Types of Carbohydrates Intake during Pregnancy and Frequency of a Small for Gestational Age Newborn: A Case-Control Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
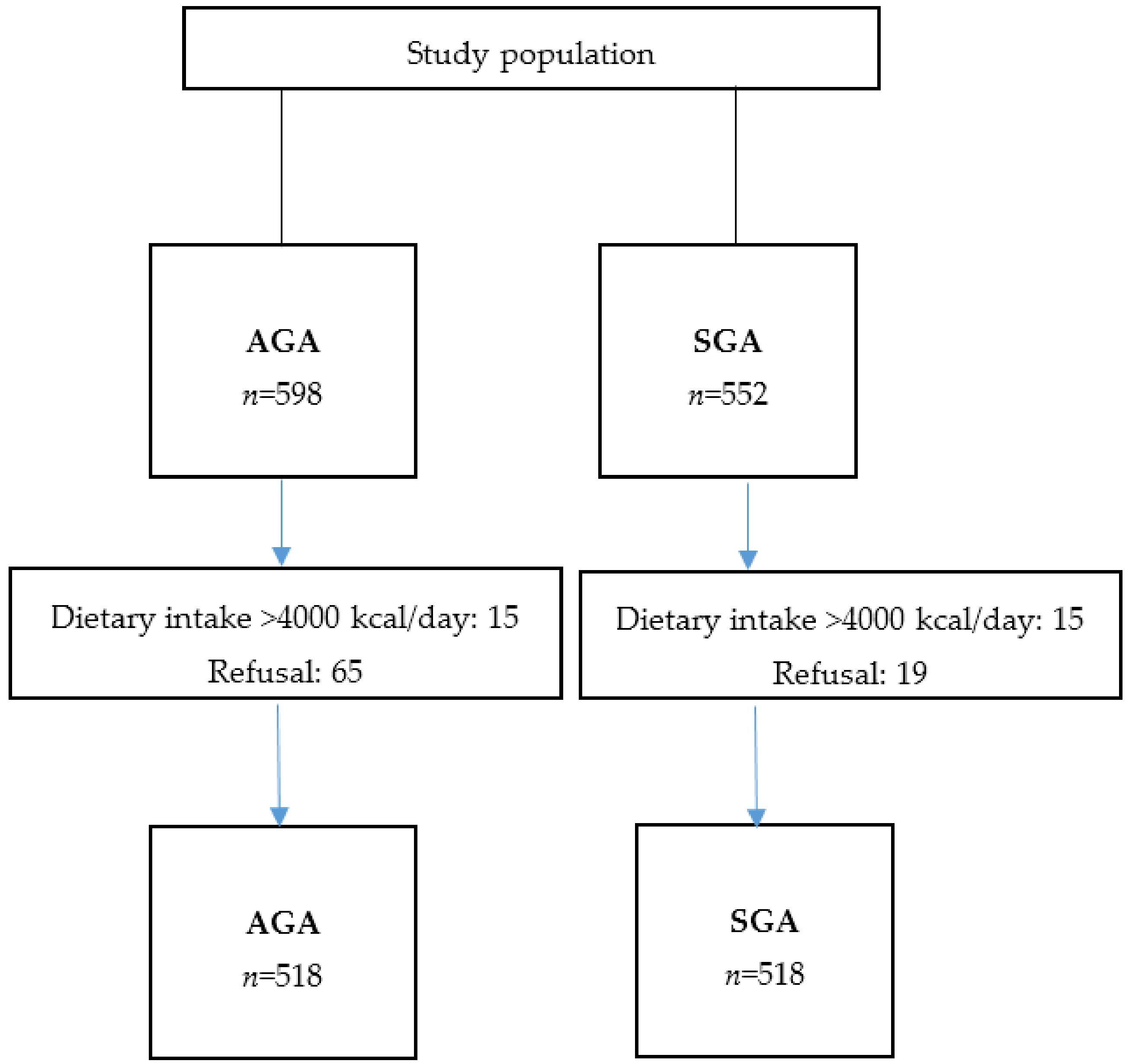
2.1. SGA Group
2.2. Control Group
2.3. Data Collection
2.4. Dietary Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schlaudecker, E.P.; Munoz, F.M.; Bardají, A.; Boghossian, N.S.; Khalil, A.; Mousa, H.; Nesin, M.; Nisar, M.I.; Pool, V.; Spiegel, H.M.; et al. Small for gestational age: Case definition & guidelines for data collection, analysis, and presentation of maternal immunisation safety data. Vaccine 2017, 35, 6518–6528. [Google Scholar] [PubMed]
- Lee, A.C.; Kozuki, N.; Cousens, S.; Stevens, G.A.; Blencowe, H.; Silveira, M.F.; Sania, A.; Rosen, H.E.; Schmiegelow, C.; Adair, L.S.; et al. Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21(st) standard: Analysis of CHERG datasets. BMJ 2017, 358, j3677. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, E.A.; Robinson, E.; Clark, P.M.; Becroft, D.M.O.; Glavish, N.; Pattison, N.S.; Pryor, J.E.; Thompson, J.M.D.; Wild, C.J. Maternal nutritional risk factors for small for gestational age babies in a developed country: A case-control study. Arch. Dis Child. Fetal Neonatal Ed. 2004, 89, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Emond, J.A.; Karagas, M.R.; Baker, E.R.; Gilbert-Diamond, D. Better diet quality during pregnancy is associated with a reduced likelihood of an infant born small for gestational age: An analysis of the prospective New Hampshire birth cohort study. J. Nutr. 2018, 148, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Galiano, J.M.; Olmedo-Requena, R.; Barrios-Rodríguez, R.; Amezcua-Prieto, C.; Bueno-Cavanillas, A.; Salcedo-Bellido, I.; Jimenez-Moleon, J.J.; Delgado-Rodríguez, M. Effect of adherence to a Mediterranean diet and olive oil intake during pregnancy on risk of small for gestational age infants. Nutrients 2018, 10, 1234. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Dietary Reference Values for Nutrients Summary Report. 2017. Available online: https://doi.org/10.2903/sp.efsa.2017.e15121 (accessed on 6 November 2018).
- Bartrina, J.A. Guías alimentarias para la población española (SENC, 2016); la nueva pirámide de la alimentación saludable. Nutr. Hosp. 2016, 33, 1–48. [Google Scholar]
- British Nutrition Foundation. Carbohydrates. Available online: https://www.nutrition.org.uk/healthyliving/healthydiet/starchyfoods.html (accessed on 6 November 2018).
- Fardet, A. New hypotheses for the health-protective mechanisms of whole-grain cereals: What is beyond fibre? Nutr. Res. Rev. 2010, 23, 65–134. [Google Scholar] [CrossRef] [PubMed]
- Robson, A.A. Preventing diet induced disease: Bioavailable nutrient-rich, low-energy-dense diets. Nutr. Health 2009, 20, 135–166. [Google Scholar] [CrossRef] [PubMed]
- Goletzke, J.; Buyken, A.E.; Louie, J.C.; Moses, R.G.; Brand-Miller, J.C. Dietary micronutrient intake during pregnancy is a function of carbohydrate quality. Am. J. Clin. Nutr. 2015, 102, 626–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, J.M.; McGowan, C.A.; Mahony, R.; Foley, M.E.; McAuliffe, F.M. Low glycaemic index diet in pregnancy to prevent macrosomia (ROLO study): Randomised control trial. BMJ 2012, 345, e5605. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary patterns during pregnancy are associated with risk of gestational diabetes mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef] [PubMed]
- Lenders, C.M.; Hediger, M.L.; Scholl, T.O.; Khoo, C.-S.; Slap, G.B.; Stallings, V.A. Effect of high-sugar intake by low-income pregnant adolescents on infant birth weight. J. Adolesc. Health 1994, 15, 596–602. [Google Scholar] [CrossRef]
- Grundt, J.H.; Eide, G.E.; Brantsæter, A.L.; Haugen, M.; Markestad, T. Is consumption of sugar-sweetened soft drinks during pregnancy associated with birth weight? Matern. Child Nutr. 2017, 13, 12405. [Google Scholar] [CrossRef] [PubMed]
- Crume, T.L.; Brinton, J.T.; Shapiro, A.; Kaar, J.; Glueck, D.H.; Siega-Riz, A.M.; Dabelea, D. Maternal dietary intake during pregnancy and offspring body composition: The Healthy Start Study. Am. J. Obstet. Gynecol. 2016, 215, 609–e1. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A.; Thomas, T.; Bosch, R.J.; Dwarkanath, P.; Thomas, A.; Duggan, C.P.; Kurpad, A.V. Fetal sex modifies the effect of maternal macronutrient intake on the incidence of small-for-gestational-age births: A prospective observational cohort study. Am. J. Clin. Nutr. 2018, 108, 814–820. [Google Scholar] [PubMed]
- Shapiro, A.L.; Kaar, J.L.; Crume, T.L.; Starling, A.P.; Siega-Riz, A.M.; Ringham, B.M.; Glueck, D.H.; Norris, J.M.; Barbour, L.A.; Friedman, J.E.; et al. Maternal diet quality in pregnancy and neonatal adiposity: The Healthy Start Study. Int. J. Obes. 2016, 40, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.S.; Greenwood, D.C.; Simpson, N.A.B.; Cade, J.E. Is dietary macronutrient composition during pregnancy associated with offspring birth weight? An observational study. Br. J. Nutr. 2018, 119, 330–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricci, E.; Chiaffarino, F.; Cipriani, S.; Malvezzi, M.; Parazzini, F. Diet in pregnancy and risk of small for gestational age birth: Results from a retrospective case-control study in Italy. Matern. Child Nutr. 2010, 6, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Beltrán, P.D.; Marcos, J.C.M.; Gómez, J.R.-A.; Uribe, A.L.; Del Rey, L.F.-L.; Cortés, M.J.B.; Bengoa, I.O.; Dúo, G.A. [The fetal development curves of newborn infants in the Hospital de Cruces (Vizcaya). I. Weight]. An. Esp. Pediatr. 1996, 44, 50–54. [Google Scholar]
- Alvarez-Dardet, C.; Alonso, J.; Domingo, A.; Poyatos, E.R. La medición de la clase social en Ciencias de la Salud: informe de un grupo de trabajo de la Sociedad Española de Epidemiología; SG. Editores S.A.: Barcelona, Spain; Sociedad Española de Epidemiología, 1995. [Google Scholar]
- Kessner, D.M.; Kalk, C.E.; Singer, J. Assessing Health Quality-the Case for Tracers. N. Engl. J. Med. 1973, 288, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.; Ángel Salas-Salvadó, J.; Martín-Moreno, J.M.; et al. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mataix Verdú, J. Tabla de composición de alimentos españoles (Food Composition Tables), 4th ed.; Universidad de Granada: Granada, Spain, 2003. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Spanish Food Composition Tables (Tablas de composición de alimentos), 7th ed.; Pirámide: Madrid, Spain, 2003. [Google Scholar]
- Willett, W.; Stampfer, M.J. Total energy intake: implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-W.; Tint, M.-T.; Fortier, M.V.; Aris, I.M.; Bernard, J.Y.; Colega, M.; Gluckman, P.D.; Saw, S.-M.; Chong, Y.-S.; Yap, F.; et al. Maternal macronutrient intake during pregnancy is associated with neonatal abdominal adiposity: The growing up in Singapore towards healthy outcomes (GUSTO) Study. J. Nutr. 2016, 146, 1571–1579. [Google Scholar] [CrossRef] [PubMed]
- Muirhead, R.; Kizirian, N.V.; Markovic, T.P.; Brodie, S.; Garnett, S.P.; Louie, J.C.Y.; Petocz, P.; Ross, G.P.; Brand-Miller, J.C. Macronutrient balance and dietary glycemic index in pregnancy predict neonatal body composition. Nutrients 2016, 8, 270. [Google Scholar]
- Beardsall, K.; Diderholm, B.M.; Dunger, D.B. Insulin and carbohydrate metabolism. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.; Robinson, S.; Barker, D.; Osmond, C.; Cox, V. Maternal nutrition in early and late pregnancy in relation to placental and fetal growth. BMJ 1996, 312, 410. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Cases n (%) | Controls n (%) | p-Value |
|---|---|---|---|
| Marital status | 0.036 | ||
| Single | 37 (7.1) | 42 (8.1) | |
| Stable couple | 161 (31.1) | 124 (23.9) | |
| Married | 320 (61.8) | 352 (68.0) | |
| Education level | 0.084 | ||
| Primary | 112 (21.6) | 93 (17.9) | |
| High school, not ended | 42 (8.1) | 28 (5.4) | |
| High school | 185 (35.7) | 190 (36.7) | |
| University | 179 (34.6) | 207 (40.0) | |
| Parity | 0.080 | ||
| Primiparous women | 331 (63.9) | 298 (57.5) | |
| Secundiparous women | 147 (28.4) | 180 (34.8) | |
| Multiparous women (≥2 previous children) | 40 (7.7) | 40 (7.7) | |
| Previous preterm or low-birthweight newborn | 64 (12.4) | 26 (5.0) | < 0.001 |
| Kessner index (prenatal care) | 0.737 | ||
| Adequate | 259 (50.0) | 253 (48.8) | |
| Intermediate | 185 (35.7) | 182 (35.2) | |
| Inadequate | 74 (14.3) | 83 (16.0) | |
| Smoking during pregnancy | 149 (28.8) | 80 (15.4) | < 0.001 |
| Preeclampsia | 46 (8.9) | 11 (2.1) | < 0.001 |
| Intrauterine growth retardation | 141 (27.2) | 8 (1.5) | < 0.001 |
| Weight gain during pregnancy (g/week), mean (SD) | 278 (121) | 310 (114) | < 0.001 |
| Pre-pregnancy body mass index, mean (SD) | 23.1 (4.5) | 23.9 (4.1) | < 0.001 |
| Alcohol intake (g/week), mean (SD) | 4.2 (18.5) | 3.1 (15.2) | 0.312 |
| Intakes (g) and Frequency | Cases n (%) | Controls n (%) | cOR (95% CI) | aOR 1 (95% CI) |
|---|---|---|---|---|
| White bread (75 g) | ||||
| Never | 126 (24.3) | 145 (28.0) | 1 (ref.) | 1 (ref.) |
| vs. 2+ a day | 83 (16.0) | 76 (14.7) | 1.27 (0.85–1.89) | 1.19 (0.78–1.81) |
| Whole wheat bread (75 g) | ||||
| Never | 333 (64.3) | 278 (53.7) | 1 (ref.) | 1 (ref.) |
| vs. 1+ a day | 60 (11.6) | 80 (15.4) | 0.60 (0.41–0.88) | 0.64 (0.43–0.96) |
| Cereals (30 g) | ||||
| Never | 356 (68.7) | 341 (65.8) | 1 (ref.) | 1 (ref.) |
| vs. 2+ a week | 72 (13.9) | 88 (17.0) | 0.78 (0.55–1.11) | 0.70 (0.48–1.03) |
| Wholegrain cereals (30 g) | ||||
| Never | 341 (65.8) | 321 (62.0) | 1 (ref.) | 1 (ref.) |
| vs. 2+ a week | 67 (12.9) | 77 (14.9) | 0.81 (0.56–1.18) | 0.88 (0.59–1.31) |
| Rice (60 g in raw) | ||||
| Never | 76 (14.7) | 78 (15.1) | 1 (ref.) | 1 (ref.) |
| vs. 2+ a week | 36 (7.0) | 46 (8.9) | 0.82 (0.49–1.38) | 1.00 (0.57–1.76) |
| Pasta (60 g in raw) | ||||
| ≤1–3 a month | 50 (9.7) | 45 (8.7) | 1 (ref.) | 1 (ref.) |
| vs 2+ a week | 95 (18.3) | 116 (22.4) | 0.72 (0.44–1.18) | 0.80 (0.47–1.37) |
| Pizza (1 portion of 200g) | ||||
| ≤ 1–3 a month | 210 (40.5) | 230 (44.4) | 1 (ref.) | 1 (ref.) |
| vs. 1+ a week | 308 (59.5) | 288 (55.6) | 1.18 (0.92–1.51) | 1.14 (0.87–1.48) |
| Quintiles Intake (g/day) | Cases n (%) | Controls n (%) | cOR (95% CI) | aOR 1 (95% CI) |
|---|---|---|---|---|
| Total amount of cereals | ||||
| Q1 (≤117.57) | 115 (22.2) | 104 (20.1) | 1 (ref.) | 1 (ref.) |
| Q2 (117.58–154.63) | 75 (14.5) | 104 (20.1) | 0.65 (0.43–0.97) | 0.68 (0.44–1.05) |
| Q3 (154.64–189.96) | 99 (19.1) | 103 (19.9) | 0.89 (0.61–1.31) | 0.93 (0.62–1.40) |
| Q4 (189.97–239.01) | 130 (25.1) | 104 (20.1) | 1.17 (0.79–1.73) | 1.14 (0.76–1.73) |
| Q5 (>239.01) | 99 (19.1) | 103 (19.9) | 0.89 (0.60–1.32) | 0.84 (0.55–1.29) |
| Total amount of wholegrain cereal and bread | ||||
| Q1 (≤0.10) | 154 (29.7) | 104 (20.1) | 1 (ref.) | 1 (ref.) |
| Q2 (0.11–2.08) | 105 (20.3) | 104 (20.1) | 0.67 (0.45–0.99) | 0.80 (0.53–1.21) |
| Q3 (2.09–10.56) | 90 (17.4) | 103 (19.9) | 0.56 (0.37–0.83) | 0.60 (0.39–0.91) |
| Q4 (10.57–45.61) | 84 (16.2) | 104 (20.1) | 0.54 (0.37–0.80) | 0.54 (0.35–0.81) |
| Q5 (>45.61) | 85 (16.4) | 103 (19.9) | 0.54 (0.37–0.80) | 0.59 (0.39–0.91) |
| Total amount of white cereals + rice & pasta | ||||
| Q1 (≤ 27.65) | 117 (22.6) | 104 (20.1) | 1 (ref.) | 1 (ref.) |
| Q2 (27.66–51.53) | 97 (18.7) | 104 (20.1) | 0.85 (0.58–1.23) | 0.86 (0.58–1.30) |
| Q3 (51.54–79.10) | 100 (19.3) | 103 (19.9) | 0.88 (0.61–1.26) | 0.88 (0.60–1.30) |
| Q4 (79.11–120.79) | 93 (18.0) | 104 (20.1) | 0.80 (0.54–1.19) | 0.88 (0.58–1.34) |
| Q5 (>120.79) | 111 (21.4) | 103 (19.9) | 0.95 (0.65–1.41) | 0.95 (0.63–1.43) |
| Frequency of Intake | Cases n (%) | Controls n (%) | cOR (95% CI) | aOR 1 (95% CI) |
|---|---|---|---|---|
| Industriall bakery and pastries (1 unit/50 g) | ||||
| Never | 158 (30.5) | 174 (33.6) | 1 (ref.) | 1 (ref.) |
| vs. 2+ a week | 74 (14.3) | 57 (11.0) | 1.44 (0.95–2.17) | 1.59 (1.02–2.48) |
| Doughnuts (1 unit) | ||||
| Never | 238 (46.0) | 263 (50.8) | 1 (ref.) | 1 (ref.) |
| vs. 2+ a week | 27 (5.2) | 12 (2.3) | 2.42 (1.21–4.84) | 2.10 (1.02–4.29) |
| Industrial muffins (1–2 units) | ||||
| Never | 159 (30.7) | 196 (37.8) | 1 (ref.) | 1 (ref.) |
| vs. 2+ a week | 56 (10.8) | 43 (8.3) | 1.61 (1.03–2.55) | 1.63 (0.99–2.66) |
| Industrial sweets (bakery and pastries, doughnuts, muffins) | ||||
| Never | 63 (12.4) | 92 (18.2) | 1 (ref.) | 1 (ref.) |
| 1–3 a month | 64 (12.6) | 66 (13.0) | 1.41 (0.85–2.32) | 1.59 (0.93–2.71) |
| 1 a week | 156 (30.7) | 169 (33.4) | 1.37 (0.91–2.08) | 1.54 (0.99–2.39) |
| 2–6 a week | 186 (36.5) | 155 (30.6) | 1.73 (1.15–2.58) | 1.84 (1.20–2.82) |
| 1+ a day | 40 (6.9) | 24 (4.7) | 2.36 (1.29–4.35) | 2.70 (1.42–5.13) |
| p for trend | 0.002 | 0.002 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amezcua-Prieto, C.; Martínez-Galiano, J.M.; Cano-Ibáñez, N.; Olmedo-Requena, R.; Bueno-Cavanillas, A.; Delgado-Rodríguez, M. Types of Carbohydrates Intake during Pregnancy and Frequency of a Small for Gestational Age Newborn: A Case-Control Study. Nutrients 2019, 11, 523. https://doi.org/10.3390/nu11030523
Amezcua-Prieto C, Martínez-Galiano JM, Cano-Ibáñez N, Olmedo-Requena R, Bueno-Cavanillas A, Delgado-Rodríguez M. Types of Carbohydrates Intake during Pregnancy and Frequency of a Small for Gestational Age Newborn: A Case-Control Study. Nutrients. 2019; 11(3):523. https://doi.org/10.3390/nu11030523
Chicago/Turabian StyleAmezcua-Prieto, Carmen, Juan Miguel Martínez-Galiano, Naomi Cano-Ibáñez, Rocío Olmedo-Requena, Aurora Bueno-Cavanillas, and Miguel Delgado-Rodríguez. 2019. "Types of Carbohydrates Intake during Pregnancy and Frequency of a Small for Gestational Age Newborn: A Case-Control Study" Nutrients 11, no. 3: 523. https://doi.org/10.3390/nu11030523