Changes in Nutritional Status and Musculoskeletal Health in a Geriatric Post-Fall Care Plan Setting

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Individuals
2.2. Demographic and Clinical Measures
2.3. Nutritional Status
2.4. Biochemical Measures
2.5. Post-Fall Care Plan
2.6. Musculoskeletal Outcome Measures
2.7. Osteopenia/Osteoporosis and Sarcopenia
2.8. Statistical Analysis
3. Results
3.1. Descriptive Characteristics, Including Change in Nutritional Status
3.2. Nutritional Status and Musculoskeletal Health at Baseline
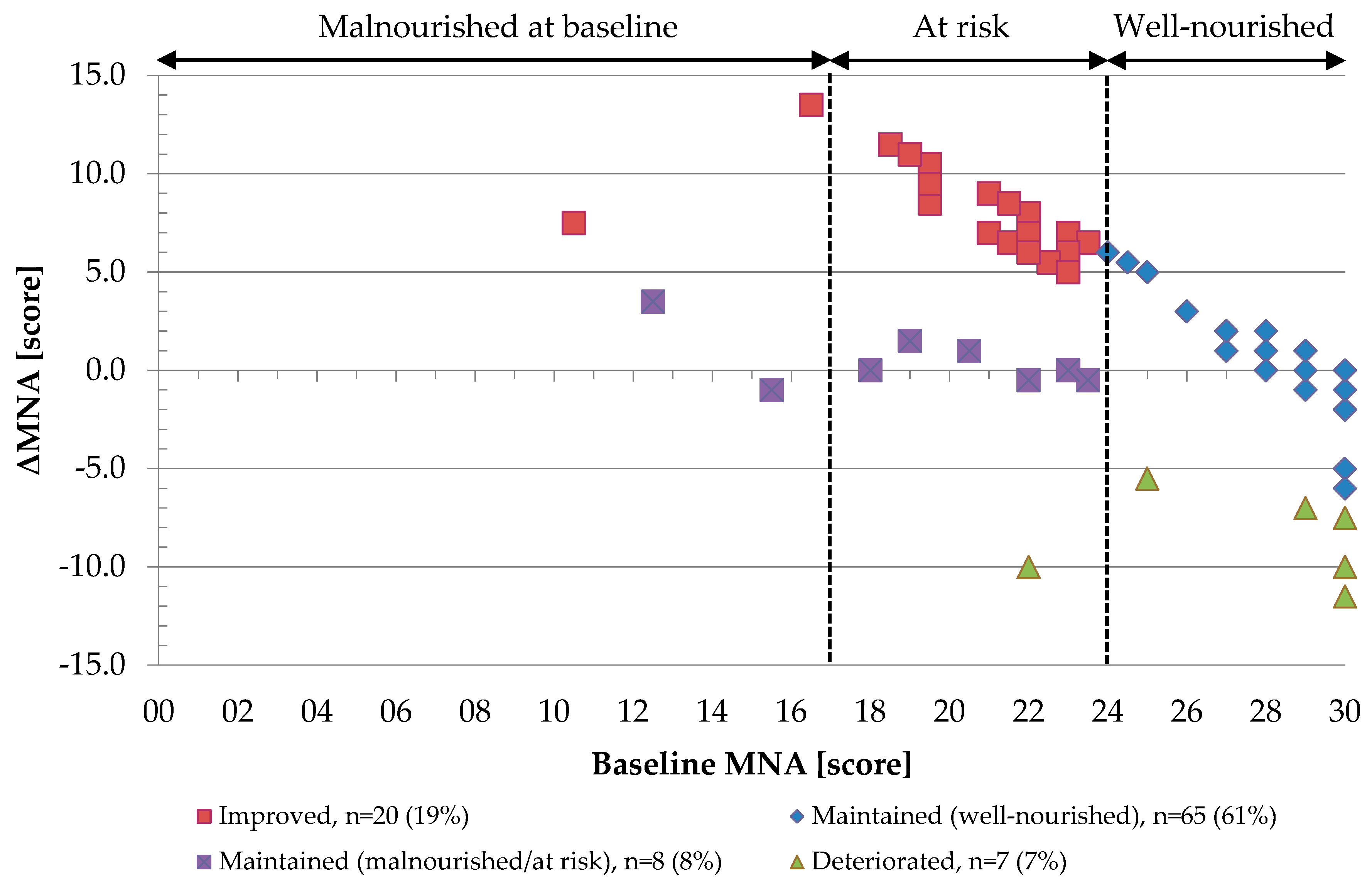
3.3. Changes in Nutritional Status and Musculoskeletal Health
4. Discussion
4.1. Changes in Nutritional Status
4.2. Changes in Nutritional Status and Musculoskeletal Health
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| 25OHD | 25-hydroxyvitamin D |
| ALM | Appendicular lean mass |
| ANZSSFR | Australian and New Zealand Society for Sarcopenia and Frailty Research |
| BMD | Bone mineral density |
| BMI | Body mass index |
| CACI | Charlson age-comorbidity index |
| CI | Confidence interval |
| CTx | C-terminal telopeptide of type 1 collagen |
| DXA | Dual energy X-ray absorptiometry |
| EWGSOP | European Working Group on Sarcopenia in Older People |
| eGFR | Estimated glomerular filtration rate |
| GDS | Geriatric Depression Scale |
| MNA | Mini Nutritional Assessment |
| PTH | Parathyroid hormone |
| Q1 | 25th percentile |
| Q3 | 75th percentile |
| SD | Standard deviation |
| SPPB | Short Physical Performance Battery |
| TUG test | Timed Up and Go test |
References
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Lamb, S.E.; Gates, S.; Cumming, R.G.; Rowe, B.H. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- WHO (World Health Organization). WHO Global Report on Falls Prevention in Older Age. Available online: https://www.who.int/ageing/publications/Falls_prevention7March.pdf (accessed on 10 May 2018).
- Torres, M.J.; Feart, C.; Samieri, C.; Dorigny, B.; Luiking, Y.; Berr, C.; Barberger-Gateau, P.; Letenneur, L. Poor nutritional status is associated with a higher risk of falling and fracture in elderly people living at home in France: the Three-City cohort study. Osteoporos. Int. 2015, 26, 2157–2164. [Google Scholar] [CrossRef]
- Trevisan, C.; Crippa, A.; Ek, S.; Welmer, A.K.; Sergi, G.; Maggi, S.; Manzato, E.; Bea, J.W.; Cauley, J.A.; Decullier, E.; et al. Nutritional Status, Body Mass Index, and the Risk of Falls in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2018. [Google Scholar] [CrossRef]
- Vellas, B.; Villars, H.; Abellan, G.; Soto, M.E.; Rolland, Y.; Guigoz, Y.; Morley, J.E.; Chumlea, W.; Salva, A.; Rubenstein, L.Z.; et al. Overview of the MNA—Its history and challenges. J. Nutr. Health Aging 2006, 10, 456–463. [Google Scholar]
- Swanenburg, J.; de Bruin, E.D.; Stauffacher, M.; Mulder, T.; Uebelhart, D. Effects of exercise and nutrition on postural balance and risk of falling in elderly people with decreased bone mineral density: randomized controlled trial pilot study. Clin. Rehabil. 2007, 21, 523–534. [Google Scholar] [CrossRef]
- Park, S.H. Tools for assessing fall risk in the elderly: a systematic review and meta-analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Vellas, B.J.; Hunt, W.C.; Romero, L.J.; Koehler, K.M.; Baumgartner, R.N.; Garry, P.J. Changes in nutritional status and patterns of morbidity among free-living elderly persons: A 10-year longitudinal study. Nutrition 1997, 13, 515–519. [Google Scholar] [CrossRef]
- Afrin, N.; Honkanen, R.; Koivumaa-Honkanen, H.; Lukkala, P.; Rikkonen, T.; Sirola, J.; Williams, L.J.; Kroger, H. Multimorbidity predicts falls differentially according to the type of fall in postmenopausal women. Maturitas 2016, 91, 19–24. [Google Scholar] [CrossRef]
- Mithal, A.; Bonjour, J.P.; Boonen, S.; Burckhardt, P.; Degens, H.; El Hajj Fuleihan, G.; Josse, R.; Lips, P.; Morales Torres, J.; Rizzoli, R.; et al. Impact of nutrition on muscle mass, strength, and performance in older adults. Osteoporos. Int. 2013, 24, 1555–1566. [Google Scholar] [CrossRef]
- Misu, S.; Asai, T.; Doi, T.; Sawa, R.; Ueda, Y.; Saito, T.; Nakamura, R.; Murata, S.; Sugimoto, T.; Yamada, M.; et al. Association between gait abnormality and malnutrition in a community-dwelling elderly population. Geriatr. Gerontol. Int. 2017, 17, 1155–1160. [Google Scholar] [CrossRef]
- Bonjour, J.P. Dietary protein: an essential nutrient for bone health. J. Am. Coll. Nutr. 2005, 24, 526S–536S. [Google Scholar] [CrossRef]
- Sanchez-Rodriguez, D.; Marco, E.; Ronquillo-Moreno, N.; Miralles, R.; Vazquez-Ibar, O.; Escalada, F.; Muniesa, J.M. Prevalence of malnutrition and sarcopenia in a post-acute care geriatric unit: Applying the new ESPEN definition and EWGSOP criteria. Clin. Nutr. 2017, 36, 1339–1344. [Google Scholar] [CrossRef]
- Salminen, H.; Saaf, M.; Johansson, S.E.; Ringertz, H.; Strender, L.E. Nutritional status, as determined by the Mini-Nutritional Assessment, and osteoporosis: a cross-sectional study of an elderly female population. Eur. J. Clin. Nutr. 2006, 60, 486–493. [Google Scholar] [CrossRef]
- Huo, Y.R.; Suriyaarachchi, P.; Gomez, F.; Curcio, C.L.; Boersma, D.; Gunawardene, P.; Demontiero, O.; Duque, G. Comprehensive nutritional status in sarco-osteoporotic older fallers. J. Nutr. Health Aging 2015, 19, 474–480. [Google Scholar] [CrossRef]
- Reiss, J.; Iglseder, B.; Alzner, R.; Mayr-Pirker, B.; Pirich, C.; Kassmann, H.; Kreutzer, M.; Dovjak, P.; Reiter, R. Sarcopenia and osteoporosis are interrelated in geriatric inpatients. Z. Gerontol. Geriatr. 2019. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, P.; Dou, Q.; Wang, C.; Zhang, W.; Yang, Y.; Wang, J.; Xie, X.; Zhou, J.; Zeng, Y. Falls among older adults with sarcopenia dwelling in nursing home or community: A meta-analysis. Clin. Nutr. 2019. [Google Scholar] [CrossRef]
- Hirschfeld, H.P.; Kinsella, R.; Duque, G. Osteosarcopenia: where bone, muscle, and fat collide. Osteoporos. Int. 2017, 28, 2781–2790. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Kumar, C. The patient who falls: “It’s always a trade-off”. Jama 2010, 303, 258–266. [Google Scholar] [CrossRef]
- Deandrea, S.; Lucenteforte, E.; Bravi, F.; Foschi, R.; La Vecchia, C.; Negri, E. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology 2010, 21, 658–668. [Google Scholar] [CrossRef]
- Nuotio, M.; Tuominen, P.; Luukkaala, T. Association of nutritional status as measured by the Mini-Nutritional Assessment Short Form with changes in mobility, institutionalization and death after hip fracture. Eur. J. Clin. Nutr. 2016, 70, 393–398. [Google Scholar] [CrossRef]
- Inoue, T.; Misu, S.; Tanaka, T.; Kakehi, T.; Ono, R. Acute phase nutritional screening tool associated with functional outcomes of hip fracture patients: A longitudinal study to compare MNA-SF, MUST, NRS-2002 and GNRI. Clin. Nutr. 2019, 38, 220–226. [Google Scholar] [CrossRef]
- Vivanti, A.; Ward, N.; Haines, T. Nutritional status and associations with falls, balance, mobility and functionality during hospital admission. J. Nutr. Health Aging 2011, 15, 388–391. [Google Scholar] [CrossRef]
- Whitley, A.; Skliros, E.; Graven, C.; McIntosh, R.; Lasry, C.; Newsome, C.; Bowie, A. Changes in Nutritional and Functional Status in Longer Stay Patients Admitted to a Geriatric Evaluation and Management Unit. J. Nutr. Health Aging 2017, 21, 686–691. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. J. Aging Ment. Health 1986, 5, 165–173. [Google Scholar]
- Vitamin, D. Supplementation Guidelines-Osteoporosis Australia. Available online: https://www.osteoporosis.org.au/sites/default/files/files/oa_medical_vitd_2nd_ed.pdf (accessed on 4 July 2019).
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Zanker, J.; Scott, D.; Reijnierse, E.M.; Brennan-Olsen, S.L.; Daly, R.M.; Girgis, C.M.; Grossmann, M.; Hayes, A.; Henwood, T.; Hirani, V.; et al. Establishing an Operational Definition of Sarcopenia in Australia and New Zealand: Delphi Method Based Consensus Statement. J. Nutr. Health Aging 2019, 23, 105–110. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, E.; Miller, M.; Yaxley, A.; Isenring, E. Malnutrition in the elderly: A narrative review. Maturitas 2013, 76, 296–302. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.S.; Charlton, K.E.; Maggio, M.; et al. Frequency of malnutrition in older adults: a multinational perspective using the mini nutritional assessment. J. Am. Geriatr. Soc. 2010, 58, 1734–1738. [Google Scholar] [CrossRef]
- Collins, J.; Porter, J.; Truby, H.; Huggins, C.E. How does nutritional state change during a subacute admission? Findings and implications for practice. Eur. J. Clin. Nutr. 2016, 70, 607–612. [Google Scholar] [CrossRef]
- McDougall, K.E.; Cooper, P.L.; Stewart, A.J.; Huggins, C.E. Can the Mini Nutritional Assessment (MNA) Be Used as a Nutrition Evaluation Tool for Subacute Inpatients over an Average Length of Stay? J. Nutr. Health Aging 2015, 19, 1032–1036. [Google Scholar] [CrossRef]
- Kruizenga, H.M.; Wierdsma, N.J.; van Bokhorst-de van der Schueren, M.A.; Haollander, H.J.; Jonkers-Schuitema, C.F.; van der Heijden, E.; Melis, G.C.; van Staveren, W.A. Screening of nutritional status in The Netherlands. Clin. Nutr. 2003, 22, 147–152. [Google Scholar] [CrossRef]
- Cabrerizo, S.; Cuadras, D.; Gomez-Busto, F.; Artaza-Artabe, I.; Marin-Ciancas, F.; Malafarina, V. Serum albumin and health in older people: Review and meta analysis. Maturitas 2015, 81, 17–27. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Morley, J.E.; Vellas, B. Patient-Centered (P4) Medicine and the Older Person. J. Am. Med. Dir. Assoc. 2017, 18, 455–459. [Google Scholar] [CrossRef]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz Jentoft, A.J.; van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef]
- Robinson, S.M.; Reginster, J.Y.; Rizzoli, R.; Shaw, S.C.; Kanis, J.A.; Bautmans, I.; Bischoff-Ferrari, H.; Bruyere, O.; Cesari, M.; Dawson-Hughes, B.; et al. Does nutrition play a role in the prevention and management of sarcopenia? Clin. Nutr. 2018, 37, 1121–1132. [Google Scholar] [CrossRef]
- Neelemaat, F.; Bosmans, J.E.; Thijs, A.; Seidell, J.C.; van Bokhorst-de van der Schueren, M.A. Post-discharge nutritional support in malnourished elderly individuals improves functional limitations. J. Am. Med. Dir. Assoc. 2011, 12, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.M.; Kjaer, S.; Hansen, B.S.; Storm, R.L.; Thal-Jantzen, K.; Bitz, C. Follow-up home visits with registered dietitians have a positive effect on the functional and nutritional status of geriatric medical patients after discharge: A randomized controlled trial. Clin. Rehabil. 2013, 27, 483–493. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Descriptive Statistics | All (n = 106) |
|---|---|---|
| Baseline | ||
| Age, year | Median (Q1, Q3) | 79 (72, 82) |
| Female | n (%) | 80 (75.5) |
| BMI at baseline, kg/m2 | Median (Q1, Q3) | 27.8 (23.8, 31.9) |
| Weight at baseline, kg | Median (Q1, Q3) | 69.6 (58.5, 85.0) |
| Height, m | Mean (SD) | 1.59 (0.09) |
| Current smoker g | n (%) | 11 (10.4) |
| Number of falls (past 12 months) | Median (Q1, Q3) | 2 (1, 2) |
| Number of fractures (past 5 years) | Median (Q1, Q3) | 1 (1, 1) |
| Severe comorbidity (CACI ≥5) | n (%) | 48 (45.3) |
| Polypharmacy (≥5 medications) | n (%) | 71 (67.0) |
| Suggestive of depression a (GDS ≥6/15) | n (%) | 26 (24.5) |
| Osteopenia/osteoporosis c | n (%) | 97 (91.5) |
| Sarcopenia b | n (%) | 22 (20.8) |
| Osteosarcopenia b | n (%) | 22 (20.8) |
| Nutritional status | ||
| MNA at baseline, score | Median (Q1, Q3) | 29 (23, 30) |
| Malnourished or at risk at baseline (MNA <24/30) | n (%) | 31 (29.3) |
| Follow-up | ||
| ΔBMI h, kg/m2 | Median (Q1, Q3) | 0.6 (−0.2, 1.5) * |
| Δweight f, kg | Median (Q1, Q3) | 0.6 (−1.0, 3.0) * |
| Number of falls d (past 6 months) | Median (Q1, Q3) | 0 (0, 1) |
| Number of fractures d (past 6 months) | Median (Q1, Q3) | 0 (0, 0) |
| Osteoporosis treatment e | n (%) | 70 (66.0) |
| Vitamin D supplement use e | n (%) | 91 (85.9) |
| Protein supplement use e | n (%) | 5 (4.7) |
| Physically active j | n (%) | 51 (48.1) |
| Nutritional status | ||
| ΔMNA d, score | Median (Q1, Q3) | 0 (0, 3.3) * |
| Malnourished or at risk at follow-up d (MNA <24/30) | n (%) | 16 (15.1) |
| Characteristic | Descriptive Statistics | Maintained (Well-Nourished) n = 65 (ref) | Improved n = 20 | Maintained (Malnourished/at Risk) n = 8 | Deteriorated n = 7 |
|---|---|---|---|---|---|
| Clinical and biochemical | |||||
| Age, year | Median (Q1, Q3) | 77 (71, 81) | 79 (73, 83) | 80 (72, 84) | 81 (79, 82) |
| BMI at baseline, kg/m2 | Median (Q1, Q3) | 29.4 (24.8, 34.2) | 25.6 (20.8, 29.6) † | 23.8 (18.9, 29.8) † | 24.1 (21.4, 27.9) † |
| ΔBMI l, kg/m2 | Median (Q1, Q3) | 0.4 (−0.3, 1.3) * | 1.2 (0.7, 2.5) *, † | −0.8 (−2.5, 0.6) | 0.0 (−0.3, 1.5) |
| Weight at baseline, kg | Median (Q1, Q3) | 74.0 (64.0, 87.7) | 64.1 (51.0, 76.6) † | 64.8 (42.3, 70.4) † | 64.7 (50.4, 74.0) |
| Δweight k, kg | Median (Q1, Q3) | 0.5 (−0.9, 2.4) * | 3.0 (1.0, 5.9) *,† | −2.0 (−9.3, 0.0) † | −2.1 (−4.0, 2.8) |
| Number of falls at follow-up f | Median (Q1, Q3) | 0 (0, 0) | 0 (0, 1) | 1 (0, 2) | 2 (0, 2) † |
| Albumin at baseline, g/L | Median (Q1, Q3) | 38.0 (36.0, 40.0) | 38.0 (36.5, 40.0) | 34.0 (29.5, 39.5) | 38.0 (34.0, 41.0) |
| Δalbumin c, g/L | Median (Q1, Q3) | 0.0 (−2.0, 2.0) | 0.0 (−2.0, 2.0) | 0.5 (−1.5, 4.5) | 1.0 (−2.0, 2.0) |
| 25OHD at baseline, nmol/L | Mean (SD) | 65.5 (22.5) | 74.7 (20.2) | 66.0 (23.7) | 77.1 (28.3) |
| Δ25OHD a, nmol/L | Median (Q1, Q3) | 4.0 (−7.0, 25.0) * | 9.5 (−11.0, 17.5) | 8.5 (−5.0, 24.5) | 12.0 (−1, 23.0) |
| PTH at baseline f, pmol/L | Median (Q1, Q3) | 6.9 (5.3, 10.3) | 7.5 (5.8, 11.2) | 6.0 (4.7, 10.5) | 5.5 (3.9, 5.7) † |
| ΔPTH g, pmol/L | Median (Q1, Q3) | −0.1 (−2.0, 2.3) | 0.8 (−1.4, 3.8) | 1.4 (1.1, 4.9) † | −0.1 (−1.4, 2.6) |
| Calcium, mmol/L | Mean (SD) | 2.4 (0.1) | 2.4 (0.1) | 2.5 (0.1) | 2.5 (0.1) |
| Phosphate, mmol/L | Mean (SD) | 1.2 (0.2) | 1.2 (0.2) | 1.2 (0.2) | 1.2 (0.1) |
| Hemoglobin at baseline a, g/L | Mean (SD) | 130.1 (13.7) | 131.5 (13.2) | 135.4 (18.9) | 130.6 (13.5) |
| Δhemoglobin c, g/L | Median (Q1, Q3) | 1.0 (−4.0, 5.0) | 1.0 (−5.0, 5.0) | 1.5 (−6.5, 10.0) | 5.0 (−11.0, 15.0) |
| eGFR at baseline, mL/min/1.73 m2 | Median (Q1, Q3) | 75.0 (59.0, 86.0) | 67.0 (52.5, 84.5) | 85.0 (79.5, 87.5) | 59.0 (55.0, 68.0) |
| ΔeGFR d, mL/min/1.73 m2 | Median (Q1, Q3) | 0.0 (−4.0, 4.0) | −3.0 (−8.0, 1.0) | −3.0 (−13.0, 0.0) | 8.0 (0.0, 14.0) † |
| Musculoskeletal | |||||
| ALM/height2 at baseline, kg/m2 | Median (Q1, Q3) | 6.8 (6.0, 8.1) | 6.0 (5.2, 6.8) † | 6.2 (5.5, 6.3) † | 5.7 (5.3, 6.6) † |
| Grip strength at baseline a, kg | Median (Q1, Q3) | 22.0 (17.0, 28.0) | 20.5 (18.0, 26.0) | 19.0 (15.0, 24.5) | 16.0 (10.0, 24.0) |
| Δgrip strength d, kg | Median (Q1, Q3) | 0.0 (−3.0, 2.0) | 0.0 (−2.0, 0.5) | 0.5 (−1.5, 1.5) | −3.0 (−4.0, 2.0) |
| Gait speed at baseline e, m/sec | Median (Q1, Q3) | 0.7 (0.5, 1.0) | 0.6 (0.5, 0.7) | 0.7 (0.5, 0.9) | 0.8 (0.6, 0.9) |
| Δgait speed h, m/sec | Median (Q1, Q3) | 0.1 (−0.1, 0.2) * | 0.1 (−0.1, 0.2) | −0.0 (−0.1, −0.0) † | −0.1 (−0.2, 0) † |
| TUG at baseline f, sec | Median (Q1, Q3) | 15.2 (10.2, 21.3) | 19.4 (16.5, 24.0) † | 15.5 (10.9, 19.9) | 18.3 (12.6, 22.0) |
| ΔTUG k, sec | Median (Q1, Q3) | −0.5 (−2.2, 1.3) | −3.2 (−7.4, −0.6) *,† | −1.2 (−2.9, 3.4) | −2.6 (−2.9, 1.1) |
| SPPB at baseline b, score (/12) | Median (Q1, Q3) | 7.0 (5.0, 10.0) | 6.0 (5.0, 7.0) | 6.0 (4.0, 9.0) | 7.0 (4.0, 8.0) |
| ΔSPPB g, score | Median (Q1, Q3) | 1.0 (0.0, 2.0) * | 1.0 (0.0, 2.0) * | 0.0 (−1.5, 1.0) | −1.5 (−2.0, 0.0) † |
| CTx at baseline j, ng/L | Median (Q1, Q3) | 330 (245, 447) | 284 (204, 604) | 278 (180, 361) | 290 (162, 308) |
| ΔCTx m, ng/L | Median (Q1, Q3) | −127 (−224, −15) * | −116 (−268, −9) | 75.0 (−151.0, 102.0) | 130 (8, 149) † |
| Change in Musculoskeletal Outcome | Change in Nutritional Status | n | Age-Sex Adjusted β (95% CI) | Multivariable Adjusted β (95% CI) | |
|---|---|---|---|---|---|
| Δgrip strength, kg | Categorized a | Improved vs. ref | 20 | −0.17 (−1.98, 1.63) | 0.34 (−1.70, 2.73) |
| Maintained (malnourished/at risk) vs. ref | 8 | −1.13 (−3.78, 1.52) | −1.22 (−4.07, 1.63) | ||
| Deteriorated vs. ref | 7 | −2.12 (5.00, 0.75) | −1.48 (−4.41, 1.44) | ||
| Continuous b | 1-point higher in ΔMNA | 96 | 0.10 (−0.10, 0.30) | 0.09 (−0.11, 0.30) | |
| Δgait speed, m/sec | Categorized a | Improved vs. ref | 16 | −0.03 (−0.12, 0.07) | 0.04 (−0.07, 0.15) |
| Maintained (malnourished/at risk) vs. ref | 8 | −0.14 (−0.27, −0.01) i | −0.07 (−0.21, 0.07) | ||
| Deteriorated vs. ref | 4 | −0.15 (−0.33, 0.02) | −0.14 (−0.31, 0.04) | ||
| Continuous b | 1-point higher in ΔMNA | 89 | 0.01 (0.00, 0.03) i | 0.01 (0.00, 0.02) i | |
| ΔTUG, sec | Categorized a | Improved vs. ref | 17 | −3.41 (−5.82, −0.99) ii | −3.30 (−6.34, −0.27) i |
| Maintained (malnourished/at risk) vs. ref | 8 | 0.04 (-3.25, 3.33) | −0.28 (−4.13, 3.56) | ||
| Deteriorated vs. ref | 3 | −1.87 (−7.09, 3.34) | −1.74 (−7.35, 3.87) | ||
| Continuous b | 1-point higher in ΔMNA | 86 | −0.18 (−0.46, 0.10) | −0.13 (−0.41, 0.15) | |
| ΔSPPB, score | Categorized a | Improved vs. ref | 18 | 0.40 (−0.54, 1.33) | 1.05 (−0.06, 2.15) |
| Maintained (malnourished/at risk) vs. ref | 8 | −1.18 (−2.47, 0.11) | −0.72 (−2.13, 0.69) | ||
| Deteriorated vs. ref | 6 | −2.21 (−3.69, −0.72) ii | −1.74 (−3.29, −0.20) i | ||
| Continuous b | 1-point higher in ΔMNA | 91 | 0.21 (0.11, 0.31) iii | 0.20 (0.10, 0.31) iii | |
| Δlog (CTx), ng/L | Categorized a | Improved vs. ref | 15 | 0.17 (−0.32, 0.66) | 0.00 (−0.56, 0.56) |
| Maintained (malnourished/at risk) vs. ref | 5 | 0.10 (−0.69, 0.89) | 0.10 (−0.79, 1.00) | ||
| Deteriorated vs. ref | 5 | 0.60 (−0.19, 1.40) | 0.69 (−0.09, 1.48) | ||
| Continuous b | 1-point higher in ΔMNA | 81 | −0.02 (−0.08, 0.04) | −0.04 (−0.09, 0.02) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conzade, R.; Phu, S.; Vogrin, S.; Bani Hassan, E.; Sepúlveda-Loyola, W.; Thorand, B.; Duque, G. Changes in Nutritional Status and Musculoskeletal Health in a Geriatric Post-Fall Care Plan Setting. Nutrients 2019, 11, 1551. https://doi.org/10.3390/nu11071551
Conzade R, Phu S, Vogrin S, Bani Hassan E, Sepúlveda-Loyola W, Thorand B, Duque G. Changes in Nutritional Status and Musculoskeletal Health in a Geriatric Post-Fall Care Plan Setting. Nutrients. 2019; 11(7):1551. https://doi.org/10.3390/nu11071551
Chicago/Turabian StyleConzade, Romy, Steven Phu, Sara Vogrin, Ebrahim Bani Hassan, Walter Sepúlveda-Loyola, Barbara Thorand, and Gustavo Duque. 2019. "Changes in Nutritional Status and Musculoskeletal Health in a Geriatric Post-Fall Care Plan Setting" Nutrients 11, no. 7: 1551. https://doi.org/10.3390/nu11071551