Quality of Dietary Fat Intake and Body Weight and Obesity in a Mediterranean Population: Secondary Analyses within the PREDIMED Trial


 , ,
, ,  , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Exposure Assessment
2.3. Outcome Assessment
2.4. Assessment of Other Variables
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Substitution of Fat Subtypes
3.2.1. Body Weight Differences
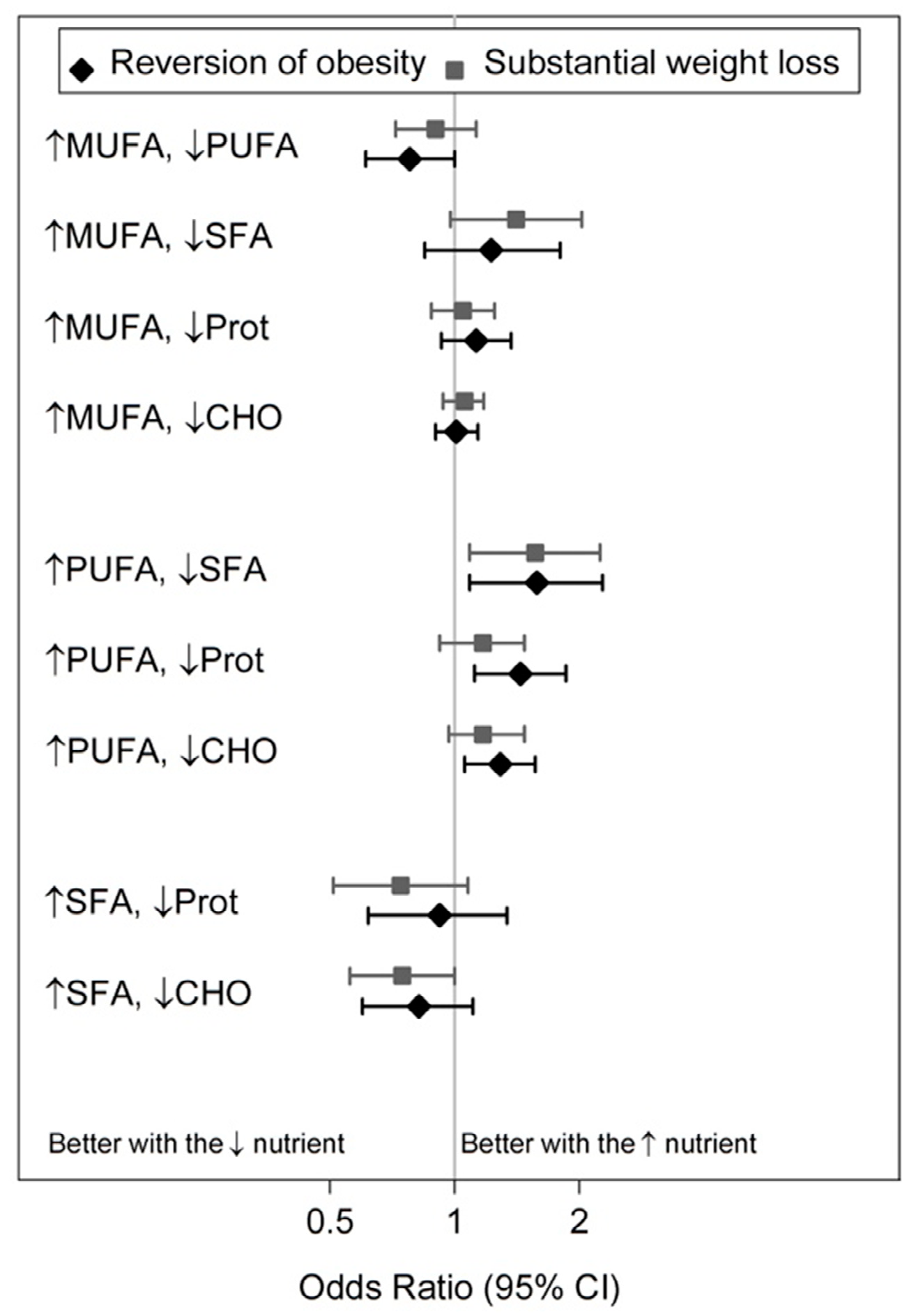
3.2.2. Obesity Incidence and Reversion, Substantial Weight Gain and Loss
3.3. Substitution of Food Items
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Factsheet Obesity and Overweight. Fact sheet N°311; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Ludwig, D.S. Lowering the bar on the low-fat diet. JAMA 2016, 316, 2087–2088. [Google Scholar] [CrossRef]
- Field, A.E.; Willett, W.C.; Lissner, L.; Colditz, G.A. Dietary fat and weight gain among women in the Nurses’ Health Study. Obesity 2007, 15, 967–976. [Google Scholar] [CrossRef]
- Liu, X.; Li, Y.; Tobias, D.K.; Wang, D.D.; Manson, J.E.; Willett, W.C.; Hu, F.B. Changes in types of dietary fats influence long-term weight change in US women and men. J. Nutr. 2018, 148, 1821–1829. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Ludwig, D.S. The 2015 US Dietary Guidelines: Lifting the Ban on Total Dietary Fat. JAMA 2015, 313, 2421–2422. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- FAO. Fats and Fatty Acids in Human Nutrition; Report of an Expert Consultation; FAO: Rome, Italy, 2010; Volume 91, pp. 1–166. ISBN 978-92-5-106733-8. [Google Scholar]
- Schwab, U.; Lauritzen, L.; Tholstrup, T.; Haldorsson, T.I.; Riserus, U.; Uusitupa, M.; Becker, W. Effect of the amount and type of dietary fat on cardiometabolic risk factors and risk of developing type 2 diabetes, cardiovascular diseases, and cancer: A systematic review. Food Nutr. Res. 2014, 58, 25145. [Google Scholar] [CrossRef] [PubMed]
- Ros, E.; Martínez-González, M.A.; Estruch, R.; Salas-Salvadó, J.; Fitó, M.; Martínez, J.A.; Corella, D. Mediterranean diet and cardiovascular health: Teachings of the PREDIMED study. Adv. Nutr. 2014, 5, 330S–336S. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Babio, N.; Martínez-González, M.A.; Corella, D.; Ros, E.; Martín-Peláez, S.; Estruch, R.; Arós, F.; Gómez-Gracia, E.; Fiol, M.; et al. Dietary fat intake and risk of cardiovascular disease and all-cause mortality in a population at high risk of cardiovascular disease. Am. J. Clin. Nutr. 2015, 102, 1563–1573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet and weight loss: Meta-analysis of randomized controlled trials. Metab. Syndr. Relat. Disord. 2011, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mancini, J.G.; Filion, K.B.; Atallah, R.; Eisenberg, M.J. Systematic Review of the Mediterranean Diet for Long-Term Weight Loss. Am. J. Med. 2016, 129, 407–415.e4. [Google Scholar] [CrossRef]
- Tobias, D.K.; Chen, M.; Manson, J.E.; Ludwig, D.S.; Willett, W.; Hu, F.B. Effect of low-fat diet interventions versus other diet interventions on long-term weight change in adults: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2015, 3, 968–979. [Google Scholar] [CrossRef]
- Fernández-Montero, A.; Bes-Rastrollo, M.; Barrio-López, M.T.; de la Fuente-Arrillaga, C.; Salas-Salvadó, J.; Moreno-Galarraga, L.; Martínez-González, M.A. Nut consumption and 5-y all-cause mortality in a Mediterranean cohort: The SUN project. Nutrition 2014, 30, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Bes-Rastrollo, M. Nut consumption, weight gain and obesity: Epidemiological evidence. Nutr. Metab. Cardiovasc. Dis. 2011, 21 (Suppl. 1), S40–S45. [Google Scholar] [CrossRef]
- Jackson, C.L.; Hu, F.B. Long-term associations of nut consumption with body weight and obesity. Am. J. Clin. Nutr. 2014, 100 (Suppl. 1), 408S–411S. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Covas, M.I.; Fiol, M.; Wärnberg, J.; Arós, F.; Ruíz-Gutiérrez, V.; Lamuela-Raventós, R.M.; et al. Cohort profile: Design and methods of the PREDIMED study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef]
- Willett, W.C. Issues in analysis and presentation of dietary data. In Nutritional Epidemiology, 3rd ed.; Willett, W.C., Ed.; Oxford University Press: New York, NY, USA, 2012; pp. 321–346. ISBN 9780199754038. [Google Scholar]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 9th ed.; Pirámide: Madrid, Spain, 2005; ISBN 978-84-368-3947-0. [Google Scholar]
- Hu, F.B.; Stampfer, M.J.; Manson, J.E.; Rimm, E.; Colditz, G.A.; Rosner, B.A.; Hennekens, C.H.; Willett, W.C. Dietary fat intake and the risk of coronary heart disease in women. N. Engl. J. Med. 1997, 337, 1491–1499. [Google Scholar] [CrossRef] [PubMed]
- Wing, R.R.; Hill, J.O. Successful weight loss maintenance. Annu. Rev. Nutr. 2001, 21, 323–341. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish men. The MARATHOM Investigators. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Garcia, M.; Aguilar, A.; Molina, L.; Covas, M.I.; Marrugat, J. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish Women. Investigators of the MARATDON Group. Med. Sci. Sports Exerc. 2000, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Groenwold, R.H.; Donders, A.R.; Roes, K.C.; Harrell, F.E.; Moons, K.G. Dealing with missing outcome data in randomized trials and observational studies. Am. J. Epidemiol. 2012, 175, 210–217. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; O’Keefe, J.H. Good Fats versus Bad Fats: A Comparison of Fatty Acids in the Promotion of Insulin Resistance, Inflammation, and Obesity. Mo. Med. 2017, 114, 303–307. [Google Scholar]
- Hannon, B.A.; Thompson, S.V.; An, R.; Teran-Garcia, M. Clinical Outcomes of Dietary Replacement of Saturated Fatty Acids with Unsaturated Fat Sources in Adults with Overweight and Obesity: A Systematic Review and Meta-Analysis of Randomized Control Trials. Ann. Nutr. Metab. 2017, 71, 107–117. [Google Scholar] [CrossRef] [Green Version]
- González, C.A.; Pera, G.; Quirós, J.R.; Lasheras, C.; Tormo, M.J.; Rodriguez, M.; Navarro, C.; Martinez, C.; Dorronsoro, M.; Chirlaque, M.D.; et al. Types of fat intake and body mass index in a Mediterranean country. Public Health Nutr. 2000, 3, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Romaguera, D.; Norat, T.; Vergnaud, A.C.; Mouw, T.; May, A.M.; Agudo, A.; Buckland, G.; Slimani, N.; Rinaldi, S.; Couto, E.; et al. Mediterranean dietary patterns and prospective weight change in participants of the EPIC-PANACEA project. Am. J. Clin. Nutr. 2010, 92, 912–921. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Chiva-Blanch, G.; Fiol, M.; Gómez-Gracia, E.; Arós, F.; Lapetra, J.; et al. Effect of a high-fat Mediterranean diet on bodyweight and waist circumference: A prespecified secondary outcome analysis of the PREDIMED randomised controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 666–676. [Google Scholar] [CrossRef]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martínez-González, M.A.; Castañer, O.; Bulló, M.; Corella, D.; Arós, F.; Gómez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. CMAJ 2014, 186, E649–E657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babio, N.; Becerra-Tomás, N.; Martínez-González, M.; Corella, D.; Estruch, R.; Ros, E.; Sayón-Orea, C.; Fitó, M.; Serra-Majem, L.; Arós, F.; et al. Consumption of Yogurt, Low-Fat Milk, and Other Low-Fat Dairy Products Is Associated with Lower Risk of Metabolic Syndrome Incidence in an Elderly Mediterranean Population. J. Nutr. 2015, 145, 2308–2316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guasch-Ferré, M.; Bulló, M.; Martínez-González, M.A.; Ros, E.; Corella, D.; Estruch, R.; Fitó, M.; Arós, F.; Wärnberg, J.; Fiol, M.; et al. Frequency of nut consumption and mortality risk in the PREDIMED nutrition intervention trial. BMC Med. 2013, 11, 164. [Google Scholar] [CrossRef]
- Flores-Mateo, G.; Rojas-Rueda, D.; Basora, J.; Ros, E.; Salas-Salvadó, J. Nut intake and adiposity: Meta-analysis of clinical trials. Am. J. Clin. Nutr. 2013, 97, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Bes-Rastrollo, M.; Román-Viñas, B.; Pfrimer, K.; Sánchez-Villegas, A.; Martínez-González, M.A. Dietary patterns and nutritional adequacy in a Mediterranean country. Br. J. Nutr. 2009, 101 (Suppl. 2), S21–S28. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Tainta, A.; Zazpe, I.; Bes-Rastrollo, M.; Salas-Salvadó, J.; Bullo, M.; Sorlí, J.V.; Corella, D.; Covas, M.I.; Arós, F.; Gutierrez-Bedmar, M.; et al. Nutritional adequacy according to carbohydrates and fat quality. Eur. J. Nutr. 2016, 55, 93–106. [Google Scholar] [CrossRef]
- Smith, J.D.; Hou, T.; Ludwig, D.S.; Rimm, E.B.; Willett, W.; Hu, F.B.; Mozaffarian, D. Changes in intake of protein foods, carbohydrate amount and quality, and long-term weight change: Results from 3 prospective cohorts. Am. J. Clin. Nutr. 2015, 101, 1216–1224. [Google Scholar] [CrossRef]
- Casas-Agustench, P.; López-Uriarte, P.; Bulló, M.; Ros, E.; Gómez-Flores, A.; Salas-Salvadó, J. Acute effects of three high-fat meals with different fat saturations on energy expenditure, substrate oxidation and satiety. Clin. Nutr. 2009, 28, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Camargo, A.; Meneses, M.E.; Perez-Martinez, P.; Delgado-Lista, J.; Jimenez-Gomez, Y.; Cruz-Teno, C.; Tinahones, F.J.; Paniagua, J.A.; Perez-Jimenez, F.; Roche, H.M.; et al. Dietary fat differentially influences the lipids storage on the adipose tissue in metabolic syndrome patients. Eur. J. Nutr. 2014, 53, 617–626. [Google Scholar] [CrossRef]
- Hermsdorff, H.H.; Zulet, M.Á.; Abete, I.; Martínez, J.A. Discriminated benefits of a Mediterranean dietary pattern within a hypocaloric diet program on plasma RBP4 concentrations and other inflammatory markers in obese subjects. Endocrine 2009, 36, 445–451. [Google Scholar] [CrossRef]
- Martínez-Fernández, L.; Laiglesia, L.M.; Huerta, A.E.; Martínez, J.A.; Moreno-Aliaga, M.J. Omega-3 fatty acids and adipose tissue function in obesity and metabolic syndrome. Prostaglandins Other Lipid Mediat. 2015, 121, 24–41. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.M.; Kesse-Guyot, E.; McManus, R.; Hercberg, S.; Lairon, D.; Planells, R.; Roche, H.M. High dietary saturated fat intake accentuates obesity risk associated with the fat mass and obesity-associated gene in adults. J. Nutr. 2012, 142, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Wehling, H.; Lusher, J. People with a body mass index ≥30 under-report their dietary intake: A systematic review. J. Health Psychol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Verweij, L.M.; Terwee, C.B.; Proper, K.I.; Hulshof, C.T.; van Mechelen, W. Measurement error of waist circumference: Gaps in knowledge. Public Health Nutr. 2013, 16, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Obesity Epidemiology; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Vittinghoff, E.; Glidden, D.V.; Shiboski, S.C.; McCulloch, C.E. Regression Methods in Biostatistics: Linear, Logistic, Survival, and Repeated Measures Models, 2nd ed.; Springer: Boston, MA, USA, 2012; ISBN 978-1-4614-1352-3. [Google Scholar]
- Harika, R.K.; Eilander, A.; Alssema, M.; Osendarp, S.J.; Zock, P.L. Intake of fatty acids in general populations worldwide does not meet dietary recommendations to prevent coronary heart disease: A systematic review of data from 40 countries. Ann. Nutr. Metab. 2013, 63, 229–238. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Q1 | Q5 | |
|---|---|---|
| Participants, n | 1391 | 1387 |
| Age (year) | 67 (6) | 67 (6) |
| Women (%) | 53.9 | 62.5 |
| Control group (%) | 35.6 | 32.2 |
| Physical activity (MET-min/week) | 249 (259) | 216 (226) |
| Smoking habit: Never smoker (%) | 61.0 | 64.4 |
| Smoking habit: Former smoker (%) | 24.4 | 22.4 |
| Smoking habit: Current smoker (%) | 14.6 | 13.2 |
| Marital status: Married (%) | 75.0 | 76.5 |
| Marital status: Single/widowed (%) | 25.0 | 23.5 |
| Educational level: Lower than high school (%) | 80.5 | 75.3 |
| Educational level: High school (%) | 11.9 | 17.7 |
| Educational level: University (%) | 7.6 | 7.0 |
| Employment status: Employed/housewife | 41.6 | 51.8 |
| Employment status: Unemployed (%) | 3.5 | 3.5 |
| Employment status: Retired (%) | 54.9 | 44.7 |
| Total energy intake (kcal/day) | 2262 (573) | 2163 (513) |
| Carbohydrates (EN%) | 51.6 (5.8) | 35.1 (4.5) |
| Protein (EN%) | 17.4 (3.1) | 16.7 (2.8) |
| Total fat (EN%) | 27.7 (3.2) | 46.5 (3.7) |
| MUFAs (EN%) | 14.4 (2.4) | 26.3 (3.4) |
| PUFAs (EN%) | 5.0 (1.6) | 7.9 (2.4) |
| SFAs (EN%) | 8.1 (1.7) | 12.1 (2.1) |
| trans fat (EN%) | 0.18 (0.12) | 0.28 (0.17) |
| Alcohol (g/day) | 11.2 (18.7) | 5.1 (9.2) |
| Dietary fiber (g/day) | 28.9 (10.1) | 21.7 (6.6) |
| Substitution | ↑MUFA | ↑PUFA | ↑SFA |
|---|---|---|---|
| ↓PUFA | 0.13 (−0.09, 0.34) | - | - |
| ↓SFA | −0.38 (−0.69, −0.07) * | −0.51 (−0.81, −0.20) * | - |
| ↓proteins | −0.14 (−0.30, 0.02) | −0.27 (−0.49, −0.04) * | 0.24 (−0.08, 0.56) |
| ↓carbohydrates | −0.07 (−0.17, 0.03) | −0.20 (−0.37, −0.02) * | 0.31 (0.06, 0.56) * |
| Substitution | Obesity Incidence | Weight Gain (≥10%) |
|---|---|---|
| ↑MUFA, ↓PUFA | 1.36 (1.02, 1.81) * | 1.16 (0.82, 1.65) |
| ↑MUFA, ↓SFA | 1.04 (0.69, 1.56) | 1.11 (0.71, 1.65) |
| ↑MUFA, ↓Proteins | 0.85 (0.69, 1.03) | 0.82 (0.66, 1.02) |
| ↑MUFA, ↓Carbohydrates | 1.08 (0.95, 1.23) | 1.02 (0.87, 1.18) |
| ↑PUFA, ↓SFA | 0.77 (0.51, 1.15) | 0.96 (0.62, 1.47) |
| ↑PUFA, ↓Proteins | 0.62 (0.47, 0.83) * | 0.70 (0.50, 0.99) * |
| ↑PUFA, ↓Carbohydrates | 0.80 (0.63, 1.01) | 0.87 (0.67, 1.15) |
| ↑SFA, ↓Proteins | 0.81 (0.53, 1.24) | 0.73 (0.46, 1.17) |
| ↑SFA, ↓Carbohydrates | 1.04 (0.75, 1.24) | 0.91 (0.63, 1.31) |
| Substitution | Mean Body Weight (kg) Difference (95% Confidence Interval) |
|---|---|
| ↓Red meat, ↑White meat | −0.64 (−0.94, −0.35) * |
| ↓Red meat, ↑Oily fish | −0.75 (−1.13, −0.38) * |
| ↓Red meat, ↑White fish | −0.87 (−1.17, −0.56) * |
| ↓Butter, ↑Olive oil | −0.25 (−0.56, 0.06) |
| ↓Butter, ↑Other vegetable oils | −0.11 (−0.44, 0.22) |
| ↓Margarine, ↑Olive oil | 0.04 (−0.18, 0.25) |
| ↓Margarine, ↑Other vegetable oils | 0.26 (0.02, 0.50) * |
| ↓Mixed nuts, ↑Walnuts | −0.15 (−0.61, 0.32) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beulen, Y.; Martínez-González, M.A.; Van de Rest, O.; Salas-Salvadó, J.; Sorlí, J.V.; Gómez-Gracia, E.; Fiol, M.; Estruch, R.; Santos-Lozano, J.M.; Schröder, H.; et al. Quality of Dietary Fat Intake and Body Weight and Obesity in a Mediterranean Population: Secondary Analyses within the PREDIMED Trial. Nutrients 2018, 10, 2011. https://doi.org/10.3390/nu10122011
Beulen Y, Martínez-González MA, Van de Rest O, Salas-Salvadó J, Sorlí JV, Gómez-Gracia E, Fiol M, Estruch R, Santos-Lozano JM, Schröder H, et al. Quality of Dietary Fat Intake and Body Weight and Obesity in a Mediterranean Population: Secondary Analyses within the PREDIMED Trial. Nutrients. 2018; 10(12):2011. https://doi.org/10.3390/nu10122011
Chicago/Turabian StyleBeulen, Yvette, Miguel A. Martínez-González, Ondine Van de Rest, Jordi Salas-Salvadó, José V. Sorlí, Enrique Gómez-Gracia, Miquel Fiol, Ramón Estruch, José M. Santos-Lozano, Helmut Schröder, and et al. 2018. "Quality of Dietary Fat Intake and Body Weight and Obesity in a Mediterranean Population: Secondary Analyses within the PREDIMED Trial" Nutrients 10, no. 12: 2011. https://doi.org/10.3390/nu10122011