The Impact of Maternal Obesity on Human Milk Macronutrient Composition: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Search Strategy
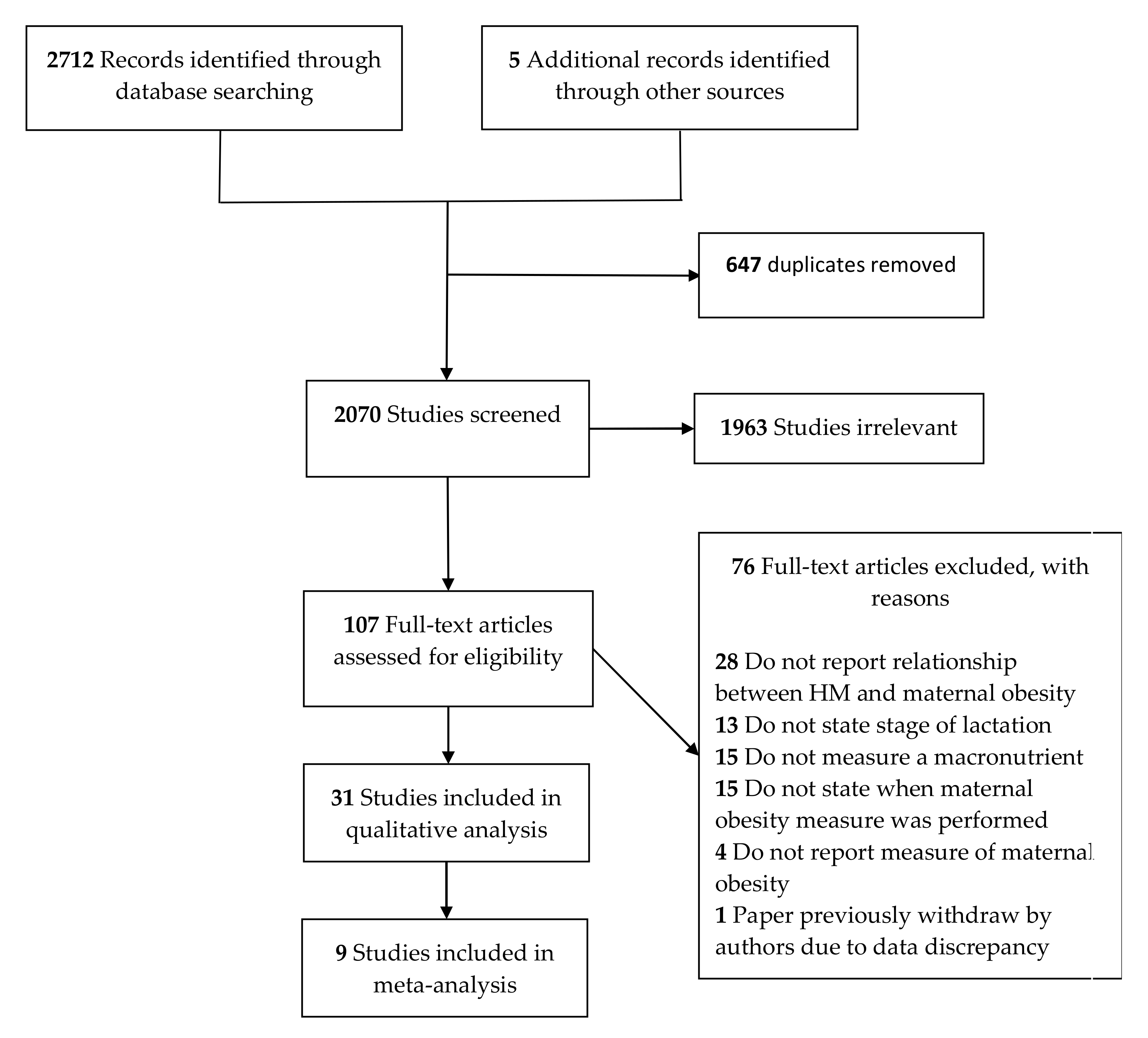
2.4. Selection Process
2.5. Data Extraction
2.6. Quality Assessment of Individual Studies
2.7. Data Synthesis
3. Results
3.1. Summary of Studies
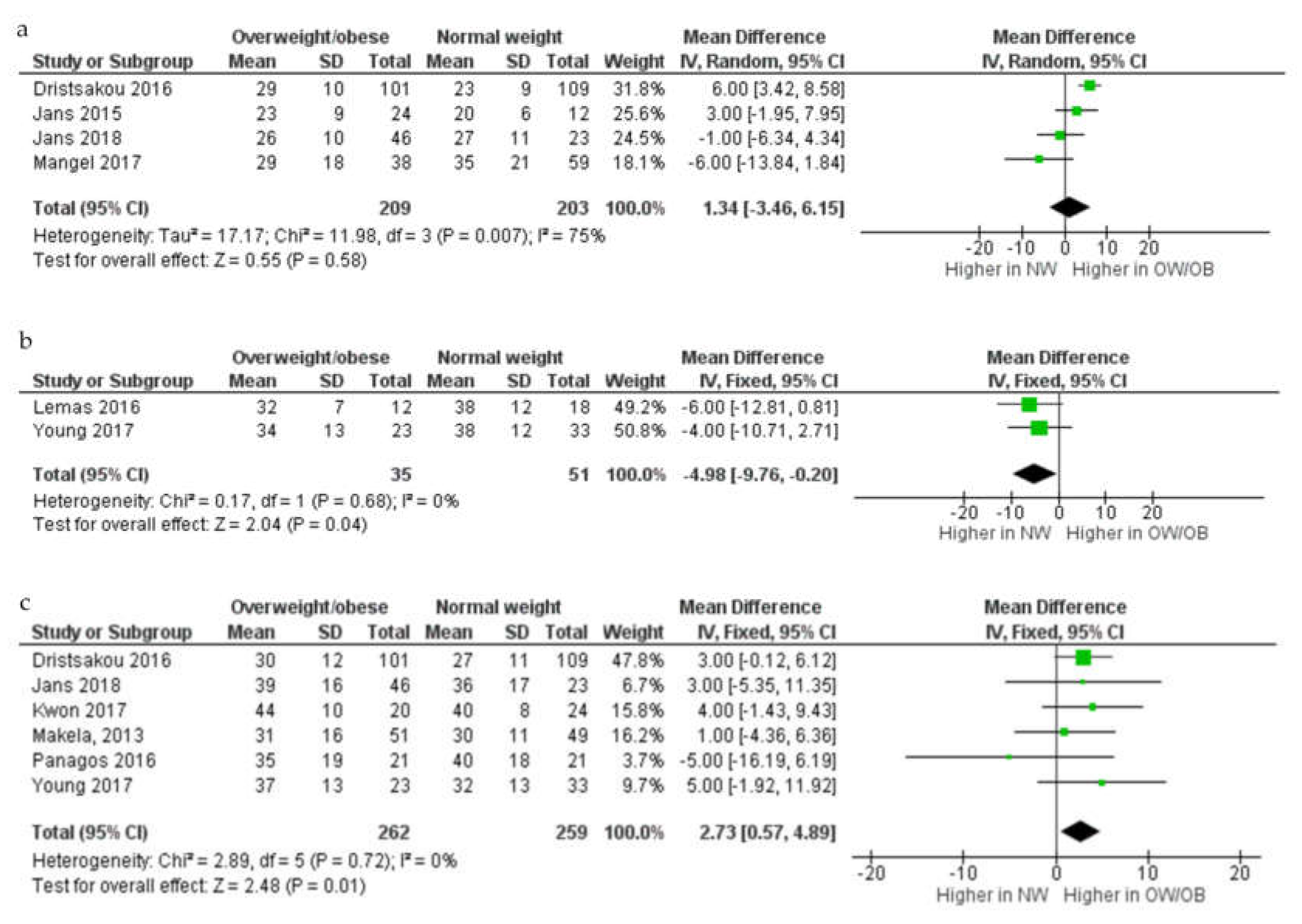
3.2. Fat Concentration
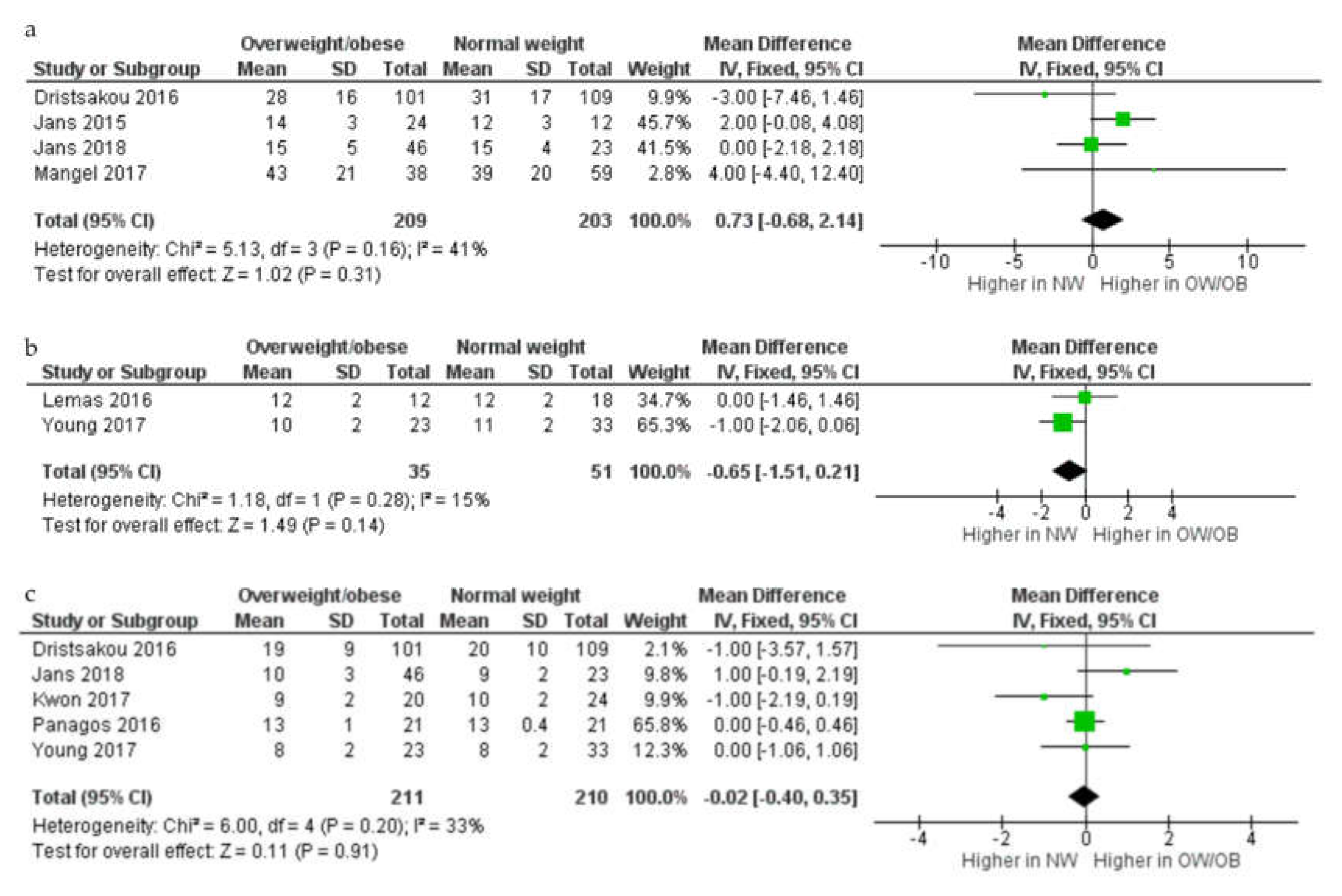
3.3. Protein Concentration
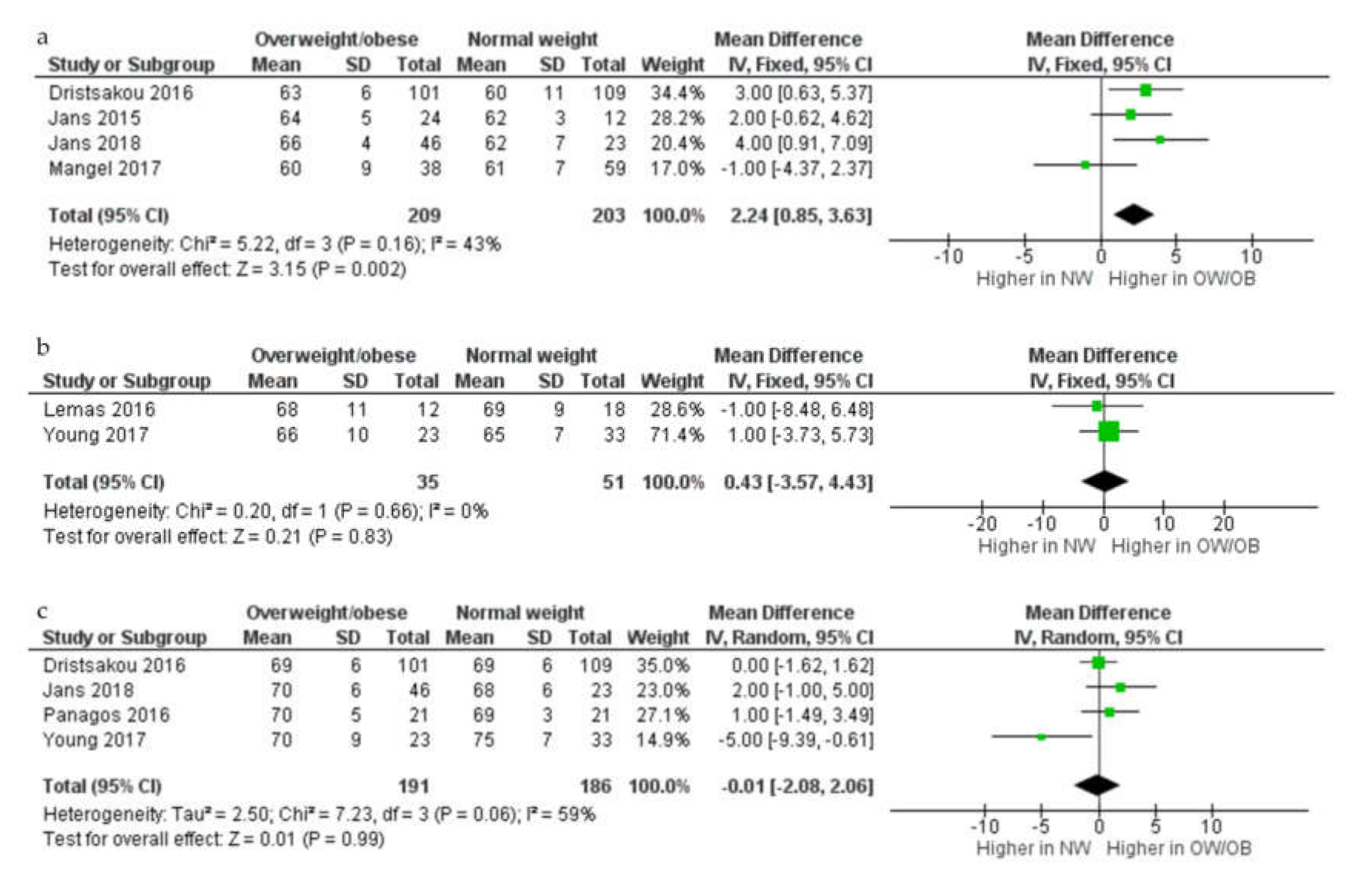
3.4. Lactose Concentration
3.5. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Obesity and Overweight. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 19 June 2019).
- WHO. Challenges, Overweight and Obesity. Available online: http://www.who.int/nutrition/challenges/en/ (accessed on 19 June 2019).
- Athukorala, C.; Rumbold, A.R.; Willson, K.J.; Crowther, C.A. The risk of adverse pregnancy outcomes in women who are overweight or obese. Bmc Pregnancy Childbirth 2010, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Dodd, J.M.; Grivell, R.M.; Nguyen, A.M.; Chan, A.; Robinson, J.S. Maternal and perinatal health outcomes by body mass index category. Aust. N. Z. J. Obs. Gynaecol. 2011, 51, 136–140. [Google Scholar] [CrossRef]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Young, B.E.; Johnson, S.L.; Krebs, N.F. Biological determinants linking infant weight gain and child obesity: Current knowledge and future directions. Adv. Nutr. (BethesdaMd.) 2012, 3, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; George, B.; Williams, M.; Whitaker, K.; Allison, D.B.; Teague, A.; Demerath, E.W. Associations between human breast milk hormones and adipocytokines and infant growth and body composition in the first 6 months of life. Pediatr. Obes. 2017. [Google Scholar] [CrossRef] [Green Version]
- Chang, N.; Jung, J.A.; Kim, H.; Jo, A.; Kang, S.; Lee, S.-W.; Yi, H.; Kim, J.; Yim, J.-G.; Jung, B.-M. Macronutrient composition of human milk from Korean mothers of full term infants born at 37–42 gestational weeks. Nutr. Res. Pract. 2015, 9, 433–438. [Google Scholar] [CrossRef]
- Panagos, P.; Vishwanathan, R.; Penfield-Cyr, A.; Matthan, N.; Shivappa, N.; Wirth, M.; Hebert, J.; Sen, S. Breastmilk from obese mothers has pro-inflammatory properties and decreased neuroprotective factors. J. Perinatol. 2016, 36, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchi, J.; Berg, M.; Dencker, A.; Olander, E.; Begley, C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes. Rev. 2015, 16, 621–638. [Google Scholar] [CrossRef]
- Prentice, P.; Ong, K.K.; Schoemaker, M.H.; van Tol, E.A.; Vervoort, J.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Breast milk nutrient content and infancy growth. Acta Paediatr. 2016, 105, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Ellsworth, L.; Perng, W.; Harman, E.; Das, A.; Pennathur, S.; Gregg, B. Impact of maternal overweight and obesity on milk composition and infant growth. Matern. Child. Nutr. 2020, e12979. [Google Scholar] [CrossRef]
- Andreas, N.J.; Hyde, M.J.; Gale, C.; Parkinson, J.R.; Jeffries, S.; Holmes, E.; Modi, N. Effect of maternal body mass index on hormones in breast milk: A systematic review. PLoS ONE 2014, 9, e115043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, 7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011; Volume 4. [Google Scholar]
- Kugananthan, S.; Gridneva, Z.; Lai, C.T.; Hepworth, A.R.; Mark, P.J.; Kakulas, F.; Geddes, D.T. Associations between Maternal Body Composition and Appetite Hormones and Macronutrients in Human Milk. Nutrients 2017, 9, 252. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2016.
- Sinanoglou, V.J.; Cavouras, D.; Boutsikou, T.; Briana, D.D.; Lantzouraki, D.Z.; Paliatsiou, S.; Volaki, P.; Bratakos, S.; Malamitsi-Puchner, A.; Zoumpoulakis, P. Factors affecting human colostrum fatty acid profile: A case study. PLoS ONE 2017, 12, e0175817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, R.; Lawrence, R. Biochemistry of Human Milk. Breastfeeding. A Guide for the Medical Profession, 6th ed.; Elsevier Mosby: Philadelphia, PA, USA, 2005; pp. 105–170. [Google Scholar]
- Wells GA, S.B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014. [Google Scholar]
- Neville, M.C.; Allen, J.C.; Watters, C. The mechanisms of milk secretion. In Lactation; Springer: Berlin, Germany, 1983; pp. 49–102. [Google Scholar]
- Czank, C.; Mitoulas, L.R.; Hartmann, P.E. Human milk composition-fat. In Hale & Hartmann’s Textbook of Human Lactation; Hale Pub.: Amarillo, TX, USA, 2007; pp. 49–63. [Google Scholar]
- Aleali, F.; Kazemian, M.; Fakhraee, S.H.; Afjeh, A. Longitudinal Changes in the Macronutrient Contents of Breast Milk in the Mothers with Preterm Delivery. Iran. J. Neonatol. Ijn 2018, 9, 29–36. [Google Scholar]
- Antonakou, A.; Skenderi, K.P.; Chiou, A.; Anastasiou, C.A.; Bakoula, C.; Matalas, A.-L. Breast milk fat concentration and fatty acid pattern during the first six months in exclusively breastfeeding Greek women. Eur. J. Nutr. 2013, 52, 963–973. [Google Scholar] [CrossRef]
- Aumeistere, L.; Ciprovica, I.; Zavadska, D.; Celmalniece, K. Lactose content of breast milk among lactating women in Latvia. Age (Years) 2017, 31, 26–39. [Google Scholar]
- Barbosa, L.; Butte, N.F.; Villalpando, S.; Wong, W.W.; Smith, E. Maternal energy balance and lactation performance of Mesoamerindians as a function of body mass index. Am. J. Clin. Nutr. 1997, 66, 575–583. [Google Scholar] [CrossRef]
- Brown, K.H.; Akhtar, N.A.; Robertson, A.D.; Ahmed, M.G. Lactational capacity of marginally nourished mothers: Relationships between maternal nutritional status and quantity and proximate composition of milk. Pediatrics 1986, 78, 909–919. [Google Scholar]
- Bzikowska-Jura, A.; Czerwonogrodzka-Senczyna, A.; Olędzka, G.; Szostak-Węgierek, D.; Weker, H.; Wesołowska, A. Maternal Nutrition and Body Composition During Breastfeeding: Association with Human Milk Composition. Nutrients 2018, 10, 1379. [Google Scholar] [CrossRef] [Green Version]
- De Luca, A.; Frasquet-Darrieux, M.; Gaud, M.-A.; Christin, P.; Boquien, C.-Y.; Millet, C.; Herviou, M.; Darmaun, D.; Robins, R.J.; Ingrand, P. Higher leptin but not human milk macronutrient concentration distinguishes normal-weight from obese mothers at 1-month postpartum. PLoS ONE 2016, 11, e0168568. [Google Scholar] [CrossRef] [PubMed]
- Dritsakou, K.; Liosis, G.; Valsami, G.; Polychronopoulos, E.; Skouroliakou, M. The impact of maternal-and neonatal-associated factors on human milk’s macronutrients and energy. J. Matern. -Fetal Neonatal. Med. 2017, 30, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Eilers, E.; Ziska, T.; Harder, T.; Plagemann, A.; Obladen, M.; Loui, A. Leptin determination in colostrum and early human milk from mothers of preterm and term infants. Early Hum. Dev. 2011, 87, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, M.; França, E.L.; Fiorin, V.; Morais, T.C.; Honorio-França, A.C.; de Abreu, L.C. Changes in the biochemical and immunological components of serum and colostrum of overweight and obese mothers. BMC Pregnancy Childbirth 2015, 15, 166. [Google Scholar] [CrossRef] [PubMed]
- Gridneva, Z.; Tie, W.; Rea, A.; Lai, C.; Ward, L.; Murray, K.; Hartmann, P.; Geddes, D. Human milk casein and whey protein and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 1332. [Google Scholar] [CrossRef] [Green Version]
- Jans, G.; Matthys, C.; Lannoo, M.; Van der Schueren, B.; Devlieger, R. Breast milk macronutrient composition after bariatric surgery. Obes. Surg. 2015, 25, 938–941. [Google Scholar] [CrossRef]
- Jans, G.; Devlieger, R.; De Preter, V.; Ameye, L.; Roelens, K.; Lannoo, M.; Van der Schueren, B.; Verhaeghe, J.; Matthys, C. Bariatric surgery does not appear to affect Women’s breast-Milk composition. J. Nutr. 2018, 148, 1096–1102. [Google Scholar] [CrossRef]
- Kierson, J.A.; Dimatteo, D.M.; Locke, R.G.; Mackley, A.B.; Spear, M.L. Ghrelin and cholecystokinin in term and preterm human breast milk. Acta Paediatr. 2006, 95, 991–995. [Google Scholar] [CrossRef]
- Kurniati, A.M.; Sunardi, D.; Sungkar, A.; Bardosono, S.; Kartinah, N.T. Associations of maternal body composition and nutritional intake with fat content of Indonesian mothers’ breast milk. Paediatr. Indones. 2016, 56, 299. [Google Scholar] [CrossRef] [Green Version]
- Kwon, M.R. Nutrient Content of Human Breast Milk from Overweight and Normal Weight Caucasian Women of Northeast Tennessee; East Tennessee State University: Johnson, TN, USA, 2017. [Google Scholar]
- Lemas, D.J.; Young, B.E.; Baker, P.R.; Tomczik, A.C.; Soderborg, T.K.; Hernandez, T.L.; de la Houssaye, B.A.; Robertson, C.E.; Rudolph, M.C.; Ir, D. Alterations in human milk leptin and insulin are associated with early changes in the infant intestinal microbiome. Am. J. Clin. Nutr. 2016, 103, 1291–1300. [Google Scholar] [CrossRef]
- Ley, S.H.; Hanley, A.J.; Sermer, M.; Zinman, B.; O’Connor, D.L. Associations of prenatal metabolic abnormalities with insulin and adiponectin concentrations in human milk. Am. J. Clin. Nutr. 2012, 95, 867–874. [Google Scholar] [CrossRef] [Green Version]
- Makela, J.; Linderborg, K.; Niinikoski, H.; Yang, B.; Lagström, H. Breast milk fatty acid composition differs between overweight and normal weight women: The STEPS Study. Eur. J. Nutr. 2013, 52, 727–735. [Google Scholar] [CrossRef]
- Mangel, L.; Mimouni, F.; Feinstein-Goren, N.; Lubetzky, R.; Mandel, D.; Marom, R. The effect of maternal habitus on macronutrient content of human milk colostrum. J. Perinatol. 2017, 37, 818. [Google Scholar] [CrossRef] [PubMed]
- Nommsen, L.A.; Lovelady, C.A.; Heinig, M.J.; Lonnerdal, B.; Dewey, K.G. Determinants of energy, protein, lipid, and lactose concentrations in human milk during the first 12 mo of lactation: The DARLING Study. Am. J. Clin. Nutr. 1991, 53, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Quinn, E.A.; Largado, F.; Power, M.; Kuzawa, C.W. Predictors of breast milk macronutrient composition in Filipino mothers. Am. J. Hum. Biol. 2012, 24, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, M.C.; Young, B.E.; Lemas, D.J.; Palmer, C.E.; Hernandez, T.L.; Barbour, L.A.; Friedman, J.E.; Krebs, N.F.; MacLean, P.S. Early infant adipose deposition is positively associated with the n-6 to n-3 fatty acid ratio in human milk independent of maternal BMI. Int. J. Obes. (Lond.) 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schueler, J.; Alexander, B.; Hart, A.M.; Austin, K.; Larson-Meyer, D.E. Presence and dynamics of leptin, GLP-1, and PYY in human breast milk at early postpartum. Obesity 2013, 21, 1451–1458. [Google Scholar] [CrossRef] [PubMed]
- Villalpando, S.; Butte, N.; Wong, W.; Flores-Huerta, S.; Hernandez-Beltran, M.d.J.; Smith, E.; Garza, C. Lactation performance of rural Mesoamerindians. Eur. J. Clin. Nutr. 1992, 46, 337–348. [Google Scholar] [PubMed]
- Villalpando, S.; Del Prado, M.; Lance, A.; Alfonso, E.; Rodríguez, M.; Demmelmair, H.; Koletzko, B. [13C] linoleic acid oxidation and transfer into milk in stunted lactating women with contrasting body mass indexes. Am. J. Clin. Nutr. 2001, 74, 827–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, T.; Zhang, Y.; Ning, Y.; You, L.; Ma, D.; Zheng, Y.; Yang, X.; Li, W.; Wang, J.; Wang, P. Breast milk macronutrient composition and the associated factors in urban Chinese mothers. Chin. Med. J. (Engl.) 2014, 127, 1721–1725. [Google Scholar] [PubMed]
- Young, B.E.; Patinkin, Z.W.; Pyle, L.; de la Houssaye, B.; Davidson, B.S.; Geraghty, S.; Morrow, A.L.; Krebs, N. Markers of oxidative stress in human milk do not differ by maternal BMI but are related to infant growth trajectories. Matern. Child. Health J. 2017, 21, 1367–1376. [Google Scholar] [CrossRef] [PubMed]
- Cannon, A.M.; Kakulas, F.; Hepworth, A.R.; Lai, C.T.; Hartmann, P.E.; Geddes, D.T. The Effects of Leptin on Breastfeeding Behaviour. Int. J. Environ. Res. Public Health 2015, 12, 12340–12355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Hepworth, A.R.; Prime, D.K.; Lai, C.T.; Trengove, N.J.; Hartmann, P.E. Variation in fat, lactose, and protein composition in breast milk over 24 h: Associations with infant feeding patterns. J. Hum. Lact. 2013, 29, 81–89. [Google Scholar] [CrossRef]
- Kim, H.; Kang, S.; Jung, B.-M.; Yi, H.; Jung, J.A.; Chang, N. Breast milk fatty acid composition and fatty acid intake of lactating mothers in South Korea. Br. J. Nutr. 2017, 117, 556–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Prime, D.K.; Hepworth, A.R.; Lai, C.T.; Trengove, N.J.; Hartmann, P.E. Investigation of short-term variations in term breast milk composition during repeated breast expression sessions. J. Hum. Lact. 2013, 29, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Grote, V.; Verduci, E.; Scaglioni, S.; Vecchi, F.; Contarini, G.; Giovannini, M.; Koletzko, B.; Agostoni, C. Breast milk composition and infant nutrient intakes during the first 12 months of life. Eur. J. Clin. Nutr. 2016, 70, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Gerss, J. Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants. Clin. Nutr. 2011, 30, 215–220. [Google Scholar] [CrossRef]
- Bachour, P.; Yafawi, R.; Jaber, F.; Choueiri, E.; Abdel-Razzak, Z. Effects of smoking, mother’s age, body mass index, and parity number on lipid, protein, and secretory immunoglobulin A concentrations of human milk. Breastfeed. Med. 2012, 7, 179–188. [Google Scholar] [CrossRef]
- Michaelsen, K.F.; Larsen, P.S.; Thomsen, B.L.; Samuelson, G. The Copenhagen Cohort Study on Infant Nutrition and Growth: Breast-milk intake, human milk macronutrient content, and influencing factors. Am. J. Clin. Nutr. 1994, 59, 600–611. [Google Scholar] [CrossRef] [Green Version]
- Dizdar, E.A.; Sari, F.N.; Degirmencioglu, H.; Canpolat, F.E.; Oguz, S.S.; Uras, N.; Dilmen, U. Effect of mode of delivery on macronutrient content of breast milk. J. Matern. -Fetal Neonatal Med. 2014, 27, 1099–1102. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, J.Y.; Kim, O.Y.; Ham, B.M.; Kim, H.-J.; Kwon, D.Y.; Jang, Y.; Lee, J.H. Metabolic profiling of plasma in overweight/obese and lean men using ultra performance liquid chromatography and Q-TOF mass spectrometry (UPLC− Q-TOF MS). J. Proteome Res. 2010, 9, 4368–4375. [Google Scholar] [CrossRef] [PubMed]
- Xie, G.; Ma, X.; Zhao, A.; Wang, C.; Zhang, Y.; Nieman, D.; Nicholson, J.K.; Jia, W.; Bao, Y.; Jia, W. The metabolite profiles of the obese population are gender-dependent. J. Proteome Res. 2014, 13, 4062–4073. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; Hankard, R.; Alexandre-Gouabau, M.-C.; Ferchaud-Roucher, V.; Darmaun, D.; Boquien, C.-Y. Higher concentrations of branched-chain amino acids in breast milk of obese mothers. Nutrition 2016, 32, 1295–1298. [Google Scholar] [CrossRef] [PubMed]
- Larnkjær, A.; Bruun, S.; Pedersen, D.; Zachariassen, G.; Barkholt, V.; Agostoni, C.; Christian, M.; Husby, S.; Michaelsen, K.F. Free amino acids in human milk and associations with maternal anthropometry and infant growth. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 374–378. [Google Scholar] [CrossRef] [Green Version]
- Czank, C.; Mitoulas, L.; Hartmann, P. Human milk composition: Nitrogen and energy content. In Hale and Hartmann’s Text Book of Human Lactation; Hartmann, P.E., Hale, T.W., Eds.; Springer: Berlin, Germany, 2007; pp. 89–102. [Google Scholar]
- Lönnerdal, B.; Forsum, E.; Hambraeus, L. A longitudinal study of the protein, nitrogen, and lactose contents of human milk from Swedish well-nourished mothers. Am. J. Clin. Nutr. 1976, 29, 1127–1133. [Google Scholar] [CrossRef] [Green Version]
- Emmett, P.M.; Rogers, I.S. Properties of human milk and their relationship with maternal nutrition. Early Hum. Dev. 1997, 49, S7–S28. [Google Scholar] [CrossRef]
- Luque, V.; Closa-Monasterolo, R.; Escribano, J.; Ferré, N. Early programming by protein intake: The effect of protein on adiposity development and the growth and functionality of vital organs. Nutr. Metab. Insights 2015, 8, NMI. S29525. [Google Scholar] [CrossRef]
- Martin, C.; Ling, P.-R.; Blackburn, G. Review of infant feeding: Key features of breast milk and infant formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef] [Green Version]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef] [Green Version]
- Kent, J.C.; Mitoulas, L.R.; Cregan, M.D.; Ramsay, D.T.; Doherty, D.A.; Hartmann, P.E. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics 2006, 117, e387–e395. [Google Scholar] [CrossRef] [Green Version]
- Peila, C.; Gazzolo, D.; Bertino, E.; Cresi, F.; Coscia, A. Influence of Diabetes during Pregnancy on Human Milk Composition. Nutrients 2020, 12, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Site | Study Design | Sample Size | Stage of Lactation | Measure Maternal Obesity | Nutrients Assessed | ||
|---|---|---|---|---|---|---|---|---|
| Milk Fat or TGs | Milk Protein | Milk Lactose or Carbohydrates | ||||||
| Aleali, 2018 [23] | Iran | Longitudinal | 51 | 1, 2, 3, and 4 wk | BMI | √ | √ | √ |
| Antonakou, 2013 [24] | Greece | Longitudinal | 64 | 1, 3, and 6 mo | BMI | √ | ||
| Aumeistere, 2017 [25] | Latvia | Cross-sectional | 28 | 2–21 mo | BMI | √ | ||
| Barbosa, 1997 [26] | Mexico | Longitudinal | 40 | 3 and 6 mo | BMI | √ | √ | √ |
| Brown, 1986 [27] | Bangladesh | Intervention | 58 | 1–9 mo | Arm circumference, skinfold | √ | √ | √ |
| Bzikowska-Jura, 2018 [28] | Poland | Longitudinal | 40 | 1, 3, and 6 mo | BMI, BIA | √ | √ | √ |
| Chang, 2015 [8] | Korea | Cross-sectional | 2,632 | 0–8 mo | BMI | √ | √ | √ |
| DeLuca, 2016 [29] | France | Cross-sectional | 100 | 1 mo | BMI | √ | √ | √ |
| Dritsakou, 2017 [30] | Greece | Longitudinal | 305 | 3, 7, and 30 day | BMI | √ | √ | √ |
| Eilers, 2011 [31] | Germany | Longitudinal | 77 | 3 and 28 day | BMI | √ | √ | |
| Fujimori, 2015 [32] | Brazil | Cross-sectional | 68 | 2–3 day | BMI | √ | √ | |
| Gridneva, 2018 [33] | Australia | Longitudinal | 20 | 2, 5, 9, and 12 mo | BMI, BIS | √ | ||
| Jans, 2015 [34] | Belgium | Cross-sectional | 48 | 4 day | BMI | √ | √ | √ |
| Jans, 2018 [35] | Belgium | Longitudinal | 75 | 3 or 4 day and 1–6 wk | BMI | √ | √ | √ |
| Kierson, 2006 [36] | USA | Cross-sectional | 20 | 7–21 day | BMI | √ | ||
| Kugananthan, 2017 [16] | Australia | Longitudinal | 59 | 2, 5, 9, and 12 mo | BMI, BIS | √ | √ | |
| Kurniati, 2016 [37] | Indonesia | Cross-sectional | 48 | 1 mo | BMI, BIA | √ | ||
| Kwon, 2017 [38] | USA | Cross-sectional | 44 | 2–14 wk | BMI | √ | √ | |
| Lemas, 2016 [39] | USA | Cross-sectional | 30 | 2 wk | BMI | √ | √ | √ |
| Ley, 2012 [40] | Canada | Longitudinal | 170 | 1 or 7 day and 3 mo | BMI | √ | √ | |
| Makela, 2013 [41] | Finland | Cross-sectional | 163 | 3 mo | BMI | √ | ||
| Mangel, 2017 [42] | Israel | Cross-sectional | 109 | 1–2 day | BMI | √ | √ | √ |
| Nommsen, 1991 [43] | USA | Longitudinal | 92 | 3, 6, 9, and 12 mo | Skinfold, % IBW | √ | √ | √ |
| Panagos, 2016 [9] | USA | Cross-sectional | 42 | 4–10 wk | BMI | √ | √ | √ |
| Quinn, 2012 [44] | Philippines | Cross-sectional | 102 | 0–18 mo | BMI, skinfold | √ | √ | √ |
| Rudolph, 2017 [45] | USA | Longitudinal | 48 | 2 wk and 4 mo | BMI | √ | ||
| Schueler, 2013 [46] | USA | Cross-sectional | 13 | 29–38 day | BMI, waist circumference, DXA | √ | ||
| Villalpando, 1992 [47] | Mexico | Cross-sectional | 30 | 4 or 6 mo | BMI, skinfold | √ | √ | √ |
| Villalpando, 2001 [48] | Mexico | Intervention | 10 | 5–6 mo | BMI, skinfold | √ | ||
| Yang, 2014 [49] | China | Cross-sectional | 436 | 5–11, 12–30, 31–60, 61–120 or 121–240 day | BMI | √ | √ | √ |
| Young, 2017 [50] | USA | Longitudinal | 56 | 2 wk and 4 mo | BMI | √ | √ | √ |
| Gestational Age | HM Method of Collection | Milk Type | Collection Time | Analytical Method | Outcomes/Effect | |
|---|---|---|---|---|---|---|
| Comparison of Macronutrients between OW/OB and NW Women | ||||||
| Aleali, 2018 [23] | Preterm | NS | Transitional and mature | 14:00–16:00 | MIRIS analyzer, Sweden | No difference in HM fat, protein or lactose between groups |
| Brown, 1986 [27] | NS | Full expression | Mature | 24 h | Gravimetric method, Kjeldahl method and colorimetry | HM fat was higher in women with higher AC and TCSF. No difference in HM protein or lactose between groups |
| DeLuca, 2016 [29] | Term | Full expression | Mature | 9:00–11:00 | MIRIS analyzer, Sweden | No difference in HM fat, protein or lactose between groups |
| Dritsakou, 2017 * [30] | Preterm and term | Full expression | Colostrum, transitional and mature | 24 h | MIRIS analyzer, Sweden | HM fat (colostrum, transitional and mature) was higher in OW/OB women. No difference in HM protein and lactose between groups |
| Fujimori, 2015 [32] | Term | NS | Colostrum | NS | Creamatocrit, Biuret colorimetric | HM fat was higher in OB women. No difference in HM protein between groups |
| Jans, 2015* [34] | Term | Mid-feed | Colostrum | NS | MIRIS analyzer, Sweden | HM fat was higher in OB women. No difference in HM protein or lactose |
| Jans, 2018* [35] | Term | Mid-feed | Colostrum, transitional and mature | NS | MIRIS analyzer, Sweden | No difference in HM fat, protein or lactose between groups |
| Kwon, 2017* [38] | NS | NS | Mature | NS | Lipid extraction, Kjeldahl method | No difference in HM fat or protein between groups |
| Lemas, 2016* [39] | Term | Mid-feed | Transitional | Morning | Creamatocrit, Bradford protein assay, colorimetric assay | No difference in HM fat, protein or lactose between groups |
| Makela, 2013* [41] | NS | Pre-feed | Mature | Morning | Lipid extraction | No difference in HM fat content between groups |
| Mangel, 2017* [42] | Term | Pre-feed | Colostrum | 8am–3pm | MIRIS analyzer, Sweden | No difference in HM fat, protein or lactose between groups |
| Panagos, 2016* [9] | Term | Full expression | Mature | Morning | Julie Z7 Automatic MilkoScope, Germany | No difference in HM fat, protein or lactose between groups |
| Rudolph, 2017 [45] | Term | Mid-feed | Transitional and mature | Morning | Creamatocrit | HM fat was higher in OW women |
| Villalpando, 2001 [48] | NS | Full expression | Mature | 10:00, 12:00 and 18:00 | Gravimetric method | No difference in HM fat between groups |
| Young, 2017 * [50] | Term | Full expression | Transitional and mature | 10:00-13:00 | Creamatocrit, Bradford assay, enzymatic method | HM protein (transitional) and lactose (mature) were lower in OW/OB women. No difference in HM fat between groups |
| Correlation between maternal measures of maternal obesity and HM macronutrient concentrations | ||||||
| Antonakou, 2013 [24] | Term | Pre-feed | Mature | Morning | Creamatocrit | No correlation between HM fat and BMI |
| Aumeistere, 2017 [25] | NS | NS | Mature | 24 h | HPLC | No correlation between HM lactose and BMI |
| Bzikowska-Jura, 2018 [28] | Term | Pre- and post-feed | Mature | 24 h | MIRIS analyzer, Sweden | HM fat (1 and 6 mo) and protein (3 mo) positively correlated with BMI, and HM protein (3 mo) with % body fat. No correlation of HM lactose with either BMI or %body fat |
| Chang, 2015 [8] | Term | Full expression | Colostrum, transitional and mature | NS | MilkoScan FT2 Foss Analytical, Denmark | HM protein at 0-1 wk, 3–4, and 4–5 mo, and HM fat at 1–2 wk, 2–3, and 7–8 mo positively correlated with BMI. HM lactose at 4–5 and 6–7 mo was negatively correlated with BMI |
| Eilers, 2011 [31] | Preterm and term | Pre- and post-feed | Colostrum and mature | 16:00–20:00 | Creamatocrit, BCA protein assay | No correlation between BMI and HM fat or protein |
| Gridneva, 2018 [33] | Term | Pre- and post-feed | Mature | NS | Bradford protein assay | No correlation between BMI and HM total protein; whey protein was positively correlated to BMI, fat-free mass, fat-free mass index, and fat mass index |
| Kierson, 2006 [36] | Preterm and term | Full expression | Transitional and mature | NS | Creamatocrit | HM fat was positively correlated to maternal BMI |
| Kugananthan, 2017 [16] | Term | Pre- and post-feed | Mature | 9:30–11:30 | Bradford assay, Enzymatic spectrophotometric method | HM protein positively correlated with %body fat, but not BMI. No correlation of either %body fat or BMI with HM lactose. |
| Kurniati, 2016 [37] | Term | Mid-feed | Mature | 6:00–8:00 | Creamatocrit | No correlation between %body fat and HM fat |
| Ley, 2012 [40] | Term | early milk Full expression | Colostrum/Transitional and mature | NS | Creamatocrit, BCA protein assay | No correlation between BMI and HM fat or protein |
| Nommsen, 1991 [43] | NS | Full expression | Mature | 24 h | Folch extraction, Lowry assay, colorimetric assay | HM fat (6, 9, and 12 mo) and protein (9 mo) positively correlated with %IBM. No correlations with HM lactose |
| Quinn, 2012 [44] | NS | Mid-feed | Colostrum, transitional and mature | 6:00–10:30 | Rose-Gottlieb extraction, automated analyzer, phenol- sulfuric acid method | HM lactose was inversely correlated with BMI. No relationship between %body fat and HM fat, protein, or lactose |
| Schueler, 2013 [46] | NS | Pre- and post-feed | Mature | 7:00-10:00 | Creamatocrit | HM fat positively correlated with total fat mass, BMI, body weight, and %body fat |
| Villalpando, 1992 [47] | Term | Full expression | Mature | 10:00, 12:00, and 18:00 | Jeejeebhoy method, Kjeldahl method, automated enzymatic method | HM fat positively correlated with body weight, BMI, and %body fat. No associations between these measures and HM protein or lactose |
| Yang, 2014 [49] | Term | Full expression | Transitional and mature | 9:00–11:00 | MIRIS analyzer, Sweden | HM protein and fat were positively correlated, and HM lactose negatively correlated, with BMI |
| Both comparison and correlation | ||||||
| Barbosa, 1997 [26] | Term | Full expression | Mature | 10:00, 14:00, and 18:00 | Gravimetric method, Kjeldahl method, automatic enzyme method | HM fat was positively correlated with BMI and %body fat, and was lower in the lower BMI group (<23 kg/m2) compared to the higher (≥23 kg/m2). HM protein and lactose were not correlated with BMI or %body fat and no different between these BMI groups |
| Milk Macronutrient | Effect | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Studies, n | Positive association with Maternal BMI/Adiposity | No Association with Maternal BMI/Adiposity | Negative Association with Maternal BMI/Adiposity | |||||||
| All | Comparison | Correlation | All | Comparison | Correlation | All | Comparison | Correlation | ||
| Fat | 19 | 11 | 4 | 8 | 8 | 3 | 5 | 0 | 0 | 0 |
| Protein | 15 | 6 | 0 | 6 | 9 | 5 | 5 | 0 | 0 | 0 |
| Lactose | 12 | 0 | 0 | 0 | 9 | 4 | 6 | 3 | 0 | 3 |
| Reference | Representativeness Cohort | Measure of Maternal Obesity | Controls for Confounders | Sample Size (Small, Medium or Large Study) | State Gestational Age | State Feeding Mode | Standard Time of HM Collection | State HM Collection Method |
|---|---|---|---|---|---|---|---|---|
| Aleali, 2018 [23] | X | √ | x | Medium | √ | x | √ | x |
| Antonakou, 2013 [24] | √ | √ | √ | Medium | √ | √ | √ | √ |
| Aumeistere, 2017 [25] | X | x | x | Small | x | √ | √ | x |
| Barbosa, 1997 [26] | X | √ | x | Small | √ | x | √ | √ |
| Brown, 1986 [27] | √ | √ | √ | Medium | x | x | √ | √ |
| Bzikowska-Jura, 2018 [28] | √ | √ | x | Small | √ | √ | √ | √ |
| Chang, 2015 [8] | √ | √ | √ | Large | √ | x | x | √ |
| DeLuca, 2016 [29] | √ | √ | √ | Medium | √ | √ | √ | √ |
| Dritsakou, 2017 [30] | X | x | x | Large | √ | √ | √ | √ |
| Eilers, 2011 [31] | √ | x | x | Medium | √ | x | √ | √ |
| Fujimori, 2015 [32] | √ | x | x | Medium | √ | √ | x | x |
| Gridneva, 2018 [33] | √ | √ | √ | Small | √ | √ | x | √ |
| Jans, 2015 [34] | √ | √ | x | Small | √ | x | x | √ |
| Jans, 2018 [35] | √ | √ | x | Medium | √ | x | x | √ |
| Kierson, 2006 [36] | X | x | x | Small | √ | x | x | √ |
| Kugananthan, 2017 [16] | √ | √ | x | Medium | √ | √ | √ | √ |
| Kurniati, 2016 [37] | √ | √ | x | Small | √ | √ | √ | √ |
| Kwon, 2017 [38] | √ | x | x | Small | x | x | x | x |
| Lemas, 2016 [39] | √ | √ | √ | Small | √ | √ | √ | √ |
| Ley, 2012 [40] | √ | x | √ | Large | √ | x | x | x |
| Makela, 2013 [41] | √ | √ | x | Large | x | x | √ | √ |
| Mangel, 2017 [42] | √ | x | x | Large | √ | x | √ | √ |
| Nommsen, 1991 [43] | √ | √ | √ | Medium | x | √ | √ | √ |
| Panagos, 2016 [9] | √ | √ | √ | Small | √ | x | √ | √ |
| Quinn, 2012 [44] | √ | √ | √ | Large | x | √ | √ | √ |
| Rudolph, 2017 [45] | √ | x | x | Small | √ | √ | √ | √ |
| Schueler, 2013 [46] | √ | √ | √ | Small | x | √ | √ | √ |
| Villalpando, 1992 [47] | X | √ | x | Small | √ | √ | √ | √ |
| Villalpando, 2001 [48] | X | √ | x | Small | x | √ | √ | √ |
| Yang, 2014 [49] | √ | √ | √ | Large | √ | √ | √ | √ |
| Young, 2017 [50] | √ | √ | √ | Medium | √ | √ | √ | √ |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leghi, G.E.; Netting, M.J.; Middleton, P.F.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. The Impact of Maternal Obesity on Human Milk Macronutrient Composition: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 934. https://doi.org/10.3390/nu12040934
Leghi GE, Netting MJ, Middleton PF, Wlodek ME, Geddes DT, Muhlhausler BS. The Impact of Maternal Obesity on Human Milk Macronutrient Composition: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(4):934. https://doi.org/10.3390/nu12040934
Chicago/Turabian StyleLeghi, Gabriela E., Merryn J. Netting, Philippa F. Middleton, Mary E. Wlodek, Donna T. Geddes, and Beverly S. Muhlhausler. 2020. "The Impact of Maternal Obesity on Human Milk Macronutrient Composition: A Systematic Review and Meta-Analysis" Nutrients 12, no. 4: 934. https://doi.org/10.3390/nu12040934