Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research Recommendations and Breast Cancer in the SUN Project

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
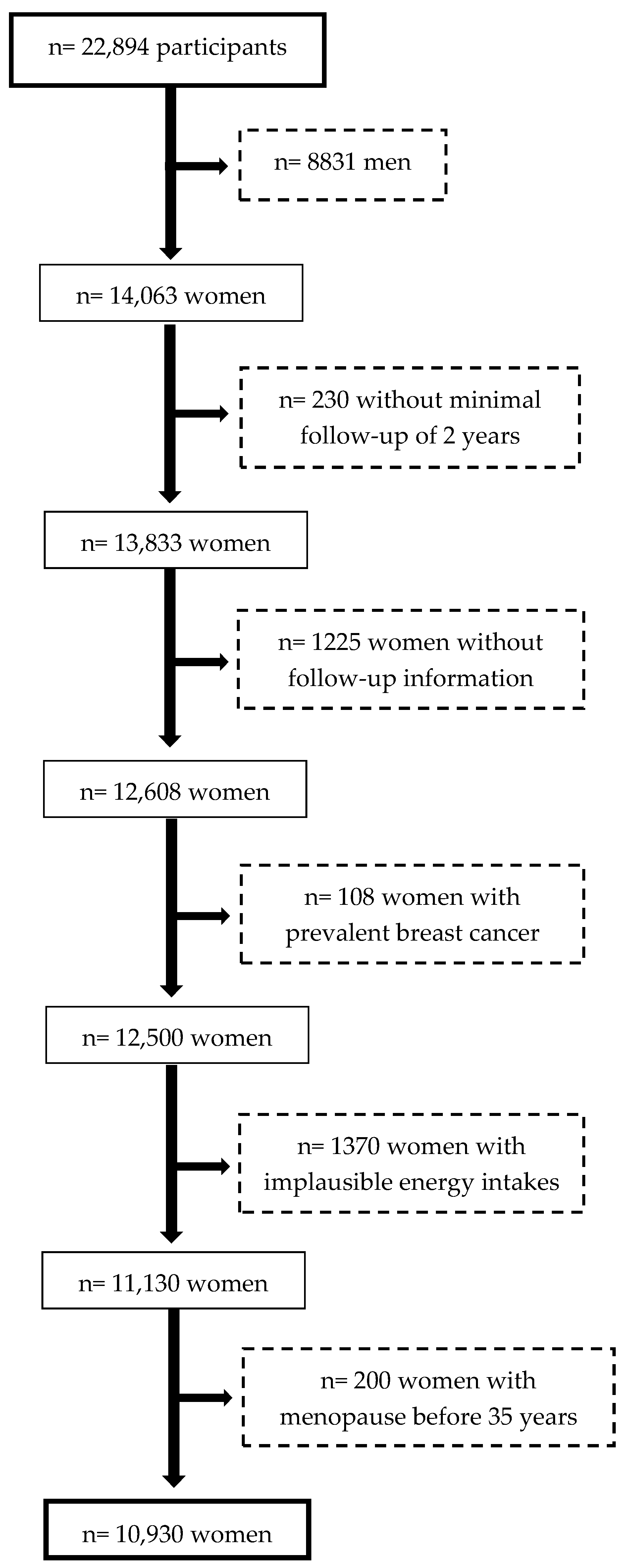
2.1. Study Design and Participants
2.2. WCRF/AICR Score Construction
2.3. Incident Breast Cancer Assessment
2.4. Covariate Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Rojas, K.; Stuckey, A. Breast Cancer Epidemiology and Risk Factors. Clin. Obstet. Gynecol. 2016, 59, 651–672. [Google Scholar] [CrossRef] [PubMed]
- Poirier, A.E.; Ruan, Y.; Volesky, K.D.; King, W.D.; O’Sullivan, D.E.; Gogna, P.; Walter, S.D.; Villeneuve, P.J.; Friedenreich, C.M.; Brenner, D.R.; et al. The current and future burden of cancer attributable to modifiable risk factors in Canada: Summary of results. Prev. Med. 2019, 122, 140–147. [Google Scholar] [CrossRef]
- Tamimi, R.M.; Spiegelman, D.; Smith-Warner, S.A.; Wang, M.; Pazaris, M.; Willett, W.C.; Eliassen, A.H.; Hunter, D.J. Population Attributable Risk of Modifiable and Nonmodifiable Breast Cancer Risk Factors in Postmenopausal Breast Cancer. Am. J. Epidemiol. 2016, 184, 884–893. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.C.; Ligibel, J.A. Lifestyle Interventions for Breast Cancer Prevention. Curr. Breast Cancer Rep. 2018, 10, 202–208. [Google Scholar] [CrossRef]
- Arthur, R.; Wassertheil-Smoller, S.; Manson, J.E.; Luo, J.; Snetselaar, L.; Hastert, T.; Caan, B.; Qi, L.; Rohan, T. The Combined Association of Modifiable Risk Factors with Breast Cancer Risk in the Women’s Health Initiative. Cancer Prev. Res. 2018, 11, 317–326. [Google Scholar] [CrossRef]
- Chan, D.S.M.; Abar, L.; Cariolou, M.; Nanu, N.; Greenwood, D.C.; Bandera, E.V.; McTiernan, A.; Norat, T. World Cancer Research Fund International: Continuous Update Project-systematic literature review and meta-analysis of observational cohort studies on physical activity, sedentary behavior, adiposity, and weight change and breast cancer risk. Cancer Causes Control 2019, 30, 1183–1200. [Google Scholar] [CrossRef] [Green Version]
- Wiseman, M. The second World Cancer Research Fund/American Institute for Cancer Research expert report. Food, nutrition, physical activity, and the prevention of cancer: A global perspective. Proc. Nutr. Soc. 2008, 67, 253–256. [Google Scholar] [CrossRef] [Green Version]
- Solans, M.; Chan, D.S.M.; Mitrou, P.; Norat, T.; Romaguera, D. A systematic review and meta-analysis of the 2007 WCRF/AICR score in relation to cancer-related health outcomes. Ann. Oncol. 2020, 31, 352–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Continuous Update Project Expert Report 2018. World Cancer Research Fund/American Institute for Cancer Research Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Available online: Dietandcancerreport.org (accessed on 10 April 2020).
- Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients 2019, 11, 1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turati, F.; Dalmartello, M.; Bravi, F.; Serraino, D.; Augustin, L.; Giacosa, A.; Negri, E.; Levi, F.; La Vecchia, C. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer. Nutrients 2020, 12, 607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karavasiloglou, N.; Hüsing, A.; Masala, G.; van Gils, C.H.; Turzanski Fortner, R.; Chang-Claude, J.; Huybrechts, I.; Weiderpass, E.; Gunter, M.; Arveux, P.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and risk of in situ breast cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. BMC Med. 2019, 17, 221. [Google Scholar] [CrossRef]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef] [Green Version]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Sánchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- De la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef]
- Bes-Rastrollo, M.; Valdivieso, J.R.P.; Sánchez-Villegas, A.; Alonso, Á.; Martínez-González, M.Á. Validación del peso e índice de masa corporal auto-declarados de los participantes de una cohorte de graduados universitarios. Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.-C.; Jaime, P.; Martins, A.P.; Canella, D.; Louzada, M.; Parra, D. NOVA. The star shines bright. World Nutr. 2016, 7, 28–38. [Google Scholar]
- Navarro, C. The National Death Index: A largely expected advance in the access to mortality data. Gac. Sanit. 2006, 20, 421–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivappa, N.; Sandin, S.; Löf, M.; Hébert, J.R.; Adami, H.-O.; Weiderpass, E. Prospective study of dietary inflammatory index and risk of breast cancer in Swedish women. Br. J. Cancer 2015, 113, 1099–1103. [Google Scholar] [CrossRef] [Green Version]
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health 2016, 16, 657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noble, N.; Paul, C.; Turon, H.; Oldmeadow, C. Which modifiable health risk behaviours are related? A systematic review of the clustering of Smoking, Nutrition, Alcohol and Physical activity (’SNAP’) health risk factors. Prev. Med. 2015, 81, 16–41. [Google Scholar] [CrossRef]
- Morimoto, Y.; Beckford, F.; Cooney, R.V.; Franke, A.A.; Maskarinec, G. Adherence to cancer prevention recommendations and antioxidant and inflammatory status in premenopausal women. Br. J. Nutr. 2015, 114, 134–143. [Google Scholar] [CrossRef]
- Tabung, F.K.; Fung, T.T.; Chavarro, J.E.; Smith-Warner, S.A.; Willett, W.C.; Giovannucci, E.L. Associations between adherence to the World Cancer Research Fund/American Institute for Cancer Research cancer prevention recommendations and biomarkers of inflammation, hormonal, and insulin response. Int. J. Cancer 2017, 140, 764–776. [Google Scholar] [CrossRef]
- Word Cancer Research Fund/American Institute for Cancer Research. How Diet, Nutrition and Physical Activity Affect Breast Cancer Risk. Available online: https://www.wcrf.org/dietandcancer/breast-cancer (accessed on 20 May 2020).
- Chen, Y.; Liu, L.; Zhou, Q.; Imam, M.U.; Cai, J.; Wang, Y.; Qi, M.; Sun, P.; Ping, Z.; Fu, X. Body mass index had different effects on premenopausal and postmenopausal breast cancer risks: A dose-response meta-analysis with 3,318,796 subjects from 31 cohort studies. BMC Public Health 2017, 17, 936. [Google Scholar] [CrossRef]
- Grosso, G.; Bella, F.; Godos, J.; Sciacca, S.; Del Rio, D.; Ray, S.; Galvano, F.; Giovannucci, E.L. Possible role of diet in cancer: Systematic review and multiple meta-analyses of dietary patterns, lifestyle factors, and cancer risk. Nutr. Rev. 2017, 75, 405–419. [Google Scholar] [CrossRef]
- Galceran, J.; Ameijide, A.; Carulla, M.; Mateos, A.; Quirós, J.R.; Rojas, D.; Alemán, A.; Torrella, A.; Chico, M.; Vicente, M.; et al. Cancer incidence in Spain, 2015. Clin. Transl. Oncol. 2017, 19, 799–825. [Google Scholar] [CrossRef]


{kind=link}
| Total n = 10,930 | Minimal Compliance n = 817 | Intermediate Compliance n = 8521 | Maximum Compliance n = 1592 | ||
|---|---|---|---|---|---|
| 0–7 points | ≤3 points | 3–≤5 points | >5 points | p-Value | |
| Age at recruitment (years), mean (SD) | 35.0 (10.6) | 32.0 (8.9) | 34.6 (10.3) | 39.9 (11.3) | <0.01 |
| Time of university education (years), mean (SD) | 4.8 (1.3) | 4.9 (1.3) | 4.8 (1.3) | 4.8 (1.4) | 0.35 |
| Smoking status, n (%) Never Former Current | 5646 (51.6) 2491 (22.8) 2794 (25.6) | 393 (48.1) 252 (30.8) 172 (21.1) | 4403 (51.7) 1980 (23.2) 2138 (25.1) | 849 (53.3) 259 (16.3) 484 (30.4) | <0.01 |
| Family history of breast cancer, n (%) No Yes, after the age of 45 years Yes, up to the age of 45 years | 9765 (89.3) 947 (8.7) 218 (2.0) | 717 (87.7) 84 (10.3) 16 (2.0) | 7627 (89.5) 729 (8.6) 165 (1.9) | 1421 (89.3) 134 (8.4) 37 (2.3) | 0.41 |
| Menopausal status at recruitment, n (%) Pre-menopausal Post-menopausal | 10,073 (92.2) 857 (7.8) | 789 (96.6) 28 (3.4) | 7935 (93.1) 586 (6.9) | 1349 (84.7) 243 (15.3) | <0.01 |
| Age at menarche, n (%) ≤11 years 12–13 years 14 years ≥15 years | 2211 (20.2) 5981 (54.7) 1852 (16.9) 886 (8.1) | 145 (17.7) 445 (54.5) 157 (19.2) 70 (8.6) | 1723 (20.2) 4663 (54.7) 1450 (17.0) 685 (8.1) | 343 (21.6) 873 (54.8) 245 (15.4) 131 (8.2) | 0.18 |
| Age at first pregnancy, n (%) Age < 25 years and nulliparous Age ≥ 25 years and nulliparous First pregnancy before 25 years First pregnancy between 25 and 30 years of age First pregnancy being 30 years old or older | 1943 (17.8) 5364 (49.1) 511 (4.7) 1582 (14.4) 1530 (14.0) | 185 (22.6) 441 (54.0) 22 (2.7) 80 (9.8) 89 (10.9) | 1595 (18.7) 4172 (49.0) 369 (4.3) 1205 (14.1) 1180 (13.9) | 163 (10.2) 751 (47.2) 120 (7.5) 297 (18.7) 261 (16.4) | <0.01 |
| Hormone-replacement therapy, n (%) No Yes | 10,414 (95.3) 516 (4.7) | 800 (97.9) 17 (2.1) | 8165 (95.8) 356 (4.2) | 1449 (91.0) 143 (9.0) | <0.01 |
| Oral contraceptive use, n (%) No Yes | 10,665 (97.6) 265 (2.4) | 793 (91.1) 24 (2.9) | 8308 (97.5) 213 (2.5) | 1564 (98.2) 28 (1.8) | 0.13 |
| Overall Breast Cancer | Pre-Menopausal Breast Cancer | Post-Menopausal Breast Cancer | |||||
|---|---|---|---|---|---|---|---|
| Cases/No Cases | HR (95% CI) | Cases/No Cases | HR (95% CI) | Cases/No Cases | HR (95% CI) | ||
| WCRF/AICR score, continuous (0–7) for each additional point | Model 1* | 119/10,811 | 0.85 (0.68–1.06) | 67/9904 | 0.92 (0.68–1.24) | 42/3256 | 0.68 (0.47–0.99) |
| Model 2** | 119/10,811 | 0.89 (0.69–1.08) | 67/9904 | 0.94 (0.69–1.27) | 42/3256 | 0.74 (0.51–1.06) | |
| WCRF/AICR score: ≤ 3 > 3.00-≤ 5.00 > 5.00 | Model 1* | 9/808 94/8427 16/1576 | 1.00 0.81 (0.41–1.61) 0.55 (0.24–1.27) | 3/786 57/7878 7/1342 | 1.00a 1.00a 0.66 (0.30–1.45) | 5/164 31/2494 6/759 | 1.00 0.31 (0.12–0.81) 0.18 (0.05–0.59) |
| ≤ 3 > 3.00-≤ 5.00 > 5.00 | Model 2** | 9/808 94/8427 16/1576 | 1.00 0.87 (0.44–1.74) 0.62 (0.27–1.43) | 3/786 57/7878 7/1342 | 1.00a 1.00a 0.67 (0.30–1.47) | 5/164 31/2494 6/759 | 1.00 0.45 (0.16–1.23) 0.27 (0.08–0.93) |
| Total Study Population | |||
|---|---|---|---|
| Component of the Score | Cases/No Cases | HR (95% CI)a | p-Trend |
| Be in a healthy weight 0 0.5 1 | 9/881 16/1391 94/8539 | 1.00 0.72 (0.31–1.64) 0.90 (0.45–1.79) | 0.85 |
| Be physically active 0 0.5 1 | 13/844 20/1301 86/8666 | 1.00 0.96 (0.47–1.94) 0.65 (0.36–1.19) | 0.07 |
| Eat whole grains, vegetables, fruit, and beans 0–0.25 0.5 0.75–1 | 7/637 7/713 105/9461 | 1.00 1.02 (0.34–2.98) 0.64 (0.26–1.54) | 0.17 |
| Limit “fast foods” 0 0.5 1 | 30/3613 47/3596 42/3602 | 1.00 1.47 (0.92–2.34) 1.11 (0.67–1.82) | 0.77 |
| Limit red and processed meat 0 0.5 1 | 110/9953 7/681 2/177 | 1.000.91 (0.41–2.01) 1.17 (0.28–4.90) | 0.99 |
| Limit sugary drinks 0 0.5 1 | 2/291 79/7569 38/2951 | 1.00b 1.00b 0.93 (0.62–1.40) | - |
| Limit alcohol 0 0.5 1 | 10/623 79/7267 30/2921 | 1.00 0.93 (0.48–1.83) 0.89 (0.43–1.87) | 0.76 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrios-Rodríguez, R.; Toledo, E.; Martinez-Gonzalez, M.A.; Aguilera-Buenosvinos, I.; Romanos-Nanclares, A.; Jiménez-Moleón, J.J. Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research Recommendations and Breast Cancer in the SUN Project. Nutrients 2020, 12, 2076. https://doi.org/10.3390/nu12072076
Barrios-Rodríguez R, Toledo E, Martinez-Gonzalez MA, Aguilera-Buenosvinos I, Romanos-Nanclares A, Jiménez-Moleón JJ. Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research Recommendations and Breast Cancer in the SUN Project. Nutrients. 2020; 12(7):2076. https://doi.org/10.3390/nu12072076
Chicago/Turabian StyleBarrios-Rodríguez, Rocio, Estefanía Toledo, Miguel Angel Martinez-Gonzalez, Inmaculada Aguilera-Buenosvinos, Andrea Romanos-Nanclares, and José Juan Jiménez-Moleón. 2020. "Adherence to the 2018 World Cancer Research Fund/American Institute for Cancer Research Recommendations and Breast Cancer in the SUN Project" Nutrients 12, no. 7: 2076. https://doi.org/10.3390/nu12072076