Dietary Inflammatory Index, Dietary Non-Enzymatic Antioxidant Capacity, and Colorectal and Breast Cancer Risk (MCC-Spain Study)

 , , , , , ,
, , , , , ,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
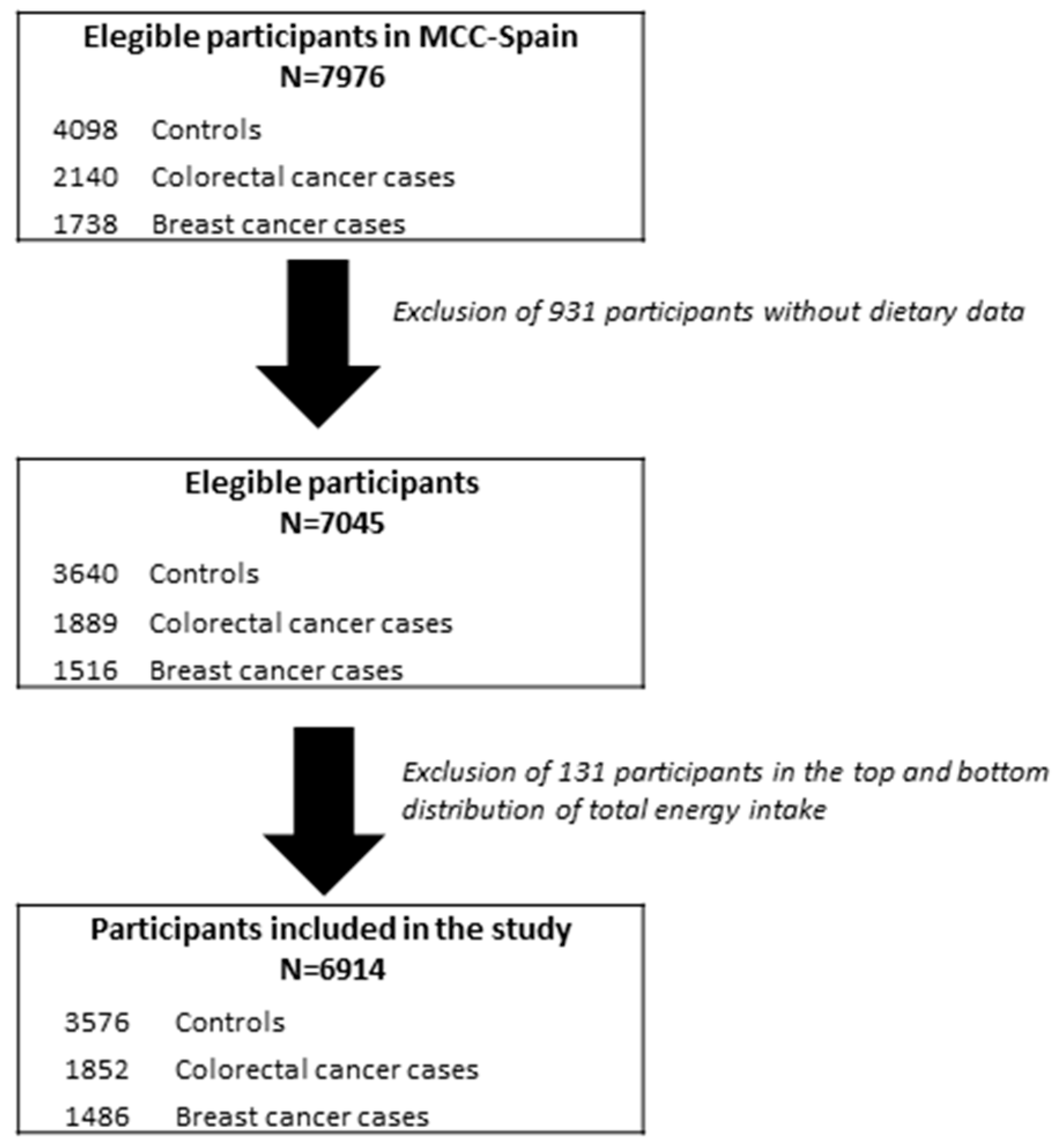
2.1. Study Population and Design
2.2. Epidemiological Data Collection
2.3. Dietary Non-Enzymatic Antioxidant Capacity and Dietary Inflammatory Index Assessment
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Cases and Controls in the MCC-Study
3.2. E-DII and Colorectal Cancer Risk
3.3. E-DII and Breast Cancer Risk
3.4. E-DII, NEAC, and Colorectal and Breast Cancer Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, H.; Chen, C. The colorectal cancer epidemic: Challenges and opportunities for primary, secondary and tertiary prevention. Br. J. Cancer 2018, 119, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Fagunwa, I.O.; Loughrey, M.B.; Coleman, H.G. Alcohol, smoking and the risk of premalignant and malignant colorectal neoplasms. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 561–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marley, A.R.; Nan, H. Epidemiology of colorectal cancer. Int. J. Mol. Epidemiol. Genet. 2016, 7, 105–114. [Google Scholar] [PubMed]
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Colorectal Cancer; World Cancer Research Fund International/American Institute for Cancer Research: Arlington, VA, USA, 2017. [Google Scholar]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2017, 26, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.M.; Rasanayagam, S.; Engel, C.; Rizzo, J. State of the evidence 2017: An update on the connection between breast cancer and the environment. Environ. Health 2017, 16. [Google Scholar] [CrossRef]
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity and Breast Cancer; World Cancer Research Fund International/American Institute for Cancer Research: Arlington, VA, USA, 2018. [Google Scholar]
- Sosa, V.; Moliné, T.; Somoza, R.; Paciucci, R.; Kondoh, H.; LLeonart, M.E. Oxidative stress and cancer: An overview. Ageing Res. Rev. 2013, 12, 376–390. [Google Scholar] [CrossRef]
- Eiró, N.; Vizoso, F.J. Inflammation and cancer. World J. Gastrointest. Surg. 2012, 4, 62–72. [Google Scholar] [CrossRef]
- Kang, D.-H. Oxidative stress, DNA damage, and breast cancer. AACN Clin. Issues 2002, 13, 540–549. [Google Scholar] [CrossRef]
- Carini, F.; Mazzola, M.; Rappa, F.; Jurjus, A.; Geagea, A.G.; Al Kattar, S.; Bou-Assi, T.; Jurjus, R.; Damiani, P.; Leone, A.; et al. Colorectal Carcinogenesis: Role of Oxidative Stress and Antioxidants. Anticancer Res. 2017, 37, 4759–4766. [Google Scholar] [PubMed] [Green Version]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartsch, H.; Nair, J. Chronic inflammation and oxidative stress in the genesis and perpetuation of cancer: Role of lipid peroxidation, DNA damage, and repair. Langenbecks Arch. Surg. 2006, 391, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- Haghighatdoost, F.; Bellissimo, N.; Totosy de Zepetnek, J.O.; Rouhani, M.H. Association of vegetarian diet with inflammatory biomarkers: A systematic review and meta-analysis of observational studies. Public Health Nutr. 2017, 20, 2713–2721. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R. Anti-inflammatory effects of the Mediterranean diet: The experience of the PREDIMED study. Proc. Nutr. Soc. 2010, 69, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef]
- Wirth, M.D.; Shivappa, N.; Davis, L.; Hurley, T.G.; Ortaglia, A.; Drayton, R.; Blair, S.N.; Hébert, J.R. Construct Validation of the Dietary Inflammatory Index among African Americans. J. Nutr. Health Aging 2017, 21, 487–491. [Google Scholar] [CrossRef]
- Shivappa, N.; Wirth, M.D.; Murphy, E.A.; Hurley, T.G.; Hébert, J.R. Association between the Dietary Inflammatory Index (DII) and urinary enterolignans and C-reactive protein from the National Health and Nutrition Examination Survey-2003–2008. Eur. J. Nutr. 2019, 58, 797–805. [Google Scholar] [CrossRef]
- Bodén, S.; Wennberg, M.; Van Guelpen, B.; Johansson, I.; Lindahl, B.; Andersson, J.; Shivappa, N.; Hebert, J.R.; Nilsson, L.M. Dietary inflammatory index and risk of first myocardial infarction; a prospective population-based study. Nutr. J. 2017, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.-E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; González-Gil, E.; Frederic, G.; et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.L.; Norhaizan, M.E.; Liew, W.-P.-P. Nutrients and Oxidative Stress: Friend or Foe? Oxid. Med. Cell. Longev. 2018, 2018. [Google Scholar] [CrossRef]
- Serafini, M.; Del Rio, D. Understanding the association between dietary antioxidants, redox status and disease: Is the Total Antioxidant Capacity the right tool? Redox Rep. Commun. Free Radic. Res. 2004, 9, 145–152. [Google Scholar] [CrossRef]
- Amiano, P.; Molina-Montes, E.; Molinuevo, A.; Huerta, J.-M.; Romaguera, D.; Gracia, E.; Martín, V.; Castaño-Vinyals, G.; Pérez-Gómez, B.; Moreno, V.; et al. Association study of dietary non-enzymatic antioxidant capacity (NEAC) and colorectal cancer risk in the Spanish Multicase-Control Cancer (MCC-Spain) study. Eur. J. Nutr. 2018. [Google Scholar] [CrossRef]
- Shivappa, N.; Godos, J.; Hébert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary Inflammatory Index and Colorectal Cancer Risk-A Meta-Analysis. Nutrients 2017, 9, 1043. [Google Scholar] [CrossRef]
- Namazi, N.; Larijani, B.; Azadbakht, L. Association between the dietary inflammatory index and the incidence of cancer: A systematic review and meta-analysis of prospective studies. Public Health 2018, 164, 148–156. [Google Scholar] [CrossRef]
- Shivappa, N.; Sandin, S.; Löf, M.; Hébert, J.R.; Adami, H.-O.; Weiderpass, E. Prospective study of dietary inflammatory index and risk of breast cancer in Swedish women. Br. J. Cancer 2015, 113, 1099–1103. [Google Scholar] [CrossRef] [Green Version]
- Ge, I.; Rudolph, A.; Shivappa, N.; Flesch-Janys, D.; Hébert, J.R.; Chang-Claude, J. Dietary inflammation potential and postmenopausal breast cancer risk in a German case-control study. Breast (Edinb. Scotl.) 2015, 24, 491–496. [Google Scholar] [CrossRef]
- Vece, M.M.; Agnoli, C.; Grioni, S.; Sieri, S.; Pala, V.; Pellegrini, N.; Frasca, G.; Tumino, R.; Mattiello, A.; Panico, S.; et al. Dietary Total Antioxidant Capacity and Colorectal Cancer in the Italian EPIC Cohort. PLoS ONE 2015, 10, e0142995. [Google Scholar] [CrossRef] [PubMed]
- Mekary, R.A.; Wu, K.; Giovannucci, E.; Sampson, L.; Fuchs, C.; Spiegelman, D.; Willett, W.C.; Smith-Warner, S.A. Total antioxidant capacity intake and colorectal cancer risk in the Health Professionals Follow-up Study. Cancer Causes Control 2010, 21, 1315–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Vecchia, C.; Decarli, A.; Serafini, M.; Parpinel, M.; Bellocco, R.; Galeone, C.; Bosetti, C.; Zucchetto, A.; Polesel, J.; Lagiou, P.; et al. Dietary total antioxidant capacity and colorectal cancer: A large case-control study in Italy. Int. J. Cancer 2013, 133, 1447–1451. [Google Scholar] [CrossRef] [PubMed]
- Karimi, Z.; Bahadoran, Z.; Abedini, S.; Houshyar-Rad, A.; Rashidkhani, B. Dietary total antioxidant capacity and the risk of breast cancer: A case-control study. East. Mediterr. Health J. Rev. (Sante Mediterr. Orient. Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit) 2015, 21, 564–571. [Google Scholar] [CrossRef]
- Pantavos, A.; Ruiter, R.; Feskens, E.F.; de Keyser, C.E.; Hofman, A.; Stricker, B.H.; Franco, O.H.; Kiefte-de Jong, J.C. Total dietary antioxidant capacity, individual antioxidant intake and breast cancer risk: The Rotterdam Study. Int. J. Cancer 2015, 136, 2178–2186. [Google Scholar] [CrossRef]
- Castaño-Vinyals, G.; Aragonés, N.; Pérez-Gómez, B.; Martín, V.; Llorca, J.; Moreno, V.; Altzibar, J.M.; Ardanaz, E.; de Sanjosé, S.; Jiménez-Moleón, J.J.; et al. Population-based multicase-control study in common tumors in Spain (MCC-Spain): Rationale and study design. Gac. Sanit. 2015, 29, 308–315. [Google Scholar] [CrossRef] [PubMed]
- García-Closas, R.; García-Closas, M.; Kogevinas, M.; Malats, N.; Silverman, D.; Serra, C.; Tardón, A.; Carrato, A.; Castaño-Vinyals, G.; Dosemeci, M.; et al. Food, nutrient and heterocyclic amine intake and the risk of bladder cancer. Eur. J. Cancer 2007, 43, 1731–1740. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Farran, A.; Zamora, R.; Cervera, P. CESNID. Tablas de Composicion de Alimentos del CESNID.; McGraw-Hill Interamericana: Madrid, Spain, 2004. [Google Scholar]
- Harmon, B.E.; Wirth, M.D.; Boushey, C.J.; Wilkens, L.R.; Draluck, E.; Shivappa, N.; Steck, S.E.; Hofseth, L.; Haiman, C.A.; Le Marchand, L.; et al. The Dietary Inflammatory Index Is Associated with Colorectal Cancer Risk in the Multiethnic Cohort. J. Nutr. 2017, 147, 430–438. [Google Scholar] [CrossRef]
- Shivappa, N.; Prizment, A.E.; Blair, C.K.; Jacobs, D.R.; Steck, S.E.; Hébert, J.R. Dietary inflammatory index and risk of colorectal cancer in the Iowa Women’s Health Study. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2014, 23, 2383–2392. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Ma, Y.; Liese, A.D.; Zhang, J.; Caan, B.; Hou, L.; Johnson, K.C.; Mossavar-Rahmani, Y.; Shivappa, N.; et al. The association between dietary inflammatory index and risk of colorectal cancer among postmenopausal women: Results from the Women’s Health Initiative. Cancer Causes Control 2015, 26, 399–408. [Google Scholar] [CrossRef]
- Wirth, M.D.; Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hébert, J.R. The dietary inflammatory index is associated with colorectal cancer in the National Institutes of Health-American Association of Retired Persons Diet and Health Study. Br. J. Nutr. 2015, 113, 1819–1827. [Google Scholar] [CrossRef]
- Kim, J.; Cho, Y.A.; Kim, D.-H.; Lee, B.-H.; Hwang, D.-Y.; Jeong, J.; Lee, H.-J.; Matsuo, K.; Tajima, K.; Ahn, Y.-O. Dietary intake of folate and alcohol, MTHFR C677T polymorphism, and colorectal cancer risk in Korea. Am. J. Clin. Nutr. 2012, 95, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Sharma, I.; Zhu, Y.; Woodrow, J.R.; Mulay, S.; Parfrey, P.S.; Mclaughlin, J.R.; Hebert, J.R.; Shivappa, N.; Li, Y.; Zhou, X.; et al. Inflammatory diet and risk for colorectal cancer: A population-based case-control study in Newfoundland, Canada. Nutrition (Burbank Los Angel. Cty. Calif.) 2017, 42, 69–74. [Google Scholar] [CrossRef]
- Shivappa, N.; Hébert, J.R.; Steck, S.E.; Hofseth, L.J.; Shehadah, I.; Bani-Hani, K.E.; Al-Jaberi, T.; Al-Nusairr, M.; Heath, D.; Tayyem, R. Dietary inflammatory index and odds of colorectal cancer in a case-control study from Jordan. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2017, 42, 744–749. [Google Scholar] [CrossRef]
- Shivappa, N.; Zucchetto, A.; Montella, M.; Serraino, D.; Steck, S.E.; La Vecchia, C.; Hébert, J.R. Inflammatory potential of diet and risk of colorectal cancer: A case-control study from Italy. Br. J. Nutr. 2015, 114, 152–158. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Shivappa, N.; Steck, S.E.; Canzian, F.; Landi, S.; Alonso, M.H.; Hébert, J.R.; Moreno, V. Dietary inflammatory index and inflammatory gene interactions in relation to colorectal cancer risk in the Bellvitge colorectal cancer case-control study. Genes Nutr. 2015, 10, 447. [Google Scholar] [CrossRef]
- Fan, Y.; Jin, X.; Man, C.; Gao, Z.; Wang, X. Meta-analysis of the association between the inflammatory potential of diet and colorectal cancer risk. Oncotarget 2017, 8, 59592–59600. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, W.; Zhang, D. Association Between Dietary Inflammation Index and The Risk of Colorectal Cancer: A Meta-Analysis. Nutr. Cancer 2018, 70, 14–22. [Google Scholar] [CrossRef]
- Wirth, M.; Burch, J.; Shivappa, N.; Violanti, J.M.; Burchfiel, C.M.; Fekedulegn, D.; Andrew, M.E.; Hartley, T.A.; Miller, D.B.; Mnatsakanova, A.; et al. Association of a Dietary Inflammatory Index with Inflammatory Indices and the Metabolic Syndrome among Police Officers. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2014, 56, 986–989. [Google Scholar] [CrossRef]
- Castelló, A.; Amiano, P.; Fernández de Larrea, N.; Martín, V.; Alonso, M.H.; Castaño-Vinyals, G.; Pérez-Gómez, B.; Olmedo-Requena, R.; Guevara, M.; Fernandez-Tardon, G.; et al. Low adherence to the western and high adherence to the Mediterranean dietary patterns could prevent colorectal cancer. Eur. J. Nutr. 2018, 58, 1495–1505. [Google Scholar] [CrossRef]
- Allen, M.D.; Jones, L.J. The role of inflammation in progression of breast cancer: Friend or foe? (Review). Int. J. Oncol. 2015, 47, 797–805. [Google Scholar] [CrossRef]
- Graffouillère, L.; Deschasaux, M.; Mariotti, F.; Neufcourt, L.; Shivappa, N.; Hébert, J.R.; Wirth, M.D.; Latino-Martel, P.; Hercberg, S.; Galan, P.; et al. The Dietary Inflammatory Index Is Associated with Prostate Cancer Risk in French Middle-Aged Adults in a Prospective Study. J. Nutr. 2016, 146, 785–791. [Google Scholar] [CrossRef]
- Shivappa, N.; Blair, C.K.; Prizment, A.E.; Jacobs, D.R.; Hébert, J.R. Prospective study of the dietary inflammatory index and risk of breast cancer in postmenopausal women. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Liese, A.D.; Zhang, J.; Ma, Y.; Caan, B.; Chlebowski, R.T.; Freudenheim, J.L.; Hou, L.; Mossavar-Rahmani, Y.; et al. Association between dietary inflammatory potential and breast cancer incidence and death: Results from the Women’s Health Initiative. Br. J. Cancer 2016, 114, 1277–1285. [Google Scholar] [CrossRef]
- Huang, W.-Q.; Mo, X.-F.; Ye, Y.-B.; Shivappa, N.; Lin, F.-Y.; Huang, J.; Hébert, J.R.; Yan, B.; Zhang, C.-X. A higher Dietary Inflammatory Index score is associated with a higher risk of breast cancer among Chinese women: A case-control study. Br. J. Nutr. 2017, 117, 1358–1367. [Google Scholar] [CrossRef]
- Shivappa, N.; Hébert, J.R.; Rosato, V.; Montella, M.; Serraino, D.; La Vecchia, C. Association between the dietary inflammatory index and breast cancer in a large Italian case-control study. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Gardeazabal, I.; Ruiz-Canela, M.; Sánchez-Bayona, R.; Romanos-Nanclares, A.; Aramendía-Beitia, J.M.; Shivappa, N.; Hébert, J.R.; Martínez-González, M.A.; Toledo, E. Dietary inflammatory index and incidence of breast cancer in the SUN project. Clin. Nutr. (Edinb. Scotl.) 2018. [Google Scholar] [CrossRef]
- Vahid, F.; Shivappa, N.; Hatami, M.; Sadeghi, M.; Ameri, F.; Naeini, Y.J.; Hebert, J.R.; Davoodi, S.H. Association between Dietary Inflammatory Index (DII) and Risk of Breast Cancer: A Case-Control Study. Asian Pac. J. Cancer Prev. 2018, 19, 1215–1221. [Google Scholar]
- Jalali, S.; Shivappa, N.; Hébert, J.R.; Heidari, Z.; Hekmatdoost, A.; Rashidkhani, B. Dietary Inflammatory Index and Odds of Breast Cancer in a Case-Control Study from Iran. Nutr. Cancer 2018, 70, 1034–1042. [Google Scholar] [CrossRef]
- Jayedi, A.; Emadi, A.; Shab-Bidar, S. Dietary Inflammatory Index and Site-Specific Cancer Risk: A Systematic Review and Dose-Response Meta-Analysis. Adv. Nutr. (Bethesda Md.) 2018, 9, 388–403. [Google Scholar] [CrossRef]
- Moradi, S.; Issah, A.; Mohammadi, H.; Mirzaei, K. Associations between dietary inflammatory index and incidence of breast and prostate cancer: A systematic review and meta-analysis. Nutrition (Burbank Los Angel. Cty. Calif.) 2018, 55–56, 168–178. [Google Scholar] [CrossRef]
- Wang, L.; Liu, C.; Zhou, C.; Zhuang, J.; Tang, S.; Yu, J.; Tian, J.; Feng, F.; Liu, L.; Zhang, T.; et al. Meta-analysis of the association between the dietary inflammatory index (DII) and breast cancer risk. Eur. J. Clin. Nutr. 2019, 73, 509–517. [Google Scholar] [CrossRef]
- World Cancer Research Fund International/American Institute for Cancer Research. Continuous Update Project Expert Report 2018. Alcoholic Drinks and the Risk of Cancer; World Cancer Research Fund International/American Institute for Cancer Research: Arlington, VA, USA, 2018. [Google Scholar]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Pavlova, N.N.; Thompson, C.B. The Emerging Hallmarks of Cancer Metabolism. Cell Metab. 2016, 23, 27–47. [Google Scholar] [CrossRef] [Green Version]
- Federico, A.; Morgillo, F.; Tuccillo, C.; Ciardiello, F.; Loguercio, C. Chronic inflammation and oxidative stress in human carcinogenesis. Int. J. Cancer 2007, 121, 2381–2386. [Google Scholar] [CrossRef]
- Boldo, E.; Castelló, A.; Aragonés, N.; Amiano, P.; Pérez-Gómez, B.; Castaño-Vinyals, G.; Martín, V.; Guevara, M.; Urtiaga, C.; Dierssen-Sotos, T.; et al. Meat intake, methods and degrees of cooking and breast cancer risk in the MCC-Spain study. Maturitas 2018, 110, 62–70. [Google Scholar] [CrossRef] [Green Version]
- Hébert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII)-Lessons Learned, Improvements Made, and Future Directions. Adv. Nutr. (Bethesda Md.) 2019, 10, 185–195. [Google Scholar] [CrossRef]
- Rafiee, P.; Shivappa, N.; Hébert, J.R.; Nasab, S.J.; Bahrami, A.; Hekmatdoost, A.; Rashidkhani, B.; Sadeghi, A.; Houshyari, M.; Hejazi, E. Dietary Inflammatory Index and Odds of Colorectal Cancer and Colorectal Adenomatous Polyps in A Case-Control Study from Iran. Nutrients 2019, 11, 1213. [Google Scholar] [CrossRef]


{kind=link}
| Colorectal Cancer Study (n = 5299) | Breast Cancer Study (n = 3138) | |||||
|---|---|---|---|---|---|---|
| Controls | CRC Cases | p-Value 1 | Controls | BC Cases | p-Value 1 | |
| mean(sd)/N(%) | mean(sd)/N(%) | mean(sd)/N(%) | mean(sd)/N(%) | |||
| Sex | ||||||
| Male | 1781 (51.7%) | 1183 (63.9%) | <0.001 | - | - | |
| Female | 1666 (48.3%) | 669 (36.1%) | 1652 (52.6) | 1486 (47.4) | ||
| E-DII score | −0.39 (1.9) | 0.03 (1.9) | <0.001 | −0.75 (1.8) | −0.50 (1.9) | <0.001 |
| Total dietary NEAC (without coffee) | ||||||
| TEAC (µmol TE/day) | 4.01 (1.83) | 3.96 (1.82) | 0.33 | 3.74 (1.68) | 3.75 (1.72) | 0.98 |
| Age (years) | 63.2 (11.7) | 66.8 (10.6) | <0.0012 | 59.0 (13.0) | 56.2 (12.4) | <0.001 |
| BMI (kg/m2) | 26.6 (4.4) | 27.6 (4.5) | <0.001 | 25.7 (4.8) | 25.9 (4.6) | 0.40 |
| Energy intake (without alcohol; kcal/day) | 1805 (535) | 1900 (588) | <0.001 | 1727 (499) | 1808 (529) | <0.001 |
| Ethanol intake (g/day) | 11.0 (15.9) | 12.0 (19.3) | <0.0012 | 4.97 (8.2) | 5.16 (9.3) | 0.29 2 |
| Physical activity | ||||||
| Inactive | 1316 (38.6%) | 949 (51.2%) | <0.001 | 628 (38.3%) | 613 (41.3%) | 0.40 |
| Moderately active | 501 (14.7%) | 214 (11.6%) | 305 (18.6%) | 256 (17.2%) | ||
| Active | 416 (12.2%) | 159 (8.59%) | 214 (13.1%) | 190 (12.8%) | ||
| Very active | 1178 (34.5%) | 530 (28.6%) | 491 (30.0%) | 427 (28.7%) | ||
| Education level | ||||||
| Less than primary | 604 (17.5%) | 578 (31.2%) | <0.001 | 272 (16.5%) | 209 (14.1%) | 0.07 |
| Primary | 1120 (32.5%) | 715 (38.6%) | 500 (30.3%) | 491 (33.0%) | ||
| High school | 992 (28.8%) | 373 (20.1%) | 520 (31.5%) | 492 (33.1%) | ||
| University | 731 (21.2%) | 186 (10.0%) | 360 (21.8%) | 294 (19.8%) | ||
| Tobacco smoking | ||||||
| Never smoker | 1522 (44.3%) | 766 (41.6%) | <0.001 | 991 (60.1%) | 822 (55.5%) | 0.004 |
| Former smoker | 1204 (35.1%) | 747 (40.6%) | 330 (20.0%) | 294 (19.8%) | ||
| Current smoker | 709 (20.6%) | 329 (17.9%) | 329 (19.9%) | 366 (24.7%) | ||
| Family history 3 | ||||||
| Yes | 297 (8.62%) | 304 (16.4%) | <0.001 | 144 (8.72%) | 218 (14.7%) | <0.001 |
| No | 2960 (85.9%) | 1415 (76.4%) | 1441 (87.2%) | 1232 (82.9%) | ||
| Missing-Unknown | 190 (5.5%) | 133 (7.2%) | 67 (4.1%) | 36 (2.4%) | ||
| Use of NSAIDs/aspirin | ||||||
| Yes | 1334 (38.7%) | 604 (32.6%) | <0.001 | - | - | |
| No | 2000 (58.0%) | 1184 (63.9%) | - | - | ||
| Missing | 113 (3.3%) | 64 (3.46%) | ||||
| Hormone replacement therapy use | ||||||
| Never | - | - | 1469 (88.9%) | 1347 (90.6%) | 0.15 | |
| Ever | - | - | 126 (7.6%) | 104 (7.0%) | ||
| Not Known (or not remember) | - | - | 57 (3.5%) | 35 (2.4%) | ||
| Oral contraceptive use | ||||||
| No | - | - | 839 (50.8%) | 772 (52.0%) | 0.52 | |
| Yes | - | - | 812 (49.2%) | 712 (48.0%) | ||
| Age at menarche | ||||||
| <13 years old | - | - | 667 (40.4%) | 630 (42.4%) | <0.001 | |
| ≥13 years old | - | - | 925 (56.0%) | 837 (56.3%) | ||
| Not known | - | - | 60 (3.6%) | 19 (1.3%) | ||
| Number of children | 1.9 (1.5) | 1.7 (1.3) | <0.001 2 | |||
| Age at first pregnancy | ||||||
| Nulliparous | - | - | 310 (18.8%) | 317 (21.5%) | 0.33 | |
| <20 years | - | - | 58 (3.53%) | 59 (4.0%) | ||
| 20–24 years | - | - | 407 (24.7%) | 345 (23.4%) | ||
| 25–29 years | - | - | 537 (32.6%) | 454 (30.8%) | ||
| >29 years | - | - | 333 (20.2%) | 301 (20.4%) | ||
| Menopausal status | ||||||
| Premenopausal | - | - | 476 (28.8%) | 532 (35.8%) | <0.001 | |
| Postmenopausal | - | - | 1175 (71.2%) | 953 (64.2%) | ||
| Variables | Q1 N = 894 | Q2 N = 895 | Q3 N = 892 | Q4 N = 895 | p-Value 1 | n | |
|---|---|---|---|---|---|---|---|
| Men | (−5.11, −1.49) | (−1.49, −0.167) | (−0.167, 1.41) | (1.41, 5.47) | |||
| Women | (−5.64, −2.15) | (−2.15, −1.01) | (−1.01, 0.426) | (0.426, 5.12) | |||
| mean(sd) / N(%) | mean(sd) / N(%) | mean(sd) / N(%) | mean(sd) / N(%) | ||||
| Age | 65.3 (10.8) | 64.5 (11.1) | 63.0 (12.0) | 58.6 (13.0) | <0.001 2 | 3576 | |
| BMI (kg/m2) | 26.9 (4.4) | 26.7 (4.43) | 26.4 (4.3) | 26.4 (4.52) | 0.05 | 3576 | |
| Energy intake (without alcohol; kcal/day) | 1627 (471) | 1776 (495) | 1841 (528) | 1966 (581) | <0.001 | 3576 | |
| Ethanol intake (g/day) | 9.4 (12.8) | 9.5 (13.3) | 11.3 (16.6) | 13.6 (19.3) | <0.001 2 | 3576 | |
| Total dietary NEAC (without coffee) | |||||||
| TEAC (µmol TE/day) | 4.76 (1.95) | 4.25 (1.74) | 3.82 (1.68) | 3.17 (1.53) | <0.001 | 3450 | |
| Sex | 1 | 3576 | |||||
| Men | 455 (50.9%) | 456 (50.9%) | 455 (51.0%) | 456 (50.9%) | |||
| Women | 439 (49.1%) | 439 (49.1%) | 437 (49.0%) | 439 (49.1%) | |||
| Education | <0.001 | 3576 | |||||
| Less than primary school | 171 (19.1%) | 169 (18.9%) | 147 (16.5%) | 130 (14.5%) | |||
| Primary school | 298 (33.3%) | 299 (33.4%) | 301 (33.7%) | 245 (27.4%) | |||
| Secondary school | 241 (27.0%) | 233 (26.0%) | 259 (29.0%) | 316 (35.3%) | |||
| University | 184 (20.6%) | 194 (21.7%) | 185 (20.7%) | 204 (22.8%) | |||
| Tobacco smoking | <0.001 | 3562 | |||||
| Never smoker | 445 (49.9%) | 427 (48.0%) | 389 (43.7%) | 328 (36.8%) | |||
| Former smoker | 316 (35.5%) | 333 (37.5%) | 312 (35.1%) | 278 (31.2%) | |||
| Current smoker | 130 (14.6%) | 129 (14.5%) | 189 (21.2%) | 286 (32.1%) | |||
| Physical activity | <0.001 | 3540 | |||||
| Inactive | 314 (35.4%) | 303 (34.2%) | 336 (38.1%) | 405 (45.9%) | |||
| Moderately active | 119 (13.4%) | 137 (15.4%) | 135 (15.3%) | 139 (15.7%) | |||
| Active | 107 (12.1%) | 122 (13.8%) | 102 (11.6%) | 102 (11.6%) | |||
| Very active | 347 (39.1%) | 325 (36.6%) | 310 (35.1%) | 237 (26.8%) | |||
| Use of NSAIDs/aspirin | 0.32 | 3576 | |||||
| Yes | 346 (38.7%) | 335 (37.4%) | 353 (39.6%) | 356 (39.8%) | |||
| No | 515 (57.6%) | 522 (58.3%) | 512 (57.4%) | 519 (58.0%) | |||
| Missing | 33 (3.7%) | 38 (4.3%) | 27 (3.0%) | 20 (2.2%) | |||
| Hormone replacement therapy use | 0.01 | 1754 | |||||
| Never | 377 (85.9%) | 383 (87.2%) | 393 (89.9%) | 407 (92.7%) | |||
| Ever | 38 (8.7%) | 40 (9.1%) | 28 (6.4%) | 26 (5.9%) | |||
| Not Known (or not remember) | 24 (5.5%) | 16 (3.6%) | 16 (3.7%) | 6 (1.4%) | |||
| Oral contraceptive use | <0.001 | 1753 | |||||
| No | 251 (57.2%) | 247 (56.4%) | 209 (47.8%) | 196 (44.6%) | |||
| Yes | 188 (42.8%) | 191 (43.6%) | 228 (52.2%) | 243 (55.4%) | |||
| Age at menarche | 0.30 | 1754 | |||||
| <13 | 172 (39.2%) | 179 (40.8%) | 166 (38.0%) | 194 (44.2%) | |||
| ≥13 | 247 (56.3%) | 240 (54.7%) | 259 (59.3%) | 231 (52.6%) | |||
| Missing | 20 (4.6%) | 20 (4.6%) | 12 (2.8%) | 14 (3.2%) | |||
| Age at first pregnancy | 0.30 | 1742 | |||||
| Nulliparous | 73 (16.7%) | 83 (19.1%) | 76 (17.6%) | 91 (20.8%) | |||
| <20 years | 17 (3.9%) | 11 (2.5%) | 18 (4.2%) | 15 (3.43%) | |||
| 20–24 years | 104 (23.8%) | 122 (28.0%) | 104 (24.0%) | 103 (23.6%) | |||
| 25–29 years | 144 (33.0%) | 142 (32.6%) | 159 (36.7%) | 133 (30.4%) | |||
| >29 years | 99 (22.7%) | 77 (17.7%) | 76 (17.6%) | 95 (21.7%) | |||
| Number of children | 2.0 (1.5) | 1.9 (1.4) | 2.0 (1.5) | 1.9 (1.4) | 0.41 2 | 1750 | |
| Menopausal status | <0.001 | 1753 | |||||
| Premenopausal | 81 (18.5%) | 100 (22.8%) | 128 (29.4%) | 184 (41.9%) | |||
| Postmenopausal | 358 (81.5%) | 339 (77.2%) | 308 (70.6%) | 255 (58.1%) |
| Control/Cases | Models | E-DII Score Categories | p for Trend | p for Interaction | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Per 1-Point Increment in the E-DII Score | Q1 | Q2 | Q3 | Q4 | |||||||
| M | ≤−1.49 | (−1.49, −0.167) | (−0.167, 1.41) | >1.41 | |||||||
| W | ≤−2.15 | (−2.15, −1.01) | (−1.01, 0.426) | >0.426 | |||||||
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |||||||
| All | 3447/1852 | Simple | 1.15 (1.11–1.19) | 1.00 (ref) | 1.59 (1.33–1.89) | 1.99 (1.67–2.37) | 2.03 (1.70–2.44) | <0.001 | |||
| 3399/1842 | Final | 1.14 (1.10–1.18) | 1.00 (ref) | 1.57 (1.31–1.89) | 1.97 (1.64–2.35) | 1.93 (1.60–2.32) | <0.001 | ||||
| 3399/1596 | Sensitivity | 1.15 (1.11–1.19) | 1.00 (ref) | 1.66 (1.37–2.01) | 2.06 (1.70–2.49) | 2.02 (1.66–2.47) | <0.001 | ||||
| CRC Subtype 1 | |||||||||||
| Colon cancer | 3399/1122 | Final | 1.13 (1.08–1.17) | 1.00 (ref) | 1.53 (1.24–1.89) | 1.86 (1.51–2.30) | 1.81 (1.45–2.26) | <0.001 | |||
| Rectal cancer | 3399/700 | 1.17 (1.11–1.22) | 1.00 (ref) | 1.69 (1.29–2.22) | 2.23 (1.71–2.90) | 2.27 (1.73–2.98) | <0.001 | ||||
| Sex | |||||||||||
| Men | 1748/1174 | Stratified 1 | 1.14 (1.09–1.19) | 1.00 (ref) | 1.72 (1.36–2.18) | 2.02 (1.60–2.57) | 2.14 (1.68–2.73) | <0.001 | 0.04 | ||
| Women | 1651/668 | 1.12 (1.05–1.18) | 1.00 (ref) | 1.39 (1.05–1.86) | 1.95 (1.47–2.59) | 1.57 (1.16–2.13) | <0.001 | ||||
| BMI (kg/m2) | |||||||||||
| Normal weight | 1308/544 | Stratified 2 | 1.12 (1.06–1.19) | 1.00 (ref) | 1.52 (1.09–2.12) | 1.75 (1.26–2.44) | 1.95 (1.39–2.73) | <0.001 | 0.87 | ||
| Overweight and Obese | 2091/1298 | 1.14 (1.10–1.19) | 1.00 (ref) | 1.58 (1.27–1.97) | 2.06 (1.66–2.55) | 1.90 (1.51–2.37) | <0.001 | ||||
| Physical activity 2 | |||||||||||
| Inactive | 1310/945 | Stratified 3 | 1.17 (1.08–1.20) | 1.00 (ref) | 1.69 (1.28–2.24) | 2.31 (1.76–3.03) | 2.05 (1.55–2.70) | <0.001 | 0.52 | ||
| Active | 2089/897 | 1.15 (1.09–1.20) | 1.00 (ref) | 1.50 (1.18–1.91) | 1.78 (1.39–2.26) | 1.92 (1.49–2.47) | <0.001 | ||||
| Use of NSAIDs/aspirin | |||||||||||
| Yes | 1298/601 | Stratified 4 | 1.14 (1.07–1.20) | 1.00 (ref) | 1.73 (1.26–2.37) | 1.94 (1.42–2.65) | 1.97 (1.43–2.72) | <0.001 | 0.25 | ||
| No | 1990/1178 | 1.13 (1.08–1.18) | 1.00 (ref) | 1.49 (1.18–1.88) | 1.97 (1.57–2.47) | 1.83 (1.44–2.32) | <0.001 | ||||
| Tobacco smoking | |||||||||||
| Current/Former smokers | 1893/1076 | Stratified 5 | 1.09 (1.05–1.14) | 1.00 (ref) | 1.61 (1.26–2.07) | 1.87 (1.47–2.39) | 1.72 (1.34–2.20) | <0.001 | 0.58 | ||
| Never smokers | 1506/766 | 1.18 (1.12–1.25) | 1.00 (ref) | 1.53 (1.17–2.00) | 2.05 (1.57–2.68) | 2.11 (1.58–2.82) | <0.001 | ||||
| Control/Case | Models | E-DII Score Categories | p for Trend | p for Interaction | |||||
|---|---|---|---|---|---|---|---|---|---|
| Per 1-Point Increment in the E-DII Score | Q1 | Q2 | Q3 | Q4 | |||||
| ≤−2.15 | (−2.15, −1.01) | (−1.01, 0.426) | >0.426 | ||||||
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |||||
| All women | 1652/1486 | Simple | 1.05 (1.01–1.09) | 1.00 (ref) | 1.17 (0.95–1.45) | 1.13 (0.92–1.39) | 1.25 (1.02–1.55) | 0.06 | |
| 1628/1471 | Final | 1.04 (1.00–1.08) | 1.00 (ref) | 1.16 (0.94–1.43) | 1.13 (0.91–1.39) | 1.22 (0.99–1.52) | 0.10 | ||
| 1628/1140 | Sensitivity | 1.03 (0.99–1.08) | 1.00 (ref) | 1.17 (0.93–1.47) | 1.09 (0.87–1.37) | 1.19 (0.94–1.50) | 0.24 | ||
| BC subtypes | |||||||||
| HR+ 1 | 1628/986 | Final | 1.04 (0.99–1.09) | 1.00 (ref) | 1.17 (0.92–1.49) | 1.17 (0.93–1.49) | 1.22 (0.95–1.55) | 0.14 | |
| HER2+ 1 | 1628/251 | Final | 1.04 (0.96–1.13) | 1.00 (ref) | 1.85 (1.21–2.83) | 1.27 (0.81–1.98) | 1.56 (1.01–2.04) | 0.24 | |
| TN1 | 1628/105 | Final | 1.02 (0.91–1.14) | 1.00 (ref) | 0.67 (0.37–1.23) | 0.78 (0.44–1.39) | 0.99 (0.56–1.75) | 0.97 | |
| Menopausal status | |||||||||
| Premenopausal | 469/526 | Stratified 1 | 1.01 (0.94–1.08) | 1.00 (ref) | 0.94 (0.60–1.47) | 0.97 (0.64–1.48) | 1.05 (0.70–1.57) | 0.71 | 0.33 |
| Postmenopausal | 1159/945 | 1.06 (1.01–1.12) | 1.00 (ref) | 1.23 (0.97–1.58) | 1.19 (0.93–1.54) | 1.30 (0.99–1.69) | 0.08 | ||
| HRT use | |||||||||
| Never | 1448/1335 | Stratified 2 | 1.04 (1.00–1.08) | 1.00 (ref) | 1.16 (0.93–1.46) | 1.16 (0.92–1.45) | 1.22 (0.97–1.53) | 0.11 | 0.54 |
| Ever | 125/103 | 1.12 (0.93–1.34) | 1.00 (ref) | 0.88 (0.38–2.05) | 1.12 (0.47–2.64) | 1.47 (0.62–3.49) | 0.35 | ||
| OC use | |||||||||
| No | 828/764 | Stratified 3 | 1.05 (0.99–1.11) | 1.00 (ref) | 1.25 (0.94–1.66) | 1.35 (1.01–1.81) | 1.20 (0.88–1.63) | 0.18 | 0.87 |
| Yes | 800/707 | 1.04 (0.98–1.10) | 1.00 (ref) | 1.10 (0.79–1.52) | 0.97 (0.71–1.33) | 1.25 (0.91–1.71) | 0.25 | ||
| BMI (kg/m2) | |||||||||
| Normal weight | 843/718 | Stratified 4 | 1.04 (0.98–1.10) | 1.00 (ref) | 0.88 (0.64–1.21) | 1.01 (0.74–1.38) | 1.20 (0.88–1.63) | 0.15 | 0.99 |
| Overweight and Obese | 785/753 | 1.05 (0.99–1.12) | 1.00 (ref) | 1.49 (1.11–2.01) | 1.25 (0.93–1.68) | 1.29 (0.95–1.76) | 0.23 | ||
| Physical activity 2 | |||||||||
| Inactive | 625/608 | Stratified 5 | 1.06 (0.99–1.12) | 1.00 (ref) | 1.92 (1.33–2.78) | 1.63 (1.14–2.34) | 1.48 (1.04–2.10) | 0.13 | 0.92 |
| Active | 1003/863 | 1.03 (0.97–1.09) | 1.00 (ref) | 0.93 (0.71–1.21) | 0.90 (0.69–1.18) | 1.14 (0.86–1.51) | 0.45 | ||
| Tobacco smoking | |||||||||
| Current/Former smokers | 647/656 | Stratified 6 | 1.05 (0.98–1.11) | 1.00 (ref) | 0.85 (0.59–1.22) | 1.01 (0.71–1.44) | 1.15 (0.81–1.61) | 0.21 | 0.15 |
| Never smokers | 981/815 | 1.03 (0.97–1.09) | 1.00 (ref) | 1.40 (1.07–1.82) | 1.19 (0.91–1.57) | 1.19 (0.89–1.59) | 0.39 | ||
| Control/Case | Models | E-DII+NEAC Score Categories | pfor Trend | ||||||
| ≤2 | 3 | 4 | ≥5 | ||||||
| Per 1-Point Increment in the E-DII+NEAC Score | M: mean E-DII | −1.49 | −0.12 | 0.80 | 2.15 | ||||
| W: mean E-DII | −2.12 | −0.89 | −0.16 | 1.28 | |||||
| M: mean TEAC | 5.68 | 4.11 | 3.45 | 2.39 | |||||
| W: mean TEAC | 4.93 | 3.68 | 3.02 | 2.19 | |||||
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |||||
| CRC | 3312/1798 | Final-CRC | 1.10 (1.06–1.14) | 1.00 (ref) | 1.31 (1.10–1.55) | 1.32 (1.10–1.58) | 1.48 (1.26–1.74) | <0.001 | |
| CRC Subtype 1 | |||||||||
| Colon cancer | 3312/1100 | Final-CRC | 1.09 (1.05–1.14)1. | 1.00 (ref) | 1.31 (1.07–1.60) | 1.29 (1.04–1.60) | 1.46 (1.21–1.76) | <0.001 | |
| Rectal cancer | 3312/678 | Final-CRC | 1.11 (1.06–1.17) | 1.00 (ref) | 1.29 (1.01–1.65) | 1.34 (1.04–1.73) | 1.49 (1.19–1.87) | <0.001 | |
| BC | 1585/1418 | Final-BC | 1.02 (0.98–1.07) | 1.00 (ref) | 0.98 (0.80–1.22) | 1.03 (0.82–1.28) | 1.09 (0.90–1.32) | 0.39 | |
| Menopausal status | |||||||||
| Premenopausal | 464/506 | Stratified 1 | 0.98 (0.91–1.06) | 1.00 (ref) | 1.04 (0.68–1.57) | 0.88 (0.58–1.33) | 0.91 (0.66–1.27) | 0.50 | |
| Postmenopausal | 1121/912 | Stratified 1 | 1.05 (0.99–1.11) | 1.00 (ref) | 0.95 (0.74–1.22) | 1.12 (0.85–1.48) | 1.22 (0.95–1.56) | 0.10 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obón-Santacana, M.; Romaguera, D.; Gracia-Lavedan, E.; Molinuevo, A.; Molina-Montes, E.; Shivappa, N.; Hebert, J.R.; Tardón, A.; Castaño-Vinyals, G.; Moratalla, F.; et al. Dietary Inflammatory Index, Dietary Non-Enzymatic Antioxidant Capacity, and Colorectal and Breast Cancer Risk (MCC-Spain Study). Nutrients 2019, 11, 1406. https://doi.org/10.3390/nu11061406
Obón-Santacana M, Romaguera D, Gracia-Lavedan E, Molinuevo A, Molina-Montes E, Shivappa N, Hebert JR, Tardón A, Castaño-Vinyals G, Moratalla F, et al. Dietary Inflammatory Index, Dietary Non-Enzymatic Antioxidant Capacity, and Colorectal and Breast Cancer Risk (MCC-Spain Study). Nutrients. 2019; 11(6):1406. https://doi.org/10.3390/nu11061406
Chicago/Turabian StyleObón-Santacana, Mireia, Dora Romaguera, Esther Gracia-Lavedan, Amaia Molinuevo, Esther Molina-Montes, Nitin Shivappa, James R. Hebert, Adonina Tardón, Gemma Castaño-Vinyals, Ferran Moratalla, and et al. 2019. "Dietary Inflammatory Index, Dietary Non-Enzymatic Antioxidant Capacity, and Colorectal and Breast Cancer Risk (MCC-Spain Study)" Nutrients 11, no. 6: 1406. https://doi.org/10.3390/nu11061406