Effects of Virgin Olive Oils Differing in Their Bioactive Compound Contents on Metabolic Syndrome and Endothelial Functional Risk Biomarkers in Healthy Adults: A Randomized Double-Blind Controlled Trial

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
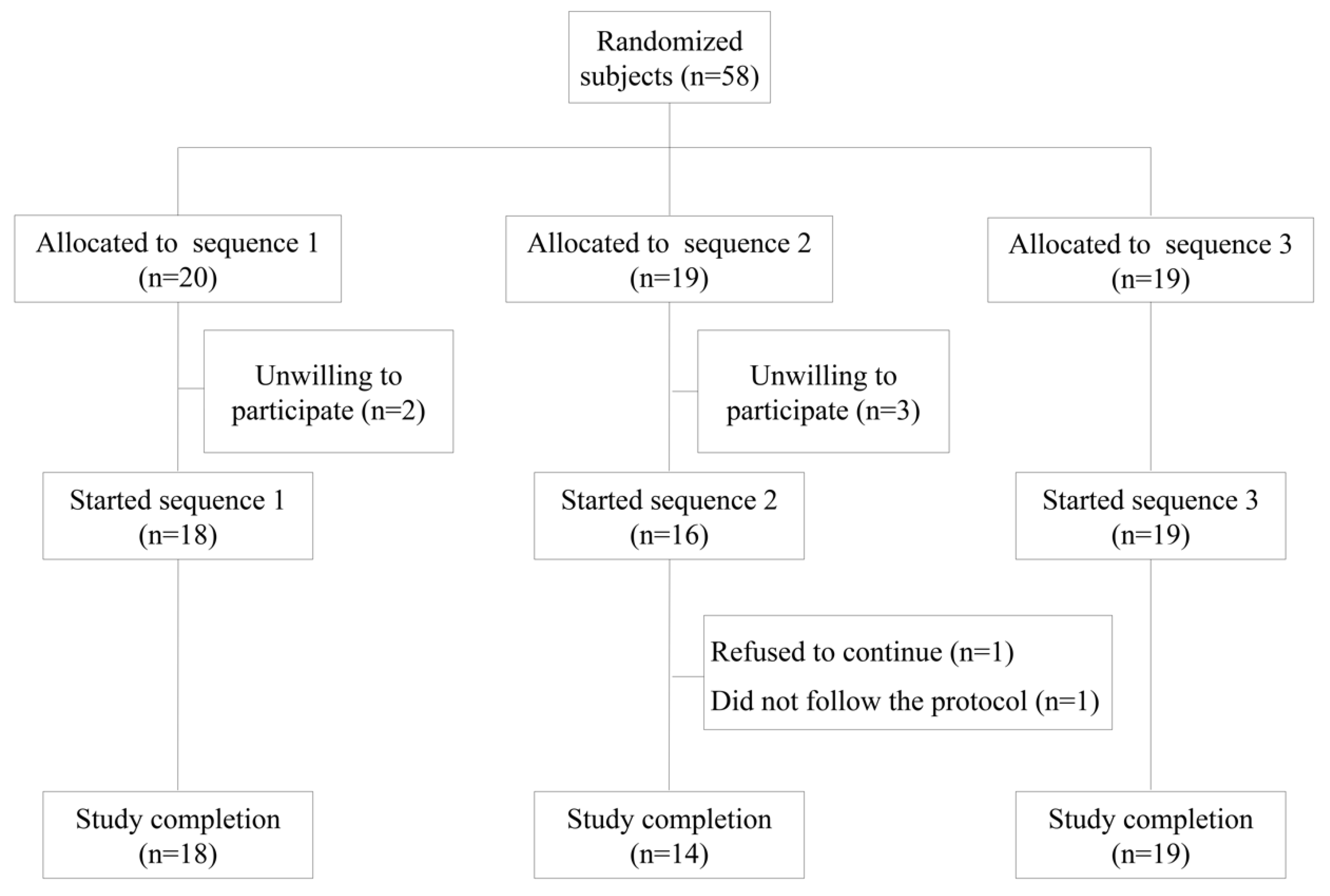
2.1. Subjects
2.2. Study Design
2.3. Evaluation of Dietary Intake
2.4. Blood Sample Collection
2.5. Ex-Vivo Whole Blood Cultures
2.6. Measurement of Metabolic Syndrome Biomarkers
2.7. Measurement of Selected Plasma Hormones and Endothelial Function Biomarkers
2.8. Measurements of Triterpenes and Phenolic Compounds in Urine
2.9. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Nutritional Analysis
3.3. Plasma Metabolic Syndrome and Endothelial Function Biomarkers
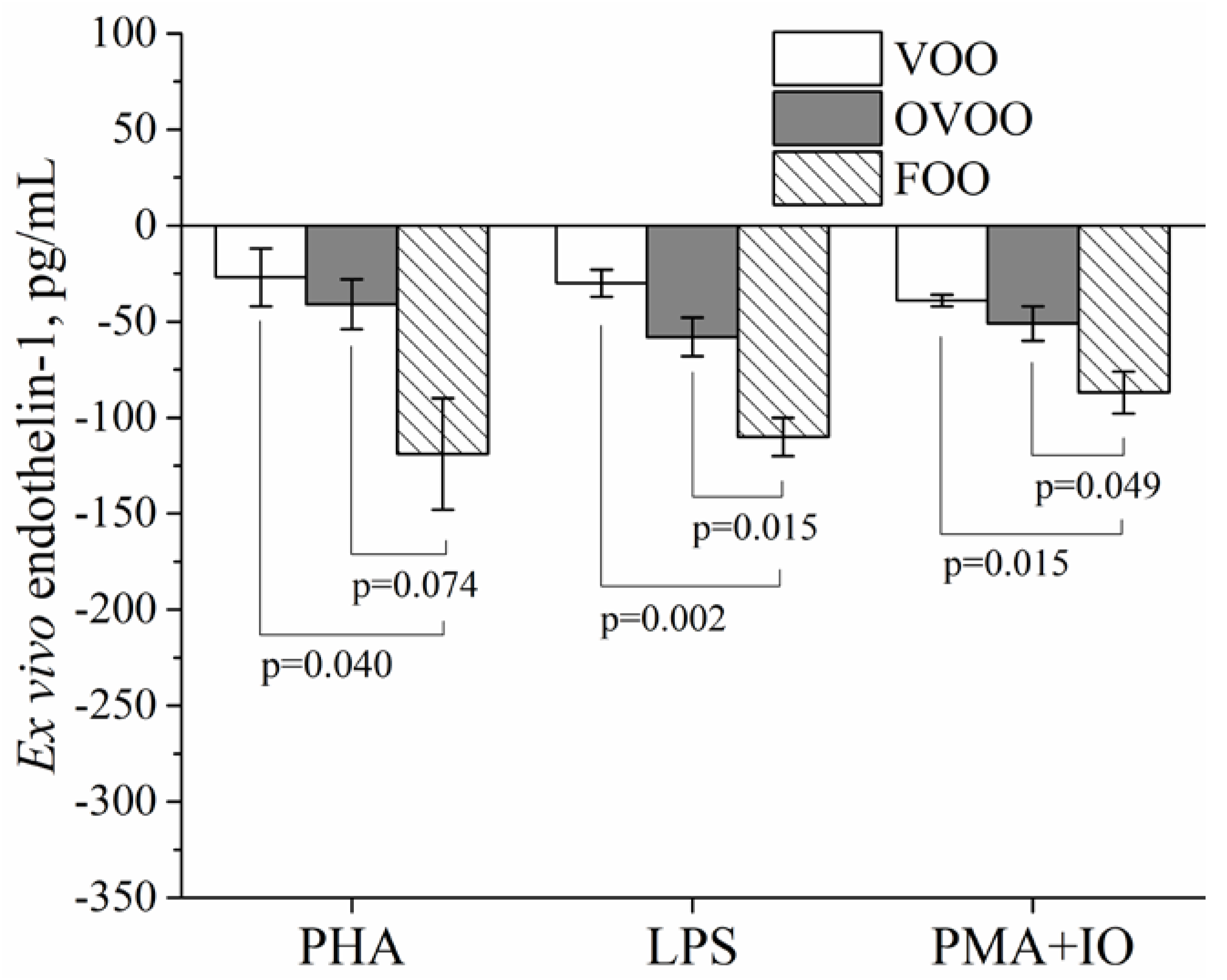
3.4. Plasma Endothelin-1 Ex Vivo Experiments
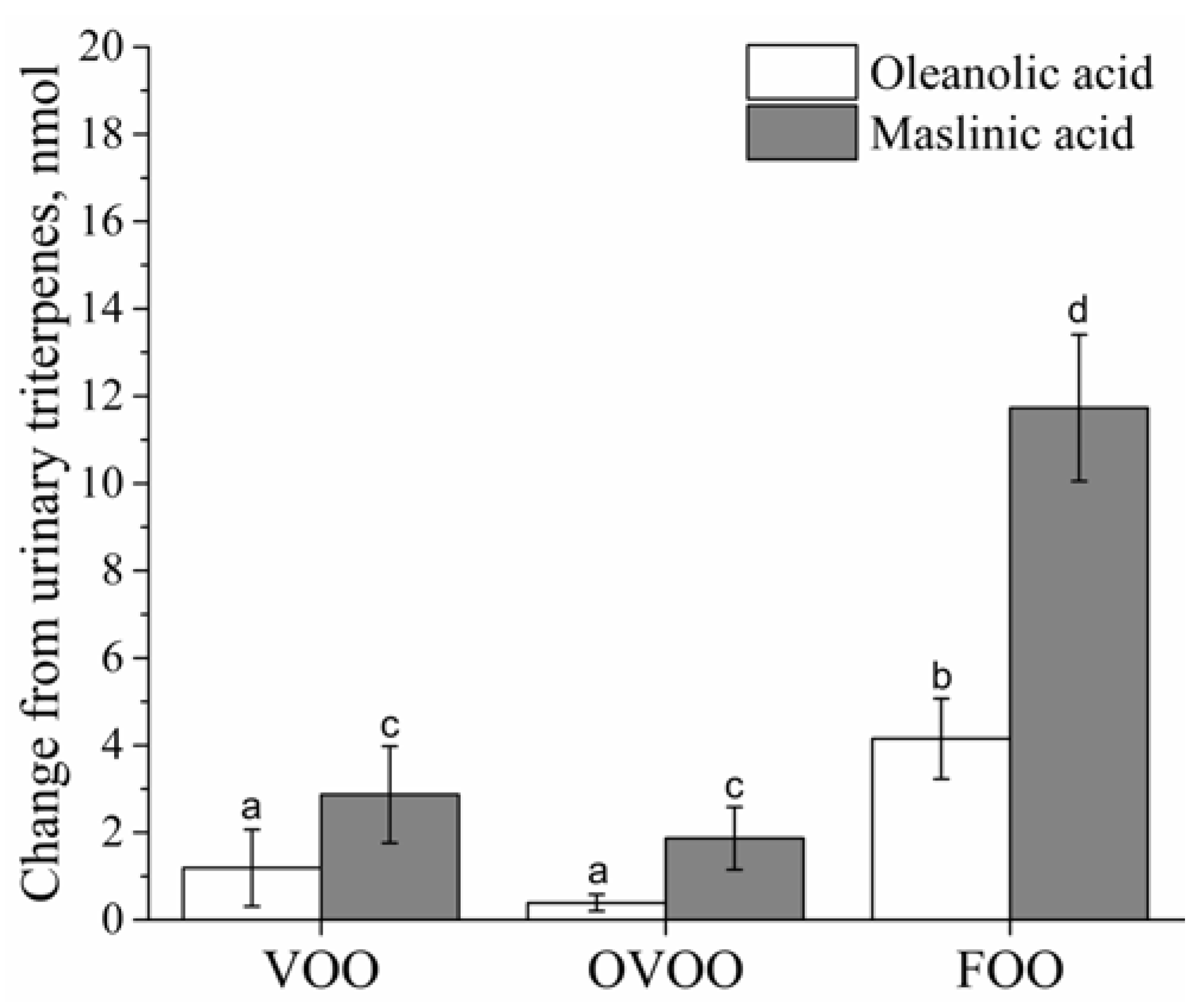
3.5. Biomarkers of Intervention Compliance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A
Analysis of Triterpenes in Urine
References
- Sarafidis, P.A.; Nilsson, P.M. The metabolic syndrome: A glance at its history. J. Hypertens. 2006, 24, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.; Shaw, J. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Freitas Lima, L.C.; Braga, V.A.; do Socorro de França Silva, M.; Cruz, J.C.; Sousa Santos, S.H.; de Oliveira Monteiro, M.M.; Balarini, C.M. Adipokines, diabetes and atherosclerosis: An inflammatory association. Front. Physiol. 2015, 6, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Gardener, H.; Wright, C.B.; Gu, Y.; Demmer, R.T.; Boden-Albala, B.; Elkind, M.S.; Sacco, R.L.; Scarmeas, N. Mediterranean-style diet and risk of ischemic stroke, myocardial infarction, and vascular death: The Northern Manhattan Study. Am. J. Clin. Nutr. 2011, 94, 1458–1464. [Google Scholar] [CrossRef] [PubMed]
- Mayneris-Perxachs, J.; Sala-Vila, A.; Chisaguano, M.; Castellote, A.I.; Estruch, R.; Covas, M.I.; Fitó, M.; Salas-Salvadó, J.; Martínez-González, M.A.; Lamuela-Raventós, R.; et al. Effects of 1-Year Intervention with a Mediterranean Diet on Plasma Fatty Acid Composition and Metabolic Syndrome in a Population at High Cardiovascular Risk. PLoS ONE 2014, 9, e85202. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Christoph, M.; Hoffmann, G. Effects of Olive Oil on Markers of Inflammation and Endothelial Function-A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 7651–7675. [Google Scholar] [CrossRef] [PubMed]
- Covas, M.I.; de la Torre, K.; Farré-Albaladejo, M.; Kaikkonen, J.; Fitó, M.; López-Sabater, C.; Pujadas-Bastardes, M.A.; Joglar, J.; Weinbrenner, T.; Lamuela-Raventós, R.M.; et al. Postprandial LDL phenolic content and LDL oxidation are modulated by olive oil phenolic compounds in humans. Free Radic. Biol. Med. 2006, 40, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Tresserra-Rimbau, A.; Medina-Remón, A.; Pérez-Jiménez, J.; Martínez-González, M.A.; Covas, M.I.; Corella, D.; Salas-Salvadó, J.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Dietary intake and major food sources of polyphenols in a Spanish population at high cardiovascular risk: The PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Storniolo, C.E.; Roselló-Catafau, J.; Pintó, X.; Mitjavila, M.T.; Moreno, J.J. Polyphenol fraction of extra virgin olive oil protects against endothelial dysfunction induced by high glucose and free fatty acids through modulation of nitric oxide and endothelin-1. Redox Biol. 2014, 2, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Quesada, C.; López-Biedma, A.; Warleta, F.; Campos, M.; Beltrán, G.; Gaforio, J.J. Bioactive Properties of the Main Triterpenes Found in Olives, Virgin Olive Oil, and Leaves of Olea europaea. J. Agric. Food Chem. 2013, 61, 12173–12182. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, R. Oleanolic acid and related triterpenoids from olives on vascular function: Molecular mechanisms and therapeutic perspectives. Curr. Med. Chem. 2015, 22, 1414–1425. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). General guidance for stakeholders on the evaluation of Article 13.1, 13.5 and 14 health claims. EFSA J. 2011, 9, 1–24. [Google Scholar]
- Biel, S.; Mesa, M.-D.; de la Torre, R.; Espejo, J.-A.; Fernández-Navarro, J.-R.; Fitó, M.; Sánchez-Rodriguez, E.; Rosa, C.; Marchal, R.; Alche, J.D.; et al. The NUTRAOLEOUM Study, a randomized controlled trial, for achieving nutritional added value for olive oils. BMC Complement. Altern. Med. 2016, 16, 404. [Google Scholar] [CrossRef] [PubMed]
- FDA. U.S. Food and Drug Administration. Available online: https://www.fda.gov/food/labelingnutrition/ucm073992.htm#cardio (accessed on 28 March 2018).
- Covas, M.-I.; Nyyssönen, K.; Poulsen, H.E.; Kaikkonen, J.; Zunft, H.-J.F.; Kiesewetter, H.; Gaddi, A.; de la Torre, R.; Mursu, J.; Bäumler, H.; et al. The Effect of Polyphenols in Olive Oil on Heart Disease Risk Factors. Ann. Intern. Med. 2006, 145, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Fielding, C.J.; Havel, R.J.; Todd, K.M.; Yeo, K.E.; Schloetter, M.C.; Weinberg, V.; Frost, P.H. Effects of dietary cholesterol and fat saturation on plasma lipoproteins in an ethnically diverse population of healthy young men. J. Clin. Investig. 1995, 95, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Kim, M.K.; Hwang, S.H.; Ahn, Y.; Shim, J.E.; Kim, D.H. Relative validities of 3-day food records and the food frequency questionnaire. Nutr. Res. Pract. 2010, 4, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Base de Datos de Composición de Alimentos (BEDCA). Available online: http://www.bedca.net/ (accessed on 28 March 2018).
- Huisman, H.W.; Schutte, A.E.; van Rooyen, J.M.; Schutte, R.; Malan, L.; Fourie, C.M.T.; Malan, N.T. The Association of Red Blood Cell Counts with Endothelin-1 in African and Caucasian Women. Clin. Exp. Hypertens. 2009, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Walter, R.; Mark, M.; Gaudenz, R.; Harris, L.G.; Reinhart, W.H. Influence of nitrovasodilators and endothelin-1 on rheology of human blood in vitro. Br. J. Pharmacol. 1999, 128, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Pozo, O.J.; Pujadas, M.; Gleeson, S.B.; Mesa-García, M.D.; Pastor, A.; Kotronoulas, A.; Fitó, M.; Covas, M.I.; Navarro, J.R.F.; Espejo, J.A.; et al. Liquid chromatography tandem mass spectrometric determination of triterpenes in human fluids: Evaluation of markers of dietary intake of olive oil and metabolic disposition of oleanolic acid and maslinic acid in humans. Anal. Chim. Acta 2017, 990, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Senn, S. Cross-over Trials in Clinical Research, 2nd ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2002; pp. 35–53. [Google Scholar]
- Liu, G.F.; Lu, K.; Mogg, R.; Mallich, M.; Mehrotra, D.V. Should baseline be a covariate or dependent variable in analyses of change from baseline in clinical trials? Stat. Med. 2009, 28, 2509–2530. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Salas-Salvadó, J. Towards an even healthier mediterranean diet. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 1163–1166. [Google Scholar] [CrossRef] [PubMed]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martínez-González, M.A.; Castañer, O.; Bulló, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. CMAJ 2014, 186, E649–E657. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Bulló, M.; Estruch, R.; Ros, E.; Covas, M.-I.; Ibarrola-Jurado, N.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; et al. Prevention of Diabetes with Mediterranean Diets. Ann. Intern. Med. 2014, 160, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Peyrol, J.; Riva, C.; Amiot, M. Hydroxytyrosol in the Prevention of the Metabolic Syndrome and Related Disorders. Nutrients 2017, 9, 306. [Google Scholar] [CrossRef] [PubMed]
- Hohmann, C.D.; Cramer, H.; Michalsen, A.; Kessler, C.; Steckhan, N.; Choi, K.; Dobos, G. Effects of high phenolic olive oil on cardiovascular risk factors: A systematic review and meta-analysis. Phytomedicine 2015, 22, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Giacosa, A.; Morazzoni, P.; Guido, D.; Grassi, M.; Morandi, G.; Bologna, C.; Riva, A.; Allegrini, P.; Perna, S. MediterrAsian Diet Products that Could Raise HDL-Cholesterol: A Systematic Review. BioMed. Res. Int. 2016, 2016, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Farràs, M.; Castañer, O.; Martín-Peláez, S.; Hernáez, Á.; Schröder, H.; Subirana, I.; Muñoz-Aguayo, D.; Gaixas, S.; de la Torre, R.; Farré, M.; et al. Complementary phenol-enriched olive oil improves HDL characteristics in hypercholesterolemic subjects. A randomized, double-blind, crossover, controlled trial. The VOHF study. Mol. Nutr. Food Res. 2015, 59, 1758–1770. [Google Scholar] [CrossRef] [PubMed]
- Hernaez, A.; Fernandez-Castillejo, S.; Farras, M.; Catalan, U.; Subirana, I.; Montes, R.; Sola, R.; Munoz-Aguayo, D.; Gelabert-Gorgues, A.; Diaz-Gil, O.; et al. Olive Oil Polyphenols Enhance High-Density Lipoprotein Function in Humans: A Randomized Controlled Trial. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2115–2119. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Castillejo, S.; Valls, R.-M.; Castañer, O.; Rubió, L.; Catalán, Ú.; Pedret, A.; Macià, A.; Sampson, M.L.; Covas, M.-I.; Fitó, M.; et al. Polyphenol rich olive oils improve lipoprotein particle atherogenic ratios and subclasses profile: A randomized, crossover, controlled trial. Mol. Nutr. Food Res. 2016, 60, 1544–1554. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Castañer, O.; Goday, A.; Ros, E.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Arós, F.; Serra-Majem, L.; et al. The Mediterranean Diet decreases LDL atherogenicity in high cardiovascular risk individuals: A randomized controlled trial. Mol. Nutr. Food Res. 2017, 61, 1601015. [Google Scholar] [CrossRef] [PubMed]
- Nordestgaard, B.G.; Langsted, A.; Mora, S.; Kolovou, G.; Baum, H.; Bruckert, E.; Watts, G.F.; Sypniewska, G.; Wiklund, O.; Borén, J.; et al. Fasting is not routinely required for determination of a lipid profile: Clinical and laboratory implications including flagging at desirable concentration cut-points—A joint consensus statement from the European Atherosclerosis Society and European Federation of Clinical Chemistry and Laboratory Medicine. Eur. Heart J. 2016, 37, 1944–1958. [Google Scholar] [PubMed]
- Saibandith, B.; Spencer, J.; Rowland, I.; Commane, D. Olive Polyphenols and the Metabolic Syndrome. Molecules 2017, 22, 1082. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Liu, J.; Ouyang, Q.; Xuan, C.; Wang, L.; Li, T.; Liu, J. The effects of oleanolic acid on atherosclerosis in different animal models. Acta Biochim. Biophys. Sin. 2017, 49, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Ross, R. The pathogenesis of atherosclerosis: A perspective for the 1990s. Nature 1993, 362, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Gkaliagkousi, E.; Gavriilaki, E.; Triantafyllou, A.; Douma, S. Clinical Significance of Endothelial Dysfunction in Essential Hypertension. Curr. Hypertens. Rep. 2015, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Cambiaggi, C.; Mencarelli, M.; Muscettola, M.; Grasso, G. Gene expression of endothelin-1 (ET-1) and release of mature peptide by activated human neutrophils. Cytokine 2001, 14, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Shinagawa, S.; Okazaki, T.; Ikeda, M.; Yudoh, K.; Kisanuki, Y.Y.; Yanagisawa, M.; Kawahata, K.; Ozaki, S. T cells upon activation promote endothelin 1 production in monocytes via IFN-γ and TNF-α. Sci. Rep. 2017, 7, 14500. [Google Scholar] [CrossRef] [PubMed]
- Massai, L.; Carbotti, P.; Cambiaggi, C.; Mencarelli, M.; Migliaccio, P.; Muscettola, M.; Grasso, G. Prepro-endothelin-1 mRNA and its mature peptide in human appendix. Gastrointest. Liver Physiol. 2003, 284, G340–G348. [Google Scholar] [CrossRef] [PubMed]
- Mencarelli, M.; Pecorelli, A.; Carbotti, P.; Valacchi, G.; Grasso, G.; Muscettola, M. Endothelin receptor A expression in human inflammatory cells. Regul. Pept. 2009, 158, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Achmad, T.H.; Rao, G.S. Chemotaxis of human boold monocytes toward endothelin-1 and the influence of calcium channel blockers. Biochem. Biophys. Res. Commun. 1992, 189, 994–1000. [Google Scholar] [CrossRef]
- Ruetten, H.; Thiemermann, C. Endothelin-1 stimulates the biosynthesis of tumour necrosis factor in macrophages: ET-receptors, signal transduction and inhibitionby dexamethasone. J. Physiol. Pharmacol. 1997, 48, 675–688. [Google Scholar] [PubMed]
- Zouki, C.; Baron, C.; Fournie, A.; Filep, J.G. Endothelin-1 enhances neutrophil adhesion to human coronary artery endothelial cells: Role of ETA receptors and platelet activating factor. Br. J. Pharmacol. 1999, 127, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Zern, T.L.; Fernandez, M.L. Cardioprotective effects of dietary polyphenols. J. Nutr. 2005, 135, 2291–2294. [Google Scholar] [CrossRef] [PubMed]
- Musini, V.M.; Wright, J.M. Factors affecting blood pressure variability: Lessons learned from two systematic reviews of randomized controlled trials. PLoS ONE 2009, 4, e5673. [Google Scholar] [CrossRef] [PubMed]
- Handler, J. The Importance of Accurate Blood Pressure Measurement. Perm. J. 2009, 13, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Rodriguez, R.; Herrera, M.D.; de Sotomayor, M.A.; Ruiz-Gutierrez, V. Pomace Olive Oil Improves Endothelial Function in Spontaneously Hypertensive Rats by Increasing Endothelial Nitric Oxide Synthase Expression. Am. J. Hypertens. 2007, 20, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Valero-Muñoz, M.; Martín-Fernández, B.; Ballesteros, S.; de la Fuente, E.; Quintela, J.C.; Lahera, V.; de las Heras, N. Protective effect of a pomace olive oil concentrated in triterpenic acids in alterations related to hypertension in rats: Mechanisms involved. Mol. Nutr. Food Res. 2014, 58, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Dell’Agli, M.; Fagnani, R.; Mitro, N.; Scurati, S.; Masciadri, M.; Mussoni, L.; Galli, G.V.; Bosisio, E.; Crestani, M.; De Fabiani, E.; et al. Minor Components of Olive Oil Modulate Proatherogenic Adhesion Molecules Involved in Endothelial Activation. J. Agric. Food Chem. 2006, 54, 3259–3264. [Google Scholar] [CrossRef] [PubMed]
- Fitó, M.; Cladellas, M.; de la Torre, R.; Martí, J.; Muñoz, D.; Schröder, H.; Alcántara, M.; Pujadas-Bastardes, M.; Marrugat, J.; López-Sabater, M.C.; et al. Anti-inflammatory effect of virgin olive oil in stable coronary disease patients: A randomized, crossover, controlled trial. Eur. J. Clin. Nutr. 2007, 62, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, N.; Tousoulis, D.; Psaltopoulou, T.; Giolis, A.; Antoniades, C.; Tsiamis, E.; Miliou, A.; Toutouzas, K.; Siasos, G.; Stefanadis, C. Divergent anti-inflammatory effects of different oil acute consumption on healthy individuals. Eur. J. Clin. Nutr. 2011, 65, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Martín-Peláez, S.; Castañer, O.; Konstantinidou, V.; Subirana, I.; Muñoz-Aguayo, D.; Blanchart, G.; Gaixas, S.; de la Torre, R.; Farré, M.; Sáez, G.T.; et al. Effect of olive oil phenolic compounds on the expression of blood pressure-related genes in healthy individuals. Eur. J. Nutr. 2017, 56, 663–670. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| VOO | OVOO | FOO | |
|---|---|---|---|
| Fatty Acid Profile (%) | |||
| C18:0 | 2.3 | 2.2 | 2.1 |
| C18:1n9 | 78.9 | 78.2 | 78.4 |
| C18:2n6 | 6.6 | 6.8 | 6.9 |
| C18:3n3 | 0.6 | 0.7 | 0.7 |
| C20:0 | 0.4 | 0.4 | 0.4 |
| C20:1 | 0.3 | 0.4 | 0.4 |
| C22:0 | 0.1 | 0.1 | 0.1 |
| C24:0 | <0.1 | <0.1 | <0.1 |
| Total phenolic compounds (ppm) | 124 | 490 | 487 |
| Hydroxytyrosol and derivates | 105 | 424.0 | 423.0 |
| Lignanes | 18.2 | 61.3 | 59.2 |
| Flavonoids | 0.7 | 3.4 | 3.2 |
| Simple phenols | 0.0 | 0.9 | 0.9 |
| Total triterpenes (mg/kg) | 86.5 | 86.3 | 388.8 |
| Maslinic acid | 47.3 | 47.3 | 217.7 |
| Oleanolic acid | 39.2 | 39.1 | 171.1 |
| Ursolic acid | <10 | <10 | <10 |
| α-tocopherol (ppm) | 174 | 183 | 176 |
| Squalene (mg/100 g) | 529.2 | 536.2 | 545.5 |
| Total pigments (ppm) | 15.73 | 17.59 | 16.78 |
| Total carotenoid pigments (ppm) | 7.08 | 6.79 | 6.97 |
| Total sterols (ppm) | 1437 | 1396 | 1460 |
| Characteristics | Sequence 1 | Sequence 2 | Sequence 3 |
|---|---|---|---|
| Age, years | 32 ± 2 | 29 ± 2 | 28 ± 2 |
| Gender, male n (%) | 12 (60) | 10 (53) | 8 (42) |
| BMI, kg/m2 | 24 ± 1 | 24 ± 1 | 24 ± 1 |
| Waist circumference, cm | 80 ± 2 | 78 ± 3 | 77 ± 2 |
| Males | 80 ± 3 | 82 ± 4 | 82 ± 2 |
| Females | 81 ± 5 | 73 ± 3 | 73 ± 2 |
| HDLc, mg/dL | 58 ± 2 | 58 ± 3 | 59 ± 2 |
| Males | 55 ± 3 | 51 ± 3 | 52 ± 3 |
| Females | 64 ± 2 | 65 ± 5 | 64 ± 3 |
| LDLc, mg/dL | 117 ± 9 | 107 ± 7 | 102 ± 5 |
| Total cholesterol, mg/dL | 192 ± 10 | 180 ± 7 | 175 ± 7 |
| Triacylglycerols, mg/dL | 87 ± 7 | 81 ± 13 | 67 ± 5 |
| Glucose, mg/dL | 90 ± 2 | 92 ± 2 | 87 ± 2 |
| Adiponectin, mg/L | 11.40 ± 1.38 | 12.49 ± 1.69 | 17.20 ± 2.78 |
| Resistin, µg/L | 16.38 ± 1.88 | 16.57 ± 1.82 | 15.26 ± 1.69 |
| SBP, mmHg | 121 ± 2 | 120 ± 3 | 118 ± 3 |
| DBP, mmHg | 77 ± 2 | 74 ± 2 | 71 ± 2 |
| Pulse pressure, mmHg | 44 ± 2 | 46 ± 3 | 47 ± 2 |
| Endothelin-1, pg/mL | 1.35 ± 0.08 | 1.36 ± 0.10 | 1.38 ± 0.12 |
| sICAM, ng/mL | 74.48 ± 4.50 | 62.26 ± 3.16 | 66.10 ± 4.63 |
| sVCAM, ng/mL | 459 ± 21 | 459 ± 30 | 443 ± 25 |
| Nutritional Characteristics | Sequence 1 | Sequence 2 | Sequence 3 |
|---|---|---|---|
| Energy, kcal | 1976 ± 90 | 2151 ± 138 | 2074 ± 109 |
| Total carbohydrates, g | 200 ± 10 | 213 ± 16 | 214 ± 13 |
| Proteins, g | 80 (16–222) | 96 (37–258) | 93 (21–215) |
| Total fat, g | 86 ± 4 | 102 ± 10 | 89 ± 6 |
| MUFA, g | 31 (12–80) | 33 (6–85) | 33(6–89) |
| PUFA, g | 13 (3–43) | 11 (1–44) | 14 (2–49) |
| SFA, g | 21 (6–64) | 27 (11–80) | 26 (4–66) |
| Vitamin A, µg retinol equivalents | 440 (111–1552) | 512 (109–158) | 539 (7–1669) |
| Vitamin C, mg ascorbic acid | 70 (4–400) | 88 (11–428) | 81 (3–335) |
| Vitamin D, µg | 2 (0–41) | 2 (0–40) | 2 (0–34) |
| Vitamin E, mg α-tocopherol equivalents | 9 (2–29) | 9 (1–67) | 11 (1–39) |
| Cholesterol, mg | 284 ± 26 | 354 ± 31 | 287 ± 24 |
| Alcohol, g | 0 (0–52) | 0 (0–48) | 0 (0–84) |
| Selenium, µg | 31 (5–130) | 34 (1–114) | 36 (3–117) |
| Nutritional Characteristics | VOO | OVOO | FOO |
|---|---|---|---|
| Energy, kcal | 1983 (873–4342) | 2006 (697–4561) | 1914 (780–3457) |
| Total carbohydrates, g | 199 (47–408) | 203 (30–531) | 175 (38–533) |
| Proteins, g | 77 (24–180) | 80 (17–200) | 73 (25–207) |
| Total fat, g | 89 (27–244) | 94 (24–257) | 91 (20–227) |
| MUFA, g | 44 (8–119) | 44 (8–113) | 45 (9–123) |
| PUFA, g | 11 (4–37) | 12 (4–36) | 13 (3–41) |
| SFA, g | 25 (7–74) | 27 (6–82) | 24 (5–69) |
| Vitamin A, µg retinol equivalents | 433 (34–1477) | 427 (26–1504) | 452 (39–1515) |
| Vitamin C, mg ascorbic acid | 48 (0–280) | 60 (0–255) | 55 (1–305) |
| Vitamin D, µg | 1.5 (0–32) | 1.2 (0–82) | 1.2 (0–81) |
| Vitamin E, mg α-tocopherol equivalents | 10 (2–30) | 11 (3–32) | 11 (2–32) |
| Cholesterol, mg | 285 (11–981) | 253 (28–853) | 272 (15–1011) |
| Alcohol, g ethanol | 0 (0–97) | 0 (0–54) | 0 (0–78) |
| Selenium, µg | 30 (0–260) | 31 (0–198) | 31 (1–160) |
| Characteristics | VOO | OVOO | FOO | |||
|---|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | |
| BMI, kg/m2 | 23.9 ± 0.1 | 24 ± 0.1 | 23.9 ± 0.1 | 24 ± 0.1 | 24 ± 0.1 | 24 ± 0.1 |
| Waist circumference, cm | 77.4 ± 0.7 | 77.2 ± 0.7 | 77.2 ± 0.7 | 76.8 ± 0.7 | 77.4 ± 0.7 | 76.9 ± 0.7 |
| HDLc, mg/dL | 58 ± 2 | 59 ± 2 | 57 ± 2 | 60 ± 2 * | 58 ± 2 | 60 ± 2 |
| Males | 52 ± 2 | 53 ± 2 | 52 ± 2 | 52 ± 2 | 52 ± 2 | 54 ± 2 |
| Females | 64 ± 2 | 65 ± 2 | 63 ± 2 | 67 ± 2 * | 65 ± 2 | 66 ± 2 |
| LDLc, mg/dL | 105 ± 4 | 108 ± 4 a,b | 104 ± 4 | 106 ± 4 a | 104 ± 4 | 111 ± 4 b |
| Total cholesterol, mg/dL | 179 ± 5 | 182 ± 5 | 177 ± 5 | 183 ± 5 | 178 ± 5 | 186 ± 5 * |
| Triacylglycerols, mg/dL | 72 ± 7 | 75 ± 7 * | 74 ± 7 | 81 ± 7 * | 75 ± 7 | 75 ± 7 |
| Glucose, mg/dL | 91 ± 2 | 91 ± 2 | 91 ± 2 | 91 ± 2 | 90 ± 2 | 91 ± 2 |
| Adiponectin, mg/L | 13.74 ± 1.7 | 12.8 ± 1.7 | 12.48 ± 1.7 | 13.6 ± 1.71 | 12.62 ± 1.71 | 13.74 ± 1.71 |
| Resistin, µg/L | 14.1 ± 1.1 | 14.1 ± 1.1 | 14.5 ± 1.1 | 13.8 ± 1.1 | 13.8 ± 1.1 | 14.1 ± 1.1 |
| SBP, mmHg | 117 ± 3 | 115 ± 3 *,a | 119 ± 3 | 116 ± 3 a,b | 114 ± 3 | 118 ± 3 *,b |
| DBP, mmHg | 72 ± 2 | 72 ± 2 | 75 ± 2 | 73 ± 2 | 72 ± 2 | 74 ± 2 |
| Pulse pressure, mmHg | 45 ± 1 | 43 ± 1 | 44 ± 1 | 42 ± 1 | 42 ± 1 | 45 ± 1 |
| Endothelin-1, pg/mL | 1.53 ± 0.15 | 1.38 ± 0.15 * | 1.58 ± 0.15 | 1.41 ± 0.15 * | 1.49 ± 0.15 | 1.35 ± 0.15 * |
| sICAM-1, ng/mL | 68.09 ± 3.19 | 67.11 ± 3.19 | 65.17 ± 3.20 | 67.73 ± 3.19 | 65.1 ± 3.20 | 66.7 ± 3.21 |
| sVCAM-1, ng/mL | 451 ± 22 | 443 ± 23 | 435 ± 22 | 451 ± 22 | 431 ± 22 | 442 ± 23 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez-Rodriguez, E.; Lima-Cabello, E.; Biel-Glesson, S.; Fernandez-Navarro, J.R.; Calleja, M.A.; Roca, M.; Espejo-Calvo, J.A.; Gil-Extremera, B.; Soria-Florido, M.; De la Torre, R.; et al. Effects of Virgin Olive Oils Differing in Their Bioactive Compound Contents on Metabolic Syndrome and Endothelial Functional Risk Biomarkers in Healthy Adults: A Randomized Double-Blind Controlled Trial. Nutrients 2018, 10, 626. https://doi.org/10.3390/nu10050626
Sanchez-Rodriguez E, Lima-Cabello E, Biel-Glesson S, Fernandez-Navarro JR, Calleja MA, Roca M, Espejo-Calvo JA, Gil-Extremera B, Soria-Florido M, De la Torre R, et al. Effects of Virgin Olive Oils Differing in Their Bioactive Compound Contents on Metabolic Syndrome and Endothelial Functional Risk Biomarkers in Healthy Adults: A Randomized Double-Blind Controlled Trial. Nutrients. 2018; 10(5):626. https://doi.org/10.3390/nu10050626
Chicago/Turabian StyleSanchez-Rodriguez, Estefania, Elena Lima-Cabello, Sara Biel-Glesson, Jose R. Fernandez-Navarro, Miguel A. Calleja, Maria Roca, Juan A. Espejo-Calvo, Blas Gil-Extremera, Maria Soria-Florido, Rafael De la Torre, and et al. 2018. "Effects of Virgin Olive Oils Differing in Their Bioactive Compound Contents on Metabolic Syndrome and Endothelial Functional Risk Biomarkers in Healthy Adults: A Randomized Double-Blind Controlled Trial" Nutrients 10, no. 5: 626. https://doi.org/10.3390/nu10050626