Pre-Pregnancy Adherence to the Mediterranean Diet and Gestational Diabetes Mellitus: A Case-Control Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Setting
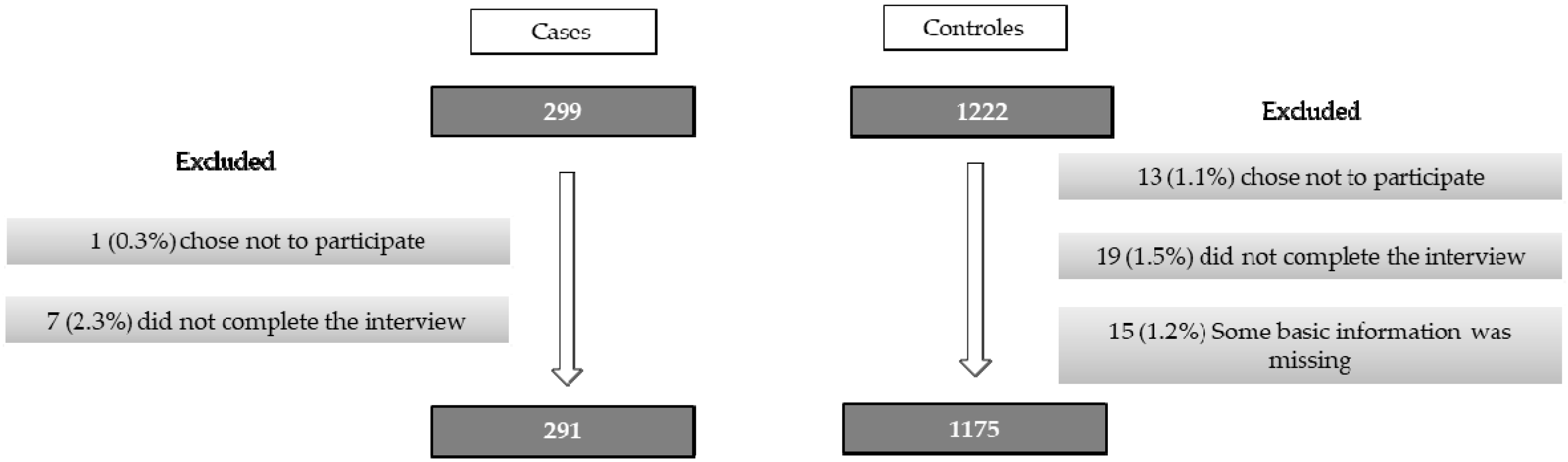
2.2. Participants
2.3. Data Sources and Variables
2.3.1. Dietary Assessment
2.3.2. Other Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2019, 42, S13–S28. [Google Scholar]
- Shepherd, E.; Gomersall, J.C.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 11, CD010443. [Google Scholar] [CrossRef]
- Ruiz-Ramos, M.; Escolar-Pujolar, A.; Mayoral-Sánchez, E.; Corral-San Laureano, F.; Fernández-Fernández, I. Diabetes mellitus in Spain: Death rates, prevalence, impact, costs and inequalities. Gac. Sanit. 2006, 20, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Moleon, J.J.; Bueno-Cavanillas, A.; Luna-Del-Castillo, J.D.; Garciá-Martín, M.; Lardelli-Claret, P.; Gálvez-Vargas, R. Prevalence of gestational diabetes mellitus: Variations related to screening strategy used. Eur. J. Endocrinol. 2002, 146, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.W.; Yang, H.X.; Wang, C.; Su, R.N.; Feng, H.; Kapur, A. High Prevalence of Gestational Diabetes Mellitus in Beijing: Effect of Maternal Birth Weight and Other Risk Factors. Chin. Med. J. (Engl.) 2017, 130, 1019–1025. [Google Scholar] [CrossRef]
- Chatzi, L.; Garcia, R.; Roumeliotaki, T.; Basterrechea, M.; Begiristain, H.; Iñiguez, C.; Vioque, J.; Kogevinas, M.; Sunyer, J.; INMA Study Group; et al. Mediterranean diet adherence during pregnancy and risk of wheeze and eczema in the first year of life: INMA (Spain) and RHEA (Greece) mother-child cohort studies. Br. J. Nutr. 2013, 110, 2058–2068. [Google Scholar]
- Delnord, M.; Blondel, B.; Zeitlin, J. What contributes to disparities in the preterm birth rate in European countries? Curr. Opin. Obstet. Gynecol. 2015, 27, 133–142. [Google Scholar] [CrossRef]
- Morrison, J.L.; Regnault, T.R. Nutrition in pregnancy: Optimising maternal diet and fetal adaptations to altered nutrient supply. Nutrients 2016, 8, 342. [Google Scholar] [CrossRef]
- Murphy, M.M.; Stettler, N.; Smith, K.M.; Reiss, R. Associations of consumption of fruits and vegetables during pregnancy with infant birth weight or small for gestational age births: A systematic review of the literature. Int. J. Womens Healt. 2014, 6, 899–912. [Google Scholar] [CrossRef]
- Timmermans, S.; Steegers-Theunissen, R.P.; Vujkovic, M.; den Breeijen, H.; Russcher, H.; Lindemans, J.; Mackenbach, J.; Hofman, A.; Lesaffre, E.E.; Jaddoe, V.V.; et al. The Mediterranean diet and fetal size parameters: The Generation R Study. Br. J. Nutr. 2012, 108, 1399–1409. [Google Scholar] [CrossRef]
- Dietary Nutrition and Your Health: Dietary Guidelines for Americans 2015–2020. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 24 January 2019).
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; Lamuela-Raventos, R.M.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Dietary patterns, Mediterranean diet, and cardiovascular disease. Curr. Opin. Lipidol. 2014, 25, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Romaguera, D.; Norat, T.; Mouw, T.; May, A.M.; Bamia, C.; Slimani, N.; Travier, N.; Besson, H.; Luan, J.; Wareham, N.; et al. Adherence to the Mediterranean diet is associated with lower abdominal adiposity in European men and women. J. Nutr. 2009, 139, 1728–1737. [Google Scholar] [CrossRef] [PubMed]
- Toledo, E.; de A Carmona-Torre, F.; Alonso, A.; Puchau, B.; Zulet, M.A.; Martinez, J.A.; Martinez-Gonzalez, M.A. Hypothesis-oriented food patterns and incidence of hypertension: 6-year follow-up of the SUN (Seguimiento Universidad de Navarra) prospective cohort. Public Health Nutr. 2010, 13, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Verberne, L.; Bach-Faig, A.; Buckland, G.; Serra-Majem, L. Association between the Mediterranean diet and cancer risk: A review of observational studies. Nutr. Cancer 2010, 62, 860–870. [Google Scholar] [CrossRef]
- Castro-Quezada, I.; Roman-Vinas, B.; Serra-Majem, L. The Mediterranean diet and nutritional adequacy: A review. Nutrients 2014, 6, 231–248. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Guasch-Ferre, M.; Lee, C.H.; Estruch, R.; Clish, C.B.; Ros, E. Protective effects of the Mediterranean diet on type 2 diabetes and metabolic syndrome. J. Nutr. 2016, 146, 920S–927S. [Google Scholar] [CrossRef] [PubMed]
- He, J.R.; Yuan, M.Y.; Chen, N.N.; Lu, J.H; Hu, C.Y.; Mai, W.B.; Zhang, R.F.; Pan, Y.H.; Qiu, L.; Wu, Y.F.; et al. Maternal dietary patterns and gestational diabetes mellitus: A large prospective cohort study in China. Br. J. Nutr. 2015, 113, 1292–1300. [Google Scholar] [CrossRef]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Cheung, N.W.; Markovic, T.; Ross, G.; Senior, A.; Brand-Miller, J.C.; et al. Associations of diet and physical activity with risk for gestational diabetes mellitus: A systematic review and meta-analysis. Nutrients 2018, 10, 698. [Google Scholar] [CrossRef]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary patterns during pregnancy are associated with risk of gestational diabetes mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef]
- Tryggvadottir, E.A.; Medek, H.; Birgisdottir, B.E.; Geirsson, R.T.; Gunnarsdottir, I. Association between healthy maternal dietary pattern and risk for gestational diabetes mellitus. Eur. J. Clin. Nutr. 2016, 70, 237–242. [Google Scholar] [CrossRef]
- Izadi, V.; Tehrani, H.; Haghighatdoost, F.; Dehghan, A.; Surkan, P.J.; Azadbakht, L. Adherence to the DASH and Mediterranean diets is associated with decreased risk for gestational diabetes mellitus. Nutrition 2016, 32, 1092–1096. [Google Scholar] [CrossRef] [PubMed]
- Karamanos, B.; Thanopoulou, A.; Anastasiou, E.; Assaad-Khalil, S.; Albache, N.; Bachaoui, M.; Slama, C.B.; El Ghomari, H.; Jotic, A.; Lalic, N.; et al. Relation of the Mediterranean diet with the incidence of gestational diabetes. Eur. J. Clin. Nutr. 2014, 68, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Tobias, D.K.; Zhang, C.; Chavarro, J.; Bowers, K.; Rich-Edwards, J.; Rosner, B.; Mozaffarian, D.; Hu, F.B. Prepregnancy adherence to dietary patterns and lower risk of gestational diabetes mellitus. Am. J. Clin. Nutr. 2012, 96, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Gicevic, S.; Gaskins, A.J.; Fung, T.T.; Rosner, B.; Tobias, D.K.; Isanaka, S.; Willett, W.C. Evaluating pre-pregnancy dietary diversity vs. dietary quality scores as predictors of gestational diabetes and hypertensive disorders of pregnancy. PloS ONE 2018, 13, e0195103. [Google Scholar] [CrossRef] [PubMed]
- Schoenaker, D.A.; Soedamah-Muthu, S.S.; Callaway, L.K.; Mishra, G.D. Pre-pregnancy dietary patterns and risk of gestational diabetes mellitus: Results from an Australian population-based prospective cohort study. Diabetologia 2015, 58, 2726–2735. [Google Scholar] [CrossRef] [PubMed]
- Donazar-Ezcurra, M.; Lopez-Del Burgo, C.; Martinez-Gonzalez, M.A.; Basterra-Gortari, F.J; de Irala, J.; Bes-Rastrollo, M. Pre-pregnancy adherences to empirically derived dietary patterns and gestational diabetes risk in a Mediterranean cohort: The Seguimiento Universidad de Navarra (SUN) project. Br. J. Nutr. 2017, 118, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Junta de Andalucıa. Manual de atencion al embarazo, parto y puerperio [Guidelines for Pregnancy, Delivery and Puerperium Care]; Direccion General de Salud Pública: València, Spain,, 2006.
- Gonzalez, C.A.; Argilaga, S.; Agudo, A.; Amiano, P.; Barricarte, A.; Beguiristain, J.M.; Chirlaque, M.D.; Dorronsoro, M.; Martinez, C.; Navarro, C.; et al. Sociodemographic differences in adherence to the Mediterranean dietary pattern in Spanish populations. Gac. Sanit. 2002, 16, 214–221. [Google Scholar] [PubMed]
- Kelsey, J.L.; Thompson, W.D.; Evans, A.S. Methods in Observational Epidemiology; Oxford University Press: New York, NY, USA, 1986. [Google Scholar]
- National Diabetes Data Group. Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 1979, 28, 1039–1057. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B.; Grupo Colaborativo de la SEEDO. SEEDO 2007 Consensus for the evaluation of overweight and obesity and the establishment of therapeutic intervention criteria. Med. Clin. (Barc.) 2007, 10, 184–196. [Google Scholar] [CrossRef]
- Willett, W.; Stampfer, M. Implications of total energy intake for epidemiologic analyses. In Nutritional Epidemiology, 2nd ed.; Willett, W., Ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Cespedes, E.M.; Hu, F.B. Dietary patterns: From nutritional epidemiologic analysis to national guidelines. Am. J. Clin. Nutr. 2015, 101, 899–900. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Roman-Viñas, B.; Ribas Barba, L.; Ngo, J.; Martínez-González, M.A; Wijnhoven, T.M.; Serra-Majem, L. Validity of dietary patterns to assess nutrient intake adequacy. Br. J. Nutr. 2009, 101, S12–S20. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Al Wattar, B.H.; Dodds, J.; Placzek, A.; Spyreli, E.; Moore, A.; Hooper, R.; Beresford, L.; Roseboom, T.J.; Bes-Rastrollo, M.; Hitman, G.; et al. Effect of simple, targeted diet in pregnant women with metabolic risk factors on maternal and fetal outcomes (ESTEEM): Study protocol for a pragmatic multicentre randomised trial. BMJ Open 2016, 6, e013495. [Google Scholar] [CrossRef] [PubMed]
- Assaf-Balut, C.; Garcia de la Torre, N.; Duran, A.; Fuentes, M.; Bordiú, E.; Del Valle, L.; Familiar, C.; Ortolá, A.; Jiménez, I.; Herraiz, M.A.; et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): A randomized controlled trial: The St. Carlos GDM prevention study. PloS ONE 2017, 12, e0185873. [Google Scholar] [CrossRef]
- Perez-Ferre, N.; Del Valle, L.; Torrejon, M.J.; Barca, I.; Calvo, M.I.; Matía, P.; Rubio, M.A.; Calle-Pascual, A.L. Diabetes mellitus and abnormal glucose tolerance development after gestational diabetes: A three-year, prospective, randomized, clinical-based, Mediterranean lifestyle interventional study with parallel groups. Clin. Nutr. 2015, 34, 579–585. [Google Scholar] [CrossRef]
- Jacques, P.F.; Tucker, K.L. Are dietary patterns useful for understanding the role of diet in chronic disease? Am. J. Clin. Nutr. 2001, 73, 1–2. [Google Scholar] [CrossRef]
- Aune, D.; Ursin, G.; Veierod, M.B. Meat consumption and the risk of type 2 diabetes: A systematic review and meta-analysis of cohort studies. Diabetologia 2009, 52, 2277–2287. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Cases (n = 291) | Controls (n = 1175) | p Value | |
|---|---|---|---|
| Age (Mean; SD) | 33.50; SD = 5.5 | 29.80; SD = 5.1 | <0.001 |
| (Years) | n (%) | n (%) | |
| <25 | 18 (6.2) | 178 (15.2) | |
| 25–29 | 49 (16.8) | 345 (29.4) | |
| 30–34 | 91 (31.3) | 436 (37.1) | |
| ≥35 | 133 (45.7) | 216 (18.3) | |
| Education | 0.140 | ||
| University | 80 (27.5) | 358 (30.5) | |
| Secondary | 74 (25.4) | 339 (28.8) | |
| Primary | 137 (47.1) | 478 (40.7) | |
| Employment | <0.001 | ||
| Work outside the home | 94 (32.4) | 558 (47.5) | |
| Unemployment | 24 (8.3) | 84 (7.2) | |
| Sick leave in pregnancy | 61 (21.0) | 105 (8.9) | |
| Retired | 2 (0.7) | 6 (0.5) | |
| Housewife | 109 (37.6) | 421 (35.9) | |
| Antecedents of Diabetes Mellitus | 135 (46.4) | 300 (25.5) | <0.001 |
| Previous Gestational Diabetes Mellitus | 58 (19.9) | 23 (1.9) | <0.001 |
| Gravidity | <0.001 | ||
| 0 | 106 (36.4) | 555 (47.2) | |
| 1 | 89 (30.6) | 365 (31.1) | |
| 2 | 57 (19.6) | 168 (14.3) | |
| 3 | 22 (7.6) | 61 (5.2) | |
| ≥4 | 17 (5.8) | 26 (2.2) | |
| Parity | <0.001 | ||
| 0 | 146 (50.2) | 631 (53.7) | |
| 1 | 85 (29.2) | 416 (35.4) | |
| 2 | 42 (14.4) | 108 (9.2) | |
| ≥3 | 18 (6.2) | 20 (1.7) | |
| Miscarriage | <0.001 | ||
| 0 | 201 (69.1) | 933 (79.4) | |
| 1 | 69 (23.7) | 199 (16.9) | |
| ≥2 | 21 (7.2) | 43 (3.7) | |
| History of macrosomia | 10 (3.4) | 37 (3.1) | 0.062 |
| Body Mass Index (kg/m2) | <0.001 | ||
| (Mean; SD) | 27.62; SD = 6.2 | 24.22; SD = 4.5 | |
| 18.5–24.9 | 117 (40.2) | 789 (67.2) | |
| 25–29.9 | 83 (28.5) | 268 (22.8) | |
| ≥30 | 91 (31.8) | 118 (10.0) | |
| Smoking | 0.161 | ||
| Never | 110 (37.8) | 504 (42.9) | |
| Ex-smoker | 73 (25.1) | 242 (20.6) | |
| Current smoker | 108 (37.1) | 429 (36.5) | |
| Components of the MD | Cases (n = 291) Mean (SD) 95% CI p25, p50, p75 | Controls (n = 1175) Mean (SD) 95% CI p25, p50, p75 | p Value |
|---|---|---|---|
| Vegetables (g/day) | 584.14 (294.03) | 588.72 (314.88) | 0.082 |
| 550.22–618.07 | 570.69–606.74 | ||
| 355.95, 560.71, 738.09 | 345.24, 540.48, 795.24 | ||
| Fruits (g/day) | 241.34 (185.86) | 217.86 (150.69) | 0.023 |
| 219.89–262.78 | 209.24–226.49 | ||
| 125.16, 207.44, 313.86 | 111.72, 191.30, 291.36 | ||
| Legumes (g/day) | 0.23 (0.12) | 0.23 (0.13) | 0.954 |
| 0.22–0.24 | 0.22–0.24 | ||
| 0.17, 0.22, 0.27 | 0.17, 0.22, 0.27 | ||
| Cereals (g/day) | 236.47 (98.84) | 227.90 (89.02) | 0.151 |
| 225.07–247.88 | 222.80–232.99 | ||
| 173.50, 227.14, 287.14 | 162.86, 227,14, 278.57 | ||
| Fish (g/day) | 89.86 (61.59) | 80.75 (50.18) | 0.008 |
| 82.76–96.97 | 77.88–83.63 | ||
| 47.26, 74.19, 121.43 | 47.26, 70.71, 107.62 | ||
| Dairy products (g/day) | 474.31 (287.95) | 492 (283.38) | 0.342 |
| 441.09–507.53 | 475.78–508.22 | ||
| 275, 397.62, 632.26 | 286.90, 439.52, 648.80 | ||
| Meat and derivatives (g/day) | 172.92 (76.02) | 149.91 (70.65) | <0.001 |
| 164.15–181.69 | 145.87–153.95 | ||
| 119.28, 163.45, 208.69 | 103.09, 141.07, 184.28 | ||
| Ratio of monounsaturated/saturated lipids | 0.98 (0.18) | 0.92 (0.14) | 0.695 |
| 0.95–1.00 | 0.92–0.93 | ||
| 0.85, 0.94, 1.06 | 0.83, 0.91, 1.00 | ||
| Ethanol (g/day) | 0.55 (1.37) | 0.60 (1.83) | <0.001 |
| 0.39–0.71 | 0.49–0.70 | ||
| 0, 0, 0.66 | 0, 0, 0.33 |
| Components of the MD | cOR | (95 % CI) | aOR | (95% CI) | p Value |
|---|---|---|---|---|---|
| Vegetables | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 1.15 | (0.89 , 1.49) | 0.95 | (0.69 , 1.29) | 0.753 |
| Fruits | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 1.17 | (0.91, 1.52) | 0.84 | (0.62, 1.14) | 0.282 |
| Legumes | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 0.87 | (0.67, 1.13) | 0.75 | (0.55, 1.01) | 0.066 |
| Cereals | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 1.00 | (0.78, 1.30) | 0.79 | (0.58, 1.06) | 0.125 |
| Fish | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 1.00 | (0.78, 1.30) | 0.81 | (0.61, 1.08) | 0.163 |
| Dairy products | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 1.28 | (0.99, 1.66) | 1.25 | (0.95, 1.64) | 0.104 |
| Meat and derivatives | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 0.53 | (0.41, 0.70) * | 0.56 | (0.42, 0.74) * | 0.000 |
| Ratio of monounsaturated/saturated lipids | |||||
| ≥Median | 1 | Reference | 1 | Reference | |
| <Median | 1.35 | (1.04, 1.74) * | 1.13 | (0.85, 1.51) | 0.381 |
| Ethanol | |||||
| <5 and >25 g/day | 1 | Reference | 1 | Reference | |
| 5–25 g/day | 0.67 | (0.26, 1.73) | 0.61 | (0.21, 1.74) | 0.361 |
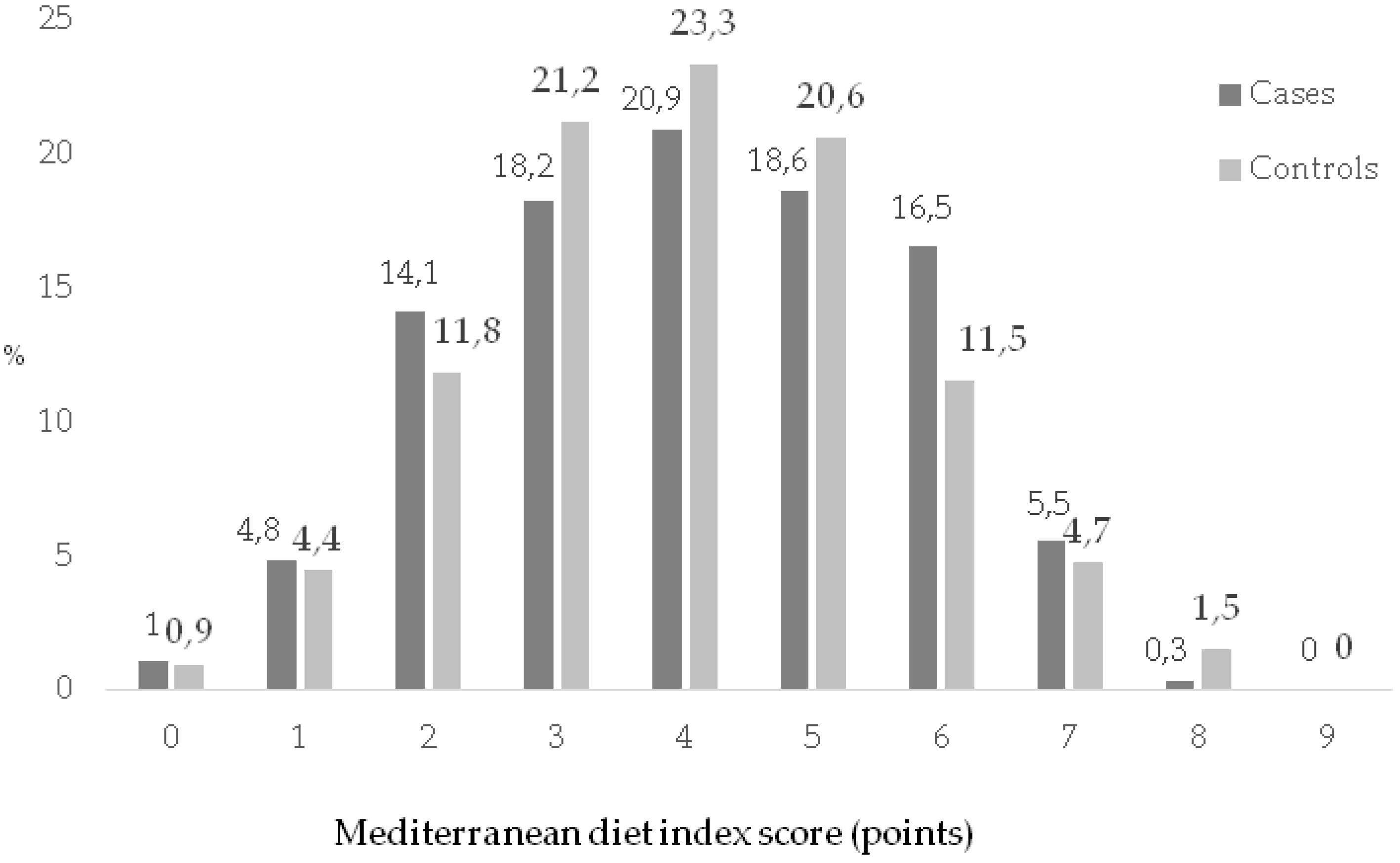
| Adherence to the MD (level) | Cases (n = 291) | Controls (n = 1175) | cOR | 95% CI | aOR | 95% CI | p Value |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | ||||||
| Low (0–2) | 58 (19.9) | 202 (17.2) | 1 | Reference | 1 | Reference | Reference |
| Middle (3–4) | 114 (39.1) | 523 (44.5) | 0.75 | (0.53, 1.08) | 0.67 | (0.44, 1.01) | 0.060 |
| High (5–6) | 102 (35.1) | 377 (32.1) | 0.94 | (0.65, 1.35) | 0.61 | (0.39, 0.94) * | 0.028 |
| Very high (≥7) | 17 (5.8) | 73 (6.2) | 0.81 | (0.44, 1.48) | 0.33 | (0.15, 0.72) * | 0.005 |
| p trend | 0.014 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olmedo-Requena, R.; Gómez-Fernández, J.; Amezcua-Prieto, C.; Mozas-Moreno, J.; Khan, K.S.; Jiménez-Moleón, J.J. Pre-Pregnancy Adherence to the Mediterranean Diet and Gestational Diabetes Mellitus: A Case-Control Study. Nutrients 2019, 11, 1003. https://doi.org/10.3390/nu11051003
Olmedo-Requena R, Gómez-Fernández J, Amezcua-Prieto C, Mozas-Moreno J, Khan KS, Jiménez-Moleón JJ. Pre-Pregnancy Adherence to the Mediterranean Diet and Gestational Diabetes Mellitus: A Case-Control Study. Nutrients. 2019; 11(5):1003. https://doi.org/10.3390/nu11051003
Chicago/Turabian StyleOlmedo-Requena, Rocío, Julia Gómez-Fernández, Carmen Amezcua-Prieto, Juan Mozas-Moreno, Khalid S. Khan, and José J. Jiménez-Moleón. 2019. "Pre-Pregnancy Adherence to the Mediterranean Diet and Gestational Diabetes Mellitus: A Case-Control Study" Nutrients 11, no. 5: 1003. https://doi.org/10.3390/nu11051003