Body Mass Index, Lean Mass, and Body Fat Percentage as Mediators of the Relationship between Milk Consumption and Bone Health in Young Adults

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Ethics Approval and Consent to Participate
2.4. Variables and Measuring Instruments
2.5. Statistical Analysis
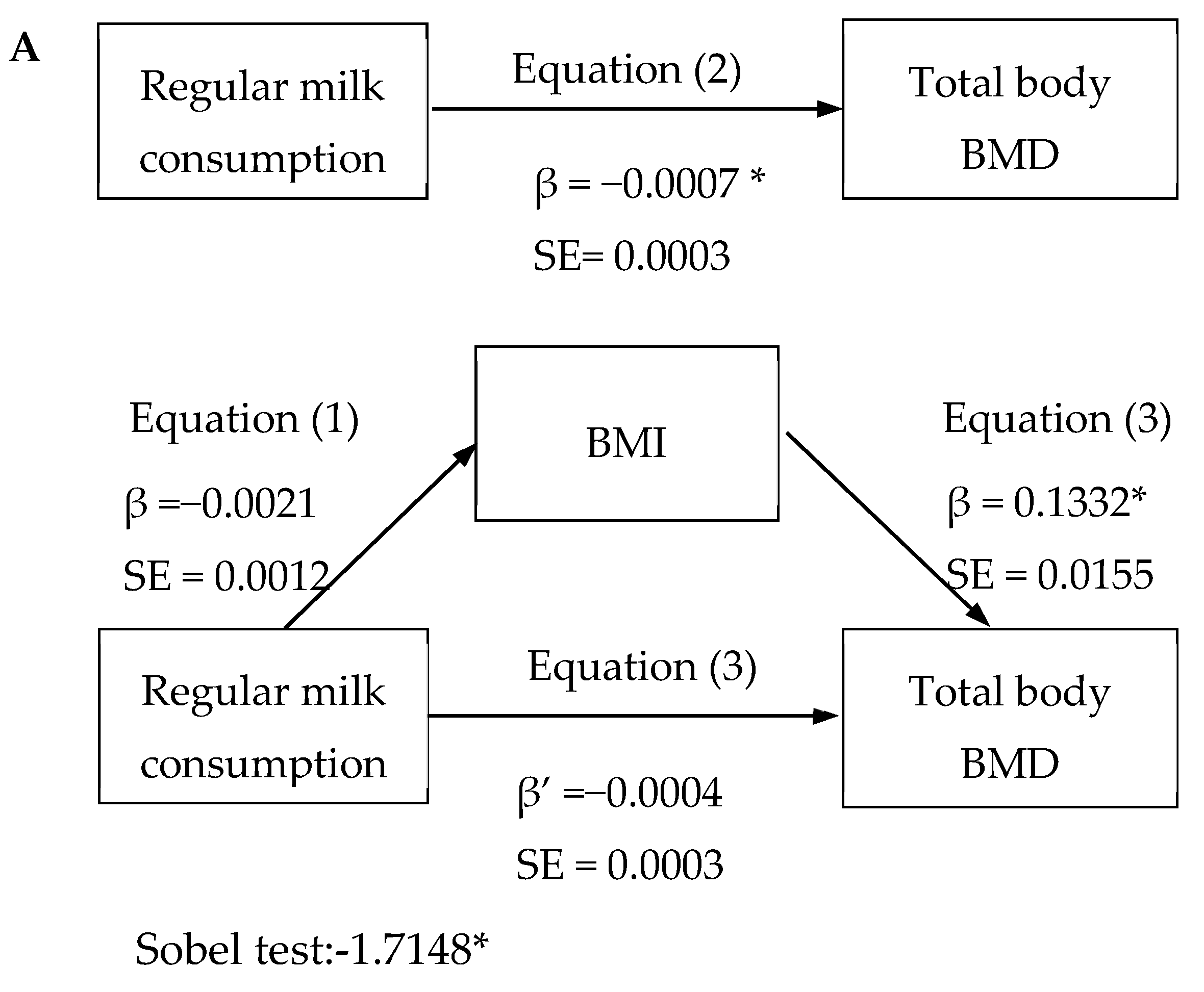
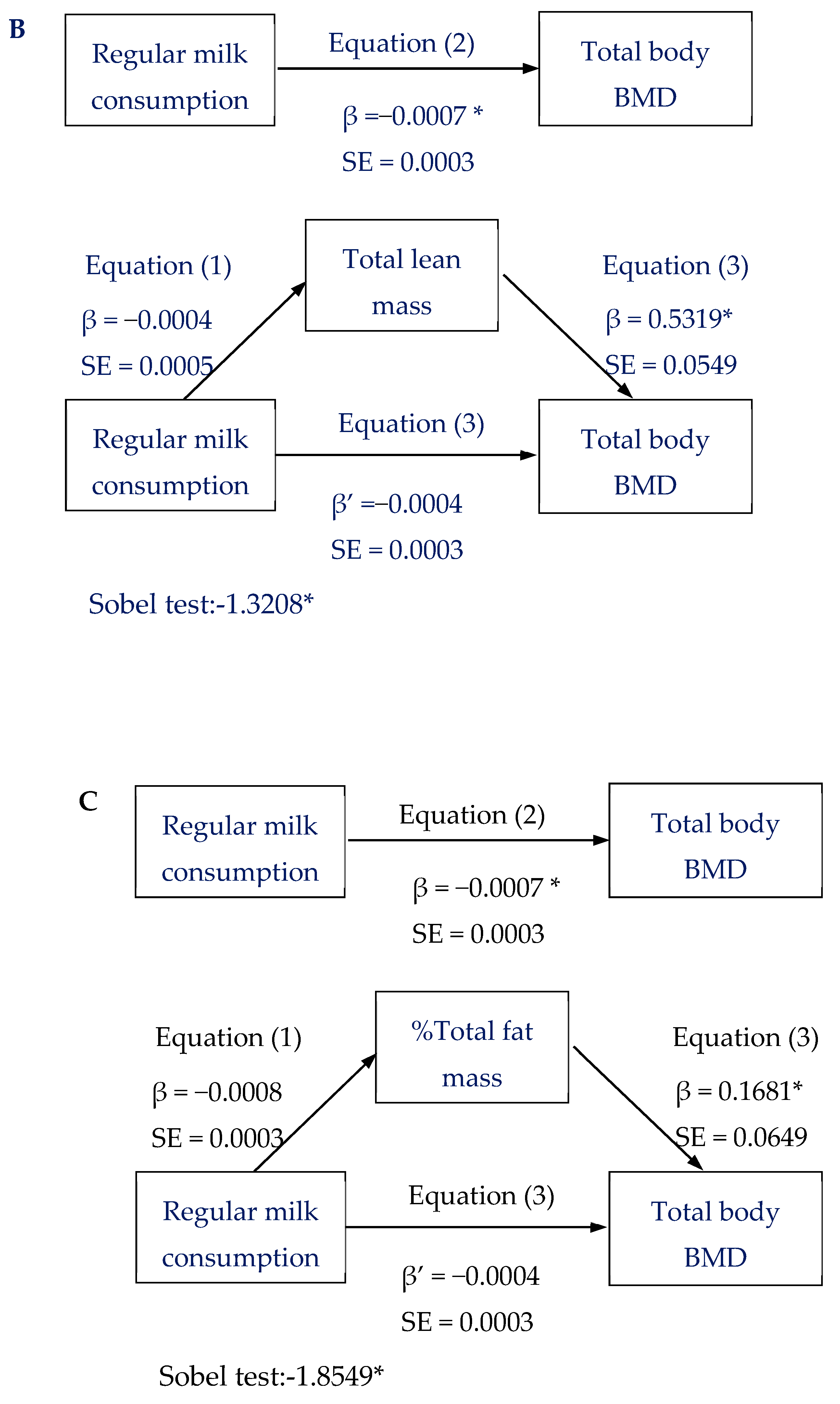
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rizzoli, R.; Bonjour, J.; Ferrari, S.L. Osteoporosis, genetics and hormones. J. Mol. Endocrinol. 2001, 26, 79–94. [Google Scholar] [Green Version]
- Borrelli, J. The Relationship of Peak Bone Mass, Aging, and Bone Loss to Osteoporosis and Fragility Fractures. In Arthroplasty for the Treatment of Fractures in the Older Patient; Springer: Cham, Switzerland, 2018; pp. 3–17. [Google Scholar]
- Rizzoli, R.; Bianchi, M.L.; Garabedian, M.; McKay, H.A.; Moreno, L.A. Maximizing bone mineral mass gain during growth for the prevention of fractures in the adolescents and the elderly. Bone 2010, 46, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Baxter-Jones, A.D.; Eisenmann, J.C.; Mirwald, R.L.; Faulkner, R.A.; Bailey, D.A. The influence of physical activity on lean mass accrual during adolescence: A longitudinal analysis. J. Appl. Physiol. 2008, 105, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Rodríguez, G.; Ara, I.; Pérez-Gómez, J.; Dorado, C.; Calbet, J.A. Muscular development and physical activity as major determinants of femoral bone mass acquisition during growth. Br. J. Sports Med. 2005, 39, 611–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, C.M.; Zemel, B.S.; Wren, T.A.; Leonard, M.B.; Bachrach, L.K.; Rauch, F.; Gilsanz, V.; Rosen, C.J.; Winer, K.K. The determinants of peak bone mass. J. Pediatr. 2017, 180, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Gracia-Marco, L.; Ortega, F.; Jimenez-Pavon, D.; Rodriguez, G.; Castillo, M.; Vicente-Rodriguez, G.; Moreno, L.A. Adiposity and bone health in Spanish adolescents. The HELENA study. Osteoporos. Int. 2012, 23, 937–947. [Google Scholar] [CrossRef]
- Rocher, E.; Chappard, C.; Jaffre, C.; Benhamou, C.-L.; Courteix, D. Bone mineral density in prepubertal obese and control children: Relation to body weight, lean mass, and fat mass. J. Bone Miner. Metab. 2008, 26, 73–78. [Google Scholar] [CrossRef]
- Winther, A.; Jørgensen, L.; Ahmed, L.A.; Christoffersen, T.; Furberg, A.-S.; Grimnes, G.; Jorde, R.; Nilsen, O.A.; Dennison, E.; Emaus, N. Bone mineral density at the hip and its relation to fat mass and lean mass in adolescents: The Tromsø Study, Fit Futures. BMC Musculoskelet. Disord. 2018, 19, 21. [Google Scholar] [CrossRef]
- Wang, M.; Bachrach, L.; Van Loan, M.; Hudes, M.; Flegal, K.; Crawford, P. The relative contributions of lean tissue mass and fat mass to bone density in young women. Bone 2005, 37, 474–481. [Google Scholar] [CrossRef]
- Marangoni, F.; Pellegrino, L.; Verduci, E.; Ghiselli, A.; Bernabei, R.; Calvani, R.; Cetin, I.; Giampietro, M.; Perticone, F.; Piretta, L.; et al. Cow’s milk consumption and health: A health professional’s guide. J. Am. Coll. Nutr. 2019, 38, 197–208. [Google Scholar] [CrossRef]
- Mensink, G.; Fletcher, R.; Gurinovic, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vissers, P.A.; Streppel, M.T.; Feskens, E.J.; de Groot, L.C. The contribution of dairy products to micronutrient intake in the Netherlands. J. Am. Coll. Nutr. 2011, 30, 415S–421S. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P. Ethnicity, bone status, and the calcium requirement. Nutr. Res. 2002, 22, 153–178. [Google Scholar] [CrossRef]
- De Beer, H. Dairy products and physical stature: A systematic review and meta-analysis of controlled trials. Econ. Hum. Biol. 2012, 10, 299–309. [Google Scholar] [CrossRef] [PubMed]
- De Lamas, C.; de Castro, M.J.; Gil-Campos, M.; Gil, Á.; Couce, M.L.; Leis, R. Effects of dairy product consumption on height and bone mineral content in children: A systematic review of controlled trials. Adv. Nutr. 2019, 10, S88–S96. [Google Scholar]
- Dietary. Guidelines for Americans, 8th ed.; USA. gov 2015. Available online: https://health.gov/dietaryguidelines/2015/ (accessed on 20 June 2019).
- Dougkas, A.; Barr, S.; Reddy, S.; Summerbell, C.D. A critical review of the role of milk and other dairy products in the development of obesity in children and adolescents. Nutr. Res. Rev. 2019, 32, 106–127. [Google Scholar] [CrossRef]
- Mataix Verdú, J. Tablas de Composición de Alimentos, 4th ed.; Universidad de Granada: Granada, Spain, 2003. [Google Scholar]
- Tuni, O.M.; Carbajal, A.; Forneiro, L.C.; Vives, C.C. Spanish Food Composition Tables (Tablas de Composición de Alimentos), 7th ed.; Pirámide: Madrid, Spain, 2003. [Google Scholar]
- Chilet-Rosell, E.; Álvarez-Dardet, C.; Domingo-Salvany, A. Utilización de las propuestas españolas de medición de la clase social en salud. Gac. Sanit. 2012, 26, 566–569. [Google Scholar] [CrossRef]
- Da Silva, I.C.; van Hees, V.T.; Ramires, V.V.; Knuth, A.G.; Bielemann, R.M.; Ekelund, U.; Brage, S.; Hallal, P.C. Physical activity levels in three Brazilian birth cohorts as assessed with raw triaxial wrist accelerometry. Int. J. Epidemiol. 2014, 43, 1959–1968. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The Moderator–Mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Weaver, C.; Gordon, C.; Janz, K.; Kalkwarf, H.; Lappe, J.M.; Lewis, R.; O’Karma, M.; Wallace, T.C.; Zemel, B.S. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: A systematic review and implementation recommendations. Osteoporos. Int. 2016, 27, 1281–1386. [Google Scholar] [CrossRef] [PubMed]
- Dror, D.K.; Allen, L.H. Dairy product intake in children and adolescents in developed countries: Trends, nutritional contribution, and a review of association with health outcomes. Nutr. Rev. 2014, 72, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R. Dairy products, yogurts, and bone health. Am. J. Clin. Nutr. 2014, 99, 1256S–1262S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Villegas, A.; Martinez, J.; Prättälä, R.; Toledo, E.; Roos, G.; Martinez-Gonzalez, M. A systematic review of socioeconomic differences in food habits in Europe: Consumption of cheese and milk. Eur. J. Clin. Nutr. 2003, 57, 917. [Google Scholar] [CrossRef] [PubMed]
- Berro, A.-J.; Ayoub, M.-L.; Pinti, A.; Ahmaidi, S.; El Khoury, G.; El Khoury, C.; Zakhem, E.; Cortet, B.; El Hage, R. Trabecular Bone Score in Overweight and Normal-Weight Young Women. In International Conference on Bioinformatics and Biomedical Engineering; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Iwaniec, U.T.; Turner, R.T. Influence of body weight on bone mass, architecture and turnover. J. Endocrinol. 2016, 230, R115–R130. [Google Scholar] [CrossRef]
- Suthutvoravut, U.; Abiodun, P.O.; Chomtho, S.; Chongviriyaphan, N.; Cruchet, S.; Davies, P.S.; Fuchs, G.J.; Gopalan, S.; van Goudoever, J.B.; Nel Ede, L.; et al. Composition of follow-up formula for young children aged 12-36 months: Recommendations of an international expert group coordinated by the Nutrition Association of Thailand and the Early Nutrition Academy. Ann. Nutr. Metab. 2015, 67, 119–132. [Google Scholar] [CrossRef]
- Marques-Vidal, P.; Goncalves, A.; Dias, C. Milk intake is inversely related to obesity in men and in young women: Data from the Portuguese Health Interview Survey 1998–1999. Int. J. Obes. 2006, 30, 88. [Google Scholar] [CrossRef]
- Lu, L.; Xun, P.; Wan, Y.; He, K.; Cai, W. Long-Term association between dairy consumption and risk of childhood obesity: A systematic review and meta-analysis of prospective cohort studies. Eur. J. Clin. Nutr. 2016, 70, 414. [Google Scholar] [CrossRef]
- Frost, H.M. Bone’s mechanostat: A 2003 update. In The Anatomical Record Part A, Discoveries in Molecular, Cellular, and Evolutionary Biology; The American Association of Anatomists: Rockville, MD, USA, 2003; Volume 275, pp. 1081–1101. [Google Scholar] [CrossRef]
- Petak, S.; Barbu, C.G.; Elaine, W.Y.; Fielding, R.; Mulligan, K.; Sabowitz, B.; Wu, C.H.; Shepherd, J.A. The Official Positions of the International Society for Clinical Densitometry: Body composition analysis reporting. J. Clin. Densitom. 2013, 16, 508–519. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (239) | Boys (79) | Girls (160) | p | |
|---|---|---|---|---|
| Age (years) | 21.44 ± 3.36 | 21.31 ± 2.52 | 21.51 ± 3.71 | n.s. |
| Weight (kg) | 64.33 ± 2.12 | 70.75 ± 10.62 | 61.15 ± 11.57 | <0.001 |
| Height (cm) | 166.26 ± 8.36 | 174.11 ± 6.99 | 162.44 ± 5.96 | <0.001 |
| BMI (kg/m2) | 23.17 ± 3.60 | 23.24 ± 2.64 | 23.14 ± 3.99 | n.s. |
| %Total fat mass | 26.66 ± 10.00 | 18.85 ± 6.85 | 30.68 ± 8.95 | <0.001 |
| Total lean mass (Kg) | 43.04 ± 9.31 | 53.54 ± 6.83 | 37.82 ± 4.96 | <0.001 |
| Total body BMD (g/cm2) | 1.131 ± 0.111 | 1.197 ± 0.121 | 1.099 ± 0.092 | <0.001 |
| Spine BMD (g/cm2) | 1.045 ± 0.129 | 1.075 ± 0.152 | 1.030 ± 0.113 | 0.010 |
| Pelvis BMD (g/cm2) | 1.061 ± 0.147 | 1.141 ± 0.159 | 1.022 ± 0.123 | <0.001 |
| Regular milk (mL/d) | 87.27 ± 199.24 | 127.38 ± 233.68 | 67.97 ± 177.95 | n.s. |
| Fat-free milk (mL/d) | 37.58 ± 121.42 | 6.47 ± 30.35 | 52.55 ± 144.04 | <0.001 |
| Total milk consumption (mL/d) | 120.18 ± 200.22 | 148.34 ± 250.67 | 104.88 ± 189.67 | n.s. |
| Total dairy products (g/d) | 392.26 ± 277.40 | 426.97 ± 279.87 | 373.40 ± 274.81 | n.s. |
| Total energy intake (Kcal) | 2342.78 ± 769.94 | 2459.26 ± 805.18 | 2340.60 ± 747.95 | 0.038 |
| Ca from milk (%) | 23.19 ± 14.92 | 24.82 ± 16.07 | 22.30 ± 14.22 | n.s. |
| Ca (mg/dL) | 1219.77 ± 555.30 | 1241.32 ± 562.64 | 1208.07 ± 542.65 | n.s. |
| Average PA (min/d) | 223.17 ± 65.33 | 221.48 ± 76.91 | 223.69 ± 67.68 | n.s. |
| SES (%) | ||||
| Low | 28.3 | 30.8 | 27.0 | 0.048 |
| Medium | 46.6 | 52.1 | 43.7 | |
| High | 25.1 | 17.1 | 29.3 |
| Less than Daily Intake (187) | Daily Intake (52) | p | |
|---|---|---|---|
| Age (years) | 21.17 ± 3.34 | 20.74 ± 2.12 | n.s. |
| Weight (kg) | 65.92 ± 12.70 | 63.27 ± 10.68 | n.s. |
| Height (cm) | 166.99 ± 8.65 | 168.45 ± 8.38 | n.s. |
| BMI (kg/m2) | 23.55 ± 3.78 | 22.21 ± 2.79 | 0.006 |
| % Total fat mass | 27.56 ± 10.12 | 23.24 ± 9.07 | 0.002 |
| Total lean mass (Kg) | 42.44 ± 9.09 | 44.86 ± 9.68 | n.s. |
| Total body BMD (g/cm2) | 0.050 ± 0.999 | −0.137 ± 0.902 | 0.05 |
| Spine BMD (g/cm2) | 0.039 ± 1.014 | −0.134 ± 0.865 | n.s. |
| Pelvis BMD (g/cm2) | 0.042 ± 0.987 | −0.105 ± 0.940 | n.s. |
| Total milk consumption (mL/d) | 55.77 ± 123.17 | 332.73 ± 203.98 | <0.001 |
| Total dairy products (g/d) | 343.44 ± 238.60 | 541.63 ± 252.53 | <0.001 |
| Total energy intake (Kcal) | 2630.55 ± 1270.72 | 3119.23 ± 1191.15 | 0.004 |
| Average PA (min/d) | 224.27 ± 72.56 | 220.25 ± 56.59 | n.s. |
| SES (%) | |||
| Low | 23.8 | 4.8 | n.s. |
| Medium | 35.8 | 9.9 | |
| High | 20.2 | 5.4 |
| Regular Milk | Fat-Free Milk | Total Milk Consumption | Total Dairy Products | Total Body BMD | Spine BMD | Pelvis BMD | BMI | % Total Fat Mass | Total Lean Mass | Average PA | Total Energy Intake | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Regular milk | - | −0.118 * | 0.860 ** | 0.551 ** | −0.133 * | −0.106 | −0.101 | −0.111 * | −1.171 ** | 0.078 | 0.069 | 0.138 * |
| Fat-free milk | 0.406 ** | 0.274 ** | 0.112 | 0.145 * | 0.056 | 0.141 ** | 0.159 ** | −0.104 | −0.065 | −0.059 | ||
| Total milk consumption | - | 0.648 ** | −0.058 | −0.017 | 0.391 | −0.030 | −0.070 | 0.014 | −0.098 | 0.325 ** | ||
| Total dairy products | - | −0.065 | −0.043 | −0.079 | −0.047 | −0.133 * | 0.012 | 0.081 | 0.472 * | |||
| Total body BMD | 0.783 * | 0.730 * | 0.498 ** | 0.142 ** | 0.323 ** | 0.013 | −0.079 | |||||
| Spine BMD | - | 0.670 * | 0.477 * | 0.175 * | 0.255 ** | −0.067 | −0.075 | |||||
| Pelvis BMD | - | 0.356 * | 0.082 | 0.271 * | −0.030 | −1.132 * | ||||||
| BMI | 0.493 * | 0.323 * | 0.057 | −0.127 * | ||||||||
| %Total fat mass | - | −0.496 ** | −0.022 | −0.166 * | ||||||||
| Total lean mass | - | 0.062 | −0.061 | |||||||||
| Average PA | - | 0.024 |
| Total Body BMD | |||||
|---|---|---|---|---|---|
| Regular Milk Consumption | n | Model 0 | Model 1 | Model 2 | Model 3 |
| Less than daily intake | 185 | 0.07 (0.07) | 0.15 (0.95) | 0.17 (0.95) | 0.11 (0.08) |
| Daily intake | 51 | −0.24 (0.13) | −0.43 (0.20) | −0.50 (0.21) | −0.24 (0.18) |
| p | 0.042 | 0.011 | 0.005 | 0.081 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres-Costoso, A.; López-Muñoz, P.; Ferri-Morales, A.; Bravo-Morales, E.; Martínez-Vizcaíno, V.; Garrido-Miguel, M. Body Mass Index, Lean Mass, and Body Fat Percentage as Mediators of the Relationship between Milk Consumption and Bone Health in Young Adults. Nutrients 2019, 11, 2500. https://doi.org/10.3390/nu11102500
Torres-Costoso A, López-Muñoz P, Ferri-Morales A, Bravo-Morales E, Martínez-Vizcaíno V, Garrido-Miguel M. Body Mass Index, Lean Mass, and Body Fat Percentage as Mediators of the Relationship between Milk Consumption and Bone Health in Young Adults. Nutrients. 2019; 11(10):2500. https://doi.org/10.3390/nu11102500
Chicago/Turabian StyleTorres-Costoso, Ana, Purificación López-Muñoz, Asunción Ferri-Morales, Elisabeth Bravo-Morales, Vicente Martínez-Vizcaíno, and Miriam Garrido-Miguel. 2019. "Body Mass Index, Lean Mass, and Body Fat Percentage as Mediators of the Relationship between Milk Consumption and Bone Health in Young Adults" Nutrients 11, no. 10: 2500. https://doi.org/10.3390/nu11102500