Vitamin D Food Fortification and Nutritional Status in Children: A Systematic Review of Randomized Controlled Trials

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
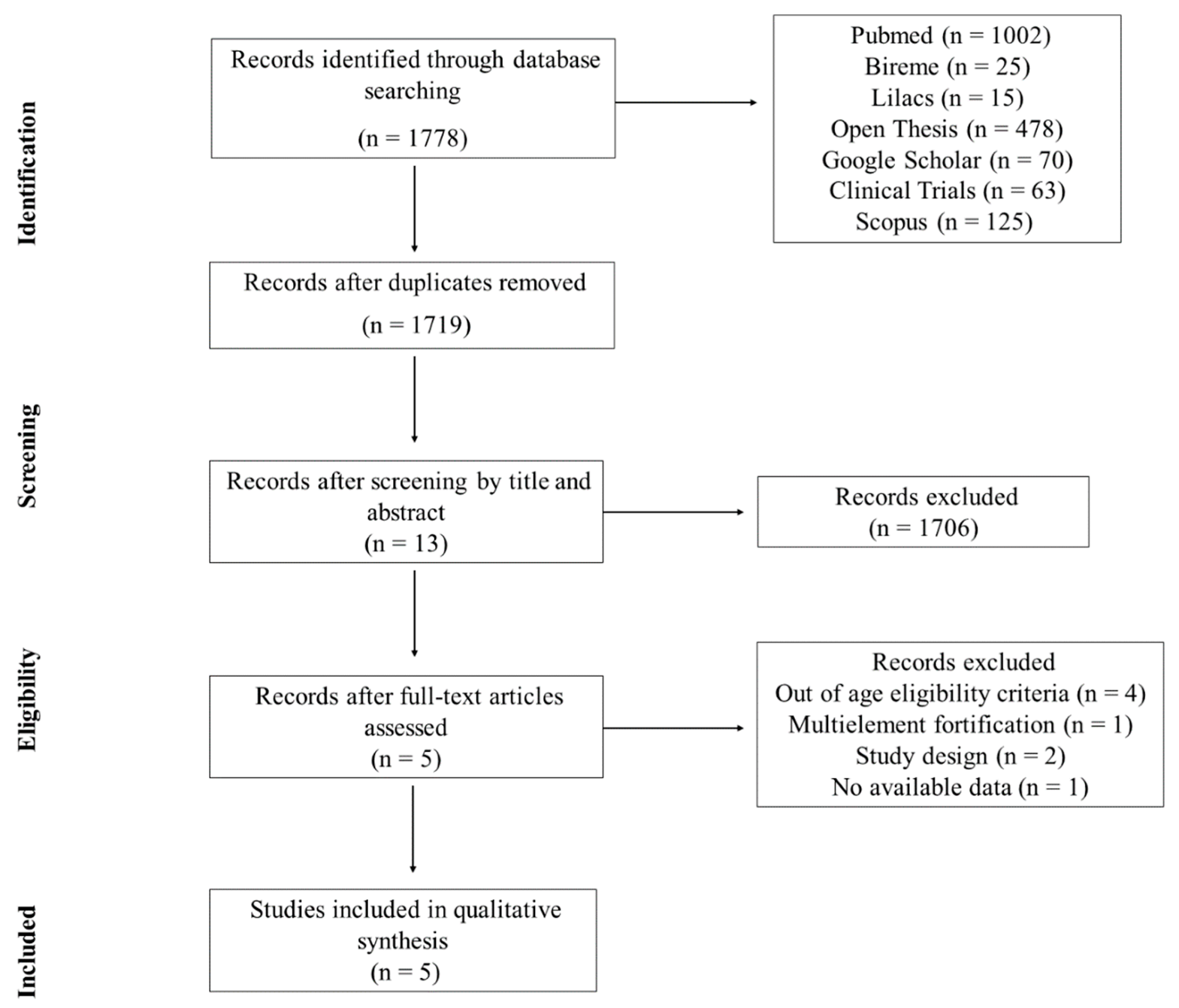
2.3. Study Selection and Data Extraction
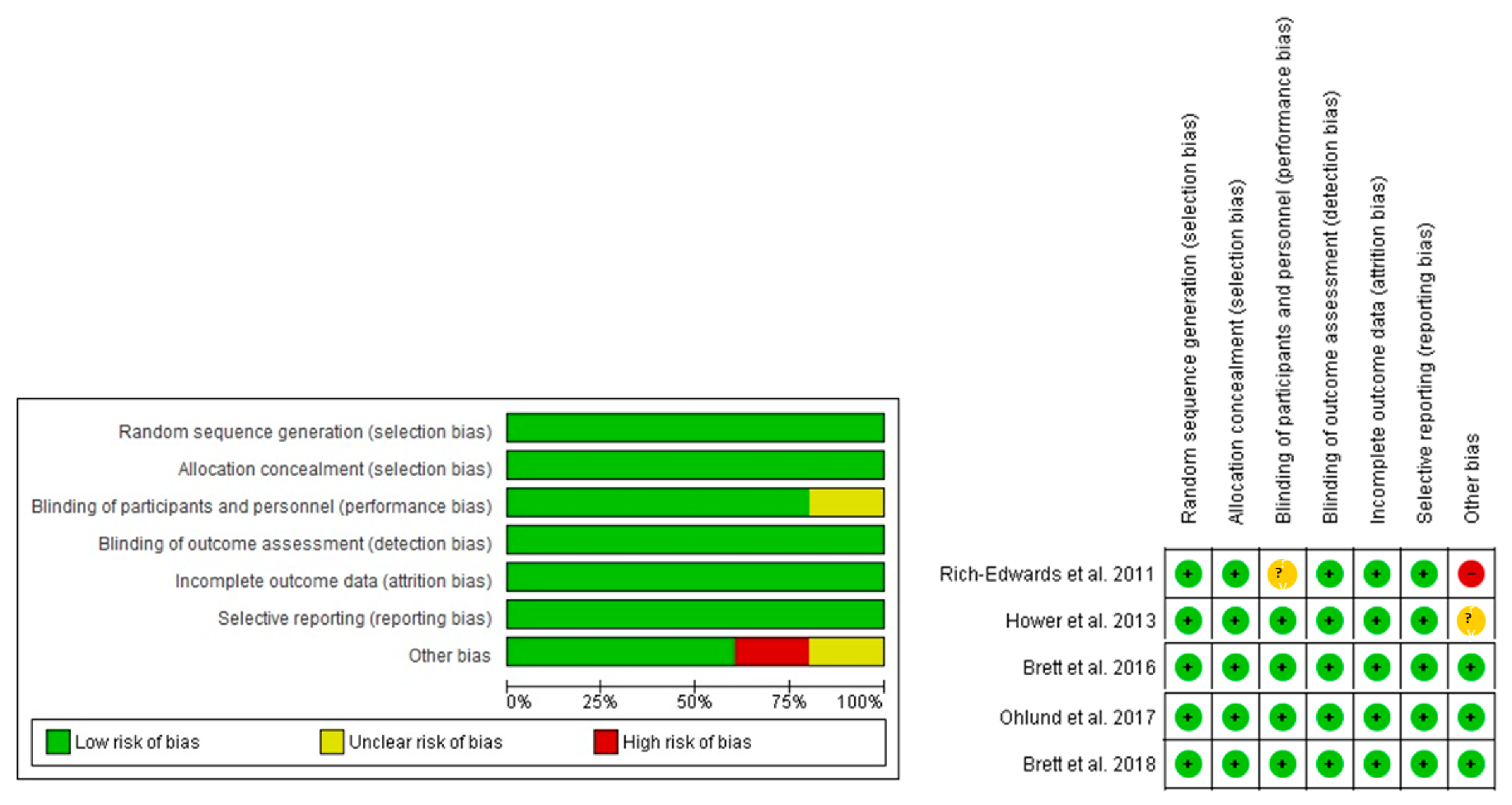
2.4. Assessment of Risk of Bias
2.5. Data Synthesis
3. Results
3.1. General Characteristics
3.2. Risk of Bias
3.3. Sample Characterization
3.4. Food Fortification and Intervention Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mortensen, C.; Mølgaard, C.; Hauger, H.; Kristensen, M.; Damsgaard, C.T. Sun behaviour and physical activity associated with autumn vitamin D status in 4–8-year-old Danish children. Public Health Nutr. 2018, 21, 3158–3167. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Shen, G.; Jiang, S.; Xu, H.; Li, M.; Wang, Z.; Zhang, S.; Yu, Y. Nutrient status of vitamin D among chinese children. Nutrients 2017, 9, 319. [Google Scholar] [CrossRef] [PubMed]
- Kamen, D.L.; Tangpricha, V. Vitamin D and molecular actions on the immune system: Modulation of innate and autoimmunity. J. Mol. Med. 2010, 88, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del, H.B., Eds.; National Academy of Sciences: Washington, DC, USA, 2011; ISBN 978-0-309-16394-1. [Google Scholar]
- Forrest, K.Y.Z.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj Fuleihan, G.; Josse, R.G.; Lips, P.; Morales-Torres, J. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.; Holick, M.F. Sunlight and Vitamin D: A global perspective for health. Derm. Endocrinol. 2013, 5, 51–108. [Google Scholar] [CrossRef]
- Hossein-nezhad, A.; Holick, M.F.; Holick, M.F.; Heaney, R.; Singh, R.J.; Pettifor, J.M. Vitamin D for Health: A Global Perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Eloi, M.; Horvath, D.V.; Szejnfeld, V.L.; Ortega, J.C.; Rocha, D.A.C.; Szejnfeld, J.; Castro, C.H.M. Vitamin D deficiency and seasonal variation over the years in São Paulo, Brazil. Osteoporos. Int. 2016, 27, 3449–3456. [Google Scholar] [CrossRef]
- Binkley, N.; Novotny, R.; Krueger, D.; Kawahara, T.; Daida, Y.G.; Lensmeyer, G.; Hollis, B.W.; Drezner, M.K. Low Vitamin D Status despite Abundant Sun Exposure. J. Clin. Endocrinol. Metab. 2007, 92, 2130–2135. [Google Scholar] [CrossRef]
- Lopes, V.M.; Lopes, J.R.; Brasileiro, J.P.; Oliveira, I.D.; Lacerda, R.P.; Andrade, M.R.; Tierno, N.I.; Souza, R.C.; Motta, L.A. Highly prevalence of vitamin D deficiency among Brazilian women of reproductive age. Arch. Endocrinol. Metab. 2017, 61, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Harinarayan, C.V.; Holick, M.F.; Prasad, U.V.; Vani, P.S.; Himabindu, G. Vitamin D status and sun exposure in India. Derm. Endocrinol. 2013, 5, 130–141. [Google Scholar] [CrossRef]
- Hower, J.; Knoll, A.; Ritzenthaler, K.L.; Steiner, C.; Berwind, R. Vitamin D fortification of growing up milk prevents decrease of serum 25-hydroxyvitamin D concentrations during winter: A clinical intervention study in Germany. Eur. J. Pediatr. 2013, 172, 1597–1605. [Google Scholar] [CrossRef] [PubMed]
- Black, L.J.; Seamans, K.M.; Cashman, K.D.; Kiely, M. An Updated Systematic Review and Meta-Analysis of the Efficacy of Vitamin D Food Fortification. J. Nutr. 2012, 142, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Brett, N.R.; Lavery, P.; Agellon, S.; Vanstone, C.A.; Maguire, J.L.; Rauch, F.; Weiler, H.A. Dietary vitamin D dose-response in healthy children 2 to 8 y of age: A 12-wk randomized controlled trial using fortified foods. Am. J. Clin. Nutr. 2016, 103, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Brett, N.R.; Parks, C.A.; Lavery, P.; Agellon, S.; Vanstone, C.A.; Kaufmann, M.; Jones, G.; Maguire, J.L.; Rauch, F.; Weiler, H.A. Vitamin D status and functional health outcomes in children aged 2–8 y: A 6-mo Vitamin D randomized controlled trial. Am. J. Clin. Nutr. 2018, 107, 355–364. [Google Scholar] [CrossRef]
- Rich-Edwards, J.W.; Ganmaa, D.; Kleinman, K.; Sumberzul, N.; Holick, M.F.; Lkhagvasuren, T.; Dulguun, B.; Burke, A.; Frazier, A.L. Randomized trial of fortified milk and supplements to raise 25-hydroxyvitamin D concentrations in schoolchildren in Mongolia. Am. J. Clin. Nutr. 2011, 94, 578–584. [Google Scholar] [CrossRef]
- Öhlund, I.; Lind, T.; Hernell, O.; Silfverdal, S.A.; Äkeson, P.K. Increased Vitamin D intake differentiated according to skin color is needed to meet requirements in young Swedish children during winter: A double-blind randomized clinical trial. Am. J. Clin. Nutr. 2017, 106, 105–112. [Google Scholar] [CrossRef]
- Brett, N.R.; Gharibeh, N.; Weiler, H.A. Effect of Vitamin D Supplementation, Food Fortification, or Bolus Injection on Vitamin D Status in Children Aged 2–18 Years: A Meta-Analysis. Adv. Nutr. 2018, 9, 454–464. [Google Scholar] [CrossRef]
- Matsuyama, M.; Harb, T.; David, M.; Davies, P.S.; Hill, R.J. Effect of fortified milk on growth and nutritional status in young children: A systematic review and meta-analysis. Public Health Nutr. 2016, 20, 1214–1225. [Google Scholar] [CrossRef]
- Ritu, G.; Ajay, G. Fortification of Foods With Vitamin D in India: Strategies Targeted at Children. J. Am. Coll. Nutr. 2015, 34, 265–272. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Chin. Integr. Med. 2009, 7, 889–896. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2016; pp. 297–303. Available online: https://training.cochrane.org/handbook/archive/v5.1/ (accessed on 29 January 2018).
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Child Growth Standards; World Health Organization: Geneva, Switzerland, 2006; pp. 7–16. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Donnell, S.O.; Cranney, A.; Horsley, T.; Weiler, H.A.; Atkinson, S.A.; Hanley, D.A.; Ooi, D.S.; Ward, L.; Barrowman, N.; Fang, M.; et al. Efficacy of food fortification on serum 25-hydroxyvitamin D concentrations: Systematic review. Am. J. Clin. Nutr. 2008, 88, 1528–1534. [Google Scholar] [CrossRef]
- Jakobsen, J.; Knuthsen, P. Stability of vitamin D in foodstuffs during cooking. Food Chem. 2014, 148, 170–175. [Google Scholar] [CrossRef]
- Agency, C.F.I. Dairy Vitamin Addition. Available online: http://www.inspection.gc.ca/food/archived-food-guidance/dairy-products/manuals-inspection-procedures/dairy-vitamin-addition/eng/1378179097522/1378180040706 (accessed on 28 March 2019).
- FAO/WHO. Human Vitamin and Mineral Requirements; FAO/WHO: Bangkok, Thailand, 2001. [Google Scholar]
- Cashman, K.D.; van den Heuvel, E.G.; Schoemaker, R.J.; Prévéraud, D.P.; Macdonald, H.M.; Arcot, J. 25-Hydroxyvitamin D as a Biomarker of Vitamin D Status and Its Modeling to Inform Strategies for Prevention of Vitamin D Deficiency within the Population. Adv. Nutr. 2017, 8, 947–957. [Google Scholar] [CrossRef]
- Hayes, A.; Cashman, K.D. Irish Section Postgraduate Meeting Food-based solutions for Vitamin D deficiency: Putting policy into practice and the key role for research. Proc. Nutr. Soc. 2017, 76, 54–63. [Google Scholar] [CrossRef]
- Corte-Real, J.; Bohn, T. Interaction of divalent minerals with liposoluble nutrients and phytochemicals during digestion and influences on their bioavailability—A review. Food Chem. 2018, 252, 285–293. [Google Scholar] [CrossRef]
- Saggese, G.; Vierucci, F.; Boot, A.M.; Czech-kowalska, J.; Weber, G., Jr.; Camargo, A.C.; Mallet, E.; Fanos, M.; Shaw, N.J.; Holick, M.F.; et al. Vitamin D in childhood and adolescence: An expert position statement. Am. Acad. Pediatr. 2015, 174, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Livsmedelsverket (Swedish National Food Administration). Föreskrifter om Berikning av Vissa Livsmedel; Livsmedelsverket: Uppsala, Sweden, 2018; pp. 1–4.
- Ministry of Health of Mongolia. Nutrition Status of the Population of Mongolia; Ministry of Health of Mongolia: Ulaanbaatar, Mongolia, 2017; ISBN 9789997859266.
- Aloia, J.F.; Patel, M.; DiMaano, R.; Li-Ng, M.; Talwar, S.A.; Mikhail, M.; Pollack, S.; Yeh, J.K. Vitamin D intake to attain a desired serum 25-hydroxyvitamin D concentration. Am. J. Clin. Nutr. 2008, 87, 1952–1958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, J.G.; Rojanasathit, S. Acute Administration of 25-Hydroxycholecalciferol in Man. J. Clin. Endocrinol. Metab. 1976, 42, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.W.; Paris, P.W.; Clemens, T.L.; Nolan, J.; Holick, M.F. Vitamin patients D absorption in healthy subjects with intestinal malabsorption and in. Am. J. Clin. Nutr. 1985, 42, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W.; Wagner, C.L. The Role of the Parent Compound Vitamin D with Respect to Metabolism and Function: Why Clinical Dose Intervals Can Affect Clinical Outcomes. J. Clin. Endocrinol. Metab. 2013, 98, 4619–4628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieth, R.; Chan, P.R.; Macfarlane, G.D. Efficacy and safety of vitamin D3 intake exceeding the lowest observed adverse effect level. Am. J. Clin. Nutr. 2001, 73, 288–294. [Google Scholar] [CrossRef]
- Heaney, R.P.; Recker, R.R.; Grote, J.; Horst, R.L.; Armas, L.A.G. Vitamin D3 Is More Potent Than Vitamin D 2 in Humans. J. Clin. Endocrinol. Metab. 2011, 96, 447–452. [Google Scholar] [CrossRef] [Green Version]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Chung, M.; Balk, E.M.; Brendel, M.; Ip, S.; Lau, J.; Lee, J.; Lichtenstein, A.; Patel, K.; Raman, G.; Tatsioni, A.; et al. Vitamin D and Calcium: A Systematic Review of Health Outcomes. Evid. Rep. Technol. Assess. 2009, 183, 1–420. [Google Scholar]
- Alonso, M.A.; Mantecón, L.; Santos, F. Vitamin D deficiency in children: A challenging diagnosis! Pediatr. Res. 2019, 85, 596–601. [Google Scholar] [CrossRef]
- Holick, M.F.; Herman, R.H.; Award, M. Vitamin D: Importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am. J. Clin. Nutr. 2004, 79, 362–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on nutrient requirements and dietary intakes of infants and young children in the European Union. EFSA J. 2013, 11, 3408. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz-Ojeda, F.J.; Anguita-Ruiz, A.; Leis, R.; Aguilera, C.M. Genetic factors and molecular mechanisms of Vitamin D and obesity relationship. Ann. Nutr. Metab. 2018, 73, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, C.; Ness, A.R.; Wills, A.K.; Lawlor, D.A.; Lewis, S.J.; Davey Smith, G. Skin pigmentation, sun exposure and vitamin D levels in children of the avon longitudinal study of parents and children. BMC Public Health 2014, 14, 597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebanks, J.P.; Koshoffer, A.; Wickett, R.R.; Schwemberger, S.; Babcock, G.; Hakozaki, T.; Boissy, R.E. Epidermal keratinocytes from light vs. Dark skin exhibit differential degradation of melanosomes. J. Investig. Dermatol. 2011, 131, 1226–1233. [Google Scholar] [CrossRef] [Green Version]
- Card, D.J.; Carter, G. Methods for Assessment of Vitamin D; Elsevier Inc.: Amsterdam, The Netherlands, 2018; ISBN 9780128130506. [Google Scholar]



{kind=link}
{kind=link}
| Author | Country | Duration of Study/Season | Group | No. of Children | Age (Years) | Vitamin D Status (n) | BMI for Age Classification ǂ | Skin Phototype (n) § | |
|---|---|---|---|---|---|---|---|---|---|
| Deficiency and Insufficiency | Sufficiency | ||||||||
| Rich-Edwards et al. [18] | Mongolia | January to March/Winter | Mongolian Milk | 140 | 10.0 ± 1.0 | NA | 1 | Normal weight | NA |
| UHT USA Milk | 137 | 5 | |||||||
| Control | 101 | 1 | |||||||
| Hower et al. [14] | Germany | November to July/Fall to Summer | Intervention | 46 | 3.8 (2.0–6.8) | 21 | 25 | Thickness, normal weight, overweight and obesity | Light skin: 78 ¥ |
| Control | 34 | 3.7 (2.0–6.2) | 19 | 15 | Dark skin: 2 ¥ | ||||
| Brett et al. [16] | Canada | January to April/Winter to mid-spring | EAR | 27 | 4.9 ± 2.1 | 7 | 20 | Normal weight | Phototype I to III: 43 Phototype IV to VI: 34 |
| RDA | 26 | 5.3 ± 2.0 | 4 | 22 | |||||
| Control | 24 | 5.0 ± 1.8 | 7 | 17 | |||||
| Ohlund et al. [19] | Sweden | November to March/Fall to Winter | 10 µg | 80 | 6.3 (6.2;6.7) | NA | 47 | Normal weight, overweight and obesity | Phototype I to IV: 108 Phototype V to VI: 98 |
| 25 µg | 86 | 6.3 (6.2;6.4) | 54 | ||||||
| Control | 40 | 6.3 (6.1;6.5) | 20 | ||||||
| Brett et al. [17] | Canada | October to March/Fall to Winter | Intervention | 26 | 5.0 ± 1.8 | 2 | 24 | Normal weight | Phototype I to III: 34 Phototype IV to VI: 17 |
| Control | 25 | 5.4 ± 2.0 | 2 | 23 | |||||
| Author | Duration of Study (Months) | Group | Food/Portion Size | Vitamin D Content in Food | Total Vitamin D (IU/Day) |
|---|---|---|---|---|---|
| Rich-Edwards et al. [18] | 1.6 | Mongolian milk | Mongolian milk/710 mL | 100 IU/236 mL | 300 |
| UHT USA milk | UHT USA milk/710 mL | 100 IU/236 mL | 300 | ||
| Control | Non-fortified milk/710 mL | NA | NA | ||
| Hower et al. [14] | 9 | Intervention | Fortified milk /350 mL | 114 IU/100 mL | 400 |
| Control | Non-fortified milk /350 mL | 1.2 IU/100 mL | 4.2 | ||
| Brett et al. [16] | 3 | EAR | Yogurt/186 mL | 42 IU/ 93 mL | 400 ¥ |
| Cheddar cheese /21 g | 200 IU/21 g | ||||
| RDA | Yogurt/186 mL | 125 IU/93 mL | 600 ¥ | ||
| Cheddar cheese/21 g | 200 IU/21 g | ||||
| Control | Non-fortified yogurt/186 mL | 15 IU/93 mL | 140–195 ¥ | ||
| Non-fortified cheddar cheese/21 g | NA | ||||
| Ohlund et al. [19] | 3 | 10 µg | UHT milk/200 mL | 480 IU/200 g | 480 |
| 25 µg | UHT milk/ 200 mL | 880 IU/200 g | 880 | ||
| Control | Non-fortified UHT milk/200 mL | 80 IU/200 mL | 80 | ||
| Brett et al. [17] | 6 | Intervention | Yogurt/186 mL Cheddar cheese/33g | Yogurt: 150 IU/93 mL Cheddar cheese: 300 IU/33 g | 400 ¥ |
| Control | Non-fortified yogurt/186 mL Non-fortified cheddar cheese/33 g | NA | 140–195 ¥ |
| Author | Methods of Vitamin D Assessment | Group | 25(OH)D (nmol/L) | Δ Change (nmol/L) | |||
|---|---|---|---|---|---|---|---|
| Baseline | End Point | ||||||
| Rich-Edwards et al. [18] | LC-MS/MS | Mongolian milk | 20.0 ± 10.0 a | 50.0 ± 15.0 b,# | 30.0 ± 13.2 | ||
| UHT USA milk | 25.0 ± 12.5 a | 72.4 ± 25.0 b,# | 47.4 ± 21.7 | ||||
| Control | 20.0 ± 10.0 a | 20.0 ± 10.0 a | 0 ± 10.0 | ||||
| Hower et al. [14] | CLIA | Intervention | 53.7 ± 20.6 a | After winter 62.0 ± 25.8 b,# | Summer 69.0 ± 13.6 b | After winter 8.3 ± 23.6 | Summer 15.3 ± 18.1 |
| Control | 46.0 ± 21.2 a | After winter 34.0 ± 18.6 b | Summer 68.5 ± 13.0 c | After winter −12.0 ± 20.0 | Summer 22.5 ± 18.5 | ||
| Brett et al. [16] | CLIA | EAR | 59.7 ± 13.0 a | 64.2 ± 9.7 b,# | 4.5 ± 11.7 | ||
| RDA | 60.9 ± 10.1 a | 64.1 ± 11.8 b,# | 3.2 ± 11.0 | ||||
| Control | 58.6 ± 14.5 a | 56.1 ± 11.9 a | −2.5 ± 13.4 | ||||
| Ohlund et al. [19] | LC-MS/MS | 10 µg | 56.0 ± 18.3 a | 69.0 ± 9.1 b,# | 13.0 ± 15.8 | ||
| 25 µg | 58.0 ± 21.3 a | 82.0 ± 14.2 b,# | 24.0 ± 18.8 | ||||
| Control | 49.0 ± 19.4 a | 50.0 ± 14.5 a | 1.0 ± 17.5 | ||||
| Brett et al. [17] | HPLC | Intervention | 65.3 ± 12.2 a | 3 months 64.7 ± 12.2 a,# | 6 months 58.4 ± 8.7 b | 3 months −0.6 ± 12.2 | 6 months −6.9 ± 10.9 |
| Control | 67.5 ± 15.1 a | 3 months 58.3 ± 15.3 b | 6 months 56.6 ± 13.9 b | 3 months −9.2 ± 15.2 | 6 months −10.9 ± 14.5 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brandão-Lima, P.N.; Santos, B.d.C.; Aguilera, C.M.; Freire, A.R.S.; Martins-Filho, P.R.S.; Pires, L.V. Vitamin D Food Fortification and Nutritional Status in Children: A Systematic Review of Randomized Controlled Trials. Nutrients 2019, 11, 2766. https://doi.org/10.3390/nu11112766
Brandão-Lima PN, Santos BdC, Aguilera CM, Freire ARS, Martins-Filho PRS, Pires LV. Vitamin D Food Fortification and Nutritional Status in Children: A Systematic Review of Randomized Controlled Trials. Nutrients. 2019; 11(11):2766. https://doi.org/10.3390/nu11112766
Chicago/Turabian StyleBrandão-Lima, Paula Nascimento, Beatriz da Cruz Santos, Concepción Maria Aguilera, Analícia Rocha Santos Freire, Paulo Ricardo Saquete Martins-Filho, and Liliane Viana Pires. 2019. "Vitamin D Food Fortification and Nutritional Status in Children: A Systematic Review of Randomized Controlled Trials" Nutrients 11, no. 11: 2766. https://doi.org/10.3390/nu11112766