Sleep Duration is Inversely Associated with Serum Uric Acid Concentrations and Uric Acid to Creatinine Ratio in an Elderly Mediterranean Population at High Cardiovascular Risk

 , , , , , , , , , , , , , ,
, , , , , , , , , , , , , ,  , , , , , , , ,
, , , , , , , ,  ,
,  , , , and
, , , and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Methods
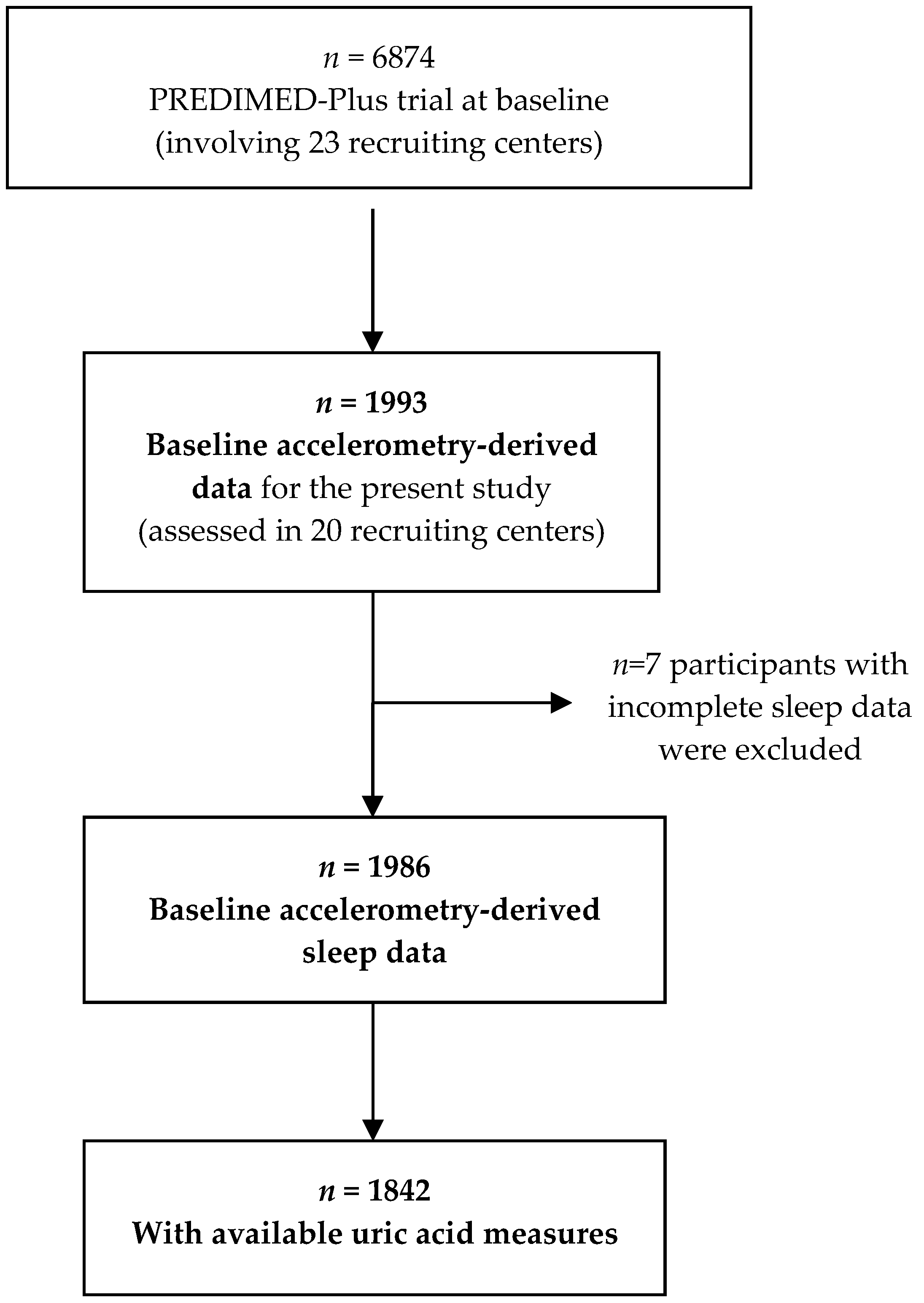
2.1. Study Design and Population
2.2. Biochemical Analyses
2.3. Sleep Assessment by Accelerometry
2.4. Covariate Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ekpenyong, C.A.E. Abnormal Serum Uric Acid Levels in Health and Disease: A Double-Edged Sword. Am. J. Intern. Med. 2014, 2, 113–130. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Al-Attas, O.S.; Wani, K.; Sabico, S.; Alokail, M.S. Serum Uric Acid to Creatinine Ratio and Risk of Metabolic Syndrome in Saudi Type 2 Diabetic Patients. Sci. Rep. 2017, 7, 12104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, L.; Huang, L.; Wu, H.; Lou, Q.; Bian, R. Serum uric acid to creatinine ratio: A predictor of incident chronic kidney disease in type 2 diabetes mellitus patients with preserved kidney function. Diab. Vasc. Dis. Res. 2017, 14, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocak, D.N.; Sasak, G.; Akturk, A.U.; Akgun, M.; Boga, S.; Sengul, A.; Gungor, S.; Arinc, S. Serum Uric Acid Levels and Uric Acid/Creatinine Ratios in Stable Chronic Obstructive Pulmonary Disease (COPD) Patients: Are These Parameters Efficient Predictors of Patients at Risk for Exacerbation and/or Severity of Disease? Med. Sci. Monit. 2016, 22, 4169–4176. [Google Scholar] [CrossRef] [Green Version]
- Hirotsu, C.; Tufik, S.; Guindalini, C.; Mazzotti, D.R.; Bittencourt, L.R.; Andersen, M.L. Association between uric acid levels and obstructive sleep apnea syndrome in a large epidemiological sample. PLoS ONE 2013, 8, e66891. [Google Scholar] [CrossRef] [PubMed]
- Kohler, M.; Stradling, J.R. Mechanisms of vascular damage in obstructive sleep apnea. Nat. Rev. Cardiol. 2010, 7, 677–685. [Google Scholar] [CrossRef]
- Irwin, M.; Thompson, J.; Miller, C.; Gillin, J.C.; Ziegler, M. Effects of sleep and sleep deprivation on catecholamine and interleukin-2 levels in humans: Clinical implications. J. Clin. Endocrinol. Metab. 1999, 84, 1979–1985. [Google Scholar] [CrossRef] [PubMed]
- Mônico-Neto, M.; Antunes, H.K.M.; Dattilo, M.; Medeiros, A.; Souza, H.S.; Lee, K.S.; de Melo, C.M.; Tufik, S.; de Mello, M.T. Resistance exercise: A non-pharmacological strategy to minimize or reverse sleep deprivation-induced muscle atrophy. Med. Hypotheses 2013, 80, 701–705. [Google Scholar] [CrossRef] [Green Version]
- Adam, K.; Oswald, I. Protein synthesis, bodily renewal and the sleep-wake cycle. Clin. Sci. (Lond.) 1983, 65, 561–567. [Google Scholar] [CrossRef]
- Wiener, R.C.; Shankar, A. Association between Serum Uric Acid Levels and Sleep Variables: Results from the National Health and Nutrition Survey 2005–2008. Int. J. Inflam. 2012. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bullo, M.; Fito, M.; Vioque, J.; Romaguera, D.; Martinez, J.A.; Warnberg, J.; Lopez-Miranda, J.; et al. Cohort Profile: Design and methods of the PREDIMED-Plus randomized trial. Int. J. Epidemiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; International Diabetes Federation Task Force on Epidemiology and Prevention; Hational Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; International Association for the Study of Obesity. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Nutrition Screening Initiative. Nutrition Interventions Manual for Professionals Caring for Older Americans; NSI: Washington, DC, USA, 1992. [Google Scholar]
- Lipschitz, D.A. Screening for nutritional status in the elderly. Prim. Care 1994, 21, 55–67. [Google Scholar] [PubMed]
- Rosique-Esteban, N.; Papandreou, C.; Romaguera, D.; Warnberg, J.; Corella, D.; Martínez-González, M.A.; Díaz-López, A.; Estruch, R.; Vioque, J.; Arós, F.; et al. Cross-sectional associations of objectively-measured sleep characteristics with obesity and type 2 diabetes in the PREDIMED-Plus trial. Sleep 2018, 41. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: http://www.who.int/dietphysicalactivity/factsheet_olderadults/en/ (accessed on 3 April 2018).
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Hillard, P.J.A.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef]
- Liu, H.; Wang, G.; Luan, G.; Liu, Q. Effects of sleep and sleep deprivation on blood cell count and hemostasis parameters in healthy humans. J. Thromb. Thrombolysis 2009, 28, 46–49. [Google Scholar] [CrossRef]
- Boudjeltia, K.Z.; Faraut, B.; Stenuit, P.; Esposito, M.J.; Dyzma, M.; Brohée, D.; Ducobu, J.; Vanhaeverbeek, M.; Kerkhofs, M. Sleep restriction increases white blood cells, mainly neutrophil count, in young healthy men: A pilot study. Vasc. Health Risk Manag. 2008, 4, 1467–1470. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.; Cherubini, A.; Ble, A.; Bos, A.J.G.; Maggio, M.; Dixit, V.D.; Lauretani, F.; Bandinelli, S.; Senin, U.; Ferrucci, L. Uric acid and inflammatory markers. Eur. Heart J. 2006, 27, 1174–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glantzounis, G.K.; Tsimoyiannis, E.C.; Kappas, A.M.; Galaris, D.A. Uric acid and oxidative stress. Curr. Pharm. Des. 2005, 11, 4145–4151. [Google Scholar] [CrossRef] [PubMed]
- Vgontzas, A.N.; Zoumakis, M.; Papanicolaou, D.A.; Bixler, E.O.; Prolo, P.; Lin, H.-M.; Vela-Bueno, A.; Kales, A. Chronic insomnia is associated with a shift of interleukin-6 and tumor necrosis factor secretion from nighttime to daytime. Metabolism 2002, 51, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Raison, C.L.; Rye, D.B.; Woolwine, B.J.; Vogt, G.J.; Bautista, B.M.; Spivey, J.R.; Miller, A.H. Chronic interferon-alpha administration disrupts sleep continuity and depth in patients with hepatitis C: Association with fatigue, motor slowing, and increased evening cortisol. Biol. Psychiatry 2010, 68, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Kamperis, K.; Hagstroem, S.; Radvanska, E.; Rittig, S.; Djurhuus, J.C. Excess diuresis and natriuresis during acute sleep deprivation in healthy adults. Am. J. Physiol. Renal Physiol. 2010, 299, 404–411. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Categories of Nocturnal Sleep Duration (h) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total n = 1842 | <6 h n = 308 | 6–<7 h n = 618 | 7–<8 h n = 654 | 8–<9 h n = 225 | ≥9 h n = 37 | p-Value | ||
| Age, mean ± SD, years | 65 ± 5 | 64 ± 5 | 65 ± 5 | 65 ± 5 | 66 ± 4 | 68 ± 4 | <0.001 | |
| Male, n (%) | 979(53) | 229(74) | 348(56) | 305(46) | 85(38) | 12(32) | <0.001 | |
| BMI, mean ± SD, kg/m2 | 32.6 ± 3.4 | 33.1 ± 3.5 | 32.5 ± 3.5 | 32.3 ± 3.4 | 32.6 ± 3.2 | 32.5 ± 3.4 | 0.031 | |
| Type 2 diabetes, n (%) | 505(27) | 95(31) | 174(28) | 170(26) | 51(22) | 15(40) | 0.156 | |
| Sleep apnea, n (%) | 237(13) | 49(16) | 73(12) | 89(13) | 23(10) | 3(8) | 0.229 | |
| Depression, n (%) | 389(21) | 59(19) | 113(17) | 153(23) | 65(29) | 11(30) | 0.001 | |
| Sedative treatment, n (%) | 442(24) | 53(17) | 114(18) | 175(27) | 86(38) | 14(38) | <0.001 | |
| Uric acid agents, n (%) | 168(9) | 27(9) | 62(10) | 66(10) | 10(4) | 3(8) | 0.117 | |
| Smoking, n (%) | ||||||||
| Never | 795(43) | 91(29) | 254(41) | 314(48) | 114(51) | 22(61) | <0.001 | |
| Former | 828(45) | 168(55) | 289(47) | 280(43) | 82(36) | 9(25) | ||
| Current | 212(11) | 48(15) | 73(12) | 58(9) | 28(12) | 5(14) | ||
| Adherence to energy-restricted MedDiet (score from 0 to 17 items), mean ± SD | 8.6 ± 2.7 | 8.2 ± 2.7 | 8.7 ± 2.7 | 8.5 ± 2.7 | 8.7 ± 2.7 | 9.6 ± 2.9 | 0.017 | |
| Compliance of MVPA recommendations a, n (%) | 352(19) | 51(16) | 133(21) | 134(20) | 33(13) | 4(11) | 0.027 | |
| Education status, n (%) | ||||||||
| Primary education | 909(49) | 136(44) | 278(45) | 338(52) | 132(59) | 25(67) | <0.001 | |
| Secondary education | 494(27) | 76(25) | 175(28) | 185(28) | 52(23) | 6(16) | ||
| Academic/graduate | 413(22) | 92(30) | 157(25) | 124(18) | 35(15) | 5(13) | ||
| Employment status, n (%) | ||||||||
| Working | 376(20) | 92(30) | 148(24) | 110(17) | 25(11) | 1(2) | <0.001 | |
| Non-working | 441(25) | 62(18) | 147(23) | 182(26) | 71(29) | 10(26) | ||
| Retired | 1017(55) | 160(53) | 331(54) | 363(55) | 136(60) | 27(73) | ||
| Marital status, n (%) | ||||||||
| Single/divorced | 267(14) | 49(16) | 95(15) | 93(14) | 22(10) | 8(21) | 0.029 | |
| Married | 1369(75) | 227(74) | 471(77) | 477(73) | 170(76) | 24(65) | ||
| Widower | 196(11) | 31(10) | 46(7) | 82(12) | 32(14) | 5(13) | ||
| Categories of Nocturnal Sleep Duration (h) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total n = 1842 | <6 h n = 308 | 6–<7 h n = 618 | 7–<8 h n = 654 | 8–<9 h n = 225 | ≥9 h n = 37 | p-Value | ||
| Sleep parameters | ||||||||
| Sleep duration, mean ± SD, h | 6.9 ± 1.1 | 5.3 ± 0.7 | 6.5 ± 0.3 | 7.4 ± 0.3 | 8.4 ± 0.2 | 9.3 ± 0.3 | <0.001 | |
| Sleep variability, median interquartile range, h | 0.8 0.6; 1.1 | 0.90.6; 1.2 | 0.8 0.6; 1.0 | 0.8 0.6; 1.1 | 0.7 0.6; 1.0 | 0.8 0.6; 0.9 | <0.001 | |
| Napping duration, median interquartile range, min | 76.749.7; 109.8 | 64.842.3; 91.1 | 67.742.9; 97.1 | 78.8 53.5; 108.6 | 113.4 79.9; 145.2 | 163.9 109.8; 203.5 | <0.001 | |
| Biochemical parameters | ||||||||
| Serum uric acid, mean ± SD, mg/dL | 6.0 ± 1.4 | 6.3 ± 1.5 | 6.1 ± 1.5 | 5.9 ± 1.4 | 5.7 ± 1.4 | 5.4 ± 1.5 | <0.001 | |
| Creatinine, mean ± SD, mg/dL | 0.83 ± 0.2 | 0.85 ± 0.2 | 0.82 ± 0.2 | 0.83 ± 0.2 | 0.83 ± 0.2 | 0.80 ± 0.2 | 0.165 | |
| Serum uric acid to creatinine ratio | 7.4 ± 1.9 | 7.6 ± 1.9 | 7.7 ± 1.9 | 7.4 ± 1.8 | 7.1 ± 1.8 | 6.9 ± 2.2 | <0.001 | |
| Leukocytes, mean ± SD, counts | 6.7 ± 1.7 | 6.9 ± 1.8 | 6.7 ± 1.7 | 6.5 ± 1.6 | 6.8 ± 1.8 | 6.7 ± 1.4 | 0.090 | |
| Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | |
|---|---|---|---|---|---|---|
| SUA | ||||||
| Sleep duration (h) | −0.08 (−0.14, −0.02) | 0.008 | −0.07 (−0.13, −0.01) | 0.047 | −0.06 (−0.13, 0.01) | 0.050 |
| Sleep variability (h) | −0.29 (−0.60, 0.01) | 0.056 | −0.26 (−0.56, 0.05) | 0.100 | −0.25 (−0.56, 0.05) | 0.101 |
| SUA/Cr | ||||||
| Sleep duration (h) | −0.20 (−0.29, −0.12) | <0.001 | −0.15 (−0.24, −0.06) | 0.001 | −0.15 (−0.24, −0.06) | 0.001 |
| Sleep variability (h) | −0.30 (−0.72, 0.12) | 0.163 | −0.23 (−0.66, 0.19) | 0.279 | −0.24 (−0.67, 0.19) | 0.272 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papandreou, C.; Babio, N.; Díaz-López, A.; Martínez-González, M.Á.; Becerra-Tomas, N.; Corella, D.; Schröder, H.; Romaguera, D.; Vioque, J.; Alonso-Gómez, Á.M.; et al. Sleep Duration is Inversely Associated with Serum Uric Acid Concentrations and Uric Acid to Creatinine Ratio in an Elderly Mediterranean Population at High Cardiovascular Risk. Nutrients 2019, 11, 761. https://doi.org/10.3390/nu11040761
Papandreou C, Babio N, Díaz-López A, Martínez-González MÁ, Becerra-Tomas N, Corella D, Schröder H, Romaguera D, Vioque J, Alonso-Gómez ÁM, et al. Sleep Duration is Inversely Associated with Serum Uric Acid Concentrations and Uric Acid to Creatinine Ratio in an Elderly Mediterranean Population at High Cardiovascular Risk. Nutrients. 2019; 11(4):761. https://doi.org/10.3390/nu11040761
Chicago/Turabian StylePapandreou, Christopher, Nancy Babio, Andrés Díaz-López, Miguel Á. Martínez-González, Nerea Becerra-Tomas, Dolores Corella, Helmut Schröder, Dora Romaguera, Jesús Vioque, Ángel M. Alonso-Gómez, and et al. 2019. "Sleep Duration is Inversely Associated with Serum Uric Acid Concentrations and Uric Acid to Creatinine Ratio in an Elderly Mediterranean Population at High Cardiovascular Risk" Nutrients 11, no. 4: 761. https://doi.org/10.3390/nu11040761