Factors Predicting the Response to a Vitamin D-Fortified Milk in Healthy Postmenopausal Women

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Anthropometric Measurements
2.3. Body Composition Measurements
2.4. Biochemical Parameters
2.5. Statistical Analyses
3. Results
3.1. Changes in Biochemical Parameters
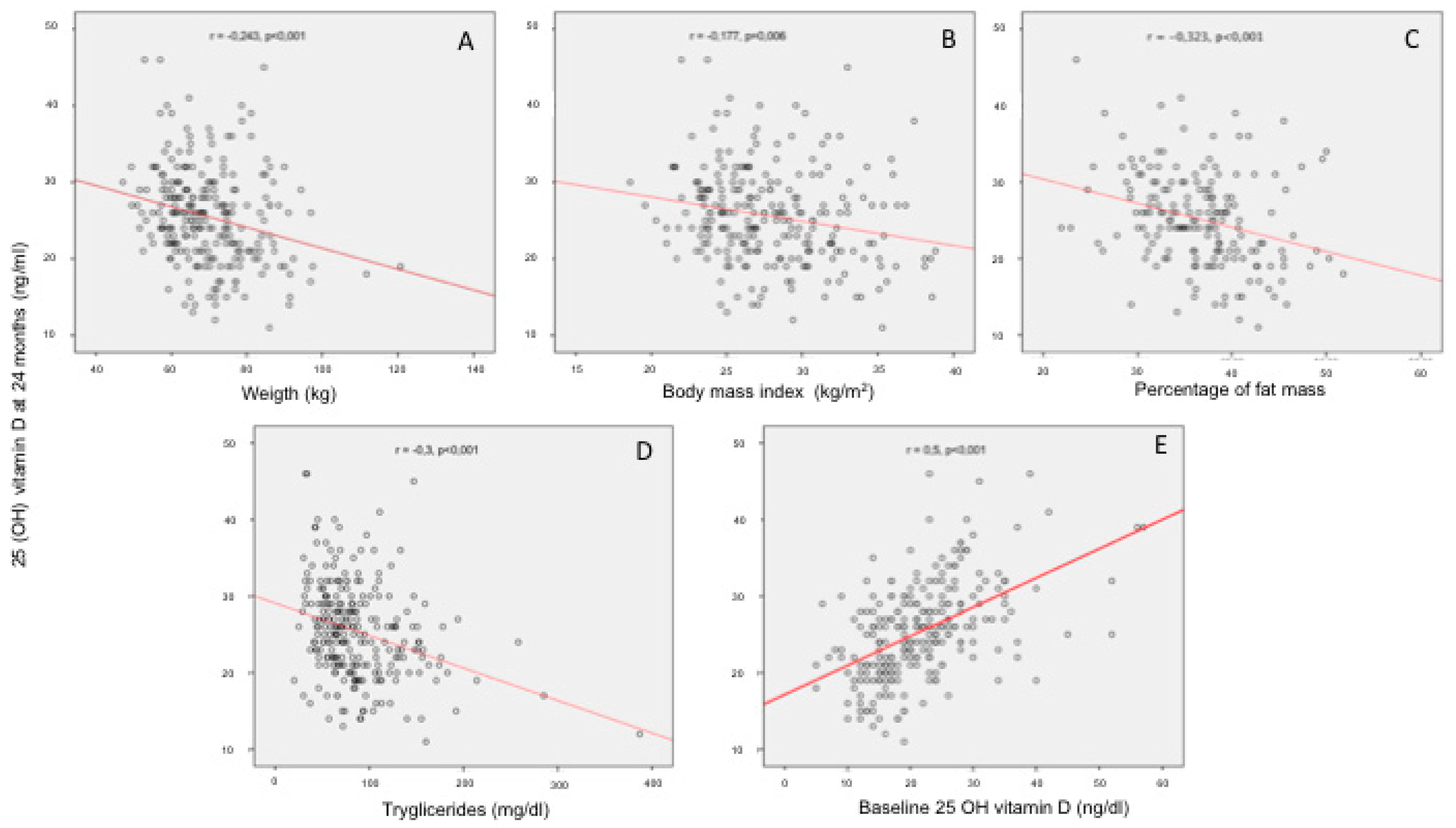
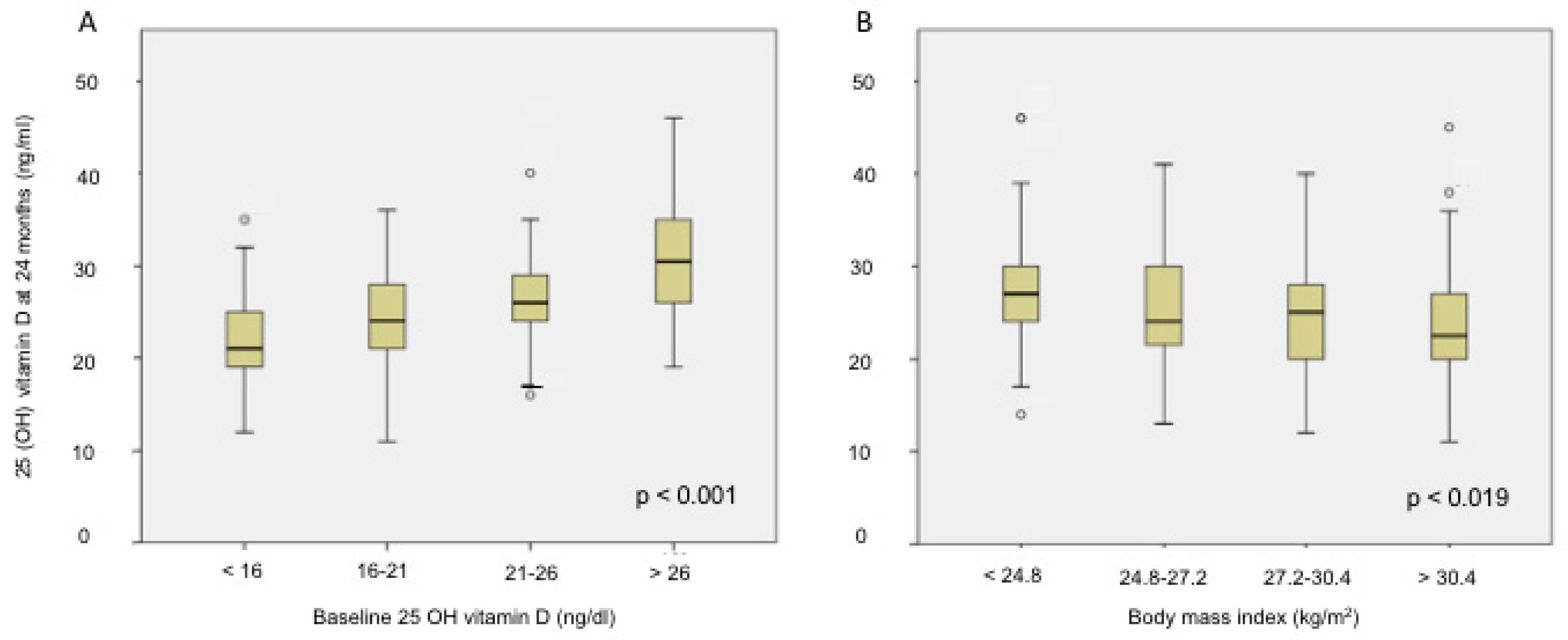
3.2. Factors Related to 25(OH)D Levels after the Intervention
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Heaney, R.P. Health is better at serum 25(OH)D above 30ng/mL. J. Steroid Biochem. Mol. Biol. 2013, 136, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J. Clin. Endocrinol. Metab. 2012, 97, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; Kovacs, C.S.; et al. IOM committee members respond to Endocrine Society vitamin D guideline. J. Clin. Endocrinol. Metab. 2012, 97, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global prevalence and disease burden of vitamin D deficiency: A roadmap for action in low- and middle-income countries. Ann N. Y. Acad. Sci. 2018, 430, 44–79. [Google Scholar] [CrossRef]
- Giustina, A.; Adler, R.A.; Binkley, N.; Bouillon, R.; Ebeling, P.R.; Lazaretti-Castro, M.; Marcocci, C.; Rizzoli, R.; Sempos, C.T.; Bilezikian, J.P. Controversies in Vitamin D: Summary Statement From an International Conference. J. Clin. Endocrinol. Metab. 2019, 104, 234–240. [Google Scholar] [CrossRef]
- Drincic, A.T.; Armas, L.A.G.; Van Diest, E.E.; Heaney, R.P. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obes. Silver Spring Md 2012, 20, 1444–1448. [Google Scholar] [CrossRef]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef]
- Didriksen, A.; Grimnes, G.; Hutchinson, M.S.; Kjærgaard, M.; Svartberg, J.; Joakimsen, R.M.; Jorde, R. The serum 25-hydroxyvitamin D response to vitamin D supplementation is related to genetic factors, BMI, and baseline levels. Eur. J. Endocrinol. 2013, 169, 559–567. [Google Scholar] [CrossRef] [Green Version]
- Pereira-Santos, M.; Costa, P.R.F.; Assis, A.M.O.; Santos, C.A.S.T.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2015, 16, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Garcia, R.; Mendoza, N.; Palacios, S.; Salas, N.; Quesada-Charneco, M.; Garcia-Martin, A.; Fonolla, J.; Lara-Villoslada, F.; Muñoz-Torres, M. Effects of Daily Intake of Calcium and Vitamin D-Enriched Milk in Healthy Postmenopausal Women: A Randomized, Controlled, Double-Blind Nutritional Study. J. Womens Health 2002 2018, 27, 561–568. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Deurenberg, P.; Pietrantuono, M.; Di Daniele, N.; Cervelli, V.; Andreoli, A. How fat is obese? Acta Diabetol. 2003, 40 (Suppl. 1), S254–S257. [Google Scholar] [CrossRef] [PubMed]
- Sanfelix-Genovés, J.; Gil-Guillén, V.F.; Orozco-Beltran, D.; Giner-Ruiz, V.; Pertusa-Martínez, S.; Reig-Moya, B.; Carratalá, C. Determinant factors of osteoporosis patients’ reported therapeutic adherence to calcium and/or vitamin D supplements: A cross-sectional, observational study of postmenopausal women. Drugs Aging 2009, 26, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Blum, M.; Dallal, G.E.; Dawson-Hughes, B. Body size and serum 25 hydroxy vitamin D response to oral supplements in healthy older adults. J. Am. Coll. Nutr. 2008, 27, 274–279. [Google Scholar] [CrossRef]
- Waterhouse, M.; Tran, B.; Armstrong, B.K.; Baxter, C.; Ebeling, P.R.; English, D.R.; Gebski, V.; Hill, C.; Kimlin, M.G.; Lucas, R.M.; et al. Environmental, personal, and genetic determinants of response to vitamin D supplementation in older adults. J. Clin. Endocrinol. Metab. 2014, 99, E1332–E1340. [Google Scholar] [CrossRef]
- Lehmann, U.; Riedel, A.; Hirche, F.; Brandsch, C.; Girndt, M.; Ulrich, C.; Seibert, E.; Henning, C.; Glomb, M.A.; Dierkes, J.; et al. Vitamin D3 supplementation: Response and predictors of vitamin D3 metabolites—A randomized controlled trial. Clin. Nutr. Edinb. Scotl. 2016, 35, 351–358. [Google Scholar] [CrossRef]
- Adab, P.; Pallan, M.; Whincup, P.H. Is BMI the best measure of obesity? BMJ 2018, 360, k1274. [Google Scholar] [CrossRef] [Green Version]
- Trevisan, C.; Veronese, N.; Berton, L.; Carraro, S.; Bolzetta, F.; De Rui, M.; Miotto, F.; Inelmen, E.M.; Coin, A.; Perissinotto, E.; et al. Factors Influencing Serum-Hydroxivitamin D Levels and Other Bone Metabolism Parameters in Healthy Older Women. J. Nutr. Health Aging 2017, 21, 131–135. [Google Scholar] [CrossRef]
- Jorde, R.; Sneve, M.; Emaus, N.; Figenschau, Y.; Grimnes, G. Cross-sectional and longitudinal relation between serum 25-hydroxyvitamin D and body mass index: The Tromsø study. Eur. J. Nutr. 2010, 49, 401–407. [Google Scholar] [CrossRef]
- Carrelli, A.; Bucovsky, M.; Horst, R.; Cremers, S.; Zhang, C.; Bessler, M.; Schrope, B.; Evanko, J.; Blanco, J.; Silverberg, S.J.; et al. Vitamin D Storage in Adipose Tissue of Obese and Normal Weight Women. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2017, 32, 237–242. [Google Scholar] [CrossRef]
- Golzarand, M.; Hollis, B.W.; Mirmiran, P.; Wagner, C.L.; Shab-Bidar, S. Vitamin D supplementation and body fat mass: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2018, 72, 1345–1357. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Ma, F.; Lou, H.; Liu, Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health 2013, 13, 629. [Google Scholar] [CrossRef] [PubMed]
- Bolanowski, M.; Nilsson, B.E. Assessment of human body composition using dual-energy x-ray absorptiometry and bioelectrical impedance analysis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2001, 7, 1029–1033. [Google Scholar]
- Gallagher, J.C.; Sai, A.; Templin, T.; Smith, L. Dose response to vitamin D supplementation in postmenopausal women: A randomized trial. Ann. Intern. Med. 2012, 156, 425–437. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline | 24 months | p | |
|---|---|---|---|
| Weight (kg) | 70 ± 11 | 70 ± 11 | 0.5 |
| Body mass index (kg/m2) | 28 ± 4 | 28 ± 4 | 0.084 |
| Obesity (%) | 28 | 32 | |
| Overweight (%) | 47 | 48 | |
| Percentage of fat mass | 37 ± 5 | 37 ± 5 | 0.047 |
| Serum calcium (mg/dL) | 9.7 ± 0.6 | 9.8 ± 0.6 | <0.001 |
| Parathyroid hormone (pg/mL) | 57 ± 21 | 58 ± 20 | 0.102 |
| 25(OH)D (ng/mL) | 22 ± 8 | 25± 6 | <0.001 |
| Total cholesterol (mg/dL) | 214 ± 33 | 208 ± 32 | <0.001 |
| HDL colesterol (mg/dL) | 55 ± 15 | 55 ± 14 | 0.62 |
| LDL colesterol (mg/dL) | 141 ± 32 | 135 ± 32 | <0.001 |
| Triglycerides (mg/dL) | 87 ± 44 | 88 ± 46 | 0.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reyes-Garcia, R.; Garcia-Martin, A.; Palacios, S.; Salas, N.; Mendoza, N.; Quesada-Charneco, M.; Fonolla, J.; Lara-Villoslada, F.; Muñoz-Torres, M. Factors Predicting the Response to a Vitamin D-Fortified Milk in Healthy Postmenopausal Women. Nutrients 2019, 11, 2641. https://doi.org/10.3390/nu11112641
Reyes-Garcia R, Garcia-Martin A, Palacios S, Salas N, Mendoza N, Quesada-Charneco M, Fonolla J, Lara-Villoslada F, Muñoz-Torres M. Factors Predicting the Response to a Vitamin D-Fortified Milk in Healthy Postmenopausal Women. Nutrients. 2019; 11(11):2641. https://doi.org/10.3390/nu11112641
Chicago/Turabian StyleReyes-Garcia, Rebeca, Antonia Garcia-Martin, Santiago Palacios, Nancy Salas, Nicolas Mendoza, Miguel Quesada-Charneco, Juristo Fonolla, Federico Lara-Villoslada, and Manuel Muñoz-Torres. 2019. "Factors Predicting the Response to a Vitamin D-Fortified Milk in Healthy Postmenopausal Women" Nutrients 11, no. 11: 2641. https://doi.org/10.3390/nu11112641