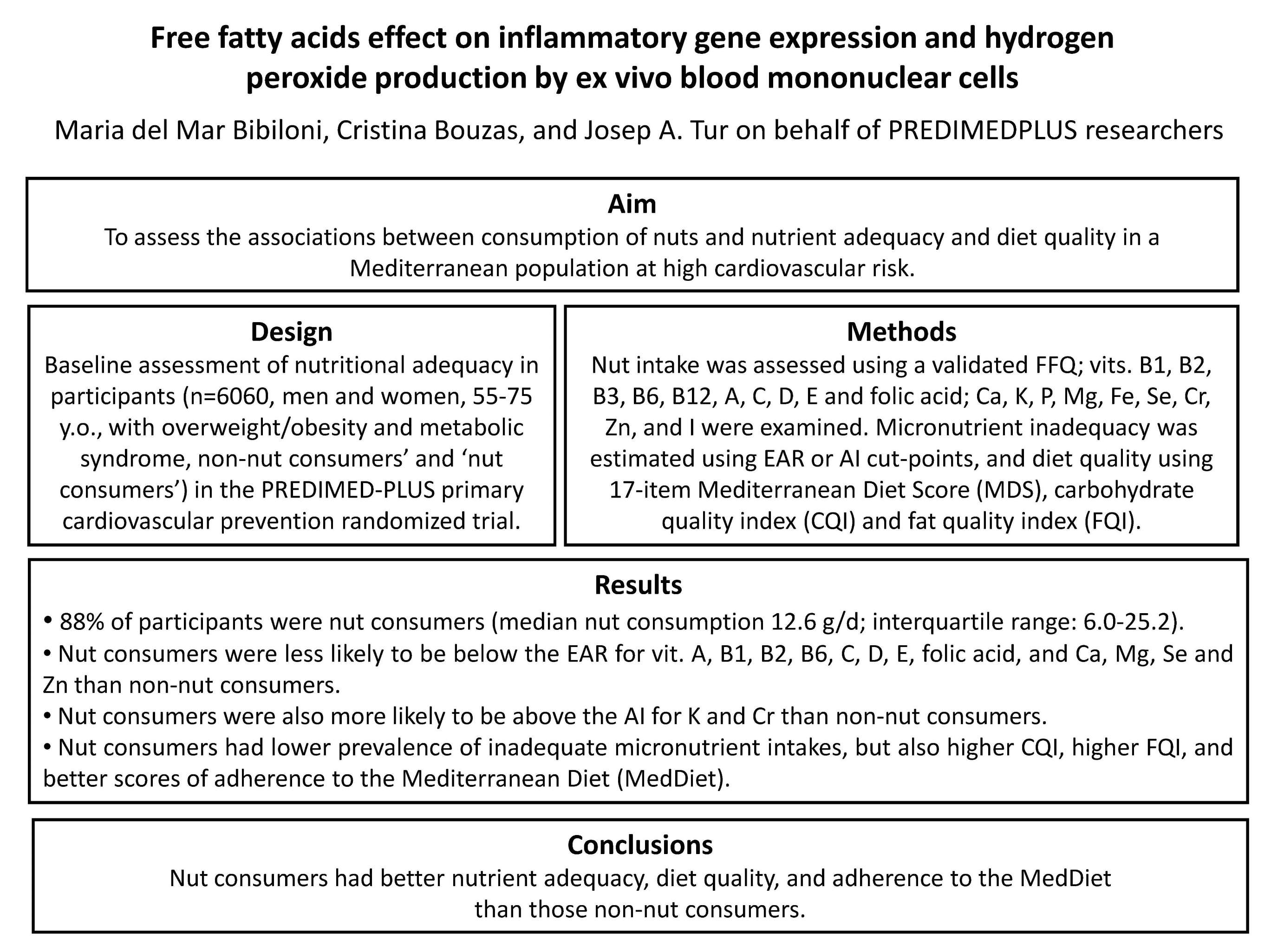
Nut Consumptions as a Marker of Higher Diet Quality in a Mediterranean Population at High Cardiovascular Risk

 , , ,
, , ,  , , , , , , , , , , ,
, , , , , , , , , , ,  , , , and add
Show full author list
, , , and add
Show full author list
Abstract
: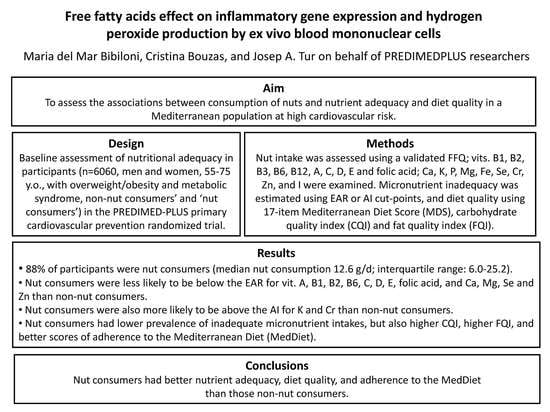
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants, Recruitment and Randomization
2.3. Dietary Assessment
2.4. Determination of Nut Consumption
2.5. Determination of Micronutrients Intake
2.6. Physical Activity
2.7. Anthropometric and Blood Pressure Measurements
2.8. Blood Collection and Analysis
2.9. Other Health Variables
2.10. Statistical Analyses
3. Results
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Adequate intake |
| CHO | Carbohydrate |
| CQI | Carbohydrate quality index |
| EAR | Estimated average requirements |
| erMedDiet | Energy-restricted traditional MedDiet |
| FFQ | Food frequency questionnaire |
| FQI | Fat quality index |
| MedDiet | Mediterranean diet |
| MET | Metabolic equivalents |
| MetS | Metabolic syndrome |
| NHANES | National Health and Nutrition Examination Survey |
| NE | Niacin equivalents |
| NZANS | New Zealand Adult Nutrition Survey |
| RAE | Retinol activity equivalents |
| RAPA | Rapid assessment of physical activity questionnaire |
| RDA | Recommended daily allowances |
| DRI | Dietary reference intake |
| TFA | Trans fatty acid |
| UL | Tolerable upper level |
References
- Castro-Quezada, I.; Román-Viñas, B.; Serra-Majem, L. The Mediterranean diet and nutritional adequacy: A review. Nutrients 2014, 6, 231–248. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Tainta, A.; Zazpe, I.; Bes-Rastrollo, M.; Salas-Salvadó, J.; Bullo, M.; Sorlí, J.V.; Corella, D.; Covas, M.I.; Arós, F.; Gutierrez-Bedmar, M.; et al. PREDIMED studyinvestigators. Nutritional adequacy according to carbohydrates and fat quality. Eur. J. Nutr. 2016, 55, 93–106. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L., 3rd; Nicklas, T.A. Tree nut consumption improves nutrient intake and diet quality in US adults: An analysis of National Health and Nutrition Examination Survey (NHANES) 1999–2004. Asia Pac. J. Clin. Nutr. 2010, 19, 142–150. [Google Scholar]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L., 3rd. Tree nut consumption is associated with better nutrient adequacy and diet quality in adults: National Health and Nutrition Examination Survey 2005–2010. Nutrients 2015, 7, 595–607. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L., 3rd. Almond Consumption Is Associated with Better Nutrient Intake, Nutrient Adequacy, and Diet Quality in Adults: National Health and Nutrition Examination Survey 2001–2010. Food Nutr. Sci. 2016, 7, 504–515. [Google Scholar]
- Brown, R.C.; Tey, S.L.; Gray, A.R.; Chisholm, A.; Smith, C.; Fleming, E.; Parnell, W. Nut consumption is associated with better nutrient intakes: Results from the 2008/09 New Zealand Adult Nutrition Survey. Br. J. Nutr. 2016, 115, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.G.; Zhang, R.; Martínez-González, M.A.; Zhang, Z.L.; Bonaccio, M.; van Dam, R.M.; Qin, L.Q. Nut consumption in relation to all-cause and cause-specific mortality: A meta-analysis 18 prospective studies. Food Funct. 2017, 8, 3893–3905. [Google Scholar] [CrossRef] [PubMed]
- Ros, E. Nuts and, C.V.D. Br. J. Nutr. 2015, 113 (Suppl. 2), S111–S120. [Google Scholar] [CrossRef]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Benefits of Nut Consumption on Insulin Resistance and Cardiovascular Risk Factors: Multiple Potential Mechanisms of Actions. Nutrients 2017, 9, 1271. [Google Scholar] [CrossRef]
- Relja, A.; Miljković, A.; Gelemanović, A.; Bošković, M.; Hayward, C.; Polašek, O.; Kolčić, I. Nut Consumption and Cardiovascular Risk Factors: A Cross-Sectional Study in a Mediterranean Population. Nutrients 2017, 9, 1296. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Liu, X.; Malik, V.S.; Sun, Q.; Willett, W.C.; Manson, J.E.; Rexrode, K.M.; Li, Y.; Hu, F.B.; Bhupathiraju, S.N. Nut Consumption and Risk of Cardiovascular Disease. J. Am. Coll. Cardiol. 2017, 70, 2519–2532. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bulló, M.; Fitó, M.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; López-Miranda, J.; et al. Cohort Profile: Design and methods of the PREDIMED-PLUS randomised trial. Int. J. Epidemiol. 2018. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- The National Academies of Sciences Engineering Medicine, Institute of Medicine (US), Food and Nutrition Board. Dietary Reference Intakes (DRIs): Estimated Average Requirements Values. Available online: http://nationalacademies.org/hmd/Activities/Nutrition/SummaryDRIs/DRI-Tables.aspx (accessed on 9 April 2018).
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin, D; National Academies Press (US): Washington, DC, USA, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK56070/ (accessed on 9 April 2018).
- Institute of Medicine (US) Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. DRI Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press (US): Washington, DC, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK222872/ (accessed on 9 April 2018).
- Zazpe, I.; Sánchez-Taínta, A.; Santiago, S.; de la Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Martínez, J.A.; Martínez-González, M.Á. SUN Project Investigators. Association between dietary carbohydrate intake quality and micronutrient intake adequacy in a Mediterranean cohort: The SUN (Seguimiento Universidad de Navarra) Project. Br. J. Nutr. 2014, 111, 2000–2009. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Molina, L.; Sarmiento, M.; Peñafiel, J.; Donaire, D.; Garcia-Aymerich, J.; Gomez, M.; Ble, M.; Ruiz, S.; Frances, A.; Schröder, H.; et al. Validation of the Regicor Short Physical Activity Questionnaire for the Adult Population. PLoS ONE 2017, 12, e0168148. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Garcia, M.; Aguilar, A.; Molina, L.; Covas, M.I.; Marrugat, J. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish Women. Investigators of the MARATDON Group. Med. Sci. Sports Exerc. 2000, 32, 1431–1437. [Google Scholar] [CrossRef]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish men. The MARATHOM Investigators. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.; Livingstone, K.M.; Affleck, A.; Navas-Carretero, S.; San-Cristobal, R.; Martinez, J.A.; Marsaux, C.F.M.; Saris, W.H.M.; O’Donovan, C.B.; Forster, H.; et al. Food4Me Study. Correlates of overall and central obesity in adults from seven European countries: Findings from the Food4Me Study. Eur. J. Clin. Nutr. 2018, 72, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Roman Viñas, B.; Ribas Barba, L.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.; van’t Veer, P.; Matthys, C.; Serra Majem, L. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Bes-Rastrollo, M.; Román-Viñas, B.; Pfrimer, K.; Sánchez-Villegas, A.; Martínez-González, M.A. Dietary patterns and nutritional adequacy in a Mediterranean country. Br. J. Nutr. 2009, 101 (Suppl. 2), S21–S28. [Google Scholar] [CrossRef]
- Mensink, G.B.; Fletcher, R.; Gurinovic, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Non-Nut Consumers (n = 1091) | Nut Consumers (n = 4969) | p | |||
|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | ||
| Subject characteristics | |||||
| Age (years) † | 65.2 (4.9) | 65.0 (61.0, 69.0) | 65.0 (4.9) | 65.0 (61.0, 69.0) | 0.222 |
| Body mass index (kg/m2) | 33.2 (3.5) | 32.9 (30.4, 35.8) | 32.6 (3.4) | 32.2 (29.9, 34.9) | <0.001 |
| Total physical activity (MET·min/week) *,† | 2074 (1845) | 1573 (707, 3019) | 2487 (1952) | 2014 (1007, 3476) | <0.001 |
| Males † | 2402 (2079) | 1958 (888, 3357) | 2837 (2174) | 2294 (1147, 4091) | <0.001 |
| Females † | 1780 (1552) | 1386 (559, 2587) | 2093 (1577) | 1734 (839, 2946) | <0.001 |
| Smoking habit ‡ | |||||
| Current smoker | 173 (16.2) | 567 (11.7) | <0.001 | ||
| Former smoker | 432 (40.4) | 2128 (43.8) | |||
| Never smoked | 463 (43.4) | 2167 (44.6) | |||
| Nutrients | |||||
| Energy intake (kcal/day) † | 2141 (555) | 2096 (1729, 2495) | 2360 (518) | 2333 (1996, 2692) | <0.001 |
| Carbohydrate intake (% total energy) | 42.3 (7.6) | 42.2 (37.3, 47.6) | 40.5 (6.6) | 40.5 (35.9, 45.0) | <0.001 |
| Solid carbohydrate (g/day) | 200.6 (69.1) | 191.0 (152.1, 243.0) | 214.6 (64.9) | 209.6 (166.3, 254.5) | <0.001 |
| Liquid carbohydrate (g/day) | 8.6 (13.8) | 1.6 (0.0, 11.4) | 8.9 (12.4) | 3.3 (0.0, 12.3) | 0.641 |
| Glycemic index | 53.7 (5.6) | 54.1 (50.5, 57.7) | 53.3 (5.1) | 53.7 (50.1, 57.0) | 0.015 |
| Protein intake (% total energy) | 16.8 (3.1) | 16.6 (14.7, 18.6) | 16.5 (2.7) | 16.3 (14.6, 18.1) | 0.002 |
| Fat intake (% total energy) | 37.6 (7.1) | 37.2 (32.7, 42.3) | 39.9 (6.3) | 39.9 (35.5, 44.2) | <0.001 |
| PUFA (% total energy) | 5.1 (1.3) | 5.0 (4.3, 5.7) | 6.6 (1.7) | 6.3 (5.3, 7.5) | <0.001 |
| MUFA (% total energy) | 19.3 (4.7) | 19.0 (15.8, 22.4) | 20.9 (4.5) | 20.7 (17.6, 23.8) | <0.001 |
| SFA (% total energy) | 9.9 (2.2) | 9.8 (8.5, 11.3) | 9.9 (1.9) | 9.8 (8.6, 11.1) | 0.543 |
| Trans fatty acid (g/d) | 0.6 (0.4) | 0.5 (0.3, 0.7) | 0.6 (0.4) | 0.5 (0.3, 0.8) | 0.901 |
| Cholesterol (mg/d) | 352.9 (114.5) | 341.2 (278.9, 422.1) | 374.9 (106.7) | 365.8 (304.1, 433.4) | <0.001 |
| Fibre intake (g/d) | 21.9 (7.4) | 21.2 (16.8, 26.3) | 25.9 (7.8) | 24.8 (20.3, 30.4) | <0.001 |
| Food groups | |||||
| Fruits (g/day) † | 309.4 (189.9) | 281.3 (175.2, 414.1) | 352.5 (186.2) | 326.6 (217.6, 456.2) | <0.001 |
| Vegetables (g/day) † | 291.7 (129.6) | 269.8 (202.1, 365.5) | 322.0 (128.8) | 304.4 (230.2, 398.1) | <0.001 |
| Legumes (g/day) † | 18.9 (11.2) | 16.4 (12.1, 24.8) | 20.3 (10.1) | 16.8 (16.1, 24.8) | <0.001 |
| Olive oil (g/day) † | 38.0 (17.5) | 35.0 (25.0, 50.0) | 40.4 (16.8) | 50.0 (25.0, 50.0) | <0.001 |
| Nuts (g/day) † | 0.0 (0.0) | 0.0 (0.0, 0.0) | 17.1 (15.8) | 12.6 (6.0, 25.2) | <0.001 |
| Total fish (g/day) † | 89.1 (44.4) | 84.6 (56.6, 119.0) | 101.0 (44.2) | 96.1 (68.1, 128.6) | <0.001 |
| Total cereals (g/day) † | 144.6 (80.1) | 114.9 (87.4, 202.0) | 148.1 (74.4) | 122.1 (91.8, 204.3) | 0.182 |
| Dairy products (g/day) † | 346.7 (195.0) | 306.9 (220.6, 518.7) | 331.3 (182.3) | 298.0 (216.6, 418.1) | 0.017 |
| Total meat (g/day) † | 138.9 (58.3) | 134.1 (101.6, 171.9) | 144.9 (54.6) | 139.6 (109.2, 177.2) | 0.002 |
| Cookies (g/day) † | 26.5 (31.3) | 14.6 (4.2, 39.4) | 26.6 (29.1) | 17.4 (6.7, 37.8) | 0.938 |
| Alcohol (g/day) † | 10.9 (16.0) | 4.3 (0.0, 12.9) | 11.0 (14.8) | 5.0 (0.7, 14.7) | 0.826 |
| Diet Quality Measures (units) | |||||
| 17-item MDS † | 7.7 (2.6) | 8.0 (6.0, 10.0) | 8.6 (2.6) | 9.0 (7.0, 10.0) | <0.001 |
| CQI † | 11.1 (3.4) | 11.0 (8.0, 14.0) | 12.1 (3.4) | 12.0 (9.0, 15.0) | <0.001 |
| FQI † | 2.5 (0.6) | 2.4 (2.1, 2.8) | 2.8 (0.6) | 2.7 (2.3, 3.1) | <0.001 |
| MetS components: n (%) | |||||
| High blood pressure ‡ | 1012 (92.8) | 4577 (92.1) | 0.469 | ||
| Hyperglycemia ‡ | 839 (76.9) | 3738 (75.2) | 0.244 | ||
| Hypertriglyceridemia ‡ | 613 (56.2) | 2781 (56.0) | 0.895 | ||
| Low HDL-cholesterol ‡ | 459 (42.1) | 2130 (42.9) | 0.631 | ||
| Abdominal obesity ‡ | 1053 (96.5) | 4771 (96.0) | 0.438 | ||
| Males ‡ | 476 (93.0) | 2424 (93.0) | 0.969 | ||
| Females ‡ | 577 (99.7) | 2347 (99.3) | 0.490 | ||
| Usual Intake | Percentile | EAR | % Below EAR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Group | Mean (SD) | P1 | 10 | 25 | 50 | 75 | 90 | % | P2 | |
| Vitamin A RAE (µg/day) | Non-nut consumers | 940.6 (517.0) | <0.001 | 439.7 | 564.9 | 783.6 | 1171.9 | 1692.4 | M: 625.0 µg/day | 23.9 | <0.001 |
| Nut-consumers | 1064.0 (533.6) | 521.2 | 662.6 | 913.2 | 1387.2 | 1826.7 | W: 500.0 µg/day | 15.1 | |||
| Vitamin B1 (mg/day) | Non-nut consumers | 1.4 (0.4) | <0.001 | 1.0 | 1.2 | 1.4 | 1.7 | 1.9 | M: 1.0 mg/day | 8.7 | <0.001 |
| Nut-consumers | 1.6 (0.4) | 1.2 | 1.4 | 1.6 | 1.8 | 2.1 | W: 0.9 mg/day | 2.5 | |||
| Vitamin B2 (mg/day) | Non-nut consumers | 1.8 (0.5) | <0.001 | 1.2 | 1.4 | 1.7 | 2.1 | 2.5 | M: 1.1 mg/day | 4.5 | <0.001 |
| Nut-consumers | 1.9 (0.5) | 1.3 | 1.6 | 1.9 | 2.3 | 2.6 | W: 0.9 mg/day | 2.0 | |||
| Vitamin B3 NE (mg/day) | Non-nut consumers | 36.3 (9.1) | <0.001 | 25.2 | 30.1 | 35.6 | 42.3 | 48.0 | M: 12.0 mg/day | 0.0 | 1.000 |
| Nut-consumers | 39.8 (8.8) | 28.8 | 33.7 | 39.6 | 45.7 | 51.4 | W: 11.0 mg/day | 0.0 | |||
| Vitamin B6 (mg/day) | Non-nut consumers | 2.0 (0.5) | <0.001 | 1.4 | 1.7 | 2.0 | 2.4 | 2.7 | M: 1.4 mg/day | 6.2 | <0.001 |
| Nut-consumers | 2.3 (0.5) | 1.7 | 1.9 | 2.3 | 2.6 | 3.0 | W: 1.3 mg/day | 2.6 | |||
| Vitamin B12 (µg/day) | Non-nut consumers | 8.7 (3.8) | <0.001 | 4.5 | 5.9 | 8.0 | 10.9 | 14.1 | M: 2.0 µg/day | 0.4 | 0.088 |
| Nut-consumers | 9.7 (3.8) | 5.3 | 6.7 | 9.0 | 12.0 | 15.1 | W: 2.0 µg/day | 0.1 | |||
| Folic acid (µg/day) | Non-nut consumers | 303.7 (86.7) | <0.001 | 200.2 | 242.0 | 295.0 | 354.3 | 419.1 | M: 320.0 µg/day | 60.6 | <0.001 |
| Nut-consumers | 345.8 (89.4) | 238.8 | 283.0 | 335.5 | 400.9 | 470.2 | W: 320.0 µg/day | 42.5 | |||
| Vitamin C (mg/day) | Non-nut consumers | 175.0 (74.6) | <0.001 | 85.5 | 120.8 | 165.6 | 217.3 | 277.3 | M: 75.0 mg/day | 4.6 | <0.001 |
| Nut-consumers | 197.5 (76.6) | 108.4 | 142.5 | 184.4 | 243.5 | 304.0 | W: 60.0 mg/day | 1.9 | |||
| Vitamin D (µg/day) | Non-nut consumers | 5.2 (3.2) | <0.001 | 1.9 | 3.0 | 4.3 | 6.8 | 10.2 | M: 10.0 µg/day | 89.6 | 0.001 |
| Nut-consumers | 6.1 (3.2) | 2.6 | 3.8 | 5.1 | 8.8 | 10.8 | W: 10.0 µg/day | 85.7 | |||
| Vitamin E (mg/day) | Non-nut consumers | 8.3 (2.7) | <0.001 | 5.3 | 6.5 | 7.9 | 9.5 | 11.5 | M: 12 mg/day | 91.8 | <0.001 |
| Nut-consumers | 10.6 (3.2) | 6.9 | 8.3 | 10.0 | 12.3 | 15.0 | W: 12 mg/day | 71.9 | |||
| Ca (mg/day) | Non-nut consumers | 950.9 (325.3) | <0.001 | 572.5 | 708.8 | 909.9 | 1144.1 | 1391.5 | M 51–70 y-o: 800.0 mg/day M >70 y-o: 1000.0 mg/day W: 1000.0 mg/day | 50.6 | <0.001 |
| Nut-consumers | 1008.4 (306.1) | 637.7 | 789.4 | 977.0 | 1208.7 | 1418.4 | 40.2 | ||||
| Mg (mg/day) | Non-nut consumers | 344.4 (86.2) | <0.001 | 245.4 | 284.7 | 331.1 | 393.7 | 461.7 | M: 350.0 mg/day | 36.7 | <0.001 |
| Nut-consumers | 402.9 (94.5) | 288.9 | 333.8 | 394.8 | 463.2 | 533.8 | W: 265.0 mg/day | 18.8 | |||
| P (mg/day) | Non-nut consumers | 1580.8 (388.3) | <0.001 | 1109.0 | 1291.8 | 1541.2 | 1827.1 | 2099.9 | M: 580.0 mg/day | 0.2 | 0.086 |
| Nut-consumers | 1728.7 (374.9) | 1253.3 | 1465.5 | 1714.3 | 1985.1 | 2225.5 | W: 580.0 mg/day | 0.0 | |||
| Fe (mg/day) | Non-nut consumers | 14.6 (3.6) | <0.001 | 10.2 | 12.1 | 14.3 | 16.8 | 19.5 | M: 6.0 mg/day | 0.2 | 0.086 |
| Nut-consumers | 16.4 (3.6) | 12.0 | 13.9 | 16.2 | 18.8 | 21.3 | W: 5.0 mg/day | 0.0 | |||
| Se (µg/day) | Non-nut consumers | 106.1 (32.1) | <0.001 | 66.9 | 83.1 | 102.7 | 126.8 | 148.8 | M: 45.0 µg/day | 1.4 | <0.001 |
| Nut-consumers | 116.5 (30.5) | 78.7 | 94.8 | 114.9 | 136.1 | 157.0 | W: 45.0 µg/day | 0.3 | |||
| Zn (mg/day) | Non-nut consumers | 12.0 (3.1) | <0.001 | 8.4 | 9.8 | 11.7 | 13.9 | 16.3 | M: 9.4 mg/day | 9.4 | <0.001 |
| Nut-consumers | 13.1 (3.0) | 9.4 | 11.0 | 12.9 | 15.0 | 17.1 | W: 6.8 mg/day | 5.0 | |||
| Iodine (µg/day) | Non-nut consumers | 282.5 (153.8) | 0.213 | 92.9 | 176.4 | 252.2 | 328.0 | 531.0 | M: 95.0 µg/day | 10.4 | 0.577 |
| Nut-consumers | 276.1 (143.5) | 95.5 | 181.5 | 258.2 | 298.2 | 531.9 | W: 95.0 µg/day | 9.8 | |||
| K (g/day) | Non-nut consumers | 4.0 (1.0) | <0.001 | 2.9 | 3.3 | 3.9 | 4.6 | 5.4 | M: 4.7 g/day | 23.5 | <0.001 |
| Nut-consumers | 4.4 (1.0) | 3.3 | 3.8 | 4.4 | 5.1 | 5.7 | W: 4.7 g/day | 37.7 | |||
| Cr (µg/day) | Non-nut consumers | 76.7 (46.1) | <0.001 | 37.4 | 46.7 | 61.4 | 89.7 | 140.1 | M: 30.0 µg/day | 98.8 | 0.046 |
| Nut-consumers | 83.8 (44.2) | 42.1 | 51.8 | 70.6 | 103.7 | 144.5 | W: 20.0 µg/day | 99.4 | |||
| Quintiles of Nut Consumption | ||||||
|---|---|---|---|---|---|---|
| Variables | Q1 (n = 1182) | Q2 (n = 980) | Q3 (n = 848) | Q4 (n = 987) | Q5 (n = 972) | p * |
| Vitamin A RAE (µg/day) | ||||||
| Mean ± SD | 980.5 ± 520.2 a,b,c,d | 1055.1 ± 519.9 a,g | 1069.9 ± 532.6 b,h,i | 1096.2 ± 525.9 c | 1136.8 ± 558.2 d,h,i | <0.001 |
| % below EAR | 20.8 | 13.2 | 14.6 | 13.3 | 12.1 | <0.001 |
| Vitamin B1 (mg/day) | ||||||
| Mean ± SD | 1.5 ± 0.4 a,b,c,d | 1.6 ± 0.4 a,f,g | 1.6 ± 0.4 b,h,i | 1.7 ± 0.3 c,f,h,j | 1.8 ± 0.3 d,g,i,j | <0.001 |
| % below EAR | 4.7 | 2.9 | 2.5 | 1.3 | 0.4 | <0.001 |
| Vitamin B2 (mg/day) | ||||||
| Mean ± SD | 1.8 ± 0.5 b,c,d | 1.9 ± 0.5 f,g | 1.9 ± 0.5 b,h,i | 2.0 ± 0.5 c,f,h,j | 2.1 ± 0.5 d,g,i,j | <0.001 |
| % below EAR | 3.2 | 1.9 | 2.0 | 1.2 | 1.4 | 0.009 |
| Vitamin B3 NE (mg/day) | ||||||
| Mean ± SD | 37.8 ± 8.8 a,b,c,d | 39.3 ± 8.7 a,f,g | 39.3 ± 8.6 b,h,i | 41.0 ± 8.6 c,f,h | 42.1 ± 8.6 d,g,i | <0.001 |
| % below EAR | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.000 |
| Vitamin B6 (mg/day) | ||||||
| Mean ± SD | 2.1 ± 0.5 a,b,c,d | 2.2 ± 0.5 a,f,g | 2.3 ± 0.5 b,h,i | 2.4 ± 0.5 c,f,h,j | 2.5 ± 0.5 d,g,i,j | <0.001 |
| % below EAR | 6.6 | 2.6 | 1.8 | 1.0 | 0.3 | <0.001 |
| Vitamin B12 (µg/day) | ||||||
| Mean ± SD | 9.2 ± 3.8 a,c,d | 9.7 ± 3.8 a | 9.6 ± 3.8 | 10.0 ± 3.9 c | 10.0 ± 3.9 d | <0.001 |
| % below EAR | 0.1 | 0.1 | 0.2 | 0.2 | 0.0 | 0.590 |
| Folic acid (µg/day) | ||||||
| Mean ± SD | 316.6 ± 83.9 a,b,c,d | 332.1 ± 87.5 a,f,g | 340.5 ± 82.4 b,h,i | 358.3 ± 86.7 c,f,h,j | 387.1 ± 89.1 d,g,i,j | <0.001 |
| % below EAR | 57.3 | 48.1 | 45.4 | 35.1 | 24.2 | <0.001 |
| Vitamin C (mg/day) | ||||||
| Mean ± SD | 181.5 ± 75.5 a,b,c,d | 194.3 ± 77.2 a,g | 195.2 ± 73.1 b,i | 202.6 ± 74.4 c,j | 216.9 ± 78.1 d,g,i,j | <0.001 |
| % below EAR | 3.8 | 1.4 | 1.9 | 1.2 | 0.9 | <0.001 |
| Vitamin D (µg/day) | ||||||
| Mean ± SD | 5.5 ± 3.1 a,b,c,d | 6.0 ± 3.1 a,f,g | 5.9 ± 3.1 b,h,i | 6.5 ± 3.3 c,f,h | 6.6 ± 3.3 d,g,i | <0.001 |
| % below EAR | 89.1 | 87.6 | 88.1 | 82.1 | 81.1 | <0.001 |
| Vitamin E (mg/day) | ||||||
| Mean ± SD | 8.9 ± 2.7 a,b,c,d | 9.9 ± 2.5 a,f,g | 10.0 ± 2.6 b,h,i | 11.4 ± 2.7 c,f,h,j | 13.1 ± 3.7 d,g,i,j | <0.001 |
| % below EAR | 89.0 | 84.8 | 80.8 | 62.5 | 39.7 | <0.001 |
| Ca (mg/day) | ||||||
| Mean ± SD | 961.6 ± 296.8 b,c,d | 983.4 ± 295.5 f,g | 1000.4 ± 310.9 b,i | 1027.3 ± 307.2 c,f,j | 1078.6 ± 308.6 d,g,i,j | <0.001 |
| % below EAR | 46.7 | 43.4 | 41.4 | 38.2 | 30.3 | <0.001 |
| Mg (mg/day) | ||||||
| Mean ± SD | 355.7 ± 83.5 a,b,c,d | 379.1 ± 84.6 a,e,f,g | 392.5 ± 81.8 b,e,h,i | 424.5 ± 87.0 c,f,h,j | 471.7 ± 88.9 d,g,i,j | <0.001 |
| % below EAR | 32.4 | 23.0 | 18.5 | 12.5 | 4.7 | <0.001 |
| P (mg/day) | ||||||
| Mean ± SD | 1609.6 ± 358.8 a,b,c,d | 1671.7 ± 358.8 a,f,g | 1706.7 ± 360.7 b,h,i | 1785.8 ± 367.9 c,f,h,j | 1891.9 ± 361.9 d,g,i,j | <0.001 |
| % below EAR | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.524 |
| Fe (mg/day) | ||||||
| Mean ± SD | 15.2 ± 3.5 a,b,c,d | 16.0 ± 3.5 a,f,g | 16.2 ± 3.4 b,h,i | 16.9 ± 3.4 c,f,h,j | 18.0 ± 3.4 d,g,i,j | <0.001 |
| % below EAR | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.524 |
| Se (µg/day) | ||||||
| Mean ± SD | 111.3 ± 31.5 b,c,d | 114.8 ± 29.8 f,g | 115.6 ± 30.6 b,i | 119.2 ± 29.7 c,f | 122.7 ± 29.54 d,g,i | <0.001 |
| % below EAR | 0.5 | 0.4 | 0.4 | 0.2 | 0.0 | 0.251 |
| Zn (mg/day) | ||||||
| Mean ± SD | 12.4 ± 3.0 a,b,c,d | 12.8 ± 3.0 a,f,g | 12.9 ± 3.0 b,h,i | 13.4 ± 2.9 c,f,h,j | 13.9 ± 2.8 d,g,i,j | <0.001 |
| % below EAR | 7.4 | 5.3 | 5.4 | 4.4 | 1.9 | <0.001 |
| Iodine (µg/day) | ||||||
| Mean ± SD | 280.7 ± 144.9 | 266.4 ± 135.5 | 279.4 ± 146.8 | 274.4 ± 145.1 | 279.3 ± 144.8 | 0.148 |
| % below EAR | 10.2 | 9.0 | 10.0 | 9.5 | 10.2 | 0.862 |
| K (g/day) | ||||||
| Mean ± SD | 4135.7 ± 927.2 a,b,c,d | 4290.8 ± 923.2 a,e,f,g | 4424.5 ± 891.3 b,e,h,i | 4597.0 ± 957.3 c,f,h,j | 4855.8 ± 954.2 d,g,i,j | <0.001 |
| % above AI | 25.2 | 30.7 | 36.1 | 43.9 | 55.1 | <0.001 |
| Cr (µg/day) | ||||||
| Mean ± SD | 77.4 ± 44.0 c,d | 79.3 ± 41.8 f,g | 82.7 ± 42.2 h,i | 88.8 ± 45.3 c,f,h | 92.2 ± 45.6 d,g,i | <0.001 |
| % above AI | 98.7 | 99.6 | 99.4 | 99.5 | 99.8 | 0.020 |
| Unmet DRI | Non-Nut Consumers (n = 1091) | Nut Consumers (n = 4969) | P1 |
|---|---|---|---|
| Failing to meet 6 or more recommendations | |||
| <6 | 64.4 | 80.6 | <0.001 |
| ≥6 | 35.6 | 19.4 | |
| Crude OR 2 (95% CI) | 1.00 (ref.) | 0.44 (0.38, 0.50) ** | |
| Adjusted OR 3 (95% CI) | 1.00 (ref.) | 0.58 (0.49, 0.69) ** | |
| Adjusted OR 4 (95% CI) | 1.00 (ref.) | 0.59 (0.49, 0.71) ** | |
| Failing to meet 8 or more recommendations | |||
| <8 | 89.2 | 95.0 | <0.001 |
| ≥8 | 10.8 | 5.0 | |
| Crude OR 2 (95% CI) | 1.00 (ref.) | 0.43 (0.34, 0.54) ** | |
| Adjusted OR 3 (95% CI) | 1.00 (ref.) | 0.73 (0.55, 0.97) * | |
| Adjusted OR 4 (95% CI) | 1.00 (ref.) | 0.80 (0.59, 1.07) NS | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bibiloni, M.d.M.; Julibert, A.; Bouzas, C.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Zomeño, M.D.; Vioque, J.; Romaguera, D.; Martínez, J.A.; et al. Nut Consumptions as a Marker of Higher Diet Quality in a Mediterranean Population at High Cardiovascular Risk. Nutrients 2019, 11, 754. https://doi.org/10.3390/nu11040754
Bibiloni MdM, Julibert A, Bouzas C, Martínez-González MA, Corella D, Salas-Salvadó J, Zomeño MD, Vioque J, Romaguera D, Martínez JA, et al. Nut Consumptions as a Marker of Higher Diet Quality in a Mediterranean Population at High Cardiovascular Risk. Nutrients. 2019; 11(4):754. https://doi.org/10.3390/nu11040754
Chicago/Turabian StyleBibiloni, Maria del Mar, Alicia Julibert, Cristina Bouzas, Miguel A. Martínez-González, Dolores Corella, Jordi Salas-Salvadó, M. Dolors Zomeño, Jesús Vioque, Dora Romaguera, J. Alfredo Martínez, and et al. 2019. "Nut Consumptions as a Marker of Higher Diet Quality in a Mediterranean Population at High Cardiovascular Risk" Nutrients 11, no. 4: 754. https://doi.org/10.3390/nu11040754