Latent Iron Deficiency as a Marker of Negative Symptoms in Patients with First-Episode Schizophrenia Spectrum Disorder

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Sociodemographic and Clinical Data
2.3. Laboratory Measures
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of interest
References
- Kim, S.W.; Jhon, M.; Kim, J.M.; Smesny, S.; Rice, S.; Berk, M.; Klier, C.M.; McGorry, P.D.; Schafer, M.R.; Amminger, G.P. Relationship between Erythrocyte Fatty Acid Composition and Psychopathology in the Vienna Omega-3 Study. PLoS ONE 2016, 11, e0151417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, K.L.; Kahn, R.S.; Ko, G.; Davidson, M. Dopamine in schizophrenia: A review and reconceptualization. Am. J. Psychiatry 1991, 148, 1474–1486. [Google Scholar] [PubMed]
- Kim, A.; Nemeth, E. New insights into iron regulation and erythropoiesis. Curr. Opin. Hematol. 2015, 22, 199–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganz, T.; Nemeth, E. Regulation of iron acquisition and iron distribution in mammals. Biochim. Biophys. Acta 2006, 1763, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Moos, T.; Morgan, E.H. The metabolism of neuronal iron and its pathogenic role in neurological disease: Review. Ann. N. Y. Acad. Sci. 2004, 1012, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Stankiewicz, J.; Panter, S.S.; Neema, M.; Arora, A.; Batt, C.E.; Bakshi, R. Iron in chronic brain disorders: Imaging and neurotherapeutic implications. Neurotherapeutics 2007, 4, 371–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hare, D.; Ayton, S.; Bush, A.; Lei, P. A delicate balance: Iron metabolism and diseases of the brain. Front. Aging Neurosci. 2013, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Valles, A.; Flores, C.; Luheshi, G.N. Prenatal Inflammation-Induced Hypoferremia Alters Dopamine Function in the Adult Offspring in Rat: Relevance for Schizophrenia. PLoS ONE 2010, 5, e10967. [Google Scholar] [CrossRef] [PubMed]
- Felt, B.T.; Beard, J.L.; Schallert, T.; Shao, J.; Aldridge, J.W.; Connor, J.R.; Georgieff, M.K.; Lozoff, B. Persistent neurochemical and behavioral abnormalities in adulthood despite early iron supplementation for perinatal iron deficiency anemia in rats. Behav. Brain Res. 2006, 171, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Unger, E.L.; Paul, T.; Murray-Kolb, L.E.; Felt, B.; Jones, B.C.; Beard, J.L. Early iron deficiency alters sensorimotor development and brain monoamines in rats. J. Nutr. 2007, 137, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Kwik-Uribe, C.L.; Gietzen, D.; German, J.B.; Golub, M.S.; Keen, C.L. Chronic marginal iron intakes during early development in mice result in persistent changes in dopamine metabolism and myelin composition. J. Nutr. 2000, 130, 2821–2830. [Google Scholar] [CrossRef] [PubMed]
- Gutteridge, J.M. Iron and oxygen radicals in brain. Ann. Neurol. 1992, 32, S16–S21. [Google Scholar] [CrossRef] [PubMed]
- Hyacinthe, C.; De Deurwaerdere, P.; Thiollier, T.; Li, Q.; Bezard, E.; Ghorayeb, I. Blood withdrawal affects iron store dynamics in primates with consequences on monoaminergic system function. Neuroscience 2015, 290, 621–635. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, L.; Zhang, L.; Qu, Y.; Mu, D. Iron Status in Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169145. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, D.; Burkman, E. Relationship of serum ferritin level and tic severity in children with Tourette syndrome. Childs Nerv. Syst. 2017, 33, 1373–1378. [Google Scholar] [CrossRef] [PubMed]
- Ghorayeb, I.; Gamas, A.; Mazurie, Z.; Mayo, W. Attention-Deficit Hyperactivity and Obsessive-Compulsive Symptoms in Adult Patients with Primary Restless Legs Syndrome: Different Phenotypes of the Same Disease? Behav. Sleep Med. 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Oner, O.; Alkar, O.Y.; Oner, P. Relation of ferritin levels with symptom ratings and cognitive performance in children with attention deficit-hyperactivity disorder. Pediatr. Int. 2008, 50, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Earley, C.J.; Connor, J.; Garcia-Borreguero, D.; Jenner, P.; Winkelman, J.; Zee, P.C.; Allen, R. Altered brain iron homeostasis and dopaminergic function in Restless Legs Syndrome (Willis-Ekbom Disease). Sleep Med. 2014, 15, 1288–1301. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Shin, I.S.; Kim, J.M.; Park, K.H.; Youn, T.; Yoon, J.S. Factors potentiating the risk of mirtazapine-associated restless legs syndrome. Hum. Psychopharmacol. 2008, 23, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Earley, C.J.; Connor, J.R.; Beard, J.L.; Malecki, E.A.; Epstein, D.K.; Allen, R.P. Abnormalities in CSF concentrations of ferritin and transferrin in restless legs syndrome. Neurology 2000, 54, 1698–1700. [Google Scholar] [CrossRef] [PubMed]
- Piao, Y.S.; Lian, T.H.; Hu, Y.; Zuo, L.J.; Guo, P.; Yu, S.Y.; Liu, L.; Jin, Z.; Zhao, H.; Li, L.X.; et al. Restless legs syndrome in Parkinson disease: Clinical characteristics, abnormal iron metabolism and altered neurotransmitters. Sci. Rep. 2017, 7, 10547. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.; Erikson, K.; Pinero, D.J.; Beard, J.L. In vivo dopamine metabolism is altered in iron-deficient anemic rats. J. Nutr. 1997, 127, 2282–2288. [Google Scholar] [CrossRef] [PubMed]
- Barton, A.; Bowie, J.; Ebmeier, K. Low plasma iron status and akathisia. J. Neurol. Neurosurg. Psychiatry 1990, 53, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.W.; Glen, S.E.; White, T. Low serum iron status and akathisia. Lancet 1987, 1, 1234–1236. [Google Scholar] [CrossRef]
- O’Loughlin, V.; Dickie, A.C.; Ebmeier, K.P. Serum iron and transferrin in acute neuroleptic induced akathisia. J. Neurol. Neurosurg. Psychiatry 1991, 54, 363–364. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, M.; Seifritz, E.; Botschev, C.; Krauchi, K.; Muller-Spahn, F. Serum iron and ferritin in acute neuroleptic akathisia. Psychiatry Res. 2000, 93, 201–207. [Google Scholar] [CrossRef]
- Kuloglu, M.; Atmaca, M.; Ustundag, B.; Canatan, H.; Gecici, O.; Tezcan, E. Serum iron levels in schizophrenic patients with or without akathisia. Eur. Neuropsychopharmacol. 2003, 13, 67–71. [Google Scholar] [CrossRef]
- Nemes, Z.C.; Rotrosen, J.; Angrist, B.; Peselow, E.; Schoentag, R. Serum iron levels and akathisia. Biol. Psychiatry 1991, 29, 411–413. [Google Scholar] [CrossRef]
- Barnes, T.R.; Halstead, S.M.; Little, P.W. Relationship between iron status and chronic akathisia in an in-patient population with chronic schizophrenia. Br. J. Psychiatry 1992, 161, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.; Loneragan, C. Acute drug-induced akathisia is not associated with low serum iron status. Psychopharmacology 1991, 103, 138–139. [Google Scholar] [CrossRef] [PubMed]
- Altamura, S.; Muckenthaler, M.U. Iron toxicity in diseases of aging: Alzheimer’s disease, Parkinson’s disease and atherosclerosis. J. Alzheimers Dis. 2009, 16, 879–895. [Google Scholar] [CrossRef] [PubMed]
- Peralta, V.; Cuesta, M.J.; Mata, I.; Serrano, J.F.; Perez-Nievas, F.; Natividad, M.C. Serum iron in catatonic and noncatatonic psychotic patients. Biol. Psychiatry 1999, 45, 788–790. [Google Scholar] [CrossRef]
- Weiser, M.; Levkowitch, Y.; Neuman, M.; Yehuda, S. Decrease of serum iron in acutely psychotic schizophrenic patients. Int. J. Neurosci. 1994, 78, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Dallman, P.R. Biochemical basis for the manifestations of iron deficiency. Annu. Rev. Nutr. 1986, 6, 13–40. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, V.; Amin, S.B.; Agarwal, A.; Srivastava, L.M.; Soni, A.; Saluja, S. Latent iron deficiency at birth influences auditory neural maturation in late preterm and term infants. Am. J. Clin. Nutr. 2015, 102, 1030–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorder, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Schimmelmann, B.G.; Huber, C.G.; Lambert, M.; Cotton, S.; McGorry, P.D.; Conus, P. Impact of duration of untreated psychosis on pre-treatment, baseline, and outcome characteristics in an epidemiological first-episode psychosis cohort. J. Psychiatr. Res. 2008, 42, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.S.; Ahn, Y.M.; Shin, H.K.; An, S.K.; Joo, Y.H.; Kim, S.H.; Yoon, D.J.; Jho, K.H.; Koo, Y.J.; Lee, J.Y. Reliability and validity of the Korean version of the Positive and Negative Syndrome Scale. J. Korean Neuropsychiatr. Assoc. 2001, 40, 1090–1105. [Google Scholar]
- Emsley, R.; Rabinowitz, J.; Torreman, M. The factor structure for the Positive and Negative Syndrome Scale (PANSS) in recent-onset psychosis. Schizophr. Res. 2003, 61, 47–57. [Google Scholar] [CrossRef]
- Addington, D.; Addington, J.; Schissel, B. A depression rating scale for schizophrenics. Schizophr. Res. 1990, 3, 247–251. [Google Scholar] [CrossRef]
- Kim, S.W.; Kim, S.J.; Yoon, B.H.; Kim, J.M.; Shin, I.S.; Hwang, M.Y.; Yoon, J.S. Diagnostic validity of assessment scales for depression in patients with schizophrenia. Psychiatry Res. 2006, 144, 57–63. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-IV-TR; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Jhon, M.; Yoo, T.; Lee, J.Y.; Kim, S.Y.; Kim, J.M.; Shin, I.S.; Williams, L.; Berk, M.; Yoon, J.S.; Kim, S.W. Gender-specific risk factors for low bone mineral density in patients taking antipsychotics for psychosis. Hum. Psychopharmacol. 2018, 33. [Google Scholar] [CrossRef] [PubMed]
- Bakerman, S.; Bakerman, P.; Strausbauch, P. Bakerman’s ABC’s of Interpretive Laboratory Data, 4th ed.; Interpretive Laboratory Data, Inc.: Scottsdale, AZ, USA, 2002; p. 243. [Google Scholar]
- Leonard, A.J.; Chalmers, K.A.; Collins, C.E.; Patterson, A.J. A study of the effects of latent iron deficiency on measures of cognition: A pilot randomised controlled trial of iron supplementation in young women. Nutrients 2014, 6, 2419–2435. [Google Scholar] [CrossRef] [PubMed]
- Youdim, M.B. Brain iron deficiency and excess; cognitive impairment and neurodegeneration with involvement of striatum and hippocampus. Neurotox. Res. 2008, 14, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shachar, D.; Finberg, J.P.; Youdim, M.B. Effect of iron chelators on dopamine D2 receptors. J. Neurochem. 1985, 45, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shachar, D.; Youdim, M.B. Neuroleptic-induced supersensitivity and brain iron: I. Iron deficiency and neuroleptic-induced dopamine D2 receptor supersensitivity. J. Neurochem. 1990, 54, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Pino, J.M.V.; da Luz, M.H.M.; Antunes, H.K.M.; Giampa, S.Q.C.; Martins, V.R.; Lee, K.S. Iron-Restricted Diet Affects Brain Ferritin Levels, Dopamine Metabolism and Cellular Prion Protein in a Region-Specific Manner. Front. Mol. Neurosci. 2017, 10, 145. [Google Scholar] [CrossRef] [PubMed]
- Brunelin, J.; Fecteau, S.; Suaud-Chagny, M.F. Abnormal striatal dopamine transmission in schizophrenia. Curr. Med. Chem. 2013, 20, 397–404. [Google Scholar] [PubMed]
- Nemeth, E.; Rivera, S.; Gabayan, V.; Keller, C.; Taudorf, S.; Pedersen, B.K.; Ganz, T. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J. Clin. Investig. 2004, 113, 1271–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, A.S.; Derkits, E.J. Prenatal infection and schizophrenia: A review of epidemiologic and translational studies. Am. J. Psychiatry 2010, 167, 261–280. [Google Scholar] [CrossRef] [PubMed]
- Corwin, E.J.; Murray-Kolb, L.E.; Beard, J.L. Low hemoglobin level is a risk factor for postpartum depression. J. Nutr. 2003, 133, 4139–4142. [Google Scholar] [CrossRef] [PubMed]
- Vahdat Shariatpanaahi, M.; Vahdat Shariatpanaahi, Z.; Moshtaaghi, M.; Shahbaazi, S.H.; Abadi, A. The relationship between depression and serum ferritin level. Eur. J. Clin. Nutr. 2007, 61, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.; Hirani, V. Relationship between depressive symptoms, anemia, and iron status in older residents from a national survey population. Psychosom. Med. 2012, 74, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Shoja Shafti, S.; Jafarabad, M.S.; Azizi, R. Amelioration of deficit syndrome of schizophrenia by norepinephrine reuptake inhibitor. Ther. Adv. Psychopharmacol. 2015, 5, 263–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arango, C.; Garibaldi, G.; Marder, S.R. Pharmacological approaches to treating negative symptoms: A review of clinical trials. Schizophr. Res. 2013, 150, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Cotter, P.E.; O’Keeffe, S.T. Improvement in neuroleptic-induced akathisia with intravenous iron treatment in a patient with iron deficiency. J. Neurol. Neurosurg. Psychiatry 2007, 78, 548. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Azoulay, R.; Castellanos, F.X.; Chalard, F.; Lecendreux, M.; Chechin, D.; Delorme, R.; Sebag, G.; Sbarbati, A.; Mouren, M.C.; et al. Brain iron levels in attention-deficit/hyperactivity disorder: A pilot MRI study. World J. Biol. Psychiatry 2012, 13, 223–231. [Google Scholar] [CrossRef] [PubMed]
- House, M.J.; St Pierre, T.G.; Milward, E.A.; Bruce, D.G.; Olynyk, J.K. Relationship between brain R(2) and liver and serum iron concentrations in elderly men. Magn. Reson. Med. 2010, 63, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B.; Pretorius, E. Serum ferritin is an important inflammaroy disease marker, as it is mainly a leakage product from damaged cells. Metallomics 2014, 6, 748–773. [Google Scholar] [CrossRef] [PubMed]
- Hare, D.J.; Doecke, J.D.; Faux, N.G.; Rembach, A.; Volitakis, I.; Fowler, C.J.; Grimm, R.; Doble, P.A.; Cherny, R.A.; Masters, C.L.; et al. Decreased plasma iron in Alzheimer’s disease is due to transferrin desaturation. ACS Chem. Neurosci. 2015, 6, 398–402. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Serum Ferritin Level | Prominent Negative Symptoms | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (N = 121) | ≤20 ng/mL (N = 34, 28.1%) | >20 ng/mL (N = 87, 71.9%) | Statistical Value | p-Value | Yes (N = 31, 25.6%) | No (N = 90, 74.4%) | Statistical Value | p-Value | |
| Sociodemographic and clinical characteristics | |||||||||
| Age, Med, (IQR) year | 27.0 (22.0–32.0) | 27.5 (22.8–32.5) | 25.0 (21.0–32.0) | U = −1.270 | 0.204 | 25.0 (20.0–30.0) | 27.0 (22.0–32.5) | U = −1.403 | 0.161 |
| Sex, female; N (%) | 73 (60.3) | 33 (45.2) | 40 (54.8) | χ2 = 26.653 | <0.001 | 21 (28.8) | 52 (72.2) | χ2 = 0.957 | 0.328 |
| DUP, Med. (IQR) Mo. | 2.2 (1.0–12.0) | 4.0 (1.0–24.0) | 2.0 (1.0–11.0) | U = −0.937 | 0.349 | 8.5 (1.1–25.0) | 2.0 (1.0–7.3) | U = −2.859 | 0.004 |
| Duration of Tx, Med. (IQR) Mo. | 1.0 (0.7–1.2) | 1.0 (0.5–1.0) | 1.0 (0.8–1.5) | U = −2.512 | 0.012 | 1.0 (0.8–1.2) | 1.0 (0.6–1.2) | U = −0.102 | 0.919 |
| Inpatient status, N (%) | 71 (58.7) | 17 (23.9) | 54 (76.1) | χ2 = 1.469 | 0.226 | 12 (16.9) | 59 (83.1) | χ2 = 6.854 | 0.009 |
| Diagnosis, N (%) | χ2 = 0.240 | 0.887 | χ2 = 5.613 | 0.060 | |||||
| Schizophrenia | 77 (63.6) | 21 (27.3) | 56 (72.7) | 24 (31.2) | 53 (68.8) | ||||
| Schizophreniform | 32 (26.4) | 10 (31.3) | 22 (68.6) | 7 (21.9) | 25 (78.1) | ||||
| Other specified. | 12 (9.9) | 3 (25.0) | 9 (75.0) | 0 (0.0) | 12 (100.0) | ||||
| Antipsychotics, N (%) | χ2 = 6.843 | 0.233 | χ2 = 7.713 | 0.173 | |||||
| Amisulpride | 32 (26.4) | 8 (25.0) | 24 (75.0) | 12 (37.5) | 20 (62.5) | ||||
| Aripiprazole | 21 (17.4) | 10 (47.6) | 11 (52.4) | 2 (9.5) | 19 (90.5) | ||||
| Paliperidone | 53 (43.8) | 14 (26.4) | 39 (73.6) | 15 (28.3) | 38 (71.7) | ||||
| Risperidone | 5 (4.1) | 0 (0.0) | 5 (100.0) | 0 (0.0) | 5 (100.0) | ||||
| Quetiapine | 7 (5.8) | 1 (14.3) | 6 (85.7) | 1 (14.3) | 6 (85.7) | ||||
| None | 3 (2.5) | 1 (33.3) | 2 (66.7) | 1 (33.3) | 2 (66.7) | ||||
| Laboratory measures | |||||||||
| Hemoglobin, mean (SD) g/dL | 13.4 (1.7) | 12.5 (10.5- 13.2) | 13.9 (13.1–14.9) | t = −6.966 | <0.001 | 12.9 (2.2) | 13.6 (1.4) | t = −1.703 | 0.097 |
| Iron, Med. (IQR) μg/dL | 90 (58–115) | 51 (26–90) | 100 (67–127) | U = −4.671 | <0.001 | 73 (40–112) | 91 (61–116) | U = −1.416 | 0.157 |
| TIBC, Med. (IQR) μg/dL | 326 (291–354) | 360 (333–396) | 310 (280–340) | U = −4.994 | <0.001 | 338 (285–367) | 325 (292–350) | U = −1.146 | 0.252 |
| Transferrin Sat., mean (SD) % | 28.6 (15.6) | 16.8 (11.0) | 33.2 (14.7) | t = −5.908 | <0.001 | 25.8 (15.9) | 29.5 (15.4) | t = −1.138 | 0.257 |
| Ferritin, Med. (IQR) ng/mL | 48.7 (18.0–105.5) | 12.4 (7.6–16.0) | 86.6 (43.7–128.5) | U = −8.529 | <0.001 | 29.3 (8.8–89.2) | 64.6 (20.9–109.4) | U = −2.238 | 0.025 |
| Ferritin ≤ 20 ng/mL, N (%) | 34 (28.1) | Not applicable | 14 (41.2) | 20 (58.8) | χ2 = 6.005 | 0.014 | |||
| Psychiatric measures | |||||||||
| PANSS, Positive, mean (SD) | 16.0 (4.8) | 16.7 (4.6) | 15.7 (4.9) | t = 1.031 | 0.305 | 19.2 (3.9) | 14.8 (4.7) | t = 4.682 | <0.001 |
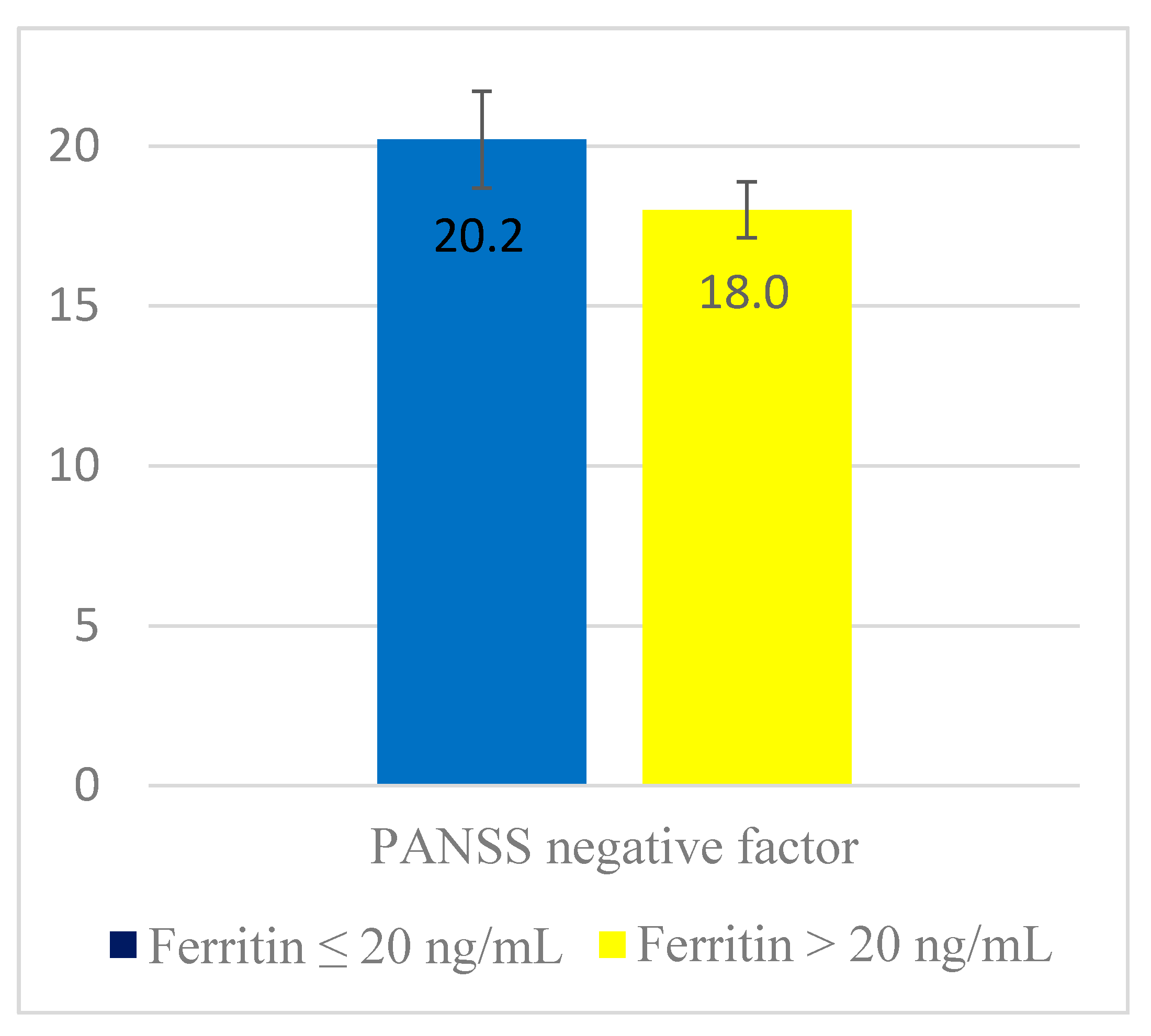
| Negative, mean (SD) | 18.6 (5.6) | 20.3 (5.8) | 18.0 (5.4) | t = 2.021 | 0.046 | 23.7 (5.6) | 16.9 (4.5) | t = 6.809 | <0.001 |
| Cognitive, mean (SD) | 14.4 (3.7) | 14.3 (3.9) | 14.5 (3.6) | t = −0.222 | 0.825 | 15.8 (3.1) | 13.9 (3.8) | t = 2.439 | 0.016 |
| Depressive, mean (SD) | 12.4 (3.7) | 12.3 (3.3) | 12.5 (3.8) | t = −0.222 | 0.825 | 14.7 (3.3) | 11.6 (3.5) | t = 6.326 | <0.001 |
| Excited, mean (SD) | 7.5 (3.0) | 7.8 (3.1) | 7.3 (3.0) | t = 0.778 | 0.438 | 8.4 (3.6) | 7.1 (2.7) | t = 1.766 | 0.085 |
| Total, mean (SD) | 68.8 (15.1) | 71.2 (15.0) | 67.8 (15.2) | t = 1.112 | 0.268 | 81.6 (12.5) | 64.3 (13.4) | t = −5.833 | <0.001 |
| Prominent negative Sx, N (%) | 31 (25.6) | 14 (45.2) | 17 (54.8) | χ2 = 6.005 | 0.014 | Not applicable | |||
| SOFAS, mean (SD) | 58.2 (10.2) | 56.9 (9.7) | 58.7 (10.4) | t = −0.872 | 0.385 | 50.4 (10.8) | 60.9 (8.5) | t = −5.550 | <0.001 |
| CDSS, mean (SD) | 4.5 (4.0) | 4.2 (3.8) | 4.6 (4.1) | t = −0.484 | 0.629 | 7.3 (4.7) | 3.6 (3.3) | t = 4.063 | <0.001 |
| Diet habit, | |||||||||
| Regular diet, mean (SD) | 17.0 (6.5) | 17.1 (6.7) | 17.0 (6.5) | t = 0.126 | 0.900 | 16.1 (6.4) | 17.3 (6.6) | t = −0.904 | 0.368 |
| Balanced diet, mean (SD) | 18.2 (6.8) | 18.7 (7.4) | 18.0 (6.6) | t = 0.490 | 0.625 | 18.2 (6.8) | 18.2 (6.9) | t = 0.016 | 0.987 |
| Healthy diet, mean (SD) | 31.8 (6.3) | 32.0 (5.6) | 31.8 (6.6) | t = 0.168 | 0.867 | 31.6 (6.0) | 31.9 (6.4) | t = −0.241 | 0.810 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-W.; Stewart, R.; Park, W.-Y.; Jhon, M.; Lee, J.-Y.; Kim, S.-Y.; Kim, J.-M.; Amminger, P.; Chung, Y.-C.; Yoon, J.-S. Latent Iron Deficiency as a Marker of Negative Symptoms in Patients with First-Episode Schizophrenia Spectrum Disorder. Nutrients 2018, 10, 1707. https://doi.org/10.3390/nu10111707
Kim S-W, Stewart R, Park W-Y, Jhon M, Lee J-Y, Kim S-Y, Kim J-M, Amminger P, Chung Y-C, Yoon J-S. Latent Iron Deficiency as a Marker of Negative Symptoms in Patients with First-Episode Schizophrenia Spectrum Disorder. Nutrients. 2018; 10(11):1707. https://doi.org/10.3390/nu10111707
Chicago/Turabian StyleKim, Sung-Wan, Robert Stewart, Woo-Young Park, Min Jhon, Ju-Yeon Lee, Seon-Young Kim, Jae-Min Kim, Paul Amminger, Young-Chul Chung, and Jin-Sang Yoon. 2018. "Latent Iron Deficiency as a Marker of Negative Symptoms in Patients with First-Episode Schizophrenia Spectrum Disorder" Nutrients 10, no. 11: 1707. https://doi.org/10.3390/nu10111707