Choi, J.; Joo, J.Y. Real-time PCR quantification of 9 periodontal pathogens in saliva samples from periodontally healthy Korean young adults. J. Periodontal Implant Sci. 2018, 48, 261–271. [Google Scholar] [CrossRef]
- Suda, R.; Lai, C.H.; Yang, H.W.; Hasegawa, K. Eikenella corrodens in subgingival plaque: Relationship to age and periodontal condition. J. Periodontol. 2002, 73, 886–891. [Google Scholar] [CrossRef]
- Noiri, Y.; Li, L.; Ebisu, S. The localization of periodontal-disease-associated bacteria in human periodontal pockets. J. Dent. Res. 2001, 80, 1930–1934. [Google Scholar] [CrossRef]
- Dye, B.A.; Tan, S.; Smith, V.; Lewis, B.G.; Barker, L.K.; Thornton-Evans, G.; Eke, P.I.; Beltrán-Aguilar, E.D.; Horowitz, A.M.; Li, C.H. Trends in oral health status: United States, 1988–1994 and 1999–2004. Vital Health Stat. 11 2007, 1–92. [Google Scholar]
- Yin, W.; Yang, Y.M.; Chen, H.; Li, X.; Wang, Z.; Cheng, L.; Yin, Q.D.; Fang, H.Z.; Fei, W.; Mi, F.L.; et al. Oral health status in Sichuan Province: Findings from the oral health survey of Sichuan, 2015–2016. Int. J. Oral Sci. 2017, 9, 10–15. [Google Scholar] [CrossRef]
- Hou, R.; Mi, Y.; Xu, Q.; Wu, F.; Ma, Y.; Xue, P.; Xiao, G.; Zhang, Y.; Wei, Y.; Yang, W. Oral health survey and oral health questionnaire for high school students in Tibet, China. Head Face Med. 2014, 10, 17. [Google Scholar] [CrossRef]
- Hu, J.; Jiang, W.; Lin, X.; Zhu, H.; Zhou, N.; Chen, Y.; Wu, W.; Zhang, D.; Chen, H. Dental caries status and caries risk factors in students ages 12–14 years in Zhejiang, China. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 3670–3678. [Google Scholar] [CrossRef]
- Yetimoglu, C.; Rafeiner, P.; Engel, D.; Fournier, J.Y. Spinal infections due to Eikenella corrodens: Case report and literature review. Neurochirurgie. 2014, 60, 197–200. [Google Scholar] [CrossRef] [Green Version]
- Udaka, T.; Hiraki, N.; Shiomori, T.; Miyamoto, H.; Fujimura, T.; Inaba, T.; Suzuki, H. Eikenella corrodens in head and neck infections. J. Infect. 2007, 54, 343–348. [Google Scholar] [CrossRef]
- Angulo López, I.; Aguirre Quiñonero, A.; Fernández Torres, M.; Alegría Echauri, E. Chorioamnionitis and neonatal septicaemia due to Eikenella corrodens. Enferm. Infecc. Microbiol. Clin. 2017, 35, 266–267. [Google Scholar] [CrossRef]
- Sheng, W.S.; Hsueh, P.R.; Hung, C.C.; Teng, L.J.; Chen, Y.C.; Luh, K.T. Clinical features of patients with invasive Eikenella corrodens infections and microbiological characteristics of the causative isolates. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 231–236. [Google Scholar] [CrossRef]
- Elikowski, W.; Małek-Elikowska, M.; Lisiceka, M.; Wróblewski, D.; Fertała, N. Eikenella corrodens endocarditis of the tricuspid valve in an intravenous drug user. Pol. Merkur. Lek. Organ Pol. Tow. Lek. 2017, 42, 81–83. [Google Scholar]
- Kanasi, E.; Dewhirst, F.E.; Chalmers, N.I.; Kent, R.; Moore, A.; Hughes, C.V.; Pradhan, N.; Loo, C.Y.; Tanner, A.C.R. Clonal analysis of the microbiota of severe early childhood caries. Caries Res. 2010, 44, 485–497. [Google Scholar] [CrossRef]
- Luppens, S.B.I.; Kara, D.; Bandounas, L.; Jonker, M.J.; Wittink, F.R.A.; Bruning, O.; Breit, T.M.; Ten Cate, J.M.; Crielaard, W. Effect of veillonella parvula on the antimicrobial resistance and gene expression of Streptococcus mutans grown in a dual-species biofilm. Oral Microbiol. Immunol. 2008, 23, 183–189. [Google Scholar] [CrossRef]
- Liljemark, W.F.; Bloomquist, C.G.; Bandt, C.L.; Pihlstrom, B.L.; Hinrichs, J.E.; Wolff, L.F. Comparison of the distribution of actinomyces in dental plaque on inserted enamel and natural tooth surfaces in periodontal health and disease. Oral Microbiol. Immunol. 1993, 8, 5–15. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Milgrom, P.M.; Kent, R.; Mokeem, S.A.; Page, R.C.; Riedy, C.A.; Weinstein, P.; Bruss, J. The microbiota of young children from tooth and tongue samples. J. Dent. Res. 2002, 81, 53–57. [Google Scholar] [CrossRef]
- Marchant, S.; Brailsford, S.R.; Twomey, A.C.; Roberts, G.J.; Beighton, D. The predominant microflora of nursing caries lesions. Caries Res. 2001, 35, 397–406. [Google Scholar] [CrossRef]
- Li, Y.; Zou, C.G.; Fu, Y.; Li, Y.; Zhou, Q.; Liu, B.; Zhang, Z.; Liu, J. Oral microbial community typing of caries and pigment in primary dentition. BMC Genomics 2016, 17, 558. [Google Scholar] [CrossRef]
- Sampaio-Maia, B.; Caldas, I.M.; Pereira, M.L.; Pérez-Mongiovi, D.; Araujo, R. The Oral microbiome in health and its implication in oral and systemic diseases. Adv. Appl. Microbiol. 2016, 97, 171–210. [Google Scholar]
- Jia, G.; Zhi, A.; Lai, P.F.H.; Wang, G.; Xia, Y.; Xiong, Z.; Zhang, H.; Che, N.; Ai, L. The oral microbiota—A mechanistic role for systemic diseases. Br. Dent. J. 2018, 224, 447–455. [Google Scholar] [CrossRef]
- Weber, E.; Reynaud, Q.; Suy, F.; Gagneux-Brunon, A.; Carricajo, A.; Guillot, A.; Botelho-Nevers, E. Bifidobacterium species bacteremia: Risk factors in adults and infants. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, 482–484. [Google Scholar] [CrossRef]
- Könönen, E.; Wade, W.G. Actinomyces and related organisms in human infections. Clin. Microbiol. Rev. 2015, 28, 419–442. [Google Scholar] [CrossRef]
- Datta, S.; Soliman, M.; Laguio, M. Actinomyces in blood: Is it clinically significant or insignificant? Open Forum Infect. Dis. 2017, 4, S554. [Google Scholar] [CrossRef]
- Binder, D.; Zbinden, R.; Widmer, U.; Opravil, M.; Krause, M. Native and prosthetic valve endocarditis caused by Rothia dentocariosa: Diagnostic and therapeutic considerations. Infection 1997, 25, 22–26. [Google Scholar] [CrossRef]
- Dhotre, S.V.; Davane, M.S.; Nagoba, B.S. Periodontitis, bacteremia and infective endocarditis: A review study. Arch. Pediatr. Infect. Dis. 2017, 5, e41067. [Google Scholar] [CrossRef]
- Gondivkar, S.; Gadbail, A.; Parikh, R.V. Role of oral foci in systemic diseases: An update. Int. J. Contemp. Dent. Med. Rev. 2017, 1–8. [Google Scholar]
- Nordholm, A.C.; Vøgg, R.O.B.; Permin, H.; Katzenstein, T. Eikenella corrodens endocarditis and liver abscess in a previously healthy male, a case report. BMC Infect. Dis. 2018, 18, 35. [Google Scholar] [CrossRef]
- Beck, J.D.; Eke, P.; Heiss, G.; Madianos, P.; Couper, D.; Lin, D.; Moss, K.; Elter, J.; Offenbacher, S. Periodontal disease and coronary heart disease: A reappraisal of the exposure. Circulation 2005, 112, 19–24. [Google Scholar] [CrossRef]
- Bagavant, H.; Dunkleberger, M.L.; Wolska, N.; Sroka, M.; Rasmussen, A.; Adrianto, I.; Montgomery, C.; Sivils, K.; Guthridge, J.M.; James, J.A.; et al. Antibodies to periodontogenic bacteria are associated with higher disease activity in lupus patients. Clin. Exp. Rheumatol. 2019, 37, 106–111. [Google Scholar]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Larsen, J.M. The immune response to Prevotella bacteria in chronic inflammatory disease. Immunology 2017, 151, 363–374. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| High Risk | Low Risk | |
|---|---|---|
| Biological (interview) | ||
| Yes | |
| Yes | |
| Protective (interview) | ||
| Yes | |
| Yes | |
| Clinical Findings (ICDAS and salivary tests) ICDAS | ||
| Yes | |
| Yes | |
| Salivary tests (hydration, salivary consistency, resting saliva pH, stimulated saliva flow, stimulated saliva pH and saliva buffering capacity) | ||
| Yes |
| High Caries Risk | Low Caries Risk | p-Value | |
|---|---|---|---|
| Subjects | |||
| Age (years) | 16.08 ± 0.81 | 15.88 ± 0.73 | 0.49 |
| Gender | 0.37 | ||
| Male | 10 (40%) | 7 (28%) | |
| Female | 15 (60%) | 18 (72%) | |
| Full mouth | |||
| Teeth | 27.80 ± 0.82 | 27.48 ± 1.23 | 0.89 |
| BOIB (%) | 96.55 ± 7.87 | 96.52 ± 5.13 | 0.52 |
| PI | 1.56 ± 0.51 | 1.76 ± 0.43 | 0.22 |
| GI | 1.92 ± 0.28 | 1.72 ± 0.46 | 0.22 |
| Interdental space diameter | 0.35 | ||
| 0.8 mm | 10 (10%) | 10 (10%) | |
| 0.9 mm | 22 (22%) | 31 (31%) | |
| 1.1 mm | 68 (68%) | 59 (59%) |
| Variable | All (n = 200) | Caries Risk | ||
|---|---|---|---|---|
| High (n = 100) | Low (n = 100) | p-Value | ||
| TB | 9.42 ± 0.48 | 9.43 ± 0.47 | 9.40 ± 0.48 | 0.796 |
| B. dentium | 0.76 ± 2.20 | 0.60 ± 1.95 | 0.91 ± 2.41 | 0.522 |
| Lactobacillus spp. | 4.54 ± 0.67 | 4.57 ± 0.72 | 4.50 ± 0.60 | 0.591 |
| R. dentocariosa | 5.91 ± 1.14 | 5.73 ± 1.43 | 6.08 ± 0.70 | 0.226 |
| S. cristatus | 4.41 ± 3.02 | 4.97 ± 2.83 | 3.85 ± 3.11 | 0.096 |
| S. mutans | 1.96 ± 2.76 | 1.95 ± 2.81 | 1.97 ± 2.72 | 0.969 |
| S. salivarius | 6.90 ± 0.70 | 7.05 ± 0.70 | 6.75 ± 0.67 | 0.068 |
| S. sobrinus | 0.30 ± 1.19 | 0.56 ± 1.58 | 0.04 ± 0.43 | 0.049 |
| S. wiggsiae | 5.85 ± 2.35 | 6.09 ± 1.88 | 5.59 ± 2.72 | 0.412 |
| A. odontolyticus | 3.77 ± 1.19 | 3.97 ± 1.18 | 3.56 ± 1.18 | 0.120 |
| V. parvula | 5.05 ± 1.36 | 5.07 ± 1.38 | 5.02 ± 1.32 | 0.881 |
| A. actinomycetemcomitans | 0.28 ± 1.32 | 0.55 ± 1.83 | 0.00 ± 0.00 | 0.076 |
| C. ochracea | 4.04 ± 2.26 | 4.18 ± 2.11 | 3.89 ± 2.40 | 0.609 |
| E. corrodens | 5.84 ± 1.27 | 6.17 ± 1.01 | 5.50 ± 1.40 | 0.006 |
| S. mitis | 5.35 ± 0.62 | 5.48 ± 0.63 | 5.22 ± 0.58 | 0.075 |
| S. sanguinis | 7.00 ± 0.98 | 7.05 ± 1.22 | 6.94 ± 0.65 | 0.580 |
| C. rectus | 5.89 ± 1.79 | 6.00 ± 1.71 | 5.77 ± 1.86 | 0.560 |
| C. gracilis | 4.22 ± 1.14 | 4.31 ± 0.89 | 4.12 ± 1.34 | 0.524 |
| F. nucleatum | 7.42 ± 0.54 | 7.40 ± 0.56 | 7.43 ± 0.50 | 0.801 |
| P. intermedia | 2.85 ± 3.43 | 3.31 ± 3.53 | 2.38 ± 3.27 | 0.153 |
| P. micra | 5.05 ± 2.50 | 4.95 ± 2.55 | 5.14 ± 2.45 | 0.741 |
| P. nigrescens | 2.12 ± 1.99 | 2.43 ± 1.92 | 1.80 ± 2.01 | 0.131 |
| P. gingivalis | 0.34 ± 1.47 | 0.68 ± 2.02 | 0.00 ± 0.00 | 0.082 |
| T. denticola | 1.82 ± 3.16 | 2.17 ± 3.39 | 1.45 ± 2.88 | 0.345 |
| T. forsythia | 4.95 ± 3.20 | 5.66 ± 2.77 | 4.24 ± 3.43 | 0.046 |
| Clostridium IV | 0.43 ± 1.25 | 0.52 ± 1.39 | 0.34 ± 1.09 | 0.441 |
| Clostridium XIV | 6.39 ± 0.75 | 6.54 ± 0.67 | 6.23 ± 0.79 | 0.078 |
| All | Sex | IDB Size | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 0.6 mm | 0.7 mm | 0.8 mm | 0.9 mm | 1.1 mm | ||||||||||||||||||||||||||
| Positive Sites 1 | Positive Subjects 2 | Positive Sites 1 | Positive Subjects 2 | Positive Sites 1 | Positive Subjects 2 | Positive Sites 1 | Positive Subjects 2 | Positive Sites 1 | Positive Subjects 2 | Positive Sites 1 | Positive Subjects 2 | Positive Sites 1 | Positive Subjects 2 | Positive Sites 1 | Positive Subjects 2 | |||||||||||||||||
| HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | HCR | LCR | |
| n | 100 | 100 | 25 | 25 | 40 | 28 | 10 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 31 | 13 | 20 | 68 | 59 | 21 | 22 |
| TB | 100 | 100 | 25 | 25 | 40 | 28 | 10 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 31 | 13 | 20 | 68 | 59 | 21 | 22 |
| Bd | 9 | 13 | 6 | 6 | 1 | 2 | 1 | 1 | 8 | 11 | 5 | 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 1 | 0 | 2 | 4 | 2 | 3 | 5 | 9 | 3 | 5 |
| Lspp | 100 | 100 | 25 | 25 | 40 | 28 | 10 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 31 | 13 | 20 | 68 | 59 | 21 | 22 |
| Rd | 96 | 100 | 24 | 25 | 36 | 28 | 9 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 31 | 13 | 20 | 64 | 59 | 20 | 22 |
| Scri | 77 | 62 | 24 | 22 | 31 | 20 | 10 | 6 | 46 | 42 | 14 | 16 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 3 | 4 | 3 | 17 | 24 | 11 | 15 | 54 | 35 | 21 | 19 |
| Smutans | 34 | 36 | 15 | 18 | 6 | 10 | 5 | 6 | 28 | 26 | 10 | 12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 6 | 3 | 4 | 5 | 10 | 5 | 9 | 24 | 20 | 8 | 13 |
| Ssal | 100 | 100 | 25 | 25 | 40 | 28 | 10 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 31 | 13 | 20 | 68 | 59 | 21 | 22 |
| Ssob | 12 | 1 | 5 | 1 | 3 | 0 | 1 | 0 | 9 | 1 | 4 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 2 | 0 | 4 | 1 | 2 | 1 | 6 | 0 | 3 | 0 |
| Sw | 93 | 82 | 24 | 21 | 34 | 27 | 9 | 7 | 59 | 55 | 15 | 14 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 9 | 5 | 6 | 21 | 25 | 13 | 16 | 62 | 48 | 16 | 18 |
| Ao | 96 | 93 | 25 | 25 | 37 | 27 | 10 | 7 | 59 | 66 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 10 | 5 | 7 | 20 | 29 | 12 | 18 | 67 | 54 | 21 | 22 |
| Vp | 95 | 95 | 25 | 25 | 37 | 25 | 10 | 7 | 58 | 70 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 29 | 13 | 19 | 63 | 56 | 21 | 22 |
| Aa | 9 | 0 | 3 | 0 | 3 | 0 | 1 | 0 | 6 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 0 | 3 | 0 |
| Co | 83 | 76 | 23 | 23 | 27 | 22 | 8 | 6 | 56 | 54 | 15 | 17 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 3 | 5 | 3 | 19 | 28 | 12 | 17 | 54 | 45 | 15 | 19 |
| Ec | 100 | 96 | 25 | 25 | 40 | 27 | 10 | 7 | 60 | 69 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 9 | 5 | 6 | 22 | 30 | 13 | 19 | 68 | 57 | 21 | 22 |
| Smitis | 100 | 100 | 25 | 25 | 40 | 28 | 10 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 21 | 31 | 13 | 20 | 68 | 59 | 21 | 22 |
| Ssan | 98 | 100 | 25 | 25 | 39 | 28 | 10 | 7 | 59 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 21 | 31 | 13 | 20 | 67 | 59 | 21 | 22 |
| Cr | 95 | 93 | 25 | 25 | 37 | 26 | 10 | 7 | 58 | 67 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 7 | 5 | 6 | 20 | 30 | 13 | 20 | 65 | 56 | 21 | 22 |
| Cg | 99 | 93 | 25 | 24 | 39 | 27 | 10 | 7 | 60 | 66 | 15 | 17 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 30 | 13 | 19 | 67 | 53 | 21 | 21 |
| Fn | 100 | 100 | 25 | 25 | 40 | 28 | 10 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 31 | 13 | 20 | 68 | 59 | 21 | 26 |
| Pi | 48 | 36 | 19 | 18 | 17 | 9 | 7 | 4 | 31 | 27 | 12 | 14 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 4 | 2 | 3 | 10 | 9 | 7 | 8 | 35 | 23 | 14 | 13 |
| Pn | 65 | 47 | 21 | 20 | 17 | 10 | 6 | 5 | 48 | 37 | 15 | 15 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 2 | 3 | 2 | 14 | 16 | 9 | 6 | 56 | 29 | 19 | 14 |
| Pm | 81 | 84 | 24 | 24 | 32 | 26 | 10 | 7 | 49 | 58 | 14 | 17 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 7 | 8 | 4 | 6 | 17 | 26 | 11 | 15 | 57 | 50 | 20 | 21 |
| Pg | 11 | 0 | 3 | 0 | 4 | 0 | 1 | 0 | 7 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 1 | 0 | 9 | 0 | 3 | 0 |
| Td | 30 | 21 | 12 | 8 | 10 | 8 | 5 | 4 | 20 | 13 | 7 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 7 | 6 | 4 | 3 | 22 | 15 | 10 | 6 |
| Tf | 83 | 62 | 24 | 20 | 30 | 14 | 10 | 4 | 53 | 48 | 14 | 16 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 7 | 5 | 5 | 16 | 19 | 10 | 12 | 58 | 36 | 20 | 16 |
| ClosIV | 13 | 9 | 7 | 7 | 4 | 5 | 2 | 3 | 9 | 4 | 5 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 2 | 5 | 2 | 8 | 7 | 6 | 6 |
| ClosXIV | 100 | 100 | 25 | 25 | 40 | 28 | 10 | 7 | 60 | 72 | 15 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 10 | 5 | 7 | 22 | 31 | 13 | 20 | 68 | 59 | 21 | 22 |
| Variable | p-Values Interaction Caries Risk x... | ||
|---|---|---|---|
| Sex | IDB Size | BOIB% | |
| TB | 0.835 | 0.812 | 0.376 |
| B. dentium | 0.246 | 0.009 1 | 0.208 |
| Lactobacillus spp. | 0.857 | 0.332 | 0.716 |
| R. dentocariosa | 0.595 | 0.492 | 0.348 |
| S. cristatus | 0.253 | 0.048 1 | 0.166 |
| S. mutans | 0.008 1 | 0.280 | 0.057 |
| S. salivarius | 0.136 | 0.144 | 0.023 1 |
| S. sobrinus | 0.123 | 0.103 | 0.147 |
| S. wiggsiae | 0.139 | 0.666 | 0.426 |
| A. odontolyticus | 0.179 | 0.331 | 0.166 |
| V. parvula | 0.882 | 0.012 1 | 0.075 |
| A. actinomycetemcomitans | 0.203 | 0.064 | 0.194 |
| C. ochracea | 0.124 | <0.001 1 | 0.374 |
| E. corrodens | 0.020 1 | 0.070 | 0.015 1 |
| S. mitis | 0.299 | 0.362 | 0.119 |
| S. sanguinis | 0.643 | 0.421 | 0.034 1 |
| C. rectus | 0.809 | 0.199 | <0.001 1 |
| C. gracilis | 0.400 | 0.752 | 0.605 |
| F. nucleatum | 0.853 | 0.674 | 0.594 |
| P. intermedia | 0.421 | 0.095 | 0.186 |
| P. micra | 0.940 | 0.559 | 0.105 |
| P. nigrescens | 0.001 1 | 0.024 1 | 0.281 |
| P. gingivalis | 0.198 | 0.203 | 0.209 |
| T. denticola | 0.762 | <0.001 1 | 0.020 1 |
| T. forsythia | 0.112 | 0.130 | 0.056 |
| Clostridium IV | 0.306 | 0.005 1 | 0.473 |
| Clostridium XIV | 0.341 | 0.014 1 | 0.062 |
| Variable | Caries Risk | |
|---|---|---|
| High (n = 100) | Low (n = 100) | |
| Streptococcus salivarius | r = 0.22, p = 0.011 | r = 0.21, p = 0.198 |
| Eikenella corrodens | r = 0.07, p = 0.388 | r = 0.22, p = 0.164 |
| Streptococcus sanguinis | r = 0.16, p = 0.008 | r = 0.23, p = 0.213 |
| Campylobacter rectus | r = 0.36, p < 0.001 | r = 0.35, p = 0.030 |
| Treponema denticola | r = 0.12, p = 0.138 | r = 0.23, p = 0.035 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inquimbert, C.; Bourgeois, D.; Bravo, M.; Viennot, S.; Tramini, P.; Llodra, J.C.; Molinari, N.; Dussart, C.; Giraudeau, N.; Carrouel, F. The Oral Bacterial Microbiome of Interdental Surfaces in Adolescents According to Carious Risk. Microorganisms 2019, 7, 319. https://doi.org/10.3390/microorganisms7090319
Inquimbert C, Bourgeois D, Bravo M, Viennot S, Tramini P, Llodra JC, Molinari N, Dussart C, Giraudeau N, Carrouel F. The Oral Bacterial Microbiome of Interdental Surfaces in Adolescents According to Carious Risk. Microorganisms. 2019; 7(9):319. https://doi.org/10.3390/microorganisms7090319
Chicago/Turabian StyleInquimbert, Camille, Denis Bourgeois, Manuel Bravo, Stéphane Viennot, Paul Tramini, Juan Carlos Llodra, Nicolas Molinari, Claude Dussart, Nicolas Giraudeau, and Florence Carrouel. 2019. "The Oral Bacterial Microbiome of Interdental Surfaces in Adolescents According to Carious Risk" Microorganisms 7, no. 9: 319. https://doi.org/10.3390/microorganisms7090319