A Diet Rich in Saturated Fat and Cholesterol Aggravates the Effect of Bacterial Lipopolysaccharide on Alveolar Bone Loss in a Rabbit Model of Periodontal Disease

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Experimental Design
2.3. Blood Biochemistry
2.4. Histopathological Analyses
2.5. Alveolar Bone Morphometric Analysis
2.6. Statistical Analysis
3. Results
3.1. Blood Biochemistry
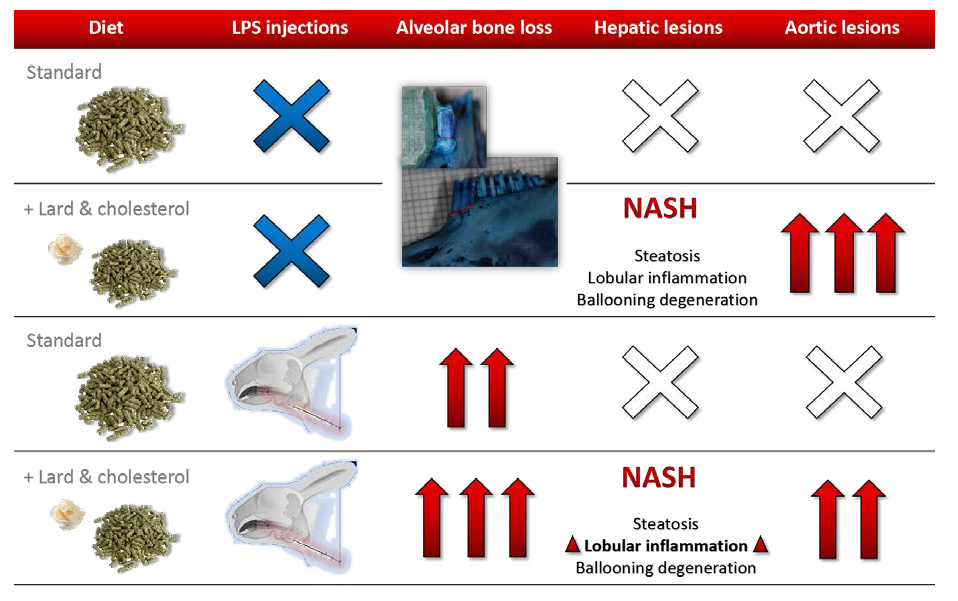
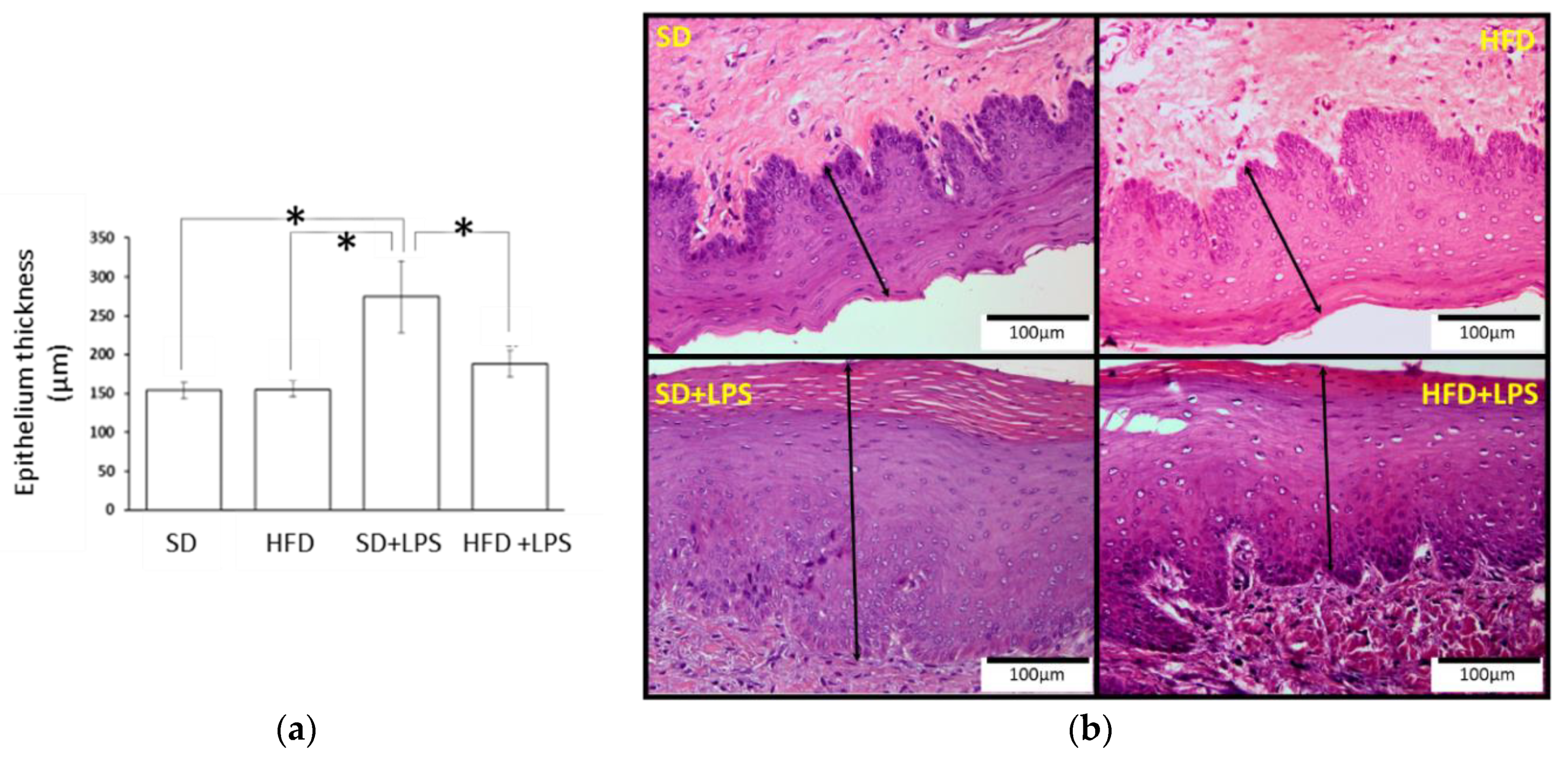
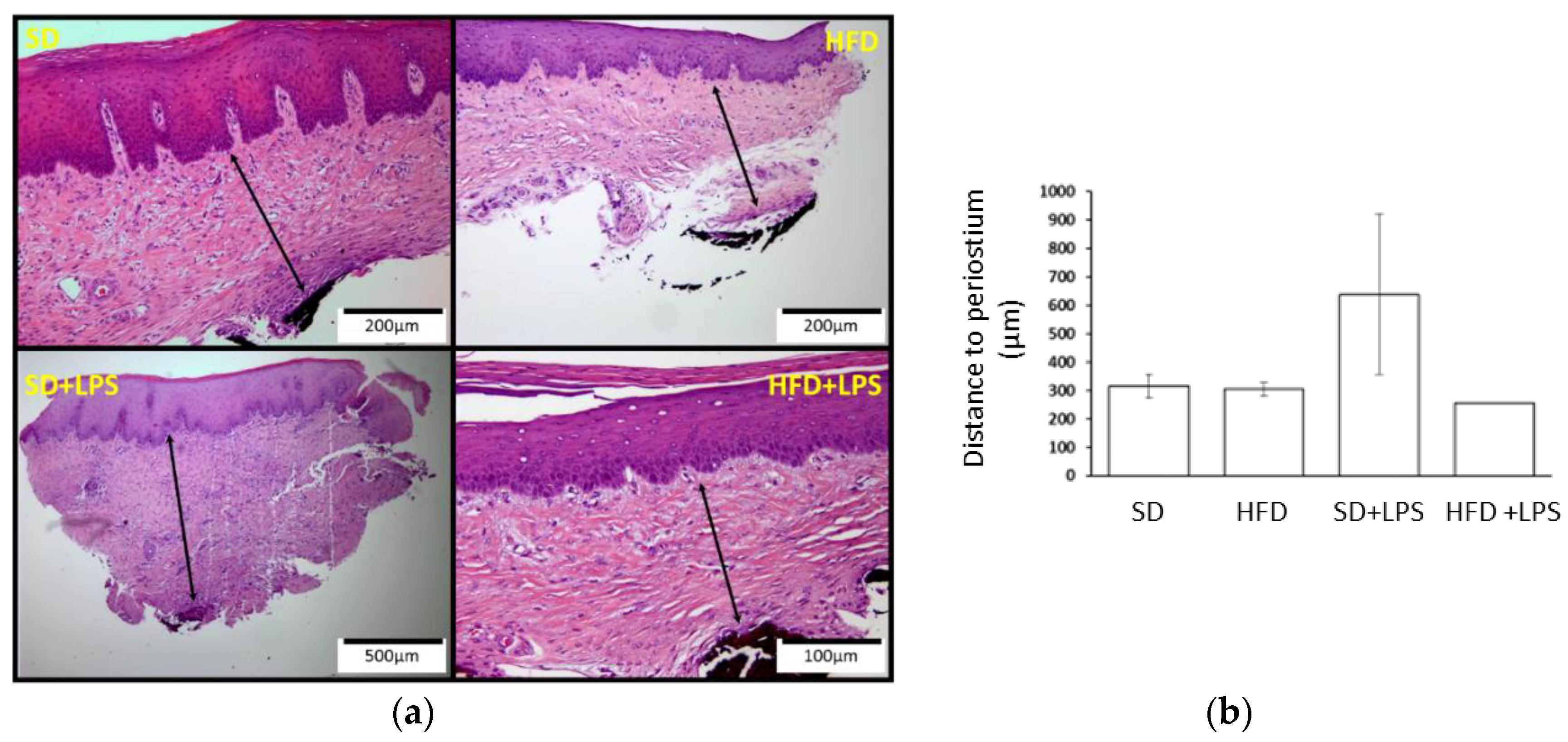
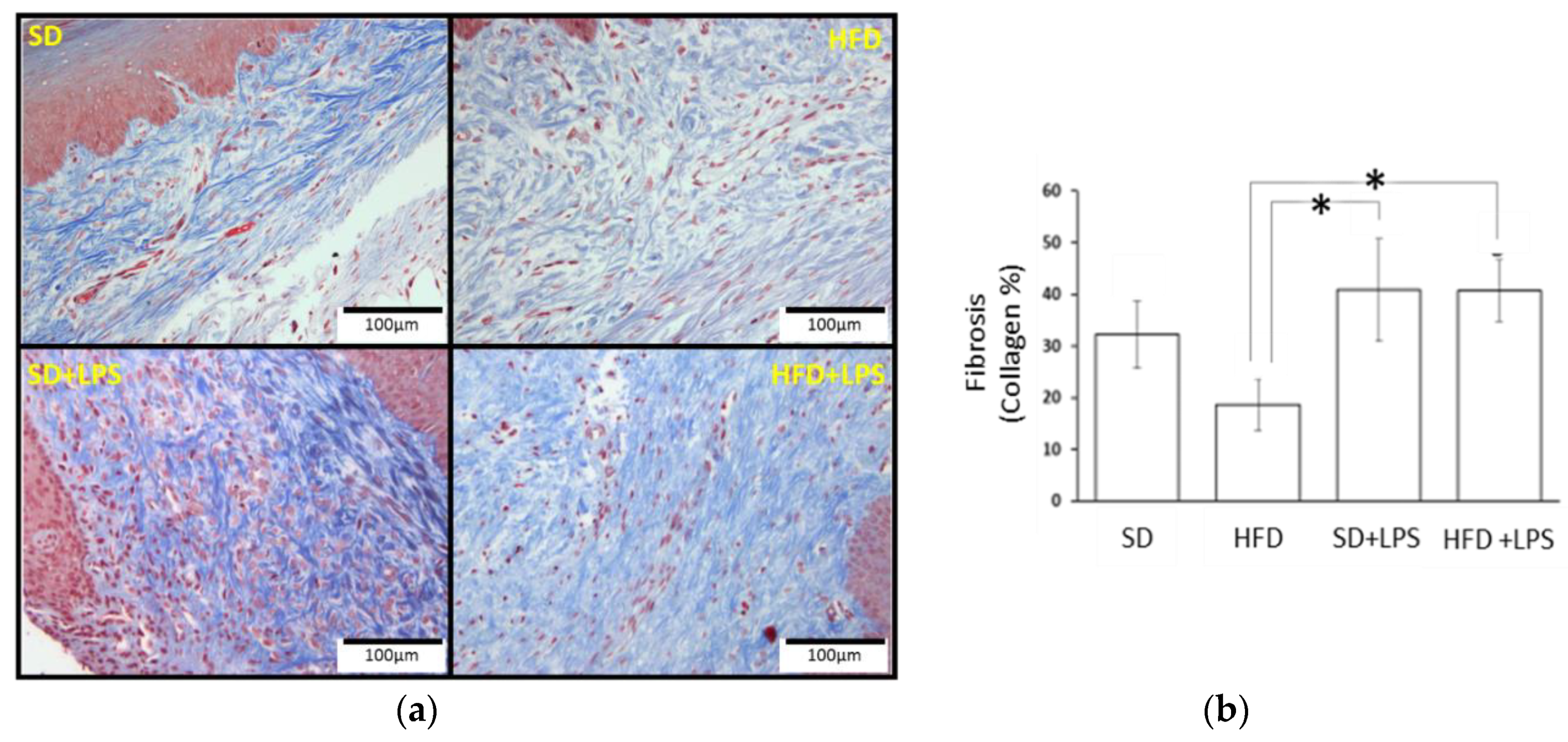
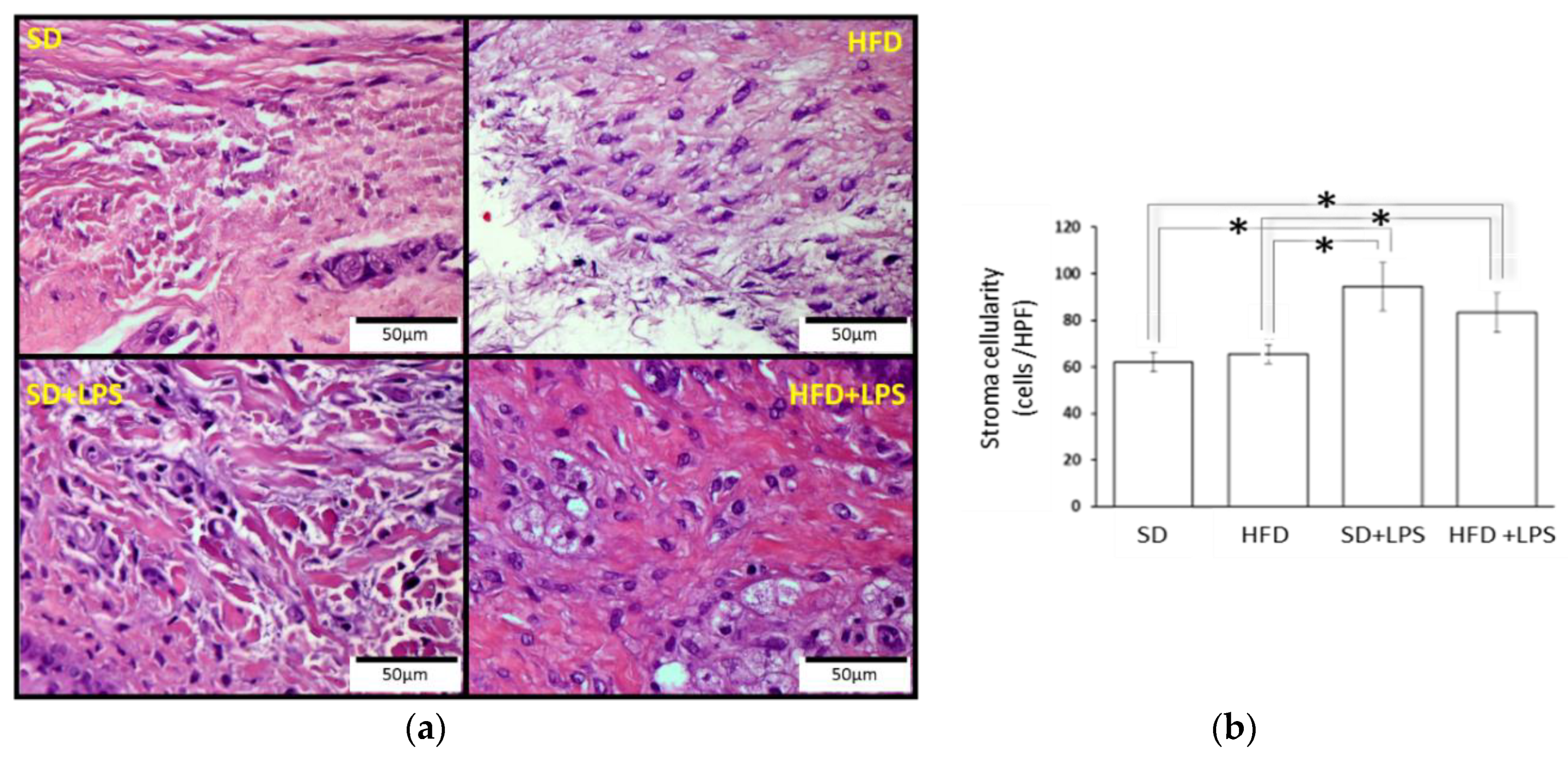
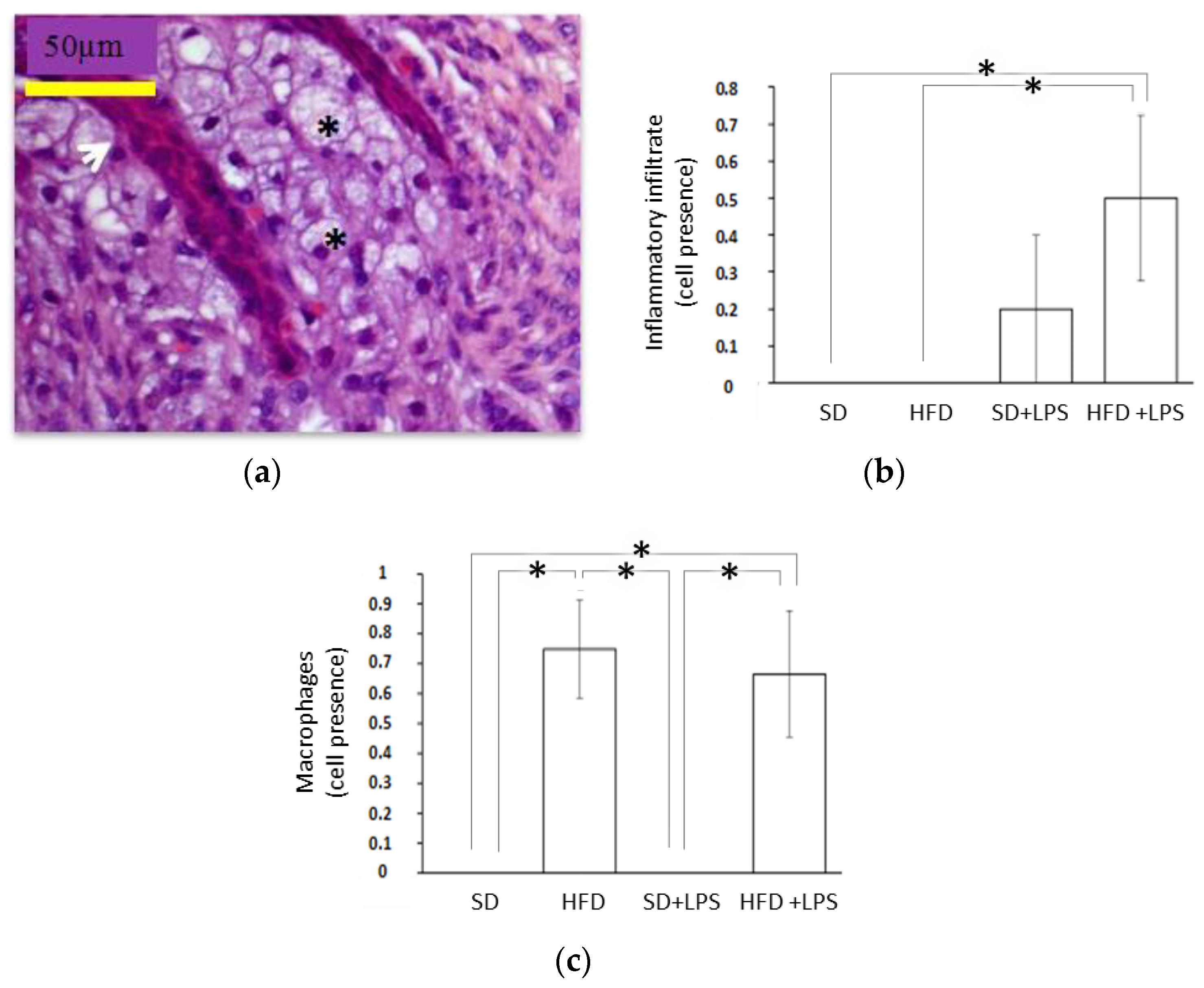
3.2. Histopathological Findings
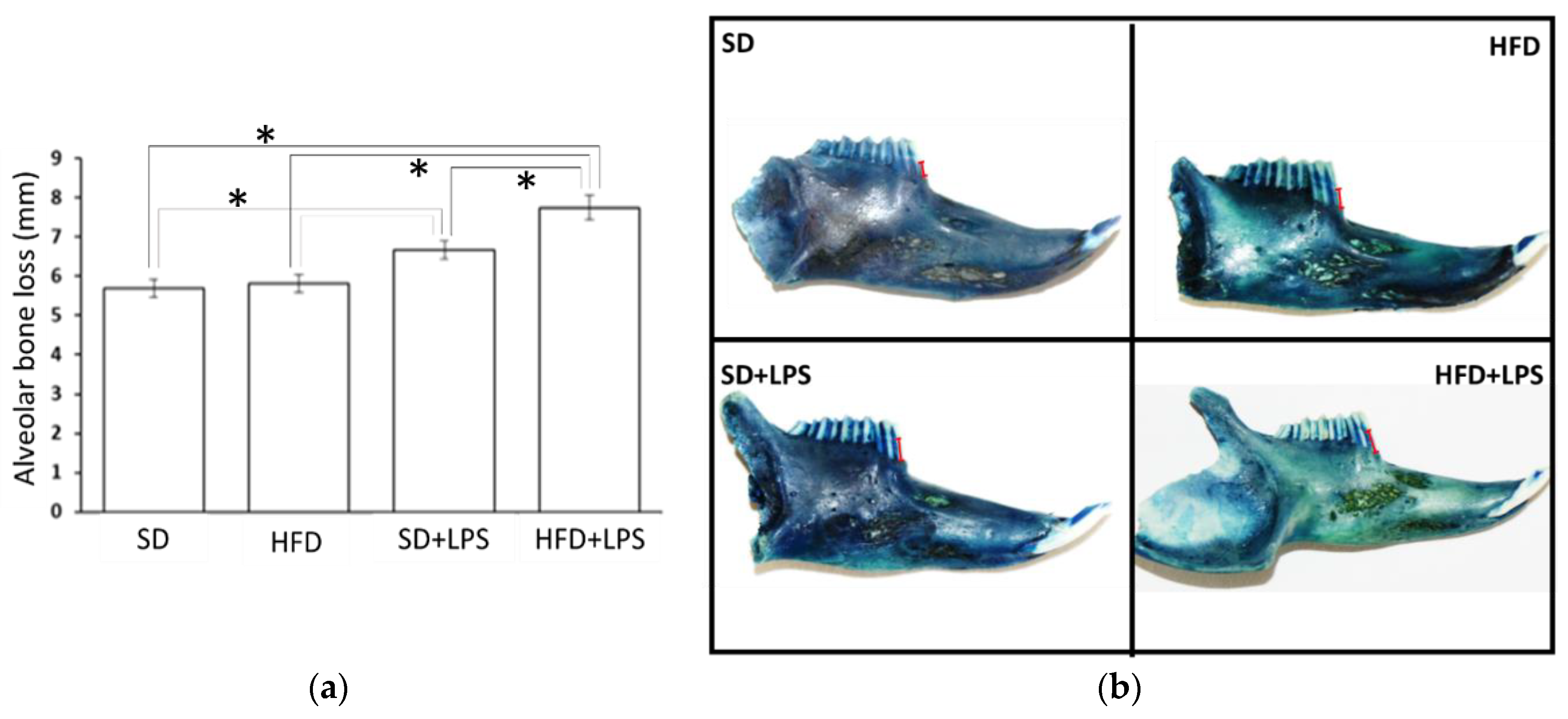
3.3. Alveolar Bone Loss
4. Discussion
5. Limitations and Perspective
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Savage, A.; Eaton, K.A.; Moles, D.; Needleman, I. A systematic review of definitions of periodontitis and methods that have been used to identify this disease. J. Clin. Periodontol. 2009, 36, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol. 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannopoulou, C.; Krause, K.-H.; Müller, F. The NADPH oxidase NOX2 plays a role in periodontal pathologies. Semin. Immunopathol. 2008, 30, 273–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, N.; Elner, S.G.; Bian, Z.-M.; Till, G.O.; Petty, H.R.; Elner, S.G. Pro-inflammatory cytokines increase reactive oxygen species through mitochondria and NADPH oxidase in cultured RPE cells. Exp. Eye Res. 2007, 85, 462–472. [Google Scholar] [CrossRef] [Green Version]
- Pourová, J.; Kottova, M.; Vopršalová, M.; Pour, M. Reactive oxygen and nitrogen species in normal physiological processes. Acta Physiol. 2010, 198, 15–35. [Google Scholar] [CrossRef]
- Liu, C.; Mo, L.; Niu, Y.; Li, X.; Zhou, X.; Xu, X. The Role of Reactive Oxygen Species and Autophagy in Periodontitis and Their Potential Linkage. Front. Physiol. 2017, 8, 439. [Google Scholar] [CrossRef]
- Martinon, F. Signaling by ROS drives inflammasome activation. Eur. J. Immunol. 2010, 40, 616–619. [Google Scholar] [CrossRef]
- Kurita-Ochiai, T.; Jia, R.; Cai, Y.; Yamaguchi, Y.; Yamamoto, M. Periodontal Disease-Induced Atherosclerosis and Oxidative Stress. Antioxidants 2015, 4, 577–590. [Google Scholar] [CrossRef] [Green Version]
- Katsuragi, H.; Ohtake, M.; Kurasawa, I.; Saito, K. Intracellular production and extracellular release of oxygen radicals by PMNs and oxidative stress on PMNs during phagocytosis of periodontopathic bacteria. Odontology 2003, 91, 13–18. [Google Scholar] [CrossRef]
- Sculley, D.V.; Langley-Evans, S.C. Salivary antioxidants and periodontal disease status. Proc. Nutr. Soc. 2002, 61, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Highfield, J. Diagnosis and classification of periodontal disease. Aust. Dent. J. 2009, 54, S11–S26. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.H.; Hwang, H.-J.; Kim, S.-H.; Kim, T.H. Associations Between Periodontitis and Chronic Obstructive Pulmonary Disease: The 2010 to 2012 Korean National Health and Nutrition Examination Survey. J. Periodontol. 2016, 87, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Spanemberg, J.C.; Cardoso, J.A.; Slob, E.; López-López, J. Quality of life related to oral health and its impact in adults. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Gil-Montoya, J.A.; De Mello, A.L.F.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral health in the elderly patient and its impact on general well-being: A nonsystematic review. Clin. Interv. Aging 2015, 10, 461–467. [Google Scholar] [CrossRef] [Green Version]
- Kuo, L.-C.; Polson, A.M.; Kang, T. Associations between periodontal diseases and systemic diseases: A review of the inter-relationships and interactions with diabetes, respiratory diseases, cardiovascular diseases and osteoporosis. Public Health 2008, 122, 417–433. [Google Scholar] [CrossRef]
- Alakhali, M.S.; Al-Maweri, S.; Al-Shamiri, H.M.; Al-Haddad, K.; Halboub, E. The potential association between periodontitis and non-alcoholic fatty liver disease: A systematic review. Clin. Oral Investig. 2018, 22, 2965–2974. [Google Scholar] [CrossRef]
- Björnsson, E.; Angulo, P. Non-alcoholic fatty liver disease. Scand. J. Gastroenterol. 2007, 42, 1023–1030. [Google Scholar] [CrossRef]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2017, 15, 11–20. [Google Scholar] [CrossRef]
- Ma, J.; Hwang, S.-J.; Pedley, A.; Massaro, J.M.; Hoffmann, U.; Chung, R.T.; Benjamin, E.J.; Levy, D.; Fox, C.S.; Long, M.T. Bi-directional analysis between fatty liver and cardiovascular disease risk factors. J. Hepatol. 2016, 66, 390–397. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Day, C.P.; Bonora, E. Risk of Cardiovascular Disease in Patients with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.; Johnson, C.; Abajobir, A.A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, C.; Schulze, M.B.; Franco, O.H.; Van Dam, R.M.; Mantzoros, C.S.; Hu, F.B. Dietary patterns and risk of mortality from cardiovascular disease, cancer, and all causes in a prospective cohort of women. Circulation 2008, 118, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Nseir, W.; Hellou, E.; Assy, N. Role of diet and lifestyle changes in nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 9338–9344. [Google Scholar] [PubMed]
- Asgari-Taee, F.; Zerafati-Shoae, N.; Dehghani, M.; Sadeghi, M.; Baradaran, H.; Jazayeri, S. Association of sugar sweetened beverages consumption with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Nutr. 2018, 58, 1759–1769. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Manson, J.E.; Willett, W.C.; Hu, F.B. Changes in red meat consumption and subsequent risk of type 2 diabetes mellitus: Three cohorts of US men and women. JAMA Intern. Med. 2013, 173, 1328–1335. [Google Scholar] [CrossRef]
- Varela-Lopez, A.; Quiles, J.L.; Cordero, M.; Giampieri, F.; Bullón, P. Oxidative Stress and Dietary Fat Type in Relation to Periodontal Disease. Antioxidants 2015, 4, 322–344. [Google Scholar] [CrossRef] [Green Version]
- Varela-Lopez, A.; Giampieri, F.; Bullón, P.; Battino, M.; Quiles, J.L. Role of Lipids in the Onset, Progression and Treatment of Periodontal Disease. A Systematic Review of Studies in Humans. Int. J. Mol. Sci. 2016, 17, 1202. [Google Scholar] [CrossRef] [Green Version]
- Abraham, S.; Premnath, A.; Arunima, P.R.; Kassim, R.M. Critical Appraisal of Bidirectional Relationship between Periodontitis and Hyperlipidemia. J. Int. Soc. Prev. Community Dent. 2019, 9, 112–118. [Google Scholar] [CrossRef]
- Scannapieco, F.A. Position paper of The American Academy of Periodontology: Periodontal disease as a potential risk factor for systemic diseases. J. Periodontol. 1998, 69, 841–850. [Google Scholar]
- Tsai, C.C.; Chen, H.S.; Chen, S.L.; Ho, Y.P.; Ho, K.Y.; Wu, Y.M.; Hung, C.C. Lipid peroxidation: A possible role in the induction and progression of chronic periodontitis. J. Periodontal Res. 2005, 40, 378–384. [Google Scholar] [CrossRef]
- Akalιn, F.A.; Baltacιoğlu, E.; Alver, A.; Karabulut, E. Lipid peroxidation levels and total oxidant status in serum, saliva and gingival crevicular fluid in patients with chronic periodontitis. J. Clin. Periodontol. 2007, 34, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Bartova, J.; Sommerova, P.; Lyuya-Mi, Y.; Myšák, J.; Prochazkova, J.; Duškova, J.; Janatova, T.; Podzimek, S. Periodontitis as a Risk Factor of Atherosclerosis. J. Immunol. Res. 2014, 2014, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, P.; Sun, D.-X.; Yang, J. Interaction between periodontitis and liver diseases. Biomed. Rep. 2016, 5, 267–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oz, H.S.; Puleo, D.A. Animal Models for Periodontal Disease. Available online: https://www.hindawi.com/journals/bmri/2011/754857/ (accessed on 23 December 2019).
- Graves, D.T.; Kang, J.; Andriankaja, O.; Wada, K.; Rossa, C. Animal models to study host-bacteria interactions involved in periodontitis. Front. Oral Boil. 2011, 15, 117–132. [Google Scholar] [CrossRef] [Green Version]
- Fan, J.; Kitajima, S.; Watanabe, T.; Xu, J.; Zhang, J.; Liu, E.; Chen, Y.E. Rabbit models for the study of human atherosclerosis: From pathophysiological mechanisms to translational medicine. Pharmacol. Ther. 2014, 146, 104–119. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, T.; Fujii, H.; Yoshizato, K.; Kawada, N. A Human-Type Nonalcoholic Steatohepatitis Model with Advanced Fibrosis in Rabbits. Am. J. Pathol. 2010, 177, 153–165. [Google Scholar] [CrossRef]
- Sanches, S.C.L.; Ramalho, L.N.; Augusto, M.J.; Da Silva, D.M.; Ramalho, L.N. Nonalcoholic Steatohepatitis: A Search for Factual Animal Models. BioMed Res. Int. 2015, 2015, 1–13. [Google Scholar] [CrossRef]
- Ramirez-Tortosa, M.C.; Ramirez-Tortosa, C.L.; Mesa, M.D.; Granados, S.; Gil, Á.; Quiles, J.L. Curcumin ameliorates rabbits’s steatohepatitis via respiratory chain, oxidative stress, and TNF-α. Free Radic. Biol. Med. 2009, 47, 924–931. [Google Scholar] [CrossRef]
- Quiles, J.L.; Mesa, M.-D.; Ramírez-Tortosa, C.; Aguilera, C.M.; Battino, M.; Gil, A.; Ramírez-Tortosa, M.C. Curcuma longa Extract Supplementation Reduces Oxidative Stress and Attenuates Aortic Fatty Streak Development in Rabbits. Arter. Thromb. Vasc. Boil. 2002, 22, 1225–1231. [Google Scholar] [CrossRef] [Green Version]
- Varela-Lopez, A.; Pérez-López, M.P.; Ramirez-Tortosa, C.L.; Battino, M.; Granados-Principal, S.; Ramirez-Tortosa, M.D.C.; Ochoa, J.J.; Vera-Ramirez, L.; Giampieri, F.; Quiles, J.L. Gene pathways associated with mitochondrial function, oxidative stress and telomere length are differentially expressed in the liver of rats fed lifelong on virgin olive, sunflower or fish oils. J. Nutr. Biochem. 2018, 52, 36–44. [Google Scholar] [CrossRef]
- Ramı́rez-Tortosa, M.; Mesa, M.-D.; Aguilera, C.M.; Quiles, J.L.; Baró, L.; Ramírez-Tortosa, C.; Martinez-Victoria, E.; Gil, A. Oral administration of a turmeric extract inhibits LDL oxidation and has hypocholesterolemic effects in rabbits with experimental atherosclerosis. Atherosclerosis 1999, 147, 371–378. [Google Scholar] [CrossRef]
- Yeh, M.M.; Brunt, E.M. Pathology of Nonalcoholic Fatty Liver Disease. Am. J. Clin. Pathol. 2007, 128, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Bullón, P.; Quiles, J.L.; Morillo, J.M.; Rubini, C.; Goteri, G.; Granados-Principal, S.; Battino, M.; Ramirez-Tortosa, M. Gingival vascular damage in atherosclerotic rabbits: Hydroxytyrosol and squalene benefits. Food Chem. Toxicol. 2009, 47, 2327–2331. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.D.S.; Vasconcelos, A.C.C.G.; Alves, E.H.P.; Da Silva, F.R.P.; França, L.F.D.C.; Neto, A.D.P.R.N.; Di Lenardo, D.; De Souza, L.K.M.; Barbosa, A.L.D.R.; Medeiros, J.V.R.; et al. Steatosis caused by experimental periodontitis is reversible after removal of ligature in rats. J. Periodontal Res. 2017, 52, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.E.; Li, F.; Coatney, D.D.; Rossa, C.; Bronson, P.; Krieder, J.M.; Giannobile, W.V.; Kirkwood, K.L. Actinobacillus actinomycetemcomitansLipopolysaccharide-Mediated Experimental Bone Loss Model for Aggressive Periodontitis. J. Periodontol. 2007, 78, 550–558. [Google Scholar] [CrossRef] [Green Version]
- De Aquino, S.G.; Leite, F.R.; Stach-Machado, D.R.; Da Silva, J.A.F.; Spolidorio, L.C.; Rossa, C. Signaling pathways associated with the expression of inflammatory mediators activated during the course of two models of experimental periodontitis. Life Sci. 2009, 84, 745–754. [Google Scholar] [CrossRef]
- Jain, A.; Batista, E.L.; Serhan, C.; Stahl, G.L.; Van Dyke, T.E. Role for Periodontitis in the Progression of Lipid Deposition in an Animal Model. Infect. Immun. 2003, 71, 6012–6018. [Google Scholar] [CrossRef] [Green Version]
- Hasturk, H.; Kantarci, A.; Goguet, E.; Blackwood, A.; Andry, C.; Serhan, C.N.; Van Dyke, T.E. Resolvin E1 regulates inflammation at the cellular and tissue level and restores tissue homeostasis in vivo. J. Immunol. 2007, 179, 7021–7029. [Google Scholar] [CrossRef] [Green Version]
- Hasturk, H.; Kantarci, A.; Ohira, T.; Arita, M.; Ebrahimi, N.; Chiang, N.; Petasis, N.A.; Levy, B.D.; Serhan, C.N.; Van Dyke, T.E. RvE1 protects from local inflammation and osteoclast-mediated bone destruction in periodontitis. FASEB J. 2006, 20, 401–403. [Google Scholar] [CrossRef]
- Chen, S.; Lin, G.; You, X.; Lei, L.; Li, Y.; Lin, M.; Luo, K.; Yan, F. Hyperlipidemia causes changes in inflammatory responses to periodontal pathogen challenge: Implications in acute and chronic infections. Arch. Oral Boil. 2014, 59, 1075–1084. [Google Scholar] [CrossRef]
- Tomofuji, T.; Kusano, H.; Azuma, T.; Ekuni, D.; Yamamoto, T.; Watanabe, T. Effects of a high-cholesterol diet on cell behavior in rat periodontitis. J. Dent. Res. 2005, 84, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Macri, E.V.; Lifshitz, F.; Ramos, C.; Orzuza, R.; Costa, O.; Zago, V.; Boyer, P.; Friedman, S. Atherogenic cholesterol-rich diet and periodontal disease. Arch. Oral Boil. 2014, 59, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Kuraji, R.; Ito, H.; Fujita, M.; Ishiguro, H.; Hashimoto, S.; Numabe, Y. Porphyromonas gingivalis induced periodontitis exacerbates progression of non-alcoholic steatohepatitis in rats. Clin. Exp. Dent. Res. 2016, 2, 216–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, G.; Shi, X.; Chen, S.; Lei, L.; You, X.; Huang, M.; Luo, L.; Li, Y.; Zhao, X.; Yan, F. Effects of micro-amounts ofPorphyromonas gingivalislipopolysaccharide on rabbit inflammatory immune response and development of atherosclerosis. J. Periodontal Res. 2014, 50, 356–362. [Google Scholar] [CrossRef]
- Li, Y.; Lu, Z.; Zhang, X.; Yu, H.; Kirkwood, K.; Lopes-Virella, M.; Huang, Y. Metabolic syndrome exacerbates inflammation and bone loss in periodontitis. J. Dent. Res. 2014, 94, 362–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Z.; Li, Y.; Brinson, C.W.; Kirkwood, K.L.; Lopes-Virella, M.F.; Huang, Y. CD36 is upregulated in mice with periodontitis and metabolic syndrome and involved in macrophage gene upregulation by palmitate. Oral Dis. 2017, 23, 210–218. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Cybulsky, M.I.; Gimbrone, M.A.; Libby, P. Inducible expression of vascular cell adhesion molecule-1 by vascular smooth muscle cells in vitro and within rabbit atheroma. Am. J. Pathol. 1993, 143, 1551–1559. [Google Scholar]
- Lopes-Virella, M.F. Interactions between bacterial lipopolysaccharides and serum lipoproteins and their possible role in coronary heart disease. Eur. Heart J. 1993, 14 (Suppl. K), 118–124. [Google Scholar]
- Prabhu, A.; Michalowicz, B.S.; Mathur, A. Detection of Local and Systemic Cytokines in Adult Periodontitis. J. Periodontol. 1996, 67, 515–522. [Google Scholar] [CrossRef]
- Tanaka, H.; Nakai, K.; Murakami, F.; Morita, T.; Yamazaki, Y.; Matsuike, R.; Shibata, C.; Nagasaki, M.; Kanda, M.; Tanabe, N.; et al. Ligature-Induced Periodontitis Increased Insulin Resistance and Triglyceride Levels in Wistar Rats. J. Hard Tissue Boil. 2017, 26, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Vasconcelos, A.C.C.G.; Vasconcelos, D.F.P.; Da Silva, F.R.P.; França, L.F.D.C.; Alves, E.H.P.; Di Lenardo, D.; Pessoa, L.D.S.; Novaes, P.D.; Barbosa, A.L.D.R.; Mani, A.; et al. Periodontitis causes abnormalities in the liver of rats. J. Periodontol. 2018, 90, 295–305. [Google Scholar] [CrossRef] [PubMed]
- De Andrade, R.S.B.; França, L.F.D.C.; Pessoa, L.D.S.; Landim, B.D.A.A.; Rodrigues, A.A.; Alves, E.H.P.; Di Lenardo, D.; Nascimento, H.M.S.; Sousa, F.B.D.M.; Barbosa, A.L.D.R.; et al. High-fat diet aggravates the liver disease caused by periodontitis in rats. J. Periodontol. 2019, 90, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Cappelli, D.; Mott, G.; Kesavalu, L.; Holt, S.C.; Singer, R.E. Systemic manifestations of periodontitis in the non-human primate. J. Periodontal Res. 1999, 34, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Trevisan, M.; Genco, R.J.; Falkner, K.L.; Dorn, J.P.; Sempos, C.T. Examination of the relation between periodontal health status and cardiovascular risk factors: Serum total and high density lipoprotein cholesterol, C-reactive protein, and plasma fibrinogen. Am. J. Epidemiol. 2000, 151, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Katz, J.; Chaushu, G.; Sharabi, Y. On the association between hypercholesterolemia, cardiovascular disease and severe periodontal disease. J. Clin. Periodontol. 2001, 28, 865–868. [Google Scholar] [CrossRef]
- Katz, J.; Flugelman, M.Y.; Goldberg, A.; Heft, M. Association Between Periodontal Pockets and Elevated Cholesterol and Low Density Lipoprotein Cholesterol Levels. J. Periodontol. 2002, 73, 494–500. [Google Scholar] [CrossRef]
- Cutler, C.W.; Shinedling, E.A.; Nunn, M.; Jotwani, R.; Kim, B.-O.; Nares, S.; Iacopino, A. Association Between Periodontitis and Hyperlipidemia: Cause or Effect? J. Periodontol. 1999, 70, 1429–1434. [Google Scholar] [CrossRef]
- Morita, M.; Horiuchi, M.; Kinoshita, Y.; Yamamoto, T.; Watanabe, T. Relationship between blood triglyceride levels and periodontal status. Community Dent Health 2004, 21, 32–36. [Google Scholar]
- Maekawa, T.; Takahashi, N.; Tabeta, K.; Aoki, Y.; Miyashita, H.; Miyauchi, S.; Miyazawa, H.; Nakajima, T.; Yamazaki, K. Chronic Oral Infection with Porphyromonas gingivalis Accelerates Atheroma Formation by Shifting the Lipid Profile. PLoS ONE 2011, 6, e20240. [Google Scholar] [CrossRef] [Green Version]
- Ekuni, D.; Tomofuji, T.; Sanbe, T.; Irie, K.; Azuma, T.; Maruyama, T.; Tamaki, N.; Murakami, J.; Kokeguchi, S.; Yamamoto, T. Periodontitis-induced lipid peroxidation in rat descending aorta is involved in the initiation of atherosclerosis. J. Periodontal Res. 2009, 44, 434–442. [Google Scholar] [CrossRef]
- Lalla, E.; Lamster Ira, B.; Hofmann Marion, A.; Bucciarelli, L.; Jerud Adrienne, P.; Tucker, S.; Lu, Y.; Papapanou Panos, N. Schmidt Ann Marie Oral Infection with a Periodontal Pathogen Accelerates Early Atherosclerosis in Apolipoprotein E–Null Mice. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1405–1411. [Google Scholar] [CrossRef]
- Kolovou, G.; Anagnostopoulou, K.; Mikhailidis, D.P.; Cokkinos, D.V. Apolipoprotein E knockout models. Curr. Pharm. Des. 2008, 14, 338–351. [Google Scholar] [CrossRef]
- Nordestgaard, B.G.; Zilversmit, D.B. Hyperglycemia in normotriglyceridemic, hypercholesterolemic insulin-treated diabetic rabbits does not accelerate atherogenesis. Atherosclerosis 1988, 72, 37–47. [Google Scholar] [CrossRef]
- Nordestgaard, B.G.; Zilversmit, D.B. Large lipoproteins are excluded from the arterial wall in diabetic cholesterol-fed rabbits. J. Lipid Res. 1988, 29, 1491–1500. [Google Scholar]
- Tomofuji, T.; Ekuni, D.; Yamanaka, R.; Kusano, H.; Azuma, T.; Sanbe, T.; Tamaki, N.; Yamamoto, T.; Watanabe, T.; Miyauchi, M.; et al. Chronic Administration of Lipopolysaccharide and Proteases Induces Periodontal Inflammation and Hepatic Steatosis in Rats. J. Periodontol. 2007, 78, 1999–2006. [Google Scholar] [CrossRef]
- Tomofuji, T.; Ekuni, D.; Sanbe, T.; Azuma, T.; Tamaki, N.; Irie, K.; Maruyama, T.; Yamamoto, T.; Watanabe, T.; Miyauchi, M.; et al. Effects of improvement in periodontal inflammation by toothbrushing on serum lipopolysaccharide concentration and liver injury in rats. Acta Odontol. Scand. 2009, 67, 200–205. [Google Scholar] [CrossRef]
- Fujita, M.; Kuraji, R.; Ito, H.; Hashimoto, S.; Toen, T.; Fukada, T.; Numabe, Y. Histological effects and pharmacokinetics of lipopolysaccharide derived from Porphyromonas gingivalis on rat maxilla and liver concerning with progression into non-alcoholic steatohepatitis. J. Periodontol. 2018, 89, 1101–1111. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Marker | SD | HFD | SD + LPS | HFD + LPS |
|---|---|---|---|---|
| Glucose (mg/dL) | 158.3 ± 21.0 a | 348.0 ± 28.3 b | 129.1 ± 20.5 a | 424.9 ± 41.3 b |
| Triglycerides (mg/dL) | 89.9 ± 15.7 a | 386.2 ± 51.0 b | 55.0 ± 9.9 a | 845.0 ± 254.2 c |
| Phospholipids (mg/dL) | 63.1 ± 4.6 a | 586.2 ± 82.6 b | 57.5 ± 3.6 a | 915.9 ± 254.2 c |
| LDL-cholesterol (mg/dL) | 1.3 ± 0.3 a | 113.7 ± 5.2 b | 2.7 ± 0.6 a | 139.7 ± 14.3 b |
| HDL-cholesterol (mg/dL) | 16.6 ± 1.3 a | 138.7 ± 5.2 b | 14.5 ± 2.2 a | 187.4 ± 34.5 b |
| Total cholesterol (mg/dL) | 89.9 ± 15.7 a | 386.2 ± 51.0 b | 55.0 ± 9.9 a | 845.0 ± 254.2 b |
| LDH (U/L) | 334.3 ± 36.0 | 303.0 ± 61.6 | 379.1 ± 100.6 | 208.9 ± 59.6 |
| GGT (U/L) | 9.0 ± 0.2 a | 17.1 ± 6.0 a | 7.8 ± 1.2 a | 57.7 ± 17.6 b |
| ALT (U/L) | 28.5 ± 8.2 | 56.5 ± 21.7 | 28.8 ± 4.9 | 25.8 ± 10.2 |
| AST (U/L) | 42.4 ± 8.3 | 53.7 ± 11.4 | 49.3 ± 15.7 | 66.1 ± 16.9 |
| Total bilirubin (mg/dL) | 2.8 ± 1.1 a,b | 5.5 ± 1.1 b | 1.6 ± 0.2 a | 10.6 ± 2.4 c |
| Direct bilirubin (mg/dL) | 0.6 ± 0.0 a | 3.2 ± 0.6 b | 0.4 ± 0.0 a | 3.7 ± 0.8 b |
| Creatinine (mg/dL) | 1.2 ± 0.1 a | 2.7 ± 0.2 b | 1.5 ± 0.1 a | 2.4 ± 0.7 a,b |
| Uric acid (mg/dL) | 1.3 ± 0.7 a | 34.0 ± 6.5 b | 0.7 ± 0.2 a | 65.4 ± 15.4 c |
| Urea (mg/dL) | 15.9 ± 1.1 a | 11.0 ± 8.2 a,b | 17.8 ± 2.5 a,b | 22.8 ± 2.4 b |
| SD | HFD | SD + LPS | HFD + LPS | |
|---|---|---|---|---|
| Aortic lesions | ||||
| Aortic arch (AU) | 0.00 ± 0.00 a | 2.38 ± 0.32 c | 0.00 ± 0.00 a | 1.50 ± 0.22 b |
| Thoracic aorta (AU) | 0.00 ± 0.00 a | 1.00 ± 0.19 c | 0.00 ± 0.00 a | 0.33 ± 0.21 b |
| Abdominal aorta (AU) | 0.00 ± 0.00 a | 0.25 ± 0.16 b | 0.00 ± 0.00 a | 0.43 ± 0.22 b |
| Hepatic Lesions | ||||
| Steatosis (hepatocytes %) | 0.5 ± 0.5 a | 65.25 ± 7.09 b | 2.25 ± 1.48 a | 73.57 ± 19.11 b |
| Lobular inflammation (inflammatory foci/20 HPF) | 0.38 ± 0.26 a | 1.5 ± 0.54 b | 0.63 ± 0.63 a | 3 ± 0.57 c |
| Ballooning degeneration (AU) | 0.75 ± 0.31 a,b | 1.63 ± 0.18 b | 0 ± 0 a | 1.4 ± 0.29 b |
| NASH score (AU) | 1 ± 0.42 a | 5.125 ± 0.52 b | 0.63 ± 0.38 a | 5.86 ± 0.67 b |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varela-López, A.; Bullón, P.; Ramírez-Tortosa, C.L.; Navarro-Hortal, M.D.; Robles-Almazán, M.; Bullón, B.; Cordero, M.D.; Battino, M.; Quiles, J.L. A Diet Rich in Saturated Fat and Cholesterol Aggravates the Effect of Bacterial Lipopolysaccharide on Alveolar Bone Loss in a Rabbit Model of Periodontal Disease. Nutrients 2020, 12, 1405. https://doi.org/10.3390/nu12051405
Varela-López A, Bullón P, Ramírez-Tortosa CL, Navarro-Hortal MD, Robles-Almazán M, Bullón B, Cordero MD, Battino M, Quiles JL. A Diet Rich in Saturated Fat and Cholesterol Aggravates the Effect of Bacterial Lipopolysaccharide on Alveolar Bone Loss in a Rabbit Model of Periodontal Disease. Nutrients. 2020; 12(5):1405. https://doi.org/10.3390/nu12051405
Chicago/Turabian StyleVarela-López, Alfonso, Pedro Bullón, César L. Ramírez-Tortosa, María D. Navarro-Hortal, María Robles-Almazán, Beatriz Bullón, Mario D. Cordero, Maurizio Battino, and José L. Quiles. 2020. "A Diet Rich in Saturated Fat and Cholesterol Aggravates the Effect of Bacterial Lipopolysaccharide on Alveolar Bone Loss in a Rabbit Model of Periodontal Disease" Nutrients 12, no. 5: 1405. https://doi.org/10.3390/nu12051405