Cardiorespiratory Fitness, Physical Activity, Sedentary Time and Its Association with the Atherogenic Index of Plasma in Chilean Adults: Influence of the Waist Circumference to Height Ratio

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Participants’ Evaluation
2.3. Anthropometric Measurements
2.4. Classification of Physical Activity and Sedentary Time
2.5. Classification of the Cardiorespiratory Fitness
2.6. Calculation of Physical Activity, Cardiorespiratory Fitness, and Sedentary Time Index Score (PACS)
2.7. Atherogenic Index of Plasma (AIP)
2.8. Covariates
2.9. Statistical Analysis
3. Results
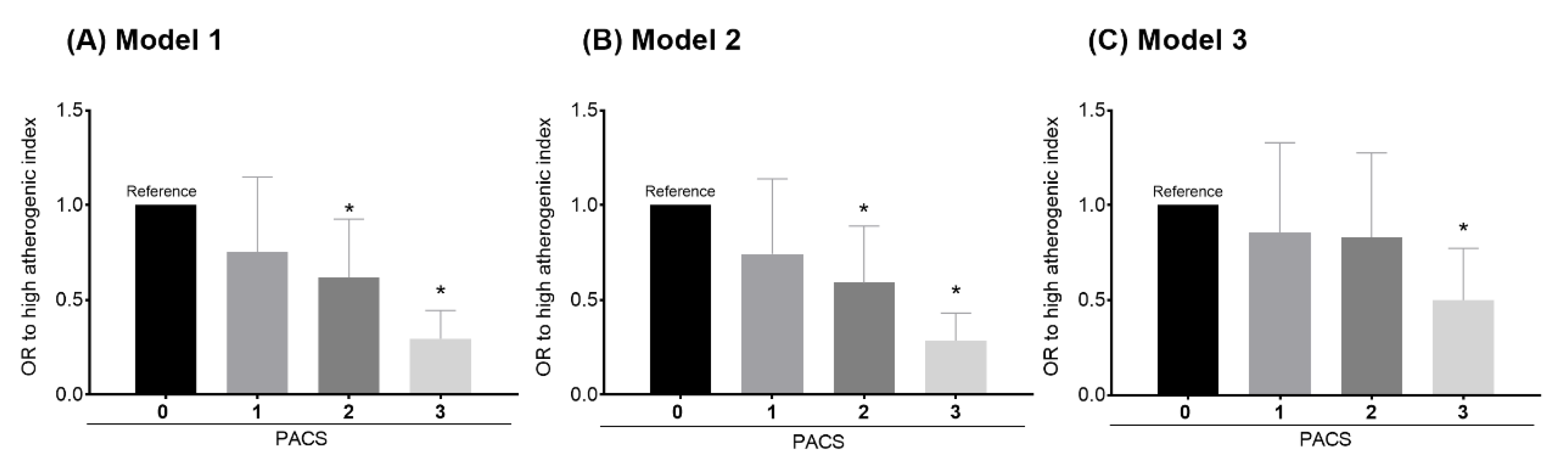
3.1. Models for Combined Analysis
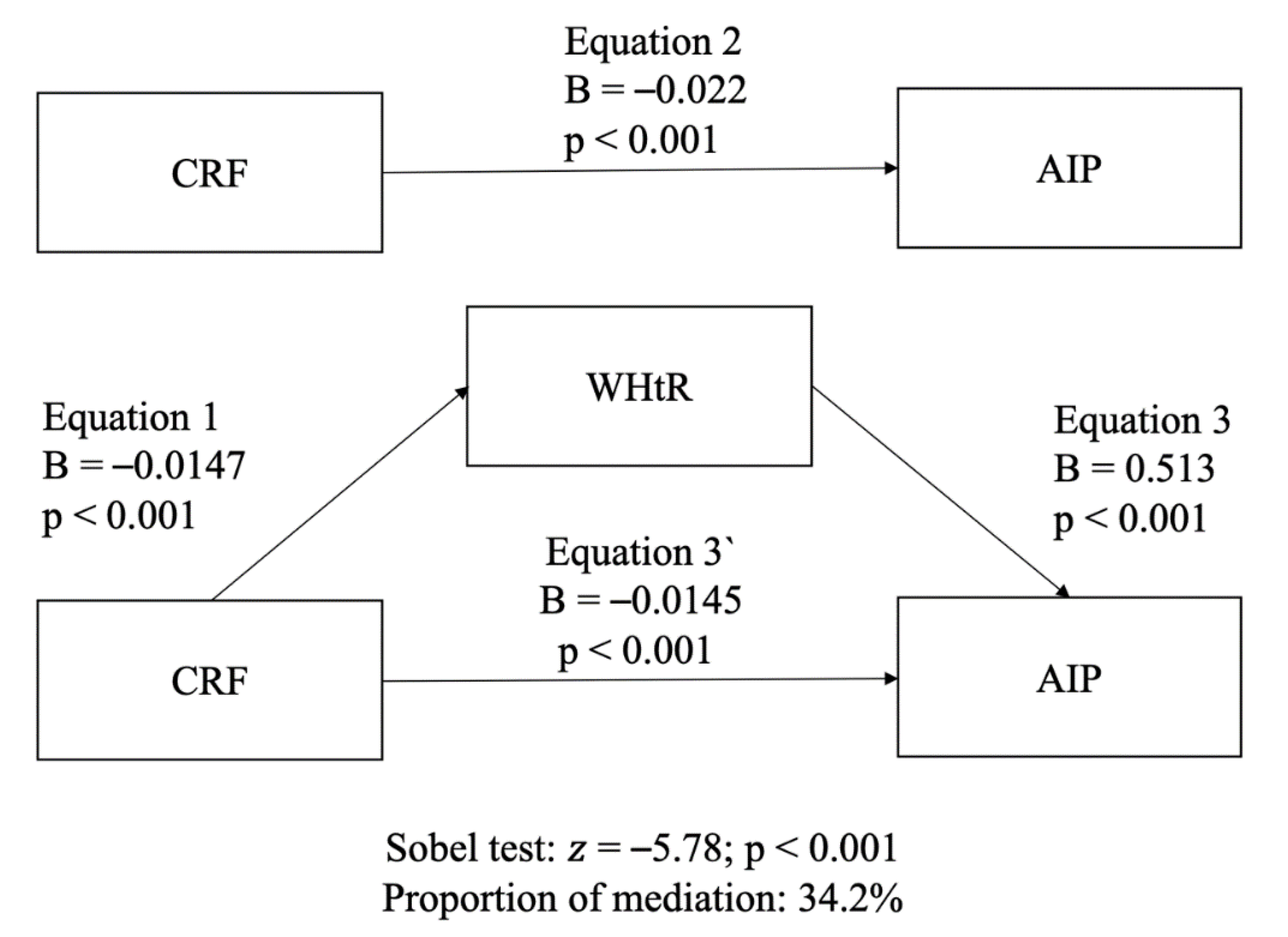
3.2. Independent Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. Circulation 2019, 139. [Google Scholar] [CrossRef]
- Fernández-Macías, J.C.; Ochoa-Martínez, A.C.; Varela-Silva, J.A.; Pérez-Maldonado, I.N. Atherogenic Index of Plasma: Novel Predictive Biomarker for Cardiovascular Illnesses. Arch. Med. Res. 2019, 50, 285–294. [Google Scholar] [CrossRef]
- Zhu, X.; Yu, L.; Zhou, H.; Ma, Q.; Zhou, X.; Lei, T.; Hu, J.; Xu, W.; Yi, N.; Lei, S. Atherogenic Index of Plasma Is a Novel and Better Biomarker Associated with Obesity: A Population-Based Cross-Sectional Study in China. Lipids Health Dis. 2018, 17, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Dobiášová, M.; Frohlich, J. The Plasma Parameter Log (TG/HDL-C) as an Atherogenic Index: Correlation with Lipoprotein Particle Size and Esterification Rate Inapob-Lipoprotein-Depleted Plasma (FERHDL). Clin. Biochem. 2001, 34, 583–588. [Google Scholar] [CrossRef]
- Zalejska-Fiolka, J.; Hubková, B.; Birková, A.; Veliká, B.; Puchalska, B.; Kasperczyk, S.; Błaszczyk, U.; Fiolka, R.; Bożek, A.; Maksym, B.; et al. Prognostic Value of the Modified Atherogenic Index of Plasma during Body Mass Reduction in Polish Obese/Overweight People. Int. J. Environ. Res. Public Health 2019, 16, 68. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, S.; Bhattacharjee, J.; Bhatnagar, M.K.; Tyagi, S. Atherogenic Index of Plasma, Castelli Risk Index and Atherogenic Coeficent—New Parameters in Assessing Cardiovascular Risk. Int. J. Pharm. Biol. Sci. 2013, 3, 359–364. [Google Scholar]
- Edwards, M.K.; Loprinzi, P.D. Atherogenic Index of Plasma and the Gamma Gap: Considerations by Physical Activity. Int. J. Cardiol. 2016, 222, 946–948. [Google Scholar] [CrossRef]
- Onat, A.; Can, G.; Kaya, H.; Hergenç, G. “Atherogenic Index of Plasma” (Log10 Triglyceride/High-Density Lipoprotein-Cholesterol) Predicts High Blood Pressure, Diabetes, and Vascular Events. J. Clin. Lipidol. 2010, 4, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.W.; Deng, F.Y.; Lei, S.F. Meta-Analysis of Atherogenic Index of Plasma and Other Lipid Parameters in Relation to Risk of Type 2 Diabetes Mellitus. Prim. Care Diabetes 2015, 9, 60–67. [Google Scholar] [CrossRef]
- Choudhary, M.K.; Eräranta, A.; Koskela, J.; Tikkakoski, A.J.; Nevalainen, P.I.; Kähönen, M.; Mustonen, J.; Pörsti, I. Atherogenic Index of Plasma Is Related to Arterial Stiffness but Not to Blood Pressure in Normotensive and Never-Treated Hypertensive Subjects. Blood Press. 2019, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Zheng, D.; Liu, J.; Fang, L.; Li, Q. Atherogenic Index of Plasma Is a Novel Predictor of Non-Alcoholic Fatty Liver Disease in Obese Participants: A Cross-Sectional Study. Lipids Health Dis. 2018, 17, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, S.W.; Lu, Y.; Li, F.; Yang, C.J.; Feng, Y.B.; Li, H.W.; Yao, W.F.; Shen, Z.H. Atherogenic Index of Plasma Is an Effective Index for Estimating Abdominal Obesity. Lipids Health Dis. 2018, 17, 4–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertelyová, Z.; Vašková, J.; Vaško, L. Waist Circumference-to-Height Ratio Detected in a Convenient Sample of Young Slovak People with Increased Cardio-Metabolic Risk. Cent. Eur. J. Public Health 2016, 24, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashwell, M.; Gibson, S. Waist-to-Height Ratio as an Indicator of Early Health Risk: Simpler and More Predictive than Using a Matrix Based on BMI and Waist Circumference. BMJ Open 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Héroux, M.; Janssen, I.; Lee, D.-C.; Sui, X.; Hebert, J.R.; Blair, S.N. Clustering of Unhealthy Behaviors in the Aerobics Center Longitudinal Study. Prev. Sci. 2012, 13, 183–195. [Google Scholar] [CrossRef] [Green Version]
- Edwards, M.K.; Blaha, M.J.; Loprinzi, P.D. Influence of Sedentary Behavior, Physical Activity, and Cardiorespiratory Fitness on the Atherogenic Index of Plasma. J. Clin. Lipidol. 2017, 11, 119–125. [Google Scholar] [CrossRef]
- Cai, G.; Liu, W.; Lv, S.; Wang, X.; Guo, Y.; Yan, Z.; Du, Y.; Zhou, Y. Gender-Specific Associations between Atherogenic Index of Plasma and the Presence and Severity of Acute Coronary Syndrome in Very Young Adults: A Hospital-Based Observational Study. Lipids Health Dis. 2019, 18, 99. [Google Scholar] [CrossRef] [Green Version]
- Lanas, F.; Serón, P.; Lanas, A. Cardiovascular Disease in Latin America: The Growing Epidemic. Prog. Cardiovasc. Dis. 2014, 57, 262–267. [Google Scholar] [CrossRef]
- Pagan, E.; Chatenoud, L.; Rodriguez, T.; Bosetti, C.; Levi, F.; Malvezzi, M.; La Vecchia, C.; Negri, E.; Bertuccio, P. Comparison of Trends in Mortality from Coronary Heart and Cerebrovascular Diseases in North and South America: 1980 to 2013. Am. J. Cardiol. 2017, 119, 862–871. [Google Scholar] [CrossRef]
- Minsal. Ministerio de Salud. Encuesta Nacional de Salud 2016–2017 Primeros Resultados. 2017. Available online: Http://Web.Minsal.Cl/Wp-Content/Uplo (accessed on 10 January 2019).
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global Physical Activity Questionnaire (GPAQ): Nine Country Reliability and Validity Study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, T.; Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solis-Urra, P.; Cristi-Montero, C.; Romero-Parra, J.; Zavala-Crichton, J.P.; Saez-Lara, M.J.; Plaza-Diaz, J. Passive Commuting and Higher Sedentary Time Is Associated with Vitamin D Deficiency in Adult and Older Women: Results from Chilean National Health Survey 2016–2017. Nutrients 2019, 11, 300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, J.; Kaminsky, L.A.; Lima, R.; Christle, J.W.; Ashley, E.; Arena, R. A Reference Equation for Normal Standards for VO2 Max: Analysis from the Fitness Registry and the Importance of Exercise National Database (FRIEND Registry). Prog. Cardiovasc. Dis. 2017, 60, 21–29. [Google Scholar] [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J. Reference Standards for Cardiorespiratory Fitness Measured with Cardiopulmonary Exercise Testing Data from the Fitness Registry and the Importance of Exercise National Database. Mayo Clin. Proc. 2015, 90, 1515–1523. [Google Scholar] [CrossRef] [Green Version]
- Edwards, M.K.; Loprinzi, P.D. The Association between Muscle Strengthening Activities and Atherogenic Index of Plasma. Prev. Med. 2016, 91, 318–321. [Google Scholar] [CrossRef]
- Lumley, T.; Diehr, P.; Emerson, S.; Chen, L. The Importance of the Normality Assumption in Large Public Health Data Sets. Annu. Rev. Public Health 2002, 23, 151–169. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and Resampling Strategies for Assessing and Comparing Indirect Effects in Multiple Mediator Models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Bolin, J.H. Andrew F. Hayes (2013). Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York, NY: The Guilford Press. J. Educ. Meas. 2014, 51, 335–337. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The Moderator-Mediator Variable Distinction in Social Psychological Research: Conceptual, Strategic, and Statistical Considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Sobel, M.E. Asymptotic Confidence Intervals for Indirect Effects in Structural Equation Models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Edwards, M.K.; Loprinzi, P.D. Physical Activity and Diet on Atherogenic Index of Plasma among Adults in the United States: Mediation Considerations by Central Adiposity. Eur. J. Clin. Nutr. 2018, 72, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Lavie, C.J.; Blair, S.N. Obesity and Cardiovascular Disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Labayen, I.; Lavie, C.J.; Blair, S.N. The Fat but Fit Paradox: What We Know and Don’t Know about It. Br. J. Sports Med. 2018, 52, 151–153. [Google Scholar] [CrossRef]
- Gaesser, G.A.; Blair, S.N. The Health Risks of Obesity Have Been Exaggerated. Med. Sci. Sports Exerc. 2018, 51, 218–221. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Rogers, R.J.; Donnelly, J.E. The Health Risks of Obesity Have Not Been Exaggerated. Med. Sci. Sports Exerc. 2019, 51, 222–225. [Google Scholar] [CrossRef]
- Després, J.P. Physical Activity, Sedentary Behaviours, and Cardiovascular Health: When Will Cardiorespiratory Fitness Become a Vital Sign? Can. J. Cardiol. 2016, 32, 505–513. [Google Scholar] [CrossRef]
- Parto, P.; Lavie, C.J.; Swift, D.; Sui, X. The Role of Cardiorespiratory Fitness on Plasma Lipid Levels. Expert Rev. Cardiovasc. Ther. 2015, 13, 1177–1183. [Google Scholar] [CrossRef]
- Breneman, C.B.; Polinski, K.; Sarzynski, M.A.; Lavie, C.J.; Kokkinos, P.F.; Ahmed, A.; Sui, X. The Impact of Cardiorespiratory Fitness Levels on the Risk of Developing Atherogenic Dyslipidemia. Am. J. Med. 2016, 129, 1060–1066. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Xu, D. Effects of Aerobic Exercise on Lipids and Lipoproteins. Lipids Health Dis. 2017, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamatakis, E.; Gill, J.M.R. Sitting Behaviour and Physical Activity: Two Sides of the Same Cardiovascular Health Coin? Br. J. Sports Med. 2019, 53, 852–853. [Google Scholar] [CrossRef] [PubMed]
- Das, S.R.; De Lemos, J.A.; Blair, S.N.; Berry, J.D. Sedentary Time in the General Population. Mayo Clin. Proc. 2014, 89, 1063–1071. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Steene-johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I. Does Physical Activity Attenuate, or Even Eliminate, the Detrimental Association of Sitting Time with Mortality? A Harmonised Meta-Analysis of Data from More than 1 Million Men and Women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Kaminsky, L.A.; Myers, J.; Arena, R. Determining Cardiorespiratory fitness with precision: Compendium of findings from the friend registry. Prog. Cardiovasc. Dis. 2019, 62, 76–82. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Overall (n = 4671) | PACS Score | p-Value | |||
|---|---|---|---|---|---|---|
| 0 (n = 291) | 1 (n = 1140) | 2 (n = 1854) | 3 (n = 1386) | |||
| Age (years) | 49.40 ± 16.40 | 48.48 ± 17.36 | 49.14 ± 16.96 | 48.95 ± 16.18 | 50.42 ± 15.97 | 0.156 |
| Sex (n/%) | M 1670/35.7 W 3001/64.2 | M 95/32.6 W 196/67.4 | M 339/29.7 W 801/70.3 | M 636/34.3 W 1218/65.7 | M 600/43.3 W 786/56.7 | 0.000 |
| Body mass (kg) | 74.90 ± 15.35 | 89.61 ± 14.30 | 80.25 ± 16.03 | 75.04 ± 15.26 | 67.24 ± 10.05 | 0.000 |
| Height (cm) | 159.93 ± 9.30 | 161.76 ± 10.17 | 159.96 ± 9.37 | 159.98 ± 9.30 | 159.46 ± 9.00 | 0.076 |
| Body mass index (kg/m2) | 29.28 ± 5.49 | 34.33 ± 5.20 | 31.39 ± 5.98 | 29.29 ± 5.31 | 26.44 ± 3.39 | 0.000 |
| Atherogenic index of plasma (mmol/L) | 0.44 ± 0.30 | 0.52 ± 0.30 | 0.48 ± 0.29 | 0.45 ± 0.29 | 0.38 ± 0.30 | 0.000 |
| % (n) meeting PA guidelines | 30.4% (1,424) | 0% (0) | 5.7% (266) | 24.7% (1,158) | 100% (1,386) | 0.000 |
| Cardiorespiratory fitness (mL/kg/min) | 30.86 ± 9.08 | 26.67 ± 8.96 | 28.63 ± 9.29 | 30.79 ± 8.83 | 33.63 ± 8.39 | 0.000 |
| Sedentary time (min/day) | 178.20 ± 176.10 | 404.32 ± 173.01 | 271.77 ± 212.07 | 153.74 ± 151.86 | 86.48 ± 57.39 | 0.000 |
| Waist circumference (cm) | 94.80 ± 13.63 | 105.88 ± 12.84 | 99.35 ± 13.88 | 94.76 ± 13.35 | 88.76 ± 10.73 | 0.000 |
| Waist-to-height ratio | 0.60 ± 0.09 | 0.65 ± 0.09 | 0.62 ± 0.09 | 0.59 ± 0.08 | 0.55 ± 0.07 | 0.000 |
| Tobacco (n/%) | 0.387 | |||||
| ≥1/day | 1085/23.2 | 70/24.1 | 258/22.6 | 417/22.5 | 340/24.5 | |
| Occasionally, < 1/day | 326/7.0 | 20/6.9 | 72/6.3 | 119/6.4 | 115/8.3 | |
| No, I quitted | 1148/24.6 | 73/25.1 | 285/25 | 454/24.5 | 336/24.2 | |
| I have never smoked | 2112/45.2 | 128/44 | 525/46.1 | 864/46.6 | 595/42.9 | |
| Alcohol (n/%) | 0.001 | |||||
| Never | 1593/34.1 | 95/32.6 | 414/36.3 | 649/35 | 435/31.4 | |
| 1/month | 1738/37.2 | 121/41.6 | 419/36.8 | 700/37.8 | 498/35.9 | |
| 2–4/month | 984/21.0 | 55/18.9 | 233/20.4 | 380/20.5 | 316/22.8 | |
| 2–3/week | 241/5.2 | 12/4.1 | 42/3.7 | 96/5.2 | 91/6.6 | |
| >3/week | 114/2.4 | 8/2.7 | 32/2.8 | 28/1.5 | 46/3.3 | |
| Educational level (n/%) | 0.000 | |||||
| <8 years | 1064/22.8 | 66/22.7 | 271/23.8 | 432/23.3 | 295/21.3 | |
| 8–12 years | 2465/52.8 | 134/46 | 566/49.6 | 965/52 | 800/57.7 | |
| >12 years | 1104/23.7 | 90/30.9 | 300/26.3 | 434/23.4 | 280/20.2 | |
| CRF | WHtR | AIP | |
|---|---|---|---|
| CRF | - | - | - |
| WHtR | −0.722 * | - | - |
| AIP | −0.306 * | 0.297 * | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reyes-Ferrada, W.; Solis-Urra, P.; Plaza-Díaz, J.; Sadarangani, K.P.; de Moraes Ferrari, G.L.; Rodríguez-Rodríguez, F.; Cristi-Montero, C. Cardiorespiratory Fitness, Physical Activity, Sedentary Time and Its Association with the Atherogenic Index of Plasma in Chilean Adults: Influence of the Waist Circumference to Height Ratio. Nutrients 2020, 12, 1250. https://doi.org/10.3390/nu12051250
Reyes-Ferrada W, Solis-Urra P, Plaza-Díaz J, Sadarangani KP, de Moraes Ferrari GL, Rodríguez-Rodríguez F, Cristi-Montero C. Cardiorespiratory Fitness, Physical Activity, Sedentary Time and Its Association with the Atherogenic Index of Plasma in Chilean Adults: Influence of the Waist Circumference to Height Ratio. Nutrients. 2020; 12(5):1250. https://doi.org/10.3390/nu12051250
Chicago/Turabian StyleReyes-Ferrada, Waleska, Patricio Solis-Urra, Julio Plaza-Díaz, Kabir P. Sadarangani, Gerson Luis de Moraes Ferrari, Fernando Rodríguez-Rodríguez, and Carlos Cristi-Montero. 2020. "Cardiorespiratory Fitness, Physical Activity, Sedentary Time and Its Association with the Atherogenic Index of Plasma in Chilean Adults: Influence of the Waist Circumference to Height Ratio" Nutrients 12, no. 5: 1250. https://doi.org/10.3390/nu12051250