Validation of Surrogate Anthropometric Indices in Older Adults: What Is the Best Indicator of High Cardiometabolic Risk Factor Clustering?

 , , , , , ,
, , , , , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Anthropometric Measurements
2.3. Serum Biochemical Examination
2.4. Blood Pressure Determination
2.5. Diagnostic Criteria of Metabolic Syndrome
2.6. Definition of Cardiometabolic Risk Index
2.7. Co-Variables
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Participants
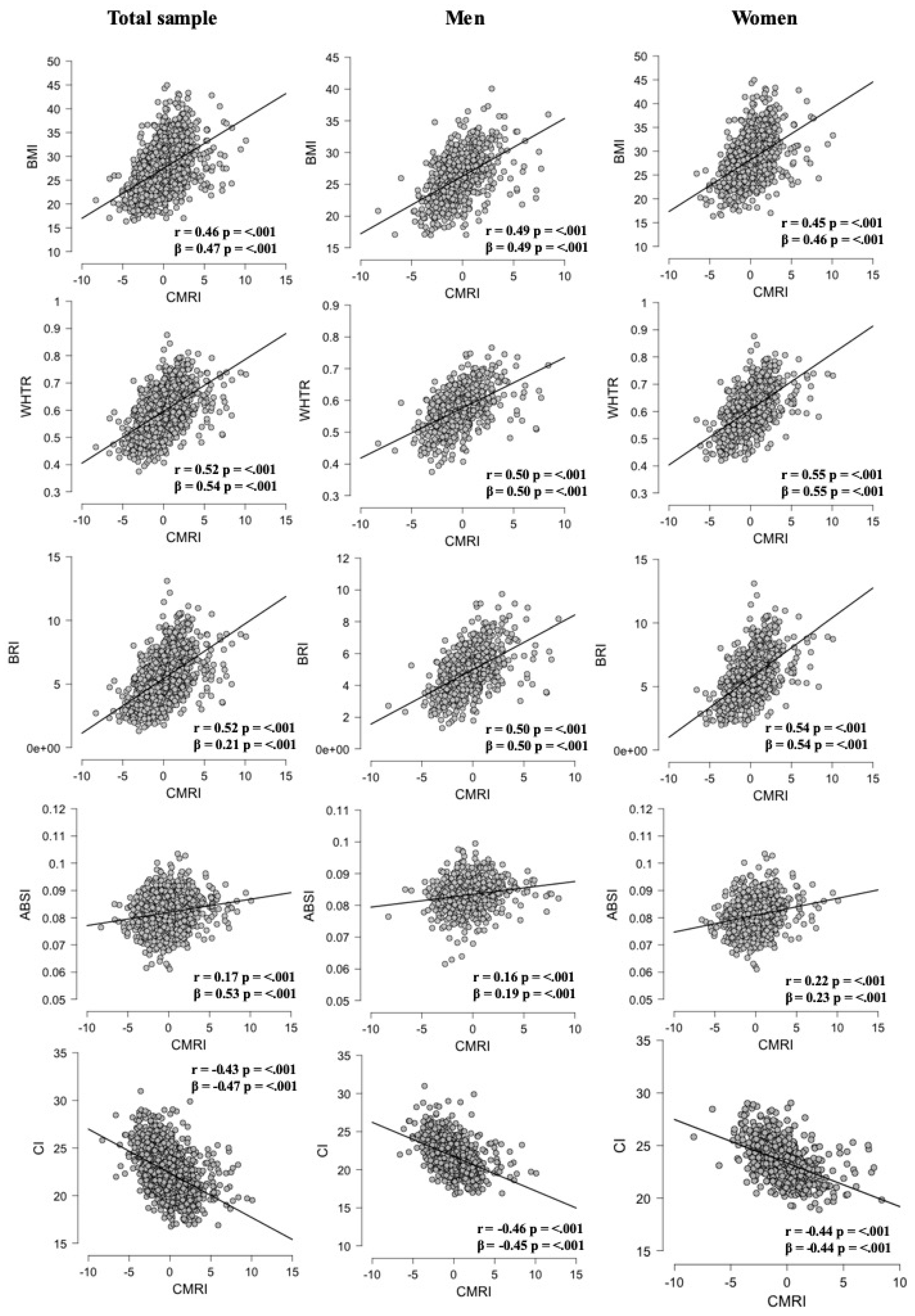
3.2. Association between Surrogate Anthropometric Indices with CMRI
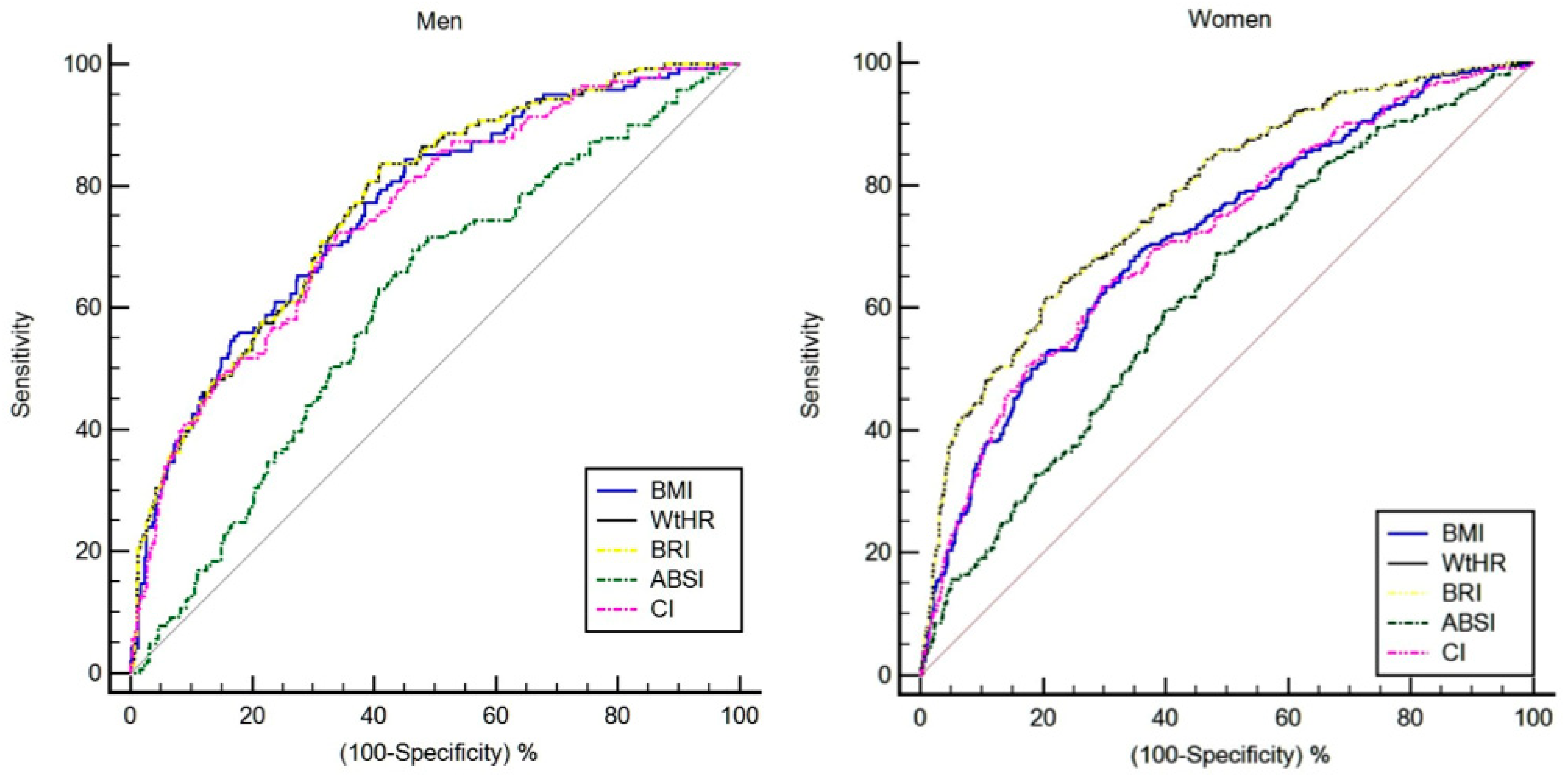
3.3. Optimal Cut-Offs for Screening for CMRI by Sex
3.4. Sex Thresholds for Surrogate Anthropometric Indices to Screen for CMRI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mente, A.; Yusuf, S.; Islam, S.; McQueen, M.J.; Tanomsup, S.; Onen, C.L.; Rangarajan, S.; Gerstein, H.C.; Anand, S.S. INTERHEART Investigators Metabolic Syndrome and Risk of Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2010, 55, 2390–2398. [Google Scholar] [CrossRef] [PubMed]
- Chien, K.-L.; Hsu, H.-C.; Sung, F.-C.; Su, T.-C.; Chen, M.-F.; Lee, Y.-T. Metabolic syndrome as a risk factor for coronary heart disease and stroke: An 11-year prospective cohort in Taiwan community. Atherosclerosis 2007, 194, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Boden-Albala, B.; Sacco, R.L.; Lee, H.-S.; Grahame-Clarke, C.; Rundek, T.; Elkind, M.V.; Wright, C.; Giardina, E.-G.V.; DiTullio, M.R.; Homma, S.; et al. Metabolic Syndrome and Ischemic Stroke Risk. Stroke 2008, 39, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Márquez-Sandoval, F.; Macedo-Ojeda, G.; Viramontes-Hörner, D.; Fernández Ballart, J.; Salas Salvadó, J.; Vizmanos, B. The prevalence of metabolic syndrome in Latin America: A systematic review. Public Health Nutr. 2011, 14, 1702–1713. [Google Scholar] [CrossRef] [PubMed]
- DeBoer, M.D.; Gurka, M.J.; Woo, J.G.; Morrison, J.A. Severity of the metabolic syndrome as a predictor of type 2 diabetes between childhood and adulthood: The Princeton Lipid Research Cohort Study. Diabetologia 2015, 58, 2745–2752. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correa-Rodríguez, M.; Ramírez-Vélez, R.; Correa-Bautista, J.; Castellanos-Vega, R.; Arias-Coronel, F.; González-Ruíz, K.; Alejandro Carrillo, H.; Schmidt-RioValle, J.; González-Jiménez, E. Association of Muscular Fitness and Body Fatness with Cardiometabolic Risk Factors: The FUPRECOL Study. Nutrients 2018, 10, 1742. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Correa-Bautista, J.; Carrillo, H.; González-Jiménez, E.; Schmidt-RioValle, J.; Correa-Rodríguez, M.; García-Hermoso, A.; González-Ruíz, K. Tri-Ponderal Mass Index vs. Fat Mass/Height3 as a Screening Tool for Metabolic Syndrome Prediction in Colombian Children and Young People. Nutrients 2018, 10, 412. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Correa-Bautista, J.; González-Ruíz, K.; Tordecilla-Sanders, A.; García-Hermoso, A.; Schmidt-RioValle, J.; González-Jiménez, E. The Role of Body Adiposity Index in Determining Body Fat Percentage in Colombian Adults with Overweight or Obesity. Int. J. Environ. Res. Public Health 2017, 14, 1093. [Google Scholar] [CrossRef] [PubMed]
- Knowles, K.M.; Paiva, L.L.; Sanchez, S.E.; Revilla, L.; Lopez, T.; Yasuda, M.B.; Yanez, N.D.; Gelaye, B.; Williams, M.A. Waist Circumference, Body Mass Index, and Other Measures of Adiposity in Predicting Cardiovascular Disease Risk Factors among Peruvian Adults. Int. J. Hypertens. 2011, 2011. [Google Scholar] [CrossRef]
- Browning, L.M.; Hsieh, S.D.; Ashwell, M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0·5 could be a suitable global boundary value. Nutr. Res. Rev. 2010, 23, 247–269. [Google Scholar] [CrossRef] [PubMed]
- Dobbelsteyn, C.; Joffres, M.; MacLean, D.; Flowerdew, G. A comparative evaluation of waist circumference, waist-to-hip ratio and body mass index as indicators of cardiovascular risk factors. The Canadian Heart Health Surveys. Int. J. Obes. 2001, 25, 652–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krakauer, N.Y.; Krakauer, J.C. A New Body Shape Index Predicts Mortality Hazard Independently of Body Mass Index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef] [PubMed]
- Mantzoros, C.; Evagelopoulou, K.; Georgiadis, E.; Katsilambros, N. Conicity Index as a Predictor of Blood Pressure Levels, Insulin and Triglyceride Concentrations of Healthy Premenopausal Women. Horm. Metab. Res. 1996, 28, 32–34. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.M.; Bredlau, C.; Bosy-Westphal, A.; Mueller, M.; Shen, W.; Gallagher, D.; Maeda, Y.; McDougall, A.; Peterson, C.M.; Ravussin, E.; et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity 2013, 21, 2264–2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Wu, H.; Wu, X.; Cao, Z.; Tu, Y.; Ma, Y.; Li, B.; Peng, Q.; Cheng, J.; Wu, B.; et al. The feasibility of two anthropometric indices to identify metabolic syndrome, insulin resistance and inflammatory factors in obese and overweight adults. Nutrition 2019, 57, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Yao, T.; Wu, X.-W.; Cao, Z.; Tu, Y.-C.; Ma, Y.; Li, B.-N.; Peng, Q.-Y.; Wu, B.; Hou, J. Novel and traditional anthropometric indices for identifying arterial stiffness in overweight and obese adults. Clin. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Stefanescu, A.; Revilla, L.; Lopez, T.; Sanchez, S.E.; Williams, M.A.; Gelaye, B. Using A Body Shape Index (ABSI) and Body Roundness Index (BRI) to predict risk of metabolic syndrome in Peruvian adults. J. Int. Med. Res. 2019. [Google Scholar] [CrossRef]
- Maessen, M.F.H.; Eijsvogels, T.M.H.; Verheggen, R.J.H.M.; Hopman, M.T.E.; Verbeek, A.L.M.; de Vegt, F. Entering a New Era of Body Indices: The Feasibility of a Body Shape Index and Body Roundness Index to Identify Cardiovascular Health Status. PLoS ONE 2014, 9, e107212. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. Untangling Waist Circumference and Hip Circumference from Body Mass Index with a Body Shape Index, Hip Index, and Anthropometric Risk Indicator. Metab. Syndr. Relat. Disord. 2018, 16, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Reardon, T. Obesity and the food system transformation in Latin America. Obes. Rev. 2018, 19, 1028–1064. [Google Scholar] [CrossRef] [PubMed]
- Valdez, R. A simple model-based index of abdominal adiposity. J. Clin. Epidemiol. 1991, 44, 955–956. [Google Scholar] [CrossRef]
- Aronow, W.S.; Banach, M. Ten most important things to learn from the ACCF/AHA 2011 expert consensus document on hypertension in the elderly. Blood Press. 2012, 21, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; García-Hermoso, A.; Cano, C.A.; Izquierdo, M. Reference values for handgrip strength and their association with intrinsic capacity domains among older adults. J. Cachexia Sarcopenia Muscle 2019, 10, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Bewick, V.; Cheek, L.; Ball, J. Statistics review 13: Receiver operating characteristic curves. Crit. Care 2004, 8, 508–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Kutner, M.H.; Nachtsheim, C.; Neter, J. Applied Linear Regression Models; McGraw-Hill/Irwin: New York, NY, USA, 2004; ISBN 0073014664. [Google Scholar]
- Tune, J.D.; Goodwill, A.G.; Sassoon, D.J.; Mather, K.J. Cardiovascular consequences of metabolic syndrome. Transl. Res. 2017, 183, 57–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamer, M.; Stamatakis, E. Metabolically healthy obesity and risk of all-cause and cardiovascular disease mortality. J. Clin. Endocrinol. Metab. 2012, 97, 2482–2488. [Google Scholar] [CrossRef]
- Davila, E.P.; Quintero, M.A.; Orrego, M.L.; Ford, E.S.; Walke, H.; Arenas, M.M.; Pratt, M. Prevalence and risk factors for metabolic syndrome in Medellin and surrounding municipalities, Colombia, 2008–2010. Prev. Med. 2013, 56, 30–34. [Google Scholar] [CrossRef]
- Escobedo, J.; Schargrodsky, H.; Champagne, B.; Silva, H.; Boissonnet, C.P.; Vinueza, R.; Torres, M.; Hernandez, R.; Wilson, E. Prevalence of the Metabolic Syndrome in Latin America and its association with sub-clinical carotid atherosclerosis: The CARMELA cross sectional study. Cardiovasc. Diabetol. 2009, 8, 52. [Google Scholar] [CrossRef]
- Tian, S.; Zhang, X.; Xu, Y.; Dong, H. Feasibility of body roundness index for identifying a clustering of cardiometabolic abnormalities compared to BMI, waist circumference and other anthropometric indices: The China Health and Nutrition Survey, 2008 to 2009. Medicine 2016, 95, e4642. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Guo, X.; Chen, Y.; Guo, L.; Li, Z.; Yu, S.; Yang, H.; Sun, Y. A body shape index and body roundness index: Two new body indices to identify diabetes mellitus among rural populations in northeast China. BMC Public Health 2015, 15, 794. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, A.; Zhao, T.; Gong, X.; Pang, T.; Zhou, Y.; Xiao, Y.; Yan, Y.; Fan, C.; Teng, W.; et al. Comparison of anthropometric indices for predicting the risk of metabolic syndrome and its components in Chinese adults: A prospective, longitudinal study. BMJ Open 2017, 7, e016062. [Google Scholar] [CrossRef] [PubMed]
- Amirabdollahian, F.; Haghighatdoost, F. Anthropometric Indicators of Adiposity Related to Body Weight and Body Shape as Cardiometabolic Risk Predictors in British Young Adults: Superiority of Waist-to-Height Ratio. J. Obes. 2018, 2018, 8370304. [Google Scholar] [CrossRef] [PubMed]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 2012, 13, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.J.; Ma, F.; Lou, H.P.; Zhu, Y.N. Comparison of the ability to identify cardiometabolic risk factors between two new body indices and waist-to-height ratio among Chinese adults with normal BMI and waist circumference. Public Health Nutr. 2017, 20, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Haghighatdoost, F.; Sarrafzadegan, N.; Mohammadifard, N.; Asgary, S.; Boshtam, M.; Azadbakht, L. Assessing body shape index as a risk predictor for cardiovascular diseases and metabolic syndrome among Iranian adults. Nutrition 2014, 30, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Perez-Sousa, M.A.; Venegas-Sanabria, L.C.; Chavarro-Carvajal, D.A.; Cano-Gutierrez, C.A.; Izquierdo, M.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Gait speed as a mediator of the effect of sarcopenia on dependency in activities of daily living. J. Cachexia Sarcopenia Muscle 2019. [Google Scholar] [CrossRef] [PubMed]
- Gomez, F.; Corchuelo, J.; Curcio, C.L.; Calzada, M.T.; Mendez, F. SABE Colombia: Survey on Health, Well-Being, and Aging in Colombia-Study Design and Protocol. Curr. Gerontol. Geriatr. Res. 2016, 2016. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Sample (n = 1502) | High CMRI ≥ 1 SD (n = 397) | Low CMRI < 1 SD (n = 1105) | p-Value |
|---|---|---|---|---|
| Sex, n (%) | ||||
| Men | 596 (39.7) | 141 (23.7) | 455 (76.3) | <0.001 |
| Women | 906 (60.3) | 254 (28.0) | 652 (72.0) | <0.001 |
| Socioeconomic status | ||||
| 1 | 456 (30.4) | 121 (30.5) | 335 (32.1) | <0.001 |
| 2 | 635 (42.3) | 176 (44.3) | 459 (41.5) | <0.001 |
| 3 | 375 (25.0) | 98 (24.7) | 277 (25.1) | <0.001 |
| 4 | 29 (1.9) | 2 (0.5) | 27 (2.4) | <0.001 |
| >5 | 7 (0.5) | 0 (0.0) | 7 (0.6) | N.A |
| Ethnic group | ||||
| Indigenous | 78 (5.2) | 25 (6.3) | 53 (4.8) | 0.002 |
| Black | 119 (7.9) | 28 (7.1) | 91 (8.2) | <0.001 |
| White | 396 (26.4) | 106 (26.7) | 290 (26.2) | <0.001 |
| Others | 909 (60.5) | 194 (48.9) | 512 (46.3) | <0.001 |
| Smoking status, n (%) | ||||
| Yes | 145 (9.7) | 29 (7.3) | 116 (10.5) | <0.001 |
| No | 1357 (90.3) | 368 (92.7) | 989 (89.5) | <0.001 |
| Alcohol intake, n (%) | ||||
| Yes | 191 (12.7) | 52 (13.1) | 139 (12.6) | <0.001 |
| No | 1310 (87.2) | 345 (86.9) | 965 (87.3) | <0.001 |
| Physical Activity “proxy”, n (%) | ||||
| Physically active | 266 (17.7) | 70 (17.6) | 196 (17.7) | 0.980 |
| Non-Physically active | 1231 (82.0) | 323 (81.4) | 908 (82.2) | <0.001 |
| Anthropometric measures/indices | ||||
| Height (m) | 1.55 (1.49–1.62) | 1.54 (1.49–1.62) | 1.55 (1.49–1.62) | 0.170 |
| Weight (kg) | 64 (57–72) | 71 (63–79) | 62 (55–69) | <0.001 |
| Waist circumference (cm) | 92 (85–100) | 101 (93–107) | 89 (83–97) | <0.001 |
| Body mass index (kg/m2) | 27 (24–30) | 29.7 (26.7–33) | 26.1 (23.3–29) | <0.001 |
| WtHR | 0.59 (0.1) | 0.64 (0.06) | 0.57 (0.06) | <0.001 |
| BRI | 5.2 (4.1–6.3) | 6.4 (5.3–7.7) | 4.8 (3.9–5.9) | <0.001 |
| ABSI (m11/6 ∙ kg −2/3) | 0.081 (0.078–0.085) | 0.083 (0.080–0.086) | 0.081 (0.077–0.084) | <0.001 |
| CI | 22.2 (20.9–23.8) | 21.1 (19.8–22.4) | 22.6 (21.4–24.1) | <0.001 |
| Metabolic syndrome components, n (%) | ||||
| Prevalence of MetS | 811 (58.7) | 308 (77.6) | 503 (45.5) | <0.001 |
| Abdominal obesity | 1177 (78.4) | 374 (94.2) | 803 (72.7) | <0.001 |
| Hypertension | 790 (52.6) | 304 (76.6) | 486 (44.0) | <0.001 |
| High levels of fasting glucose | 465 (31.0) | 220 (55.4) | 245 (22.2) | <0.001 |
| High levels of triglycerides | 696 (46.3) | 253 (63.7) | 443 (40.1) | <0.001 |
| Low levels of HDL-C | 821 (54.7) | 219 (55.2) | 602 (54.5) | 0.393 |
| Cardiometabolic measurements | ||||
| SBP (mmHg) | 130 (117–145) | 142 (130–163) | 126 (114–140) | <0.001 |
| DBP (mmHg) | 72 (65–79) | 78 (72–86) | 70 (64–77) | <0.001 |
| MBP (mmHg) | 92 (84–101) | 100 (91–111) | 89 (81–97) | <0.001 |
| Total cholesterol (mg/dL) | 193 (166–221) | 202 (171–232) | 190 (164–216) | <0.001 |
| Triglycerides (mg/dL) | 144 (105–192) | 174 (134–252) | 134 (101–180) | <0.001 |
| LDL-C (mg/dL) | 126 (102–149) | 127 (103–152) | 125 (102–147) | 0.116 |
| HDL-C (mg/dL) | 43 (36–53) | 43 (36–54) | 44 (36–53) | 0.740 |
| Glucose (mg/dL) | 94 (86–102) | 102 (93–121) | 91 (84–98) | <0.001 |
| CMRI | −0.21 (−1.41–1.07) | 2.00 (1.44–2.84) | −0.83 (−1.83–0.05) | <0.001 |
| Self-report comorbid chronic diseases, n (%) | ||||
| Hypertension | 826 (55.0) | 249 (62.7) | 577 (52.2) | <0.001 |
| Diabetes | 245 (16.3) | 113 (28.5) | 132 (11.9) | <0.001 |
| Respiratory diseases | 165 (11.0) | 49 (12.3) | 116 (10.5) | <0.001 |
| Cardiovascular diseases | 213 (14.2) | 155 (39.0) | 58 (5.2) | <0.001 |
| Stroke | 70 (4.7) | 22 (5.5) | 48 (4.3) | <0.001 |
| Osteoporosis | 184 (12.3) | 66 (16.6) | 118 (10.7) | <0.001 |
| Cancer | 80 (5.3) | 56 (14.1) | 24 (2.2) | <0.001 |
| Hearing loss | 360 (24.1) | 89 (22.4) | 271 (24.5) | <0.001 |
| Vision loss | 851 (56.7) | 228 (57.4) | 623 (56.4) | <0.001 |
| Parameters | BMI | WtHR | BRI | ABSI | CI | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | Men | Women | Men | Women | |
| Area under curve | 0.76 | 0.71 | 0.77 | 0.77 | 0.77 | 0.77 | 0.60 | 0.62 | 0.75 | 0.71 |
| p-value | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| Optimal cut-off | 25.2 | 28.4 | 0.56 | 0.63 | 4.71 | 6.20 | 0.083 | 0.080 | 22.9 | 21.0 |
| Youden index J | 0.39 | 0.33 | 0.42 | 0.41 | 0.42 | 0.41 | 0.23 | 0.20 | 0.38 | 0.33 |
| Sensitivity (%) | 84.4 | 69.5 | 83.6 | 64.4 | 83.6 | 65.2 | 69.5 | 68.7 | 72.3 | 63.6 |
| Specificity (%) | 54.7 | 64.1 | 58.9 | 76.7 | 58.9 | 76.1 | 53.6 | 51.6 | 65.9 | 70.2 |
| (+) Likelihood ratio | 1.83 | 1.93 | 2.00 | 2.70 | 2.04 | 2.74 | 1.50 | 1.42 | 2.12 | 2.14 |
| (–) Likelihood ratio | 0.29 | 0.48 | 0.28 | 0.47 | 0.28 | 0.46 | 0.57 | 0.60 | 0.42 | 0.52 |
| Parameters | BMI–WtHR | BMI–BRI | BMI–ABSI | BMI–CI | WtHR–BRI | WtHR–ABSI | WtHR–CI | BRI–ABSI | BRI–CI | ABSI–CI |
|---|---|---|---|---|---|---|---|---|---|---|
| Men | ||||||||||
| Diff. AUC | 0.000 | 0.00 | 0.15 | 0.01 | 0.00 | 0.16 | 0.01 | 0.16 | 0.02 | 0.14 |
| SE | 0.01 | 0.01 | 0.03 | 0.00 | 0.00 | 0.02 | 0.01 | 0.02 | 0.01 | 0.03 |
| p-value | 0.542 | 0.540 | 0.001 | 0.220 | 0.090 | 0.001 | 0.100 | 0.001 | 0.090 | 0.001 |
| Women | ||||||||||
| Diff. AUC | 0.06 | 0.06 | 0.08 | 0.00 | 0.00 | 0.15 | 0.06 | 0.15 | 0.06 | 0.08 |
| SE | 0.01 | 0.01 | 0.03 | 0.00 | 0.00 | 0.02 | 0.01 | 0.02 | 0.01 | 0.03 |
| p-value | 0.001 | 0.001 | 0.001 | 0.99 | 0.97 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 |
| Variables | Cut-Off | BMI | WtHR | BRI | ABSI | CI | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SE) | p-Value | Mean (SE) | p-Value | Mean (SE) | p-Value | Mean (SE) | p-Value | Mean (SE) | p-Value | ||
| Men | |||||||||||
| SBP (mmHg) | healthy | 130.1 (1.5) | 0.001 | 131.7 (1.5) | 0.107 | 131.5 (1.4) | 0.045 | 134.7 (2.1) | 0.477 | 131.3 (1.3) | 0.005 |
| unhealthy | 136.1 (1.3) | 135.0 (1.3) | 135.6 (1.4) | 133.3 (1.1) | 136.6 (1.5) | ||||||
| DBP (mmHg) | healthy | 72.3 (0.8) | 0.001 | 73.8 (0.8) | 0.250 | 73.7 (0.7) | 0.131 | 76.1 (13.4) | 0.176 | 73.1 (0.7) | 0.003 |
| unhealthy | 76.3 (0.7) | 75.3 (0.7) | 75.4 (0.7) | 74.1 (0.6) | 76.5 (0.8) | ||||||
| MBP (mmHg) | healthy | 91.5 (1.0) | 0.001 | 93.1 (0.9) | 0.148 | 92.9 (0.9) | 0.064 | 95.5 (1.3) | 0.282 | 92.4 (0.8) | 0.003 |
| unhealthy | 96.1 (0.8) | 95.0 (0.8) | 95.4 (0.9) | 93.8 (0.7) | 96.4 (0.9) | ||||||
| Total cholesterol (mg/dL) | healthy | 189.5 (2.0) | 0.011 | 190.0 (2.5) | 0.010 | 188.0 (2.4) | 0.099 | 186.6 (3.5) | 0.947 | 186.6 (2.2) | 0.224 |
| unhealthy | 181.8 (2.2) | 181.2 (2.2) | 182.4 (2.3) | 184.7 (1.9) | 183.1 (2.5) | ||||||
| Triglycerides (mg/dL) | healthy | 149.6 (5.7) | 0.22 | 149.4 (5.6) | 0.088 | 151.4 (5.3) | 0.176 | 147.4 (7.8) | 00.085 | 150.7 (4.9) | 00.054 |
| unhealthy | 162.7 (4.9) | 163.2 (4.9) | 162.5 (5.2) | 160.0 (4.2) | 165.4 (5.6) | ||||||
| LDL-C (mg/dL) | healthy | 123.5 (2.2) | 0.055 | 123.7 (2.1) | 0.058 | 122.5 (2.0) | 0.211 | 119.8 (3.0) | 0.511 | 121.3 (1.9) | 0.467 |
| unhealthy | 118.4 (1.8) | 118.1 (1.9) | 118.8 (1.9) | 120.8 (1.6) | 119.6 (2.1) | ||||||
| HDL-C (mg/dL) | healthy | 45.1 (0.7) | 0.001 | 44.3 (0.7) | 0.001 | 44.3 (12.4) | 0.001 | 45.4 (1.0) | 0.001 | 43.9 (0.6) | 0.001 |
| unhealthy | 39.5 (0.6) | 39.6 (0.6) | 39.3 (9.5) | 40.8 (0.5) | 39.2 (0.7) | ||||||
| Glucose (mg/dL) | healthy | 93.7 (1.5) | 0.005 | 93.9 (1.5) | 0.009 | 93.6 (1.4) | 0.002 | 98.0 (2.1) | 0.519 | 95.0 (1.3) | 0.028 |
| unhealthy | 99.1 (1.3) | 99.0 (1.3) | 99.8 (1.4) | 96.4 (1.1) | 99.0 (1.5) | ||||||
| CMRI | healthy | −1.09 (0.1) | 0.001 | −1.05 (0.1) | 0.001 | −1.05 (0.1) | 0.001 | −0.66 (0.18) | 0.010 | −0.87 (0.11) | 0.001 |
| unhealthy | 0.36 (0.1) | 0.36 (0.1) | 0.50 (0.1) | −0.13 (0.09) | 0.53 (0.12) | ||||||
| Women | |||||||||||
| SBP (mmHg) | healthy | 130.4 (1.1) | 0.530 | 130.6 (1.0) | 0.942 | 130.6 (1.0) | 0.935 | 129.8 (1.2) | 0.639 | 130.4 (1.0) | 0.537 |
| unhealthy | 131.1 (1.1) | 130.8 (1.3) | 130.8 (1.3) | 131.4 (1.0) | 131.1 (1.2) | ||||||
| DBP (mmHg) | healthy | 70.9 (0.5) | 0.021 | 71.6 (0.5) | 0.458 | 71.6 (0.5) | 0.414 | 72.0 (0.6) | 0.993 | 71.1 (0.5) | 0.034 |
| unhealthy | 72.9 (10.5) | 72.3 (0.6) | 72.3 (0.6) | 71.8 (0.5) | 73.1 (0.6) | ||||||
| MBP (mmHg) | healthy | 90.6 (0.6) | 0.097 | 91.2 (0.6) | 0.721 | 91.2 (0.6) | 0.691 | 91.2 (0.7) | 0.823 | 90.8 (0.6) | 0.139 |
| unhealthy | 92.3 (0.7) | 91.7 (0.8) | 91.8 (0.8) | 91.6 (0.6) | 92.4 (0.7) | ||||||
| Total cholesterol (mg/dL) | healthy | 203.7 (1.9) | 0.233 | 204.1 (1.8) | 0.098 | 203.9 (1.8) | 0.149 | 202.0 (2.1) | 0.572 | 203.2 (1.8) | 0.376 |
| unhealthy | 200.4 (2.1) | 198.8 (2.3) | 199.0 (2.4) | 202.2 (1.9) | 200.5 (2.2) | ||||||
| Triglycerides (mg/dL) | healthy | 161.1 (4.0) | 0.111 | 160.8 (3.7) | 0.059 | 161.2 (3.7) | 0.068 | 157.0 (4.4) | 0.044 | 162.3 (3.8) | 0.159 |
| unhealthy | 170.8 (4.3) | 173.5 (4.8) | 173.4 (4.9) | 172.4 (3.9) | 170.7 (4.7) | ||||||
| LDL-C (mg/dL) | healthy | 132.3 (1.7) | 0.258 | 132.6 (1.6) | 0.164 | 132.5 (1.5) | 0.132 | 132.0 (34.8) | 0.812 | 132.0 (1.6) | 0.381 |
| unhealthy | 129.8 (1.8) | 128.8 (2.0) | 128.8 (2.1) | 131.1 (37.4) | 129.9 (2.0) | ||||||
| HDL-C (mg/dL) | healthy | 48.8 (0.6) | 0.009 | 48.8 (0.5) | 0.001 | 48.6 (0.5) | 0.007 | 48.7 (13.9) | 0.104 | 48.5 (0.5) | 0.018 |
| unhealthy | 46.1 (0.6) | 45.4 (0.7) | 45.6 (0.7) | 46.9 (12.3) | 46.1 (0.7) | ||||||
| Glucose (mg/dL) | healthy | 97.3 (1.1) | 0.016 | 96.8 (1.0) | 0.001 | 96.6 (1.0) | 0.001 | 98.1 (1.2) | 0.241 | 97.0 (1.0) | 0.002 |
| unhealthy | 101.2 (1.2) | 102.9 (1.3) | 103.5 (1.3) | 99.9 (1.1) | 102.3 (1.3) | ||||||
| CMRI | healthy | −0.61 (0.09) | 0.001 | −0.57 (0.08) | 0.001 | −0.56 (0.08) | 0.001 | −0.32 (0.10) | 0.001 | −0.52 (0.08) | 0.001 |
| unhealthy | 0.82 (0.09) | 1.09 (0.10) | 1.16 (0.01) | 0.36 (0.09) | 0.94 (0.10) | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Vélez, R.; Pérez-Sousa, M.Á.; Izquierdo, M.; Cano-Gutierrez, C.A.; González-Jiménez, E.; Schmidt-RioValle, J.; González-Ruíz, K.; Correa-Rodríguez, M. Validation of Surrogate Anthropometric Indices in Older Adults: What Is the Best Indicator of High Cardiometabolic Risk Factor Clustering? Nutrients 2019, 11, 1701. https://doi.org/10.3390/nu11081701
Ramírez-Vélez R, Pérez-Sousa MÁ, Izquierdo M, Cano-Gutierrez CA, González-Jiménez E, Schmidt-RioValle J, González-Ruíz K, Correa-Rodríguez M. Validation of Surrogate Anthropometric Indices in Older Adults: What Is the Best Indicator of High Cardiometabolic Risk Factor Clustering? Nutrients. 2019; 11(8):1701. https://doi.org/10.3390/nu11081701
Chicago/Turabian StyleRamírez-Vélez, Robinson, Miguel Ángel Pérez-Sousa, Mikel Izquierdo, Carlos A. Cano-Gutierrez, Emilio González-Jiménez, Jacqueline Schmidt-RioValle, Katherine González-Ruíz, and María Correa-Rodríguez. 2019. "Validation of Surrogate Anthropometric Indices in Older Adults: What Is the Best Indicator of High Cardiometabolic Risk Factor Clustering?" Nutrients 11, no. 8: 1701. https://doi.org/10.3390/nu11081701