Dietary Energy Density and Its Association with Overweight or Obesity in Adolescents: A Systematic Review of Observational Studies

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Studies
2.2.2. Subjects
2.2.3. Variables
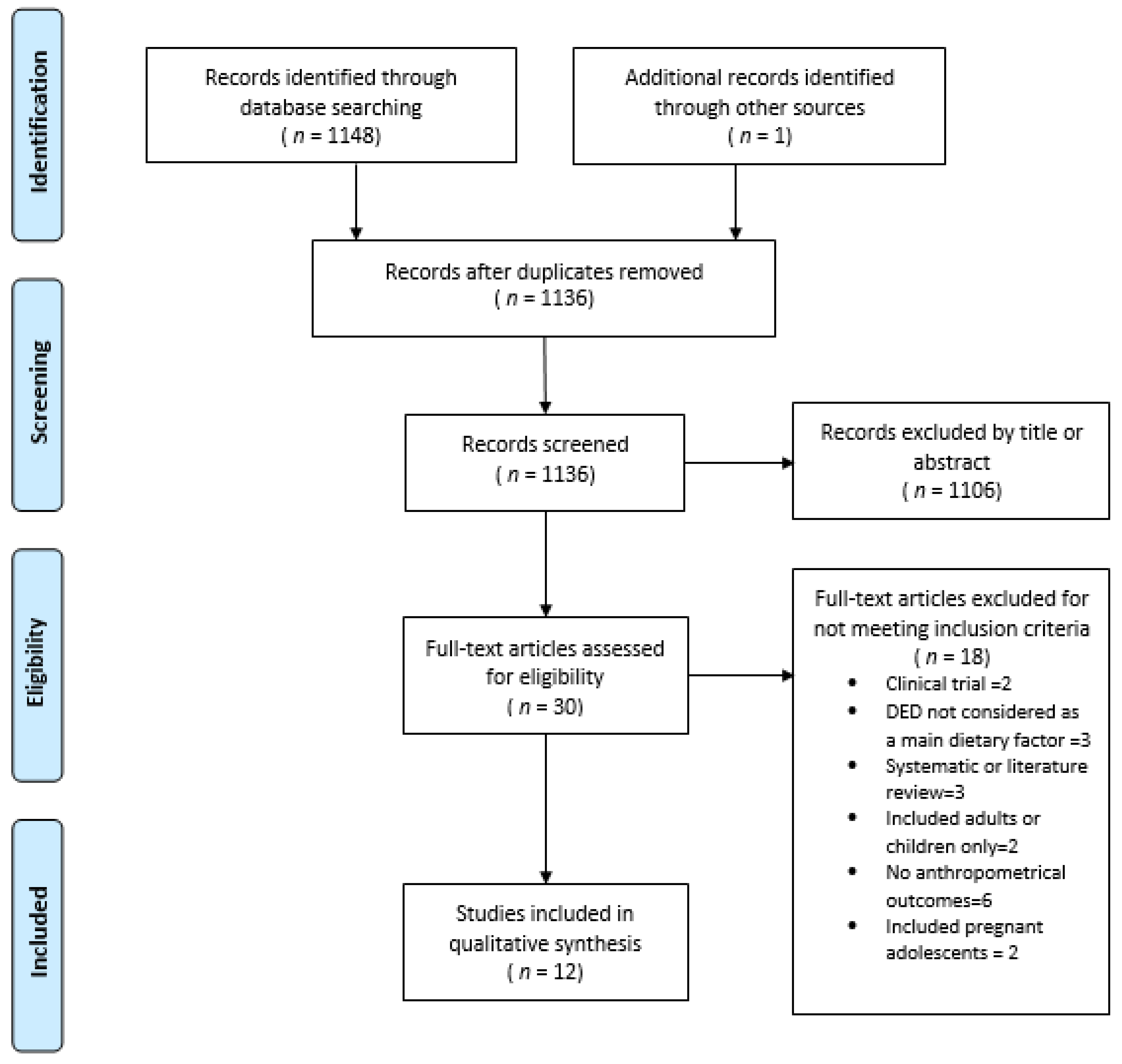
2.3. Study Selection
2.4. Data Extraction
3. Results
3.1. Characteristics of Studies
3.1.1. Anthropometric Measurement
3.1.2. Diet Instrument
3.1.3. DED Calculation Method
3.2. Analysis of the Association between DED and OW/O
3.3. Characteristics of Studies with Positive Associations between DED and OW/O
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Das, J.K.; Salam, R.A.; Thomburg, K.L.; Prentice, A.M.; Campisi, S.; Lassi, Z.S.; Koletzko, B.; Bhutta, Z.A. Nutrition in adolescents: Physiology, metabolism, and nutritional needs. Ann. N. Y. Acad. 2017, 1393, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the development of children’s eating behaviours: From infancy to adolescence. Can. J. Diet. Pract. Res. 2007, 68, s1–s56. [Google Scholar] [PubMed]
- Livingstone, M.B.; Robson, P.J.; Wallace, J.M. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, S213–S222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, M.B.; Robson, P.J. Measurement of dietary intake in children. Proc. Nutr. Soc. 2000, 59, 279–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabin, M.; Kiess, W. Childhood obesity: Current and novel approaches. Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Rivera, J.A.; de Cossio, T.G.; Pedraza, L.S.; Aburto, T.C.; Sánchez, T.G.; Martorell, R. Childhood and adolescent overweight and obesity in Latin America: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 321–332. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study. Lancet 2013, 384, 766–781. [Google Scholar] [CrossRef]
- Spruijt-Metz, D. Etiology, treatment and prevention of obesity in childhood and adolescence: A decade in review. J. Res. Adolesc. 2011, 21, 129–152. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Bach, A.; Serra-Majem, L. Obesity and the Mediterranean diet: A systematic review of observational and intervention studies. Obes. Rev. 2008, 9, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Escamilla, R.; Obbagy, J.E.; Altman, J.M.; Essery, E.V.; McGrane, M.M.; Wong, Y.P.; Spahn, J.M.; Williams, C.L. Dietary energy density and body weight in adults and children: A systematic review. J. Acad. Nutr. Diet. 2012, 112, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Rouhani, M.; Haghighatdoost, F.; Surkan, P.; Azadbakht, L. Associations between dietary energy density and obesity: A systematic review and meta-analysis of observational studies. Nutrition 2016, 32, 1037–1047. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.; Walton, J.; Flynn, A. Dietary energy density and its association with the nutritional quality of the diet of children and teenagers. J. Nutr. Sci. 2013. [Google Scholar] [CrossRef] [PubMed]
- Patterson, E.; Wärnberg, E.; Poortvliet, E.; Kearny, J.M.; Sjöström, M. Dietary energy density as a marker of dietary quality in Swedish children and adolescents: The European Youth Heart Study. EJCN 2010, 64, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Almiron-Roig, E.; Marmonier, C.; Lluch, A. Dietary energy density and body weight: Is there a relationship? Nutr. Rev. 2004, 62, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J. The relationship between dietary energy density and energy intake. Physiol. Behav. 2009, 97, 609–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, L.; Wilks, D.C.; Lindroos, A.K.; Jebb, S.A. Reflections from a systematic review of dietary energy density and weight gain: Is the inclusion of drinks valid? Obes. Rev. 2009, 10, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.; Del-Ponte, B.; Assunção, M.; Santos, I. Consumption of ultra-processed foods and body fat during childhood and adolescence: A systematic review. Public Health Nutr. 2018, 21. [Google Scholar] [CrossRef] [PubMed]
- Ledikwe, J.H.; Blanck, H.M.; Kette, L.; Serdula, M.K.; Seymour, J.D.; Tohill, B.C.; Rolls, B.J. Dietary energy density is associated with energy intake and weight status in US adults. Am. J. Clin. Nutr. 2006, 83, 1362–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendoza, J.A.; Drewnowski, A.; Christakis, D.A. Dietary energy density is associated with obesity and the metabolic syndrome in US adults. Diabetes Care 2007, 30, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am. J. Clin. Nutr. 2008, 87, 846–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilks, D.C.; Mander, A.P.; Jebb, S.A.; Thompson, S.G.; Sharp, S.J.; Turner, R.M.; Lindroos, A.K. Dietary energy density and adiposity: Employing bias adjustments in a meta-analysis of prospective studies. BMC Public Health 2011, 11, 48. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Deysher, M. Caloric compensation and sensory specific satiety: Evidence for self-regulation of food intake by young children. Appetite 1986, 7, 323–331. [Google Scholar] [PubMed]
- Leahy, K.E.; Birch, L.L.; Rolls, B.J. Reducing the energy density of multiple meals decreases the energy intake of preschool-age children. Am. J. Clin. Nutr. 2008, 88, 1459–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cecil, J.E.; Palmer, C.N.; Wrieden, W.; Murrie, I.; Bolton-Smith, C.; Watt, P.; Wallis, D.J.; Hetherington, M.M. Energy intakes of children after preloads: Adjustment, not compensation. Am. J. Clin. Nutr. 2005, 82, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.O.; Liu, Y.; Birch, L.L.; Rolls, B.J. Effects of portion size and energy density on young children’s intake at a meal. Am. J. Clin. Nutr. 2007, 88, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. A prospective analysis of dietary energy density at age 5 and 7 years and fatness at 9 years among UK children. Int. J. Obes. 2008, 32, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Aburto, T.; Cantoral, A.; Hernández, L.; Alicia, L.; Carriquiry, A.L.; Rivera, J. Usual dietary energy density distribution is positively associated with excess body weight in Mexican children. J. Nutr. 2015, 145, 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Van Sluijs, E.M.; Sharp, S.J.; Ambrosini, G.L.; Cassidy, A.; Griffin, S.J.; Ekelund, U. The independent prospective associations of activity intensity and dietary energy density with adiposity in young adolescents. Br. J. Nutr. 2016, 115, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group (2009) Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, E1000097. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses; University of Ottawa: Ottawa, ON, Canada, 2014; Available online: http://www.ohri.ca (accessed on 3 April 2018).
- Alexy, U.; Sichert-Hellert, W.; Kersting, M.; Schultze-Pawlitschko, V. Pattern of long-term fat intake and BMI during childhood and adolescence results of the DONALD Study. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1203–1209. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, T.A.; Rennie, K.L.; Kerr, M.A.; Wallace, J.M.; Hannon-Fletcher, M.P.; Coward, W.A.; Jebb, S.A.; Livingstone, M.B. Energy density of the diet and change in body fatness from childhood to adolescence: Is there a relation? Am. J. Clin. Nutr. 2008, 87, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Gunther, A.; Stahl, L.; Buyken, A.; Kroke, A. Association of dietary energy density in childhood with age and body fatness at the onset of the pubertal growth spurt. Am. J. Clin. Nutr. 2012, 106, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L.; Emmett, P.M.; Northstone, K.; Howe, L.D.; Tilling, K.; Jebb, S.A. Identification of a dietary pattern prospectively associated with increased adiposity during childhood and adolescence. Int. J. Obes. 2012, 36, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Kring, S.I.; Heitmann, B.L. Fiber intake, not dietary energy density, is associated with subsequent change in BMI z-score among sub-groups of children. Obes. Facts 2008, 1, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; van Jaarsveld, C.H.; Emmett, P.M.; Rogers, I.S.; Ness, A.R.; Hattersley, A.T.; Timpson, N.J.; Smith, G.D.; Jebb, S.A. Dietary energy density affects fat mass in early adolescence and is not modified by FTO variants. PLoS ONE 2009, 4, e4594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butte, N.F.; Cai, G.; Cole, S.A.; Wilson, T.A.; Fisher, J.O.; Zakeri, I.F.; Ellis, K.J.; Comuzzie, A.G. Metabolic and behavioral predictors of weight gain in Hispanic children: The Viva la Familia Study. Am. J. Clin. Nutr. 2007, 85, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Arakawa, M. An energy-dense diet is cross-sectionally associated with an increased risk of overweight in male children, but not in female children, male adolescents, or female adolescents in Japan: The Ryukyus child health study. Nutr. Res. 2012, 32, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Xue, H.; Duan, R.; Liu, Y.; Zhang, L.; Harvey, L.; Cheng, G. The Cross-sectional association of energy intake and dietary energy density with body composition of children in Southwest China. Nutrients 2015, 7, 5396–5412. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, T.; Bremner, A.P.; Bremer, H.K.; Seares, M.E.; Beilin, L.J.; Mori, T.A.; Lyons-Wall, P.; Devine, A.; Oddy, W.H. Dairy product consumption, dietary nutrient and energy density and associations with obesity in Australian adolescents. J. Hum. Nutr. Diet. 2015, 28, 452–464. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Méndez, M.A.; Gómez, S.F.; Fito, M.; Ribas, L.; Aranceta, J.; Serra-Majem, L. Energy density, diet quality, and central body fat in a nationwide survey of young Spaniards. Nutrition 2013, 29, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Forrestal, S.G. Energy intake misreporting among children and adolescents: A literature review. Matern. Child Nutr. 2011, 7, 112–127. [Google Scholar] [CrossRef] [PubMed]
- WCRF/AICR. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; World Cancer Research Fund/American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]
- Vernarelli, J.; Mitchell, D.C.; Hartman, T.; Rolls, B. Dietary energy density is associated with body weight status and vegetable intake in U.S. Child. J. Nutr. 2011, 141, 2204–2210. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sasaki, S.; Takahashi, Y.; Uenishi, K.; Japan Dietetic Students’ Study for Nutrition and Biomarkers Group. Dietary energy density is associated with body mass index and waist circumference, but not with other metabolic risk factors, in free-living young Japanese women. Nutrition 2007, 23, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Hartline, H.; Rose, D.; Johnson, C.; Rice, J.; Webber, L. Energy density of foods, but not beverages, is positively associated with body mass index in adult women. Eur. J. Clin. Nutr. 2009, 63, 1411–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, D.N.; Mela, D.J. Determination of energy density of freely selected diets: Methodological issues and implications. Int. J. Obes. 2000, 24, 49–54. [Google Scholar] [CrossRef]
- Peterson, C.M.; Su, H.; Thomas, D.M.; Heo, M.; Golnabi, AH.; Pietrobelli, A.; Heymsfield, S.B. Tri-Ponderal Mass Index vs. Body Mass Index in Estimating Body Fat During Adolescence. JAMA Pediatr. 2017, 171, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, M.B.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133, 895s–920s. [Google Scholar] [CrossRef] [PubMed]
- Burrows, T.; Martin, R.; Collins, A. Systematic review of the validity of dietary assessment methods in Children when compared with the method of doubly labeled Water. J. Am. Diet. Assoc. 2010, 110, 1501–1510. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.; Watson, J.; Burrows, T. Measuring dietary intake in children and adolescence in the context of overweight and obesity. Int. J. Obes. 2010, 34, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Arango-Angarita, A.; Shamah-Levy, T.; Rodríguez-Ramírez, S. Dietary energy density is associated with body mass index-for-age in Mexican adolescents. Matern. Child Nutr. 2018, e12664. [Google Scholar] [CrossRef] [PubMed]
- Méndez, M.; Popkin, B.; Buckland, G.; Schroder, H.; Amiano, P.; Barricarte, A.; Huerta, J.M.; Quirós, J.R.; Sánchez, M.J.; González, C.A. Alternative methods of accounting for underreporting and overreporting when measuring dietary intake-obesity relations. Am. J. Epidemiol. 2011, 173, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Rennie, K.; Coward, A.; Jebbi, S. Estimating under-reporting of energy intake in dietary surveys using an individualized method. Br. J. Nutr. 2007, 97, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, J.A.; Drewnowski, A.; Cheadle, A.; Christakis, D.A. Dietary energy density is associated with selected predictors of obesity in U.S. children. J. Nutr. 2006, 136, 1318–1322. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Country/Study | Design | Years Follow-Up | Age and N Subjects | Diet Instrument | DED Calculation Method | Measurement Indicator OW/O | New-Castle Ottawa Scale 1 |
|---|---|---|---|---|---|---|---|---|
| Alexy et al. (2004) [31] | Germany/DONALD | Cohort | 2 | 228 boys and girls 2 to 18 years | Dietary record | Foods and beverages | Mean of SDS of BMI 2 | 8 |
| Ambrosini et al. (2012) [34] | England/ALSPAC Avon Study | Cohort | 8 | 6672 boys and girls 7 to 15 years | Dietary record, 3-day unweighed food diary | Foods and beverages | FMI3, Risk of obesity | 8 |
| Butte et al. (2007) [37] | United States/, Viva la Familia Study | Cohort | 1 | 879 boys and girls 4 to 19 years | 24-h dietary recall | Includes food and energy containing beverages and excludes non–energy containing beverages and water | Weight gain 4 (kg/years) | 7 |
| Gunther et al. (2011) [33] | Germany/DONALD | Cohort | 3 | 219 boys and girls Mean 6.9 years at baseline 9.4 y ATO | Dietary record | ED_all: included all foods and drinks ED_energy: included all foods and energy containing drinks (5 kcal/100 g). ED_milk: included all foods and milk as a drink, but no other beverages. ED_food: included foods only (solid/liquid). | BMI z-score, FMI 5 | 7 |
| Johnson et al. (2009) [36] | England/Avon Study | Cohort | 3 | 2275 boys and girls 10 to 13 years | 3-day unweighed diet diaries | Solid food only | Fat mass, FMI 3 | 8 |
| Kring and Heitman (2008) [35] | Denmark | Cohort | 3 | 398 boys and girls 8 to 10 years 9.6 years at baseline | 24-h dietary recall | Foods and beverages | BMI Z-Score | 8 |
| McCaffrey et al. (2008) [32] | Ireland | Cohort | 8 | 48 Boys/girls; 6–8 years at baseline and followed up at 13 to 18 years | 7-d weighed food records | ED all: All foods and all energy containing beverages and energy-free beverages and water. ED Foods: All foods, milk as food. ED soup: All foods, milk as food, and soups. ED Solid: All solid foods ED Energy: All foods, milk as food, soups, and energy-containing beverages | Body weight, BMI z-score, WC, FFM 6, FMI 6, %BF 6 | 7 |
| Murakami et al. (2012) [38] | Japan/RYUCHS | Cross-sectional | NA | 15,974 children and 8202 adolescents. Children 6 to 11 years. Adolescents 12 to 15 years | Diet history questionnaire BDHQCA | Solid food only | BMI 7 | 8 |
| O’Sullivan et al. (2015) [40] | Australian | Cross-sectional | NA | 1613 boys and girls 14 years | FFQ | Food only, food and all beverages, food and all beverages excluding water, and food and energy containing beverages | BMI 8 and WR | 8 |
| Schröder et al. (2013) [41] | Spain | Cross-sectional | NA | 2513 adolescents 10 to 24 years | 24-h dietary recall | Solid food only | WC | 8 |
| Van Sluijs et al. (2016) [28] | United Kingdom/SPEEDY Study | Cohort | 4 | 367 adolescents 10 years at baseline, 14 years at follow-up | 4-d food diary | Solid food only | WC, % BF 9, FMI9, weight status | 9 |
| Zhou et al. (2015) [39] | China | Cross-sectional | NA | 1207 boys and girls 8 to 14 years | 24 -h dietary recall | ED1: Foods and beverages ED2: Solid food only ED3: All solid foods and milk ED4: solid foods and energy-containing beverages (>21 kJ or 5 kcal per 100 g) ED 5 Included solid foods, and milk and energy-containing beverages | BMI z-score, % BF10, FMI 10, FFMI 10 and WHR | 8 |
| Author | Type of Variable (DED) | Statistical Analysis | Energy (Underreporting) Estimate | Adjustment Variables | DED Value/Mean (kJ/g/kcal/g) 1 | β, OR, p Value | Results |
|---|---|---|---|---|---|---|---|
| Alexy et al. (2004) [31] | Continuous | Cluster analysis | EI:BMR Goldberg formula to estimate plausibility of energy intake | Sex, age, education level, occupation level of parents, anthropometric characteristics (BMI), energy, macronutrient and food group intakes. | 3.9 | Cluster of fat intake pattern DED p < 0.0001 Medium 4.0 (0.4) High 4.1 (0.4) Low 3.7 (0.4) BMI p 0.05 Medium 0.11 (0.85) High 0.06 (0.88) Low 0.26 (0.70) | During the study period, the highest SDS of BMI was observed in the low fat cluster (p 0.05) and the DED was lowest in the low fat cluster (p < 0.001) |
| Ambrosini et al. (2012) [34] | Categorical: Quintiles of DP at 7, 10 and 13 year | Multiple linear regression model | EI: EER Individuals were categorized as plausible, underreporters and overreporters. It was included as a categorical covariate in all analyses | Model 1: Age, sex and dietary misreporting Model 2: model 1 + physical activity Model 3: model 1 + maternal education level and maternal pre-pregnancy BMI | NR | 13 years quintile 1 and 2 Model. β 0.03 95% CI (0.01–0.03) p 0.003. 3. Model. β 0.01 95% CI (0.01–0.03) p 0.348 | Energy-dense, high-fat, low-fiber dietary patterns are positively associated with a higher FMI. |
| Butte et al. (2007) [37] | Continuous | GEE population-averaged panel data models, multiple lineal regression | NR | Model 1: Age, sex, age squared, Tanner stage Model 2:Model 1 + BMI status | 1.32 | Model 1.β 0.24 ± 0.39 p 0.53 Model 2. β 0.23 ± 0.35 p 0.50 | No significant association was found between DED and weight gain. |
| Gunther et al. (2011) [33] | Categorical: Tertiles of ED (T1–T3) | Multiple linear regression model | NR | Sex; birth year; birth weight, maternal overweight, maternal age at birth, protein percentage of total energy intake, fat, fibre and baseline BMI/FMI Z-score. | ED all 4·1 ED energy 5·1 ED milk 6·0 ED food 6·9 | Lesmean (Least square mean) BMI Z-score at ATO Tertile l. 0 CI (−0.1, 0.2) Tertile 2. 0 CI (−0.1, 0·1) Tertile 3. 0 CI (−0.1, 0·2) p 0·8 FMI Z-score at ATO Tertile l. 0 CI (−0.2, 0.1) Tertile 2. −0.1 CI (−0.2, 0·1) Tertile 3. 0.1 CI (−0.1, 0·2) p 0·9 | DED was not associated with BMI z score and FMI at age of pubertal takeoff. DED in childhood did not influence timing or body fatness at ATO. |
| Johnson et al. (2009) [36] | Continuous | Multivariate models, multiple linear regression model | EI:EER Categorical misreporting variable (under-, plausible-, and over-reporter) was used as a covariate in regression analyses | Model 1: DED, sex, height at age 13 years, misreporting of energy intake Model 2: Model 1 + Puberty, overweight status at 10 years, energy intake of drinks, maternal education, TV watching, and physical activity | 8.64 | DED β 0.21 ± 0.05 kg (0.12, 0.30) DED 2 β 0.16 ± 0.06 kg FTO β 0.68 ± 0.25 (0.44, 0.93) | Each 1 kJ/g DED at age 10 years was positively associated with fat mass at age 13 years (p 0.05) |
| Kring and Heitman (2008) [35] | Continuous | Multivariate models, multiple linear regression model | TEEDLWEI/TEEDLW (doubly labeled water) EI/EE Defined as reporting bias ratio. | Z-score, age, physical activity level, dietary volume and puberty at baseline. | Normal weight 4.6 Overweight 4.4 | BMI Z-score Boys Crude β –0.02 CI (–0.25; 0.15) p 0.60Adjusted β–0.04 CI (–0.29; 0.20) p 0.88 BMI Z-score Girls Crude β 0.21 CI (–0.3; 0.31) p 0.93 Adjusted β 0.23 CI (–0.07; 0.53) p 0.51 | No significant association between DED and subsequent excess weight change was seen. DED was not associated with weight gain among children going through puberty |
| McCaffrey et al. (2008) [32] | Continuous and categorical (DED calculation method) | Logistic regression model adjusted for covariables | EI:EE Used as a covariate in the models | Sex, pubertal status, EI:EE, ED method | ED All 5.20 (4.93–5.92) ED Food: 8.28 (7.53–8.85) ED Soup:8.22 (7.53–8.81) ED solid: 9.17 (8.54–9.97) ED energy: 6.07 (5.59–6.49) | ED all OR 1.2 CI (0.53, 2.9) p 0.629 ED Food OR 2.1 CI (1.08, 4.17) p 0.029 ED soup OR 2.2 CI (1.09, 4.25) p 0.026 ED solid OR 1.9 CI (1.05, 3.57) p 0.033 ED energy OR 1.6 CI (0.65, 3.90) p 0.306 | It depends on the method of calculation: association with FMI, but not with change in %BF, BMI, z-scores or WC. No association was found when beverages were included |
| Murakami et al. (2012) [38] | Categorical: ED categorized at quintile points | Logistic regression model crude and adjusted for covariables | EI:EER Used as a covariate in the models | Age, paternal and maternal educational level, television or computer game use, municipality, habitual exercise rate of eating,EI:EER, dietary glicemic load and energy intake from beverages | Adolescents 5.1 | DED Quintile adjusted OR Boys Q2 0.98 CI (0.73,1.33) Q3 0.85 CI (0.63,1.16) Q4 0.90 CI (0.66,1.22) Q5 0.78 CI (0.57, 1.07) p 0.10 Girls Q2 0.85 CI (0.62,1.18) Q3 0.60 CI (0.42,0.85) Q4 0.65 CI(0.46,0.92) Q5 0.86 CI (0.61–1.20) p 0.12 | DED was not associated with BMI in adolescents. |
| O’Sullivan et al. (2015) [40] | Continuous | Multivariate adjusted models, logistic regression and multiple linear regression | EI:EER Individuals were categorized as plausible, underreporters and overreporters. It was included as a categorical covariate in all analyses | Model 1: Adjusted for sex, family income, maternal education, puberty stage and physical, activity/screen use. Model 2: Model 1 adjusted for total daily kJ intake. Misreporting | 4.46 | BMI Foods and beverages Model 1 0.83 (0.70, 0.99) p 0.04 Model 2 0.85 (0.71, 1.01) p 0.07 Foods Model 1. 0.87 (0.77, 0.99) p 0.04 Model 2. 0.90 (0.80, 1.02) p 0.08 Waist-height ratio Foods and beverages 1. 0.86 (0.74, 1.01) p 0.06 2. 0.88 (0.75, 1.03) p 0.12 Foods 1. 0.88 (0.79, 0.99) p 0.03 2. 0.90 (0.80, 1.01) p 0.08 | ED measures and dairy intake were inversely associated with obesity after adjustment for confounders; associations became non-significant after energy adjustment. |
| Schröder et al. (2013) [41] | Continuous and categorical: quartiles of DED | Multiple linear regression analysis, multiple logistic regression models | EI:BMR | Model 1: Sex and age Model 2: Sex, age., Leisure-time physical activity, low energy reporting, dietary fiber, maternal educational level, population size and energy intake from beverages | Kcal/g Q1: 0.94 Q2: 1.30 Q3: 1.57 Q4: 2.09 | 1. β −0.001 (−0.003, 0.001) p 0.005 2. β 0.003 (0.001,0.005) p 0.004 WC residuals 0.724 (0.377; 1.076) p <0.001 | Higher DED is a risk for increased central fat distribution. DED was positively associated with abdominal obesity |
| Van Sluijs et al. (2016) [28] | Continuous | Multiple linear regression analysis and multiple logistic regression model | EI:EER Underreporting included as a continuous variable in the models | Model 1: Age, Sex Model 2. Model 1 socio-economic status, birth weight, maternal BMI, puberty status at follow-up, sleep duration. Model 3: model 2 + baseline DED for PA exposures and baseline MVPA for DED. Energy intake (kJ) from drinks and under-reporting. | At baseline 7.7 At follow-up 0.45 | DED at baseline: WC: β 0.72 (0.26,1.17) FMI: β 0·22 (−0·08, 0·52) % BF: β 0·18 (−0·14, 0·50) DED at follow-up: WC: β −0·27 (−1·02, 0·48) FMI:β −0.86 (−1·59, −0·12) % BF:β −0.86 (−1·25, −0·11) | Positive association between DED and WC at baseline but not at follow-up. No association with FMI and %BF at baseline or follow up. The directions of associations with DED were inconsistent. |
| Zhou et al. (2015) [39] | Categorical: tertiles of ED (T1–T3) | Multivariate regression models (Linear trends) 2 | EI:EER Underreporters were excluded from the analysis | Age, birth weight; exclusive breastfeeding duration; the timing of adding complementary foods; physical activity; parental education level; overweight parental BMI, smoking in the house; the percentage of EI from protein, fat, carbohydrate, and fiber intake | ED 1. 4.1 ED2. 6.75 ED3. 5.8 ED4. 6.5 ED 5. 5.6 | DED Tertiles BMI z-score Boys Tertil 1. 0.2 CI (0.1, 0.4) Tertil 2. 0.2 CI (0.1, 0.4) Tertil 3. 0.1 CI (0.1, 0.3) p 0.9 Girls Tertil 1. 0.3 CI (0.1, 0.5) Tertil 2. 0.4 CI (0.1, 0.6) Tertil 3. 0.5 CI (0.3, 0.7) p 0.3 FMI Boys Tertil 1. 3.3 CI(2.9, 3.7) Tertil 2. 3.4 CI (3.1, 3.8) Tertil 3. 3.5 CI (3.1, 3.8) p 0.2 Girls Tertil 1 3.2 CI (2.9, 3.5) Tertil 2 3.2 CI (2.9, 3.5) Tertil 3 3.3 CI (3.0, 3.6) p 0.9 | No association was found between DED and BMI, FMI, FFMI, WHR and %BF. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arango-Angarita, A.; Rodríguez-Ramírez, S.; Serra-Majem, L.; Shamah-Levy, T. Dietary Energy Density and Its Association with Overweight or Obesity in Adolescents: A Systematic Review of Observational Studies. Nutrients 2018, 10, 1612. https://doi.org/10.3390/nu10111612
Arango-Angarita A, Rodríguez-Ramírez S, Serra-Majem L, Shamah-Levy T. Dietary Energy Density and Its Association with Overweight or Obesity in Adolescents: A Systematic Review of Observational Studies. Nutrients. 2018; 10(11):1612. https://doi.org/10.3390/nu10111612
Chicago/Turabian StyleArango-Angarita, Andrea, Sonia Rodríguez-Ramírez, Lluis Serra-Majem, and Teresa Shamah-Levy. 2018. "Dietary Energy Density and Its Association with Overweight or Obesity in Adolescents: A Systematic Review of Observational Studies" Nutrients 10, no. 11: 1612. https://doi.org/10.3390/nu10111612