The Effect of Maternal Obesity on Breast Milk Fatty Acids and Its Association with Infant Growth and Cognition—The PREOBE Follow-Up

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statement of Ethics
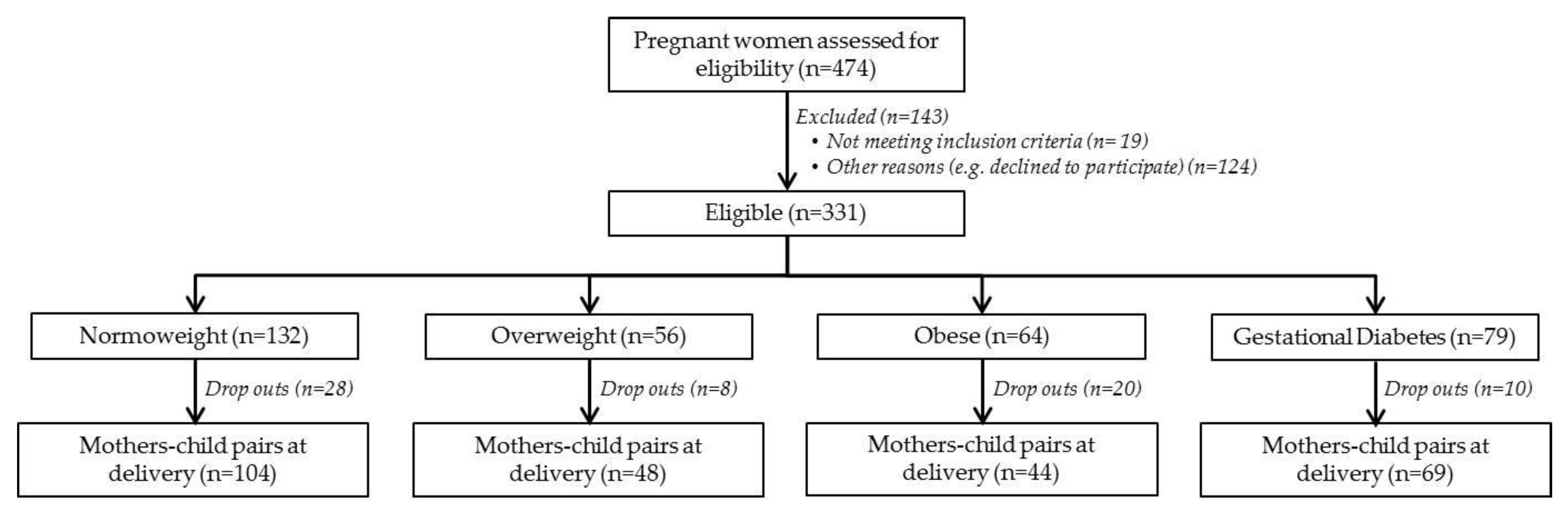
2.2. Study Population and Design
2.3. Breast Milk Sample Collection
2.4. Fatty Acid Analysis of Breast Milk
2.5. Assessment of Anthropometric Infant Outcomes
2.6. Assessment of Infant Cognitive Development
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Population
3.2. Breast Milk Fatty Acid Evolution
3.3. Breast Milk FAs According to Maternal Weight Group
3.4. Association of Breast Milk FAs with Infant Growth
3.5. Associations of Breast Milk FAs with Infant Cognition
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Koletzko, B.; Godfrey, K.M.; Poston, L.; Szajewska, H.; van Goudoever, J.B.; de Waard, M.; Brands, B.; Grivell, R.M.; Deussen, A.R.; Dodd, J.M.; et al. Nutrition During Pregnancy, Lactation and Early Childhood and its Implications for Maternal and Long-Term Child Health: The Early Nutrition Project Recommendations. Ann. Nutr. Metab. 2019, 74, 93–106. [Google Scholar] [CrossRef]
- Langley-Evans, S.C. Nutrition in early life and the programming of adult disease: A review. J. Hum. Nutr. Diet. 2015, 28, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Escamilla, R.; Martinez, J.L.; Segura-Pérez, S. Impact of the Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: A systematic review. Matern. Child Nutr. 2016, 12, 402–417. [Google Scholar] [CrossRef]
- Mosca, F.; Giannì, M.L. Human milk: Composition and health benefits. La Pediatr. Med. Chir. 2017, 39, 155. [Google Scholar] [CrossRef]
- Binns, C.; Lee, M.; Low, W.Y. The Long-Term Public Health Benefits of Breastfeeding. Asia Pac. J. Public Health 2016, 28, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenna, J.T.; Varamini, B.; Jensen, R.G.; Diersen-Schade, D.A.; Boettcher, J.A.; Arterburn, L.M. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am. J. Clin. Nutr. 2007, 85, 1457–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savino, F.; Liguori, S.A.; Fissore, M.F.; Oggero, R. Breast milk hormones and their protective effect on obesity. Int. J. Pediatr. Endocrinol. 2009, 2009, 327505. [Google Scholar] [CrossRef]
- Lauritzen, L.; Carlson, S.E. Maternal fatty acid status during pregnancy and lactation and relation to newborn and infant status. Matern. Child Nutr. 2011, 7, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Panagos, P.G.; Vishwanathan, R.; Penfield-Cyr, A.; Matthan, N.R.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Sen, S. Breastmilk from obese mothers has pro-inflammatory properties and decreased neuroprotective factors. J. Perinatol. 2016, 36, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, C.; Ling, P.R.; Blackburn, G.; Martin, C.R.; Ling, P.R.; Blackburn, G.L. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef] [PubMed]
- Muhlhausler, B.S.; Ailhaud, G.P. Omega-6 polyunsaturated fatty acids and the early origins of obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ailhaud, G.; Guesnet, P. Fatty acid composition of fats is an early determinant of childhood obesity: A short review and an opinion. Obes. Rev. 2004, 5, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Gertosio, C.; Meazza, C.; Pagani, S.; Bozzola, M. Breastfeeding and its gamut of benefits. Minerva Pediatr. 2016, 68, 201–212. [Google Scholar] [PubMed]
- Barrera, C.; Valenzuela, R.; Chamorro, R.; Bascuñán, K.; Sandoval, J.; Sabag, N.; Valenzuela, F.; Valencia, M.P.; Puigrredon, C.; Valenzuela, A.; et al. The Impact of Maternal Diet during Pregnancy and Lactation on the Fatty Acid Composition of Erythrocytes and Breast Milk of Chilean Women. Nutrients 2018, 10, 839. [Google Scholar] [CrossRef] [PubMed]
- Storck Lindholm, E.; Strandvik, B.; Altman, D.; Möller, A.; Palme Kilander, C. Different fatty acid pattern in breast milk of obese compared to normal-weight mothers. Prostaglandins Leukot. Essent. Fat. Acids 2013, 88, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Mäkelä, J.; Linderborg, K.; Niinikoski, H.; Yang, B.; Lagström, H. Breast milk fatty acid composition differs between overweight and normal weight women: The STEPS Study. Eur. J. Nutr. 2013, 52, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Marín, M.C.; Sanjurjo, A.; Rodrigo, M.A.; de Alaniz, M.J.T. Long-chain polyunsaturated fatty acids in breast milk in La Plata, Argentina: Relationship with maternal nutritional status. Prostaglandins Leukot. Essent. Fat. Acids 2005, 73, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients 2016, 8, 128. [Google Scholar] [CrossRef]
- Heerwagen, M.J.R.; Stewart, M.S.; de la Houssaye, B.A.; Janssen, R.C.; Friedman, J.E. Transgenic increase in N-3/n-6 Fatty Acid ratio reduces maternal obesity-associated inflammation and limits adverse developmental programming in mice. PLoS ONE 2013, 8, e67791. [Google Scholar] [CrossRef]
- Edlow, A.G. Maternal obesity and neurodevelopmental and psychiatric disorders in offspring. Prenat. Diagn. 2017, 37, 95–110. [Google Scholar] [CrossRef] [PubMed]
- Rivera, H.M.; Christiansen, K.J.; Sullivan, E.L. The role of maternal obesity in the risk of neuropsychiatric disorders. Front. Neurosci. 2015, 9, 194. [Google Scholar] [CrossRef]
- Veena, S.R.; Gale, C.R.; Krishnaveni, G.V.; Kehoe, S.H.; Srinivasan, K.; Fall, C.H. Association between maternal nutritional status in pregnancy and offspring cognitive function during childhood and adolescence; a systematic review. BMC Pregnancy Childbirth 2016, 16, 220. [Google Scholar] [CrossRef] [PubMed]
- Contu, L.; Hawkes, C.A. A Review of the Impact of Maternal Obesity on the Cognitive Function and Mental Health of the Offspring. Int. J. Mol. Sci. 2017, 18, 1093. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Yu, X.; Keim, S.; Li, L.; Zhang, L.; Zhang, J. Maternal prepregnancy obesity and child neurodevelopment in the Collaborative Perinatal Project. Int. J. Epidemiol. 2014, 43, 783–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heikura, U.; Taanila, A.; Hartikainen, A.L.; Olsen, P.; Linna, S.L.; Wendt, L.; Jarvelin, M.R. Variations in Prenatal Sociodemographic Factors associated with Intellectual Disability: A Study of the 20-Year Interval between Two Birth Cohorts in Northern Finland. Am. J. Epidemiol. 2007, 167, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Brion, M.J.; Zeegers, M.; Jaddoe, V.; Verhulst, F.; Tiemeier, H.; Lawlor, D.A.; Smith, G.D. Intrauterine effects of maternal prepregnancy overweight on child cognition and behavior in 2 cohorts. Pediatrics 2011, 127, e202–e211. [Google Scholar] [CrossRef]
- Craig, W.Y.; Palomaki, G.E.; Neveux, L.M.; Haddow, J.E. Maternal Body Mass Index during Pregnancy and Offspring Neurocognitive Development. Obstet. Med. 2013, 6, 20–25. [Google Scholar] [CrossRef]
- Kwon, M. Nutrient Content of Human Breast Milk from Overweight and Normal Weight Caucasian Women of Northeast Tennessee. Master’s Thesis, East Tennessee State University, Johnson City, TN, USA, 2017. [Google Scholar]
- Rudolph, M.C.; Young, B.E.; Lemas, D.J.; Palmer, C.E.; Hernandez, T.L.; Barbour, L.A.; Friedman, J.E.; Krebs, N.F.; MacLean, P.S. Early infant adipose deposition is positively associated with the n-6 to n-3 fatty acid ratio in human milk independent of maternal BMI. Int. J. Obes. (Lond.) 2017, 41, 510–517. [Google Scholar] [CrossRef]
- Kim, H.; Kang, S.; Jung, B.M.; Yi, H.; Jung, J.A.; Chang, N. Breast milk fatty acid composition and fatty acid intake of lactating mothers in South Korea. Br. J. Nutr. 2017, 117, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Sinanoglou, V.J.; Cavouras, D.; Boutsikou, T.; Briana, D.D.; Lantzouraki, D.Z.; Paliatsiou, S.; Volaki, P.; Bratakos, S.; Malamitsi-Puchner, A.; Zoumpoulakis, P. Factors affecting human colostrum fatty acid profile: A case study. PLoS ONE 2017, 12, e0175817. [Google Scholar] [CrossRef] [PubMed]
- Much, D.; Brunner, S.; Vollhardt, C.; Schmid, D.; Sedlmeier, E.M.; Brüderl, M.; Heimberg, E.; Bartke, N.; Boehm, G.; Bader, B.L.; et al. Breast milk fatty acid profile in relation to infant growth and body composition: Results from the INFAT study. Pediatr. Res. 2013, 74, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Berglund, S.K.; García-Valdés, L.; Torres-Espinola, F.J.; Segura, M.T.; Martínez-Zaldívar, C.; Aguilar, M.J.; Agil, A.; Lorente, J.A.; Florido, J.; Padilla, C.; et al. Maternal, fetal and perinatal alterations associated with obesity, overweight and gestational diabetes: An observational cohort study (PREOBE). BMC Public Health 2016, 16, 207. [Google Scholar] [CrossRef] [PubMed]
- Chisaguano, A.M.; Lozano, B.; Moltó-Puigmartí, C.; Castellote, A.I.; Rafecas, M.; López-Sabater, M.C. Elaidic acid, vaccenic acid and rumenic acid (c9,t11-CLA) determination in human plasma phospholipids and human milk by fast gas chromatography. Anal. Methods 2013, 5, 1264. [Google Scholar] [CrossRef]
- Borghi, E.; de Onis, M.; Garza, C.; Van den Broeck, J.; Frongillo, E.A.; Grummer-Strawn, L.; Van Buuren, S.; Pan, H.; Molinari, L.; Martorell, R.; et al. Construction of the World Health Organization child growth standards: Selection of methods for attained growth curves. Stat. Med. 2006, 25, 247–265. [Google Scholar] [CrossRef] [PubMed]
- Duggan, M.B. Anthropometry as a tool for measuring malnutrition: Impact of the new WHO growth standards and reference. Ann. Trop. Paediatr. 2010, 30, 1–17. [Google Scholar] [CrossRef]
- Goldstein, S.; Naglieri, J.A. Encyclopedia of Child Behavior and Development; Springer: Berlin/Heidelberg, Germany, 2011; ISBN 9780387775791. [Google Scholar]
- Faucher, M.A.; Barger, M.K. Gestational weight gain in obese women by class of obesity and select maternal/newborn outcomes: A systematic review. Women Birth 2015, 28, e70–e79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durie, D.E.; Thornburg, L.L.; Glantz, J.C. Effect of second-trimester and third-trimester rate of gestational weight gain on maternal and neonatal outcomes. Obstet. Gynecol. 2011, 118, 569–575. [Google Scholar] [CrossRef]
- Hinkle, S.N.; Sharma, A.J.; Dietz, P.M. Gestational weight gain in obese mothers and associations with fetal growth. Am. J. Clin. Nutr. 2010, 92, 644–651. [Google Scholar] [CrossRef] [Green Version]
- Patterson, E.; Wall, R.; Fitzgerald, G.F.; Ross, R.P.; Stanton, C. Health implications of high dietary omega-6 polyunsaturated Fatty acids. J. Nutr. Metab. 2012, 2012, 539426. [Google Scholar] [CrossRef]
- Alberico, S.; Montico, M.; Barresi, V.; Monasta, L.; Businelli, C.; Soini, V.; Erenbourg, A.; Ronfani, L.; Maso, G.; Multicentre Study Group on Mode of Delivery in Friuli Venezia Giulia. The role of gestational diabetes, pre-pregnancy body mass index and gestational weight gain on the risk of newborn macrosomia: Results from a prospective multicentre study. BMC Pregnancy Childbirth 2014, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Olsen, I.E.; Groveman, S.A.; Lawson, M.L.; Clark, R.H.; Zemel, B.S. New intrauterine growth curves based on United States data. Pediatrics 2010, 125, e214–e224. [Google Scholar] [CrossRef] [PubMed]
- Moltó-Puigmartí, C.; Castellote, A.I.; Carbonell-Estrany, X.; López-Sabater, M.C. Differences in fat content and fatty acid proportions among colostrum, transitional, and mature milk from women delivering very preterm, preterm, and term infants. Clin. Nutr. 2011, 30, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Haddad, I.; Mozzon, M.; Frega, N.G. Trends in fatty acids positional distribution in human colostrum, transitional, and mature milk. Eur. Food Res. Technol. 2012, 235, 325–332. [Google Scholar] [CrossRef]
- Lawn, J.E.; Blencowe, H.; Oza, S.; You, D.; Lee, A.C.C.; Waiswa, P.; Lalli, M.; Bhutta, Z.; Barros, A.J.D.; Christian, P.; et al. Every Newborn: Progress, priorities, and potential beyond survival. Lancet 2014, 384, 189–205. [Google Scholar] [CrossRef]
- Morales, E.; Bustamante, M.; Gonzalez, J.R.; Guxens, M.; Torrent, M.; Mendez, M.; Garcia-Esteban, R.; Julvez, J.; Forns, J.; Vrijheid, M.; et al. Genetic Variants of the FADS Gene Cluster and ELOVL Gene Family, Colostrums LC-PUFA Levels, Breastfeeding, and Child Cognition. PLoS ONE 2011, 6, e17181. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.G.; Song, Z.X.; Yin, H.; Wang, Y.Y.; Shu, G.F.; Lu, H.X.; Wang, S.K.; Sun, G.J. Low n-6/n-3 PUFA Ratio Improves Lipid Metabolism, Inflammation, Oxidative Stress and Endothelial Function in Rats Using Plant Oils as n-3 Fatty Acid Source. Lipids 2016, 51, 49–59. [Google Scholar] [CrossRef]
- Nishimura, R.Y.; Barbieiri, P.; de Castro, G.S.F.; Jordão, A.A.; da Silva Castro Perdoná, G.; Sartorelli, D.S. Dietary polyunsaturated fatty acid intake during late pregnancy affects fatty acid composition of mature breast milk. Nutrition 2014, 30, 685–689. [Google Scholar] [CrossRef]
- Hadley, K.B.; Ryan, A.S.; Forsyth, S.; Gautier, S.; Salem, N., Jr. The Essentiality of Arachidonic Acid in Infant Development. Nutrients 2016, 8, 216. [Google Scholar] [CrossRef]
- Lassek, W.D.; Gaulin, S.J.C. Maternal milk DHA content predicts cognitive performance in a sample of 28 nations. Matern. Child Nutr. 2015, 11, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Isanaka, S.; Villamor, E.; Shepherd, S.; Grais, R.F. Assessing the impact of the introduction of the World Health Organization growth standards and weight-for-height z-score criterion on the response to treatment of severe acute malnutrition in children: Secondary data analysis. Pediatrics 2009, 123, e54–e59. [Google Scholar] [CrossRef] [PubMed]
- Rombaldi Bernardi, J.; de Souza Escobar, R.; Ferreira, C.F.; Pelufo Silveira, P. Fetal and neonatal levels of omega-3: Effects on neurodevelopment, nutrition, and growth. Sci. World J. 2012, 2012, 202473. [Google Scholar]
- Pedersen, L.; Lauritzen, L.; Brasholt, M.; Buhl, T.; Bisgaard, H. Polyunsaturated fatty acid content of mother’s milk is associated with childhood body composition. Pediatr. Res. 2012, 72, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Buss, J. Limitations of Body Mass Index to Assess Body Fat. Workplace Health Saf. 2014, 62, 264. [Google Scholar] [CrossRef] [PubMed]
- Vanderwall, C.; Randall Clark, R.; Eickhoff, J.; Carrel, A.L. BMI is a poor predictor of adiposity in young overweight and obese children. BMC Pediatr. 2017, 17, 135. [Google Scholar] [CrossRef]
- Macé, K.; Shahkhalili, Y.; Aprikian, O.; Stan, S. Dietary fat and fat types as early determinants of childhood obesity: A reappraisal. Int. J. Obes. 2006, 30, S50–S57. [Google Scholar] [CrossRef]
- Innis, S.M. Impact of maternal diet on human milk composition and neurological development of infants. Am. J. Clin. Nutr. 2014, 99, 734S–741S. [Google Scholar] [CrossRef] [Green Version]
- Bernard, J.Y.; Armand, M.; Garcia, C.; Forhan, A.; De Agostini, M.; Charles, M.A.; Heude, B. The association between linoleic acid levels in colostrum and child cognition at 2 and 3 y in the EDEN cohort. Pediatr. Res. 2015, 77, 829–835. [Google Scholar] [CrossRef]
- Guxens, M.; Mendez, M.A.; Molto-Puigmarti, C.; Julvez, J.; Garcia-Esteban, R.; Forns, J.; Ferrer, M.; Vrijheid, M.; Lopez-Sabater, M.C.; Sunyer, J. Breastfeeding, Long-Chain Polyunsaturated Fatty Acids in Colostrum, and Infant Mental Development. Pediatrics 2011, 128, e880–e889. [Google Scholar] [CrossRef] [Green Version]
- Bernard, J.Y.; Armand, M.; Peyre, H.; Garcia, C.; Forhan, A.; De Agostini, M.; Charles, M.A.; Heude, B.; EDEN Mother-Child Cohort Study Group (Etude des Déterminants pré- et postnatals précoces du développement et de la santé de l’Enfant). Breastfeeding, Polyunsaturated Fatty Acid Levels in Colostrum and Child Intelligence Quotient at Age 5–6 Years. J. Pediatr. 2017, 183, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Loret de Mola, C.; Victora, C.G. Breastfeeding and intelligence: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.; Perera, F.; Jankowski, J.; Butscher, M.; Mroz, E.; Flak, E.; Kaim, I.; Lisowska-Miszczyk, I.; Skarupa, A.; Sowa, A. Effect of exclusive breastfeeding on the development of children’s cognitive function in the Krakow prospective birth cohort study. Eur. J. Pediatr. 2012, 171, 151–158. [Google Scholar] [CrossRef] [PubMed]
- WHO. Breastfeeding; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Nyaradi, A.; Li, J.; Hickling, S.; Foster, J.; Oddy, W.H. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front. Hum. Neurosci. 2013, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Hunter, S.; Kuzik, N.; Wiebe, S.A.; Spence, J.C.; Friedman, A.; Tremblay, M.S.; Slater, L.; Hinkley, T. Systematic review of physical activity and cognitive development in early childhood. J. Sci. Med. Sport 2016, 19, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Worobey, J. Physical activity in infancy: Developmental aspects, measurement, and importance. Am. J. Clin. Nutr. 2014, 99, 729S–733S. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Normal-Weight | Overweight | Obesity | p | |||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |||||
| Maternal characteristics | n | n | n | ||||
| Age (years) | 34 | 31 (4) | 27 | 32 (4) | 17 | 32 (4) | 0.492 |
| Pre-pregnancy BMI (kg/m2) | 34 | 22.14 (1.54) a | 27 | 27.59 (1.35) b | 17 | 33.40 (2.65) c | <0.001 * |
| Weight Gain (kg) | 25 | 13.17 (3.55) | 23 | 10.32 (5.20) | 15 | 9.14 (7.06) | 0.042 |
| Education (%) | 0.660 | ||||||
| <High school | 26 | 14.71 | 19 | 11.11 | 11 | 23.53 | |
| High school | 3 | 8.82 | 5 | 18.52 | 2 | 11.76 | |
| >High school | 5 | 76.47 | 3 | 70.37 | 4 | 64.71 | |
| Smoking during pregnancy (%) | 0.415 | ||||||
| No, never | 17 | 77.27 | 15 | 71.43 | 10 | 73.68 | |
| Yes | 3 | 13.64 | 5 | 23.81 | 1 | 7.14 | |
| Quit | 2 | 9.09 | 1 | 4.76 | 3 | 21.43 | |
| Maternal dietary intake | |||||||
| Energy (Kcal/day) | 27 | 2066.37 (261.93) | 23 | 2089.59 (542.07) | 12 | 2058.08 (469.97) | 0.961 |
| Lipids (g) | 27 | 86.89 (17.29) | 23 | 85.25 (25.86) | 12 | 93.23 (20.95) | 0.468 |
| Lipids (%) | 27 | 37.76 (5.26) | 23 | 39.04 (7.73) | 12 | 41.17 (5.38) | 0.307 |
| SFA(g/d) | 27 | 30.81 (6.36) | 23 | 30.05 (8.67) | 12 | 34.19 (5.87) | 0.203 |
| MUFA (g/d) | 27 | 36.53 (10.92) | 23 | 39.33 (17.63) | 12 | 36.32 (12.08) | 0.926 |
| PUFA(g/d) | 27 | 12.10 (3.17) | 23 | 13.34 (6.59) | 12 | 14.63 (3.95) | 0.285 |
| n6 PUFA (g/d) | 27 | 2.48 (1.95) | 23 | 2.89 (2.53) | 12 | 3.44 (1.50) | 0.122 |
| n3 PUFA (g/d) | 27 | 0.18 (0.11) | 23 | 0.21 (0.13) | 12 | 0.20 (0.09) | 0.427 |
| n-3 from fish (g/d) | 27 | 0.36 (0.31) | 23 | 0.28 (0.34) | 12 | 0.45 (0.34) | 0.690 |
| AA (g/d) | 27 | 0.11 (0.06) a | 23 | 0.17 (0.08) b | 12 | 0.16 (0.08) ab | 0.005 |
| EPA(g/d) | 27 | 0.12 (0.11) | 23 | 0.09 (0.11) | 12 | 0.16 (0.12) | 0.213 |
| DHA (g/d) | 27 | 0.24 (0.18) | 23 | 0.22 (0.21) | 12 | 0.31 (0.21) | 0.269 |
| n6:n3 | 27 | 12.99 (2.98) a | 23 | 13.53 (3.40) a | 12 | 19.12 (8.94) b | 0.004 |
| Infant characteristics | |||||||
| Sex, male (%) | 14 | 41.18 | 11 | 40.74 | 7 | 41.18 | 0.999 |
| Birth weight (g) | 32 | 3359.06 (352.35) | 27 | 3340.37 (511.85) | 16 | 3532.35 (389.61) | 0.277 |
| Birth length (cm) | 31 | 50.52 (1.57) | 27 | 50.30 (1.88) | 16 | 51.22 (1.80) | 0.245 |
| Birth head Circumference (cm) | 26 | 34.31 (1.36) | 22 | 34.36 (1.39) | 16 | 34.69 (1.40) | 0.674 |
| Placenta (g) | 30 | 496.67 (144.11) | 25 | 509.20 (130.25) | 16 | 568.13 (143.17) | 0.332 |
| Newborn according Lubchenco curves # (%) | 0.627 | ||||||
| SGA | 0 | 0.00 | 1 | 4.55 | 0 | 0.00 | |
| AGA | 26 | 81.25 | 16 | 72.73 | 11 | 73.33 | |
| LGA | 6 | 18.75 | 5 | 22.73 | 4 | 26.67 | |
| Breastfeeding † (%) | 0.290 | ||||||
| Exclusive | 16 | 53.33 | 16 | 66.67 | 8 | 50.00 | |
| Mixt | 10 | 33.33 | 3 | 12.50 | 3 | 18.75 | |
| Artificial | 4 | 13.33 | 5 | 20.83 | 5 | 31.25 | |
| Normal-Weight | Overweight | Obesity | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Colostrum (n = 26) | Mature Milk (n = 20) | p | Colostrum (n = 21) | Mature Milk (n = 23) | p | Colostrum (n = 16) | Mature Milk (n = 14) | p | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||||
| C6:0 | 0.06 (0.04) | 0.08 (0.03) | 0.19 | 0.05 (0.03) | 0.10 (0.04) | <0.001 * | 0.05 (0.03) | 0.08 (0.07) | 0.002 * |
| C8:0 | 0.13 (0.09) | 0.23 (0.07) | 0.002 * | 0.13 (0.08) | 0.24 (0.09) | <0.001 * | 0.08 (0.03) # | 0.24 (0.10) | <0.001 * |
| C10:0 | 0.86 (0.57) | 1.29 (0.37) | 0.010 | 0.86 (0.47) | 1.36 (0.33) | 0.002 * | 0.70 (0.57) | 1.47 (0.32) | <0.001 * |
| C12:0 | 4.10 (2.07) | 4.86 (1.80) | 0.039 | 4.18 (1.97) | 4.86 (1.92) | 0.14 | 3.67 (2.49) | 5.32 (1.65) | 0.029 |
| C14:0 | 5.15 (1.41) | 4.79 (1.71) | 0.88 | 5.38 (1.92) | 4.67 (1.66) | 0.38 | 5.04 (2.31) | 5.23 (1.22) | 0.32 |
| C14:1 | 0.08 (0.02) | 0.10 (0.03) | 0.20 | 0.11 (0.03) † | 0.11 (0.04) | 0.51 | 0.10 (0.05) | 0.12 (0.06) | 0.10 |
| C15:0 | 0.21 (0.03) | 0.21 (0.06) | 0.80 | 0.24 (0.04) † | 0.20 (0.05) | 0.016 | 0.19 (0.04) # | 0.22 (0.08) | 0.32 |
| C16:0 | 21.13 (2.32) | 19.56 (2.29) | 0.006 | 21.24 (1.46) | 19.53 (2.02) | 0.001 * | 21.96 (2.11) | 21.20 (2.55) # | 0.42 |
| C16:1t | 0.12 (0.03) | 0.13 (0.04) | 0.59 | 0.14 (0.04) | 0.11 (0.05) | 0.06 | 0.13 (0.04) | 0.13 (0.06) | 0.98 |
| C16:1n9 | 0.50 (0.05) | 0.43 (0.06) | <0.001 * | 0.54 (0.13) | 0.45 (0.07) | 0.010 | 0.54 (0.10) | 0.46 (0.10) | 0.024 |
| C16:1n7 | 1.48 (0.45) | 1.83 (0.62) | 0.11 | 1.63 (0.36) | 1.80 (0.49) | 0.014 | 1.78 (0.60) | 1.88 (0.58) | 0.61 |
| C17:0 | 0.30 (0.04) | 0.29 (0.08) | 0.74 | 0.34 (0.03) † | 0.29 (0.06) | 0.026 | 0.29 (0.05) # | 0.32 (0.07) | 0.28 |
| C17:1 | 0.15 (0.03) | 0.17 (0.03) | 0.28 | 0.18 (0.04) † | 0.18 (0.04) | 0.88 | 0.17 (0.07) | 0.17 (0.05) | 0.83 |
| C18:0 | 5.74 (0.67) | 5.74 (0.41) | 0.20 | 5.58 (0.85) | 5.88 (0.67) | 0.12 | 5.44 (0.81) † | 6.03 (0.49) | <0.001 * |
| C18:1n9 | 38.47 (3.51) | 39.69 (4.23) | 0.41 | 38.16 (4.57) | 38.73 (5.53) | 0.87 | 37.36 (3.11) | 36.63 (0.96) † | 0.30 |
| C18:1n9t | 0.33 (0.14) | 0.28 (0.09) | 0.12 | 0.31 (0.09) | 0.26 (0.08) | 0.24 | 0.24 (0.05) †# | 0.22 (0.04) † | 0.15 |
| C18:1n7 | 1.69 (0.22) | 1.58 (0.24) | 0.02 | 1.69 (0.28) | 1.63 (0.23) | 0.81 | 1.89 (0.42) | 1.59 (0.32) | 0.022 |
| C18:1n-7t11 | 0.28 (0.12) | 0.30 (0.12) | 0.95 | 0.28 (0.09) | 0.26 (0.11) | 0.15 | 0.27 (0.14) | 0.24 (0.08) | 0.72 |
| C18:2n6 (LA) | 13.03 (2.42) | 13.60 (3.21) | 0.31 | 13.31 (3.20) | 15.20 (3.86) | 0.050 | 12.98 (2.74) | 13.90 (3.14) | 0.49 |
| C18:2n7c9t11 | 0.12 (0.03) | 0.13 (0.05) | 0.69 | 0.14 (0.04) | 0.12 (0.04) | 0.32 | 0.13 (0.05) | 0.14 (0.06) | 0.67 |
| C18:3n6 | 0.09 (0.04) | 0.17 (0.06) | 0.010 | 0.11 (0.07) | 0.18 (0.05) | <0.001 * | 0.13 (0.09) | 0.17 (0.05) | 0.15 |
| C18:3n3 (ALA) | 0.54 (0.18) | 0.59 (0.21) | 0.61 | 0.53 (0.13) | 0.58 (0.16) | 0.14 | 0.41 (0.04) †# | 0.46 (0.08) †# | 0.16 |
| C20:0 | 0.20 (0.03) | 0.18 (0.01) | 0.012 | 0.18 (0.02) | 0.17 (0.03) | 0.005 | 0.19 (0.04) | 0.18 (0.04) | 0.75 |
| C20:1n9 | 0.77 (0.20) | 0.50 (0.07) | <0.001 * | 0.74 (0.26) | 0.46 (0.05) | <0.001 * | 0.77 (0.24) | 0.48 (0.06) | <0.001 * |
| C20:3n6 | 0.60 (0.15) | 0.47 (0.11) | <0.001 * | 0.65 (0.21) | 0.48 (0.06) | 0.004 | 0.68 (0.24) | 0.52 (0.14) | 0.05 |
| C20:4n6 (AA) | 0.67 (0.19) | 0.49 (0.05) | 0.005 | 0.66 (0.13) | 0.49 (0.12) | <0.001 * | 0.67 (0.23) | 0.47 (0.10) | 0.004 |
| C20:5n3 (EPA) | 0.05 (0.02) | 0.07 (0.03) | 0.07 | 0.04 (0.02) | 0.06 (0.02) | <0.001 * | 0.05 (0.03) | 0.07 (0.02) | 0.10 |
| C22:0 | 0.08 (0.03) | 0.06 (0.02) | 0.007 | 0.09 (0.03) | 0.08 (0.03) | 0.20 | 0.08 (0.02) | 0.07 (0.02) | 0.039 |
| C22:1n9 | 0.18 (0.06) | 0.09 (0.02) | <0.001 * | 0.19 (0.08) | 0.09 (0.02) | <0.001 * | 0.18 (0.06) | 0.09 (0.01) | <0.001 * |
| C22:2n6 | 0.07 (0.03) | 0.04 (0.01) | 0.003 | 0.08 (0.03) | 0.06 (0.03) | 0.22 | 0.06 (0.02) | 0.06 (0.02) † | 0.22 |
| C22:4n6 | 0.25 (0.13) | 0.10 (0.02) | <0.001 * | 0.28 (0.15) | 0.12 (0.04) | <0.001 * | 0.37 (0.27) | 0.12 (0.03) | <0.001 * |
| C22:5n6 | 0.12 (0.04) | 0.05 (0.01) | <0.001 * | 0.12 (0.05) | 0.07 (0.03) † | 0.048 | 0.12 (0.05) | 0.09 (0.05) † | 0.040 |
| C22:5n3 | 0.16 (0.08) | 0.11 (0.03) | 0.012 | 0.14 (0.05) | 0.11 (0.03) | 0.002 * | 0.19 (0.09) | 0.12 (0.04) | 0.007 |
| C22:6n3 (DHA) | 0.41 (0.14) | 0.28 (0.11) | <0.001 * | 0.35 (0.08) | 0.22 (0.06 † | <0.001 * | 0.39 (0.13) | 0.25 (0.07) | 0.002 * |
| C23:0 | 0.12 (0.05) | 0.05 (0.02) | <0.001 * | 0.12 (0.05) | 0.06 (0.03) | <0.001 * | 0.13 (0.05) | 0.09 (0.07) † | 0.06 |
| C24:0 | 0.10 (0.03) | 0.05 (0.02) | 0.002 * | 0.10 (0.04) | 0.06 (0.03) | 0.007 | 0.09 (0.03) | 0.06 (0.03) | 0.031 |
| C24:1 | 0.20 (0.11) | 0.06 (0.02) | <0.001 * | 0.19 (0.13) | 0.06 (0.04) | <0.001 * | 0.19 (0.09) | 0.07 (0.03) | <0.001 * |
| EPA:AA | 0.07 (0.03) | 0.12 (0.03) | 0.005 | 0.06 (0.03) | 0.09 (0.04) † | <0.001 * | 0.07 (0.03) | 0.12 (0.07) | 0.004 |
| DHA:AA | 0.63 (0.22) | 0.77 (0.19) | 0.005 | 0.55 (0.13) | 0.76 (0.24) | <0.001 * | 0.61 (0.21) | 0.90 (0.34) | 0.004 |
| SFA | 27.45 (2.66) | 25.83 (2.48) | 0.008 | 27.43 (1.93) | 25.95 (2.49) | 0.004 | 27.96 (2.34) | 27.80 (2.62) †,# | 0.96 |
| MCFA | 5.14 (2.69) | 6.46 (2.19) | 0.021 | 5.23 (2.46) | 6.56 (2.27) | 0.037 | 4.50 (3.06) | 7.11 (1.99) | 0.010 |
| MUFA | 42.80 (3.51) | 43.73 (4.17) | 0.87 | 42.61 (4.91) | 42.76 (5.70) | 0.74 | 42.17 (3.56) | 40.74 (1.37) † | 0.12 |
| n6 PUFA | 15.41 (2.53) | 15.24 (3.31) | 0.77 | 15.79 (3.23) | 16.89 (3.93) | 0.29 | 15.67 (3.01) | 15.64 (3.19) | 0.93 |
| n3 PUFA | 1.16 (0.30) | 1.05 (0.24) | 0.018 | 1.07 (0.15) | 0.96 (0.21) | 0.12 | 1.04 (0.23) | 0.90 (0.13) | 0.06 |
| n6 LC-PUFA | 2.30 (0.59) | 1.48 (0.22) | <0.001 * | 2.36 (0.63) | 1.52 (0.24) | <0.001 * | 2.56 (0.93) | 1.58 (0.34) | <0.001 * |
| n3 LC-PUFA | 0.62 (0.22) | 0.45 (0.16) | <0.001 * | 0.54 (0.12) | 0.38 (0.11) | <0.001 * | 0.63 (0.23) | 0.44 (0.09) | 0.008 |
| n6:n3 PUFA | 14.28 (4.76) | 15.08 (3.91) | 0.06 | 15.13 (4.37) | 18.28 (5.33) † | 0.033 | 15.67 (4.22) | 17.80 (4.97) | 0.15 |
| n6:n3 LC-PUFA | 4.00 (1.16) | 3.62 (1.18) | 0.08 | 4.49 (0.95) | 4.28 (1.24) | 0.41 | 4.23 (1.05) | 3.73 (0.92) | 0.14 |
| Fatty Acid | BMIZ | WAZ | LAZ | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Colostrum | Mature Milk | Colostrum | Mature Milk | Colostrum | Mature Milk | |||||||
| 6mo n = 37 | 6mo n = 39 | 6mo n = 37 | 6mo n = 39 | 6mo n = 38 | 6mo n = 39 | |||||||
| 18mo n = 38 | 18mo n = 37 | 18mo n = 38 | 18mo n = 38 | 18mo n = 38 | 18mo n = 38 | |||||||
| 36mo n = 16 | 36mo n = 13 | 36mo n = 16 | 36mo n = 13 | 36mo n = 18 | 36mo n = 14 | |||||||
| β | p | β | p | β | p | β | p | β | p | β | p | |
| C18:3n3 (ALA) | ||||||||||||
| 6mo | −0.11 | 0.63 | −0.15 | 0.40 | −0.06 | 0.77 | −0.22 | 0.24 | 0.05 | 0.80 | −0.12 | 0.49 |
| 18mo | 0.32 | 0.13 | −0.11 | 0.57 | 0.11 | 0.63 | −0.13 | 0.51 | −0.20 | 0.26 | −0.06 | 0.69 |
| 36mo | −0.44 | 0.21 | 0.01 | 0.99 | −0.27 | 0.52 | 0.06 | 0.95 | −0.17 | 0.63 | −0.86 | 0.22 |
| C18:2n6 (LA) | ||||||||||||
| 6mo | 0.33 | 0.12 | −0.13 | 0.43 | 0.42 | 0.027 | 0.16 | 0.36 | 0.15 | 0.40 | 0.09 | 0.60 |
| 18mo | −0.19 | 0.34 | 0.04 | 0.85 | 0.18 | 0.37 | 0.05 | 0.79 | 0.06 | 0.73 | 0.17 | 0.26 |
| 36mo | 0.12 | 0.75 | −0.22 | 0.50 | 0.02 | 0.96 | −0.136 | 0.75 | 0.01 | 0.98 | −0.33 | 0.41 |
| C20:4n6 (AA) | ||||||||||||
| 6mo | −0.44 | 0.016 | 0.02 | 0.91 | −0.20 | 0.26 | 0.04 | 0.84 | 0.25 | 0.13 | 0.03 | 0.86 |
| 18mo | −0.03 | 0.89 | −0.12 | 0.57 | 0.06 | 0.77 | −0.13 | 0.52 | 0.10 | 0.50 | 0.15 | 0.39 |
| 36mo | 0.30 | 0.30 | 0.09 | 0.81 | 0.42 | 0.20 | 0.07 | 0.86 | 0.20 | 0.48 | 0.12 | 0.75 |
| C20:5n3 (EPA) | ||||||||||||
| 6mo | −0.51 | 0.012 | 0.00 | 0.99 | −0.36 | 0.07 | −0.13 | 0.49 | 0.18 | 0.31 | −0.18 | 0.29 |
| 18mo | −0.30 | 0.12 | 0.00 | 0.98 | −0.13 | 0.51 | 0.08 | 0.66 | 0.15 | 0.35 | 0.09 | 0.62 |
| 36mo | −0.74 | 0.155 | −1.08 | 0.30 | −0.58 | 0.34 | −1.13 | 0.28 | 0.14 | 0.69 | −0.59 | 0.61 |
| C22:6n3 (DHA) | ||||||||||||
| 6mo | −0.37 | 0.043 | −0.16 | 0.38 | −0.31 | 0.07 | −0.29 | 0.10 | 0.00 | 0.99 | −0.23 | 0.17 |
| 18mo | 0.14 | 0.42 | 0.03 | 0.88 | 0.08 | 0.66 | 0.00 | 0.99 | −0.05 | 0.74 | −0.03 | 0.84 |
| 36mo | 0.42 | 0.29 | 0.33 | 0.46 | 0.65 | 0.13 | 0.38 | 0.39 | 0.46 | 0.22 | 0.58 | 0.14 |
| n6 PUFA | ||||||||||||
| 6mo | 0.21 | 0.32 | 0.13 | 0.45 | 0.34 | 0.07 | 0.16 | 0.35 | 0.20 | 0.27 | 0.10 | 0.55 |
| 18mo | 0.16 | 0.41 | −0.06 | 0.776 | 0.18 | 0.40 | 0.04 | 0.83 | 0.08 | 0.65 | 0.18 | 0.23 |
| 36mo | 0.20 | 0.587 | −0.19 | 0.64 | 0.15 | 0.72 | −0.11 | 0.79 | 0.07 | 0.84 | −0.31 | 0.44 |
| n3 PUFA | ||||||||||||
| 6mo | −0.38 | 0.047 | −0.19 | 0.27 | −0.33 | 0.07 | −0.32 | 0.07 | −0.00 | 0.991 | −0.22 | 0.18 |
| 18mo | 0.16 | 0.38 | −0.11 | 0.56 | 0.04 | 0.84 | −0.11 | 0.53 | −0.12 | 0.427 | −0.05 | 0.75 |
| 36mo | −0.20 | 0.60 | 0.17 | 0.78 | 0.05 | 0.90 | 0.21 | 0.74 | 0.05 | 0.897 | −0.18 | 0.77 |
| n6 LC−PUFA | ||||||||||||
| 6mo | −0.38 | 0.047 | −0.06 | 0.77 | −0.17 | 0.36 | 0.00 | 0.98 | 0.19 | 0.253 | 0.09 | 0.65 |
| 18mo | −0.05 | 0.77 | −0.27 | 0.19 | 0.03 | 0.88 | −0.17 | 0.41 | 0.10 | 0.508 | 0.19 | 0.25 |
| 36mo | 0.40 | 0.22 | 0.11 | 0.78 | 0.60 | 0.09 | 0.12 | 0.76 | 0.25 | 0.390 | −0.03 | 0.95 |
| n3 LC−PUFA | ||||||||||||
| 6mo | −0.43 | 0.020 | −0.19 | 0.28 | −0.34 | 0.05 | −0.33 | 0.06 | 0.03 | 0.866 | −0.24 | 0.16 |
| 18mo | 0.07 | 0.70 | −0.04 | 0.82 | 0.05 | 0.78 | −0.02 | 0.90 | −0.01 | 0.955 | 0.02 | 0.89 |
| 36mo | 0.28 | 0.44 | 0.19 | 0.63 | 0.53 | 0.18 | 0.21 | 0.59 | 0.42 | 0.211 | 0.40 | 0.31 |
| n6:n3 | ||||||||||||
| 6mo | 0.42 | 0.031 | 0.30 | 0.10 | 0.45 | 0.011 | 0.45 | 0.013 | 0.11 | 0.519 | 0.30 | 0.08 |
| 18mo | −0.04 | 0.82 | 0.05 | 0.78 | 0.06 | 0.74 | 0.14 | 0.47 | 0.14 | 0.369 | 0.21 | 0.19 |
| 36mo | 0.30 | 0.34 | −0.23 | 0.55 | 0.05 | 0.88 | −0.18 | 0.65 | 0.01 | 0.978 | −0.26 | 0.58 |
| LC n6:n3 | ||||||||||||
| 6mo | 0.12 | 0.56 | 0.14 | 0.41 | 0.22 | 0.24 | 0.29 | 0.09 | 0.15 | 0.373 | 0.24 | 0.13 |
| 18mo | −0.13 | 0.48 | −0.08 | 0.66 | −0.04 | 0.86 | −0.05 | 0.77 | 0.11 | 0.490 | 0.07 | 0.65 |
| 36mo | 0.35 | 0.54 | −0.07 | 0.86 | 0.16 | 0.81 | −0.08 | 0.85 | −0.31 | 0.516 | −0.30 | 0.46 |
| Fatty Acid | All | Normal-Weight | Overweight | Obesity | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Colostrum (n = 75) | Mature Milk (n = 77) | Colostrum (n = 14) | Mature Milk (n = 12) | Colostrum (n = 11) | Mature Milk (n = 15) | Colostrum (n = 12) | Mature Milk (n = 11) | |||||||||
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| C18:3n3 (ALA) | 0.08 | 0.718 | 0.01 | 0.942 | 0.29 | 0.581 | 0.82 | 0.212 | 0.44 | 0.393 | −0.15 | 0.662 | 0.55 | 0.468 | 2.34 | 0.008 |
| C18:2n6 (LA) | 0.20 | 0.339 | 0.12 | 0.527 | 0.84 | <0.001 * | 0.88 | 0.069 | −0.95 | 0.061 | −0.16 | 0.687 | 0.12 | 0.869 | 0.53 | 0.470 |
| C20:4n6 (AA) | 0.03 | 0.889 | −0.20 | 0.333 | −1.23 | 0.136 | −0.56 | 0.270 | 0.32 | 0.594 | −0.28 | 0.544 | 0.48 | 0.416 | −0.87 | 0.405 |
| C20:5n3 (EPA) | 0.31 | 0.133 | −0.11 | 0.580 | 0.00 | 0.996 | 0.59 | 0.428 | −0.07 | 0.932 | −0.18 | 0.635 | 0.80 | 0.233 | −0.29 | 0.658 |
| C22:6n3 (DHA) | −0.16 | 0.396 | −0.27 | 0.161 | −0.73 | 0.124 | −0.19 | 0.720 | 0.88 | 0.045 | 0.33 | 0.362 | −0.03 | 0.954 | −1.16 | 0.104 |
| n6 PUFA | 0.24 | 0.251 | 0.13 | 0.495 | 0.81 | 0.002 * | 0.88 | 0.064 | −0.97 | 0.111 | −0.15 | 0.713 | 0.16 | 0.803 | 0.45 | 0.520 |
| n3 PUFA | −0.01 | 0.966 | −0.12 | 0.541 | −0.23 | 0.687 | 0.37 | 0.512 | 0.70 | 0.057 | −0.04 | 0.922 | 0.13 | 0.829 | −0.78 | 0.489 |
| n6 LC-PUFA | 0.14 | 0.446 | 0.18 | 0.407 | 0.01 | 0.984 | 0.31 | 0.536 | 0.53 | 0.227 | 0.36 | 0.481 | 0.28 | 0.650 | −0.09 | 0.924 |
| n3 LC-PUFA | −0.11 | 0.563 | −0.25 | 0.190 | −0.71 | 0.113 | −0.08 | 0.873 | 1.01 | 0.004 | 0.21 | 0.585 | 0.04 | 0.949 | −0.89 | 0.189 |
| n6:n3 | 0.13 | 0.489 | 0.22 | 0.255 | 0.74 | 0.067 | 0.29 | 0.639 | −0.97 | 0.002 * | −0.10 | 0.805 | 0.01 | 0.985 | 0.57 | 0.426 |
| LC n6:n3 | 0.27 | 0.166 | 0.29 | 0.105 | 0.52 | 0.172 | 0.16 | 0.752 | 0.05 | 0.952 | −0.08 | 0.830 | 0.22 | 0.696 | 0.83 | 0.286 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Garza Puentes, A.; Martí Alemany, A.; Chisaguano, A.M.; Montes Goyanes, R.; Castellote, A.I.; Torres-Espínola, F.J.; García-Valdés, L.; Escudero-Marín, M.; Segura, M.T.; Campoy, C.; et al. The Effect of Maternal Obesity on Breast Milk Fatty Acids and Its Association with Infant Growth and Cognition—The PREOBE Follow-Up. Nutrients 2019, 11, 2154. https://doi.org/10.3390/nu11092154
de la Garza Puentes A, Martí Alemany A, Chisaguano AM, Montes Goyanes R, Castellote AI, Torres-Espínola FJ, García-Valdés L, Escudero-Marín M, Segura MT, Campoy C, et al. The Effect of Maternal Obesity on Breast Milk Fatty Acids and Its Association with Infant Growth and Cognition—The PREOBE Follow-Up. Nutrients. 2019; 11(9):2154. https://doi.org/10.3390/nu11092154
Chicago/Turabian Stylede la Garza Puentes, Andrea, Adrià Martí Alemany, Aida Maribel Chisaguano, Rosa Montes Goyanes, Ana I. Castellote, Franscisco J. Torres-Espínola, Luz García-Valdés, Mireia Escudero-Marín, Maria Teresa Segura, Cristina Campoy, and et al. 2019. "The Effect of Maternal Obesity on Breast Milk Fatty Acids and Its Association with Infant Growth and Cognition—The PREOBE Follow-Up" Nutrients 11, no. 9: 2154. https://doi.org/10.3390/nu11092154