Weight Loss after 12 Weeks of Exercise and/or Nutritional Guidance Is Not Obligatory for Induced Changes in Local Fat/Lean Mass Indexes in Adults with Excess of Adiposity

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
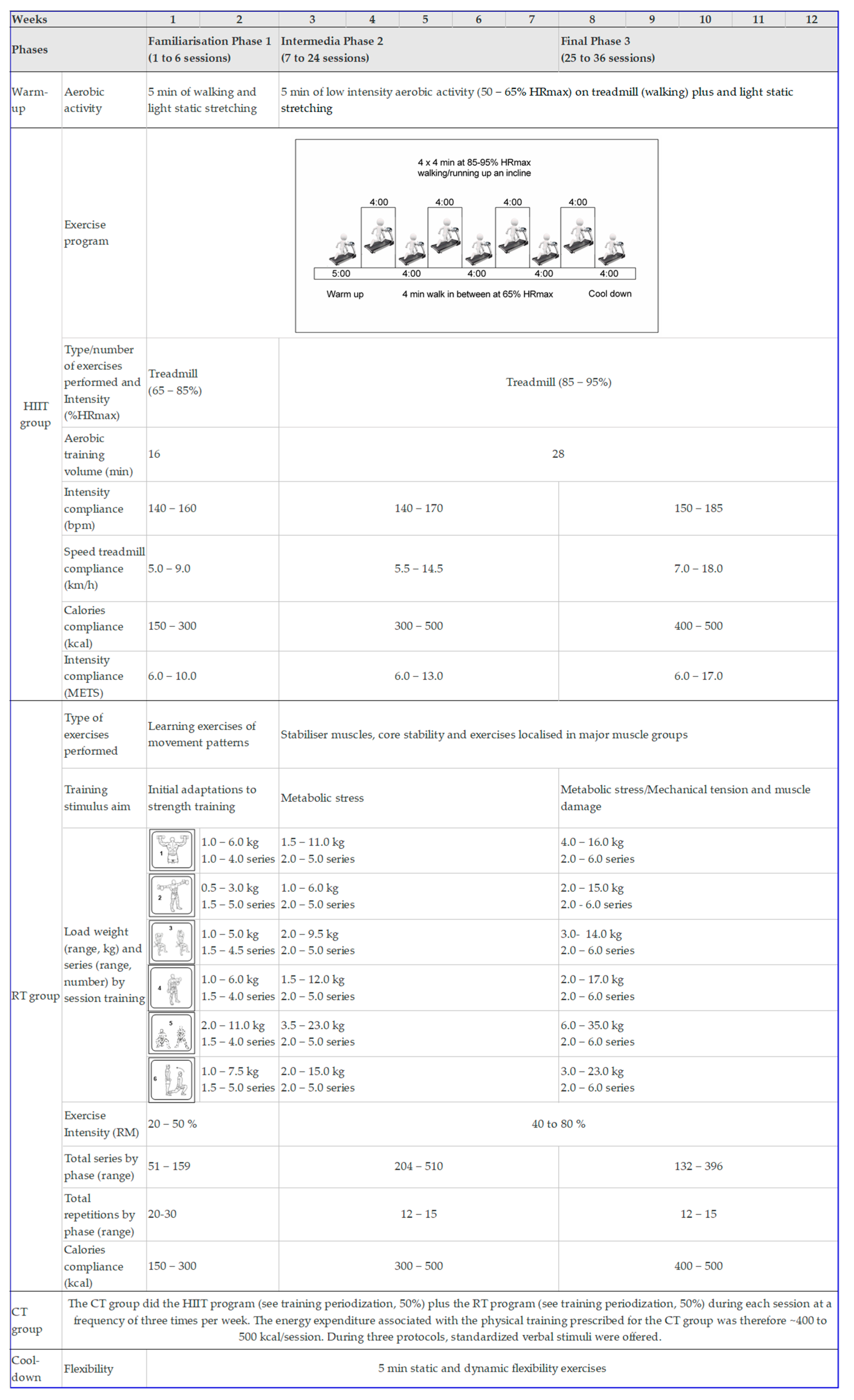
2.2. Procedures
2.3. Classification of Responders and Non-Responders
2.4. Statistical Analysis
3. Results
3.1. Change in Primary Endpoit
3.2. Response Prevalences by Clinically Meaningful Weight Loss (Primary Endpoit)
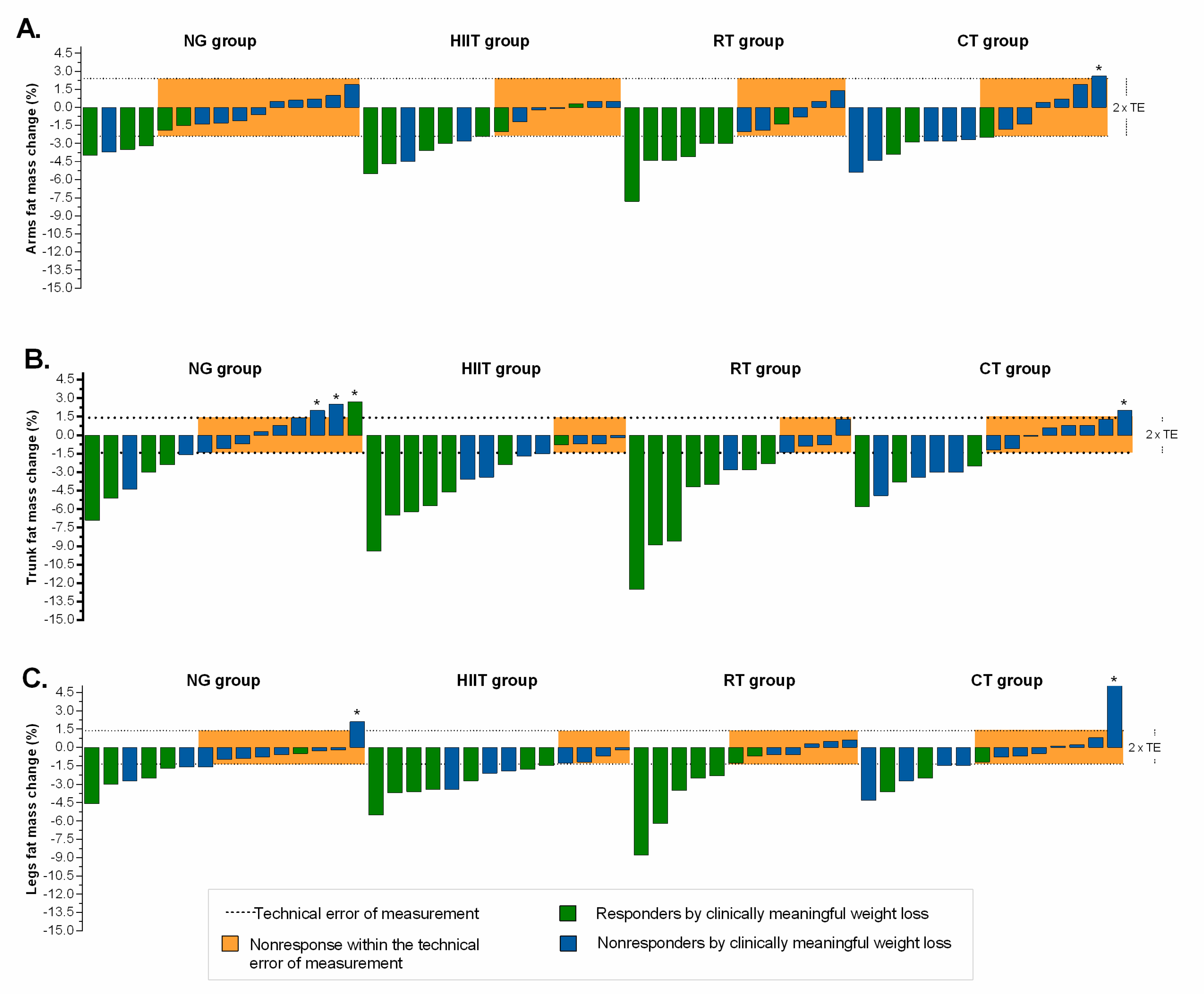
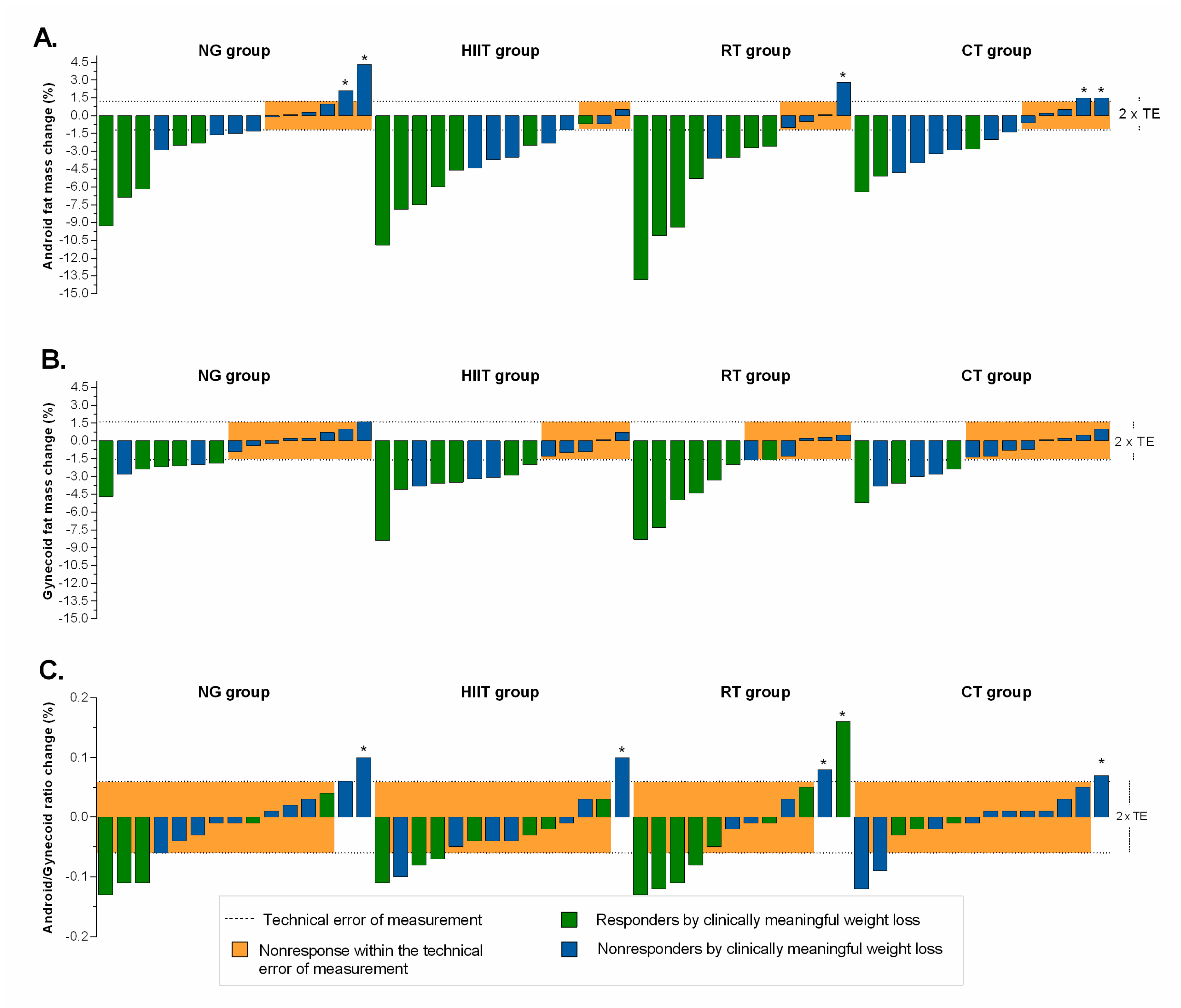
3.3. Change in Secondary Endpoints
3.4. Differences by Mode of Intervention in the Proportion of Responders
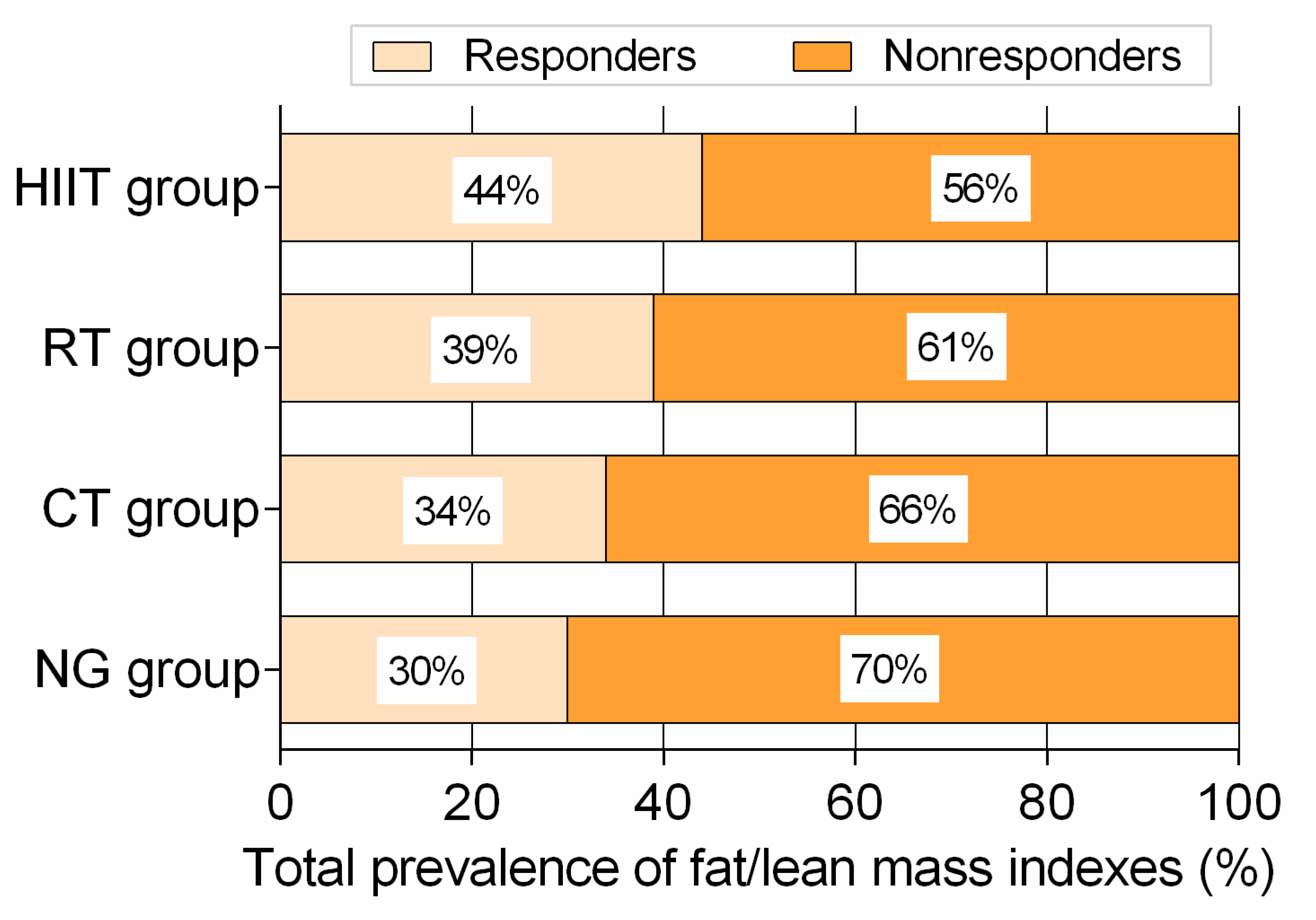
3.5. Total Prevalence of Variables Classified as Responders and Adverse Responders
3.6. Adherence and Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kelly, T.; Yang, W.; Chen, C.-S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [Green Version]
- Cominato, L.; Di Biagio, G.F.; Lellis, D.; Franco, R.R.; Mancini, M.C.; De Melo, M.E. Obesity Prevention: Strategies and Challenges in Latin America. Curr. Obes. Rep. 2018, 7, 97–104. [Google Scholar] [CrossRef]
- ENSIN: Encuesta Nacional de Situación Nutricional. Portal ICBF—Instituto Colombiano de Bienestar Familiar ICBF. Available online: https://www.icbf.gov.co/bienestar/nutricion/encuesta-nacional-situacion-nutricional (accessed on 25 November 2019).
- Lear, S.A.; Teo, K.K.; Gasevic, D.; Zhang, X.; Poirier, P.P.; Rangarajan, S.; Seron, P.; Kelishadi, R.; Tamil, A.M.; Kruger, A.; et al. The association between ownership of common household devices and obesity and diabetes in high, middle and low income countries. Can. Med. Assoc. J. 2014, 186, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Barría, R.M.; Amigo, H. Nutrition transition: A review of Latin American profile. Arch. Latinoam. Nutr. 2006, 56, 3–11. [Google Scholar] [PubMed]
- Williams, E.P.; Mesidor, M.; Winters, K.; Dubbert, P.M.; Wyatt, S.B. Overweight and Obesity: Prevalence, Consequences, and Causes of a Growing Public Health Problem. Curr. Obes. Rep. 2015, 4, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Vasileva, L.; Marchev, A.; Georgiev, M.I. Causes and solutions to “globesity”: The new fa(s)t alarming global epidemic. Food Chem. Toxicol. 2018, 121, 173–193. [Google Scholar] [CrossRef]
- Choi, S.I.; Chung, D.; Lim, J.S.; Lee, M.Y.; Shin, J.Y.; Chung, C.H.; Huh, J.H. Relationship between Regional Body Fat Distribution and Diabetes Mellitus: 2008 to 2010 Korean National Health and Nutrition Examination Surveys. Diabetes Metab. J. 2017, 41, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsing, J.C.; Nguyen, M.H.; Yang, B.; Min, Y.; Han, S.S.; Pung, E.; Winter, S.J.; Zhao, X.; Gan, D.; Hsing, A.W.; et al. Associations Between Body Fat, Muscle Mass, and Nonalcoholic Fatty Liver Disease: A Population-Based Study. Hepatol. Commun. 2019, 3, 1061–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, G.; Bouchard, C.; Bray, G.A.; Greenway, F.L.; Johnson, W.; Newton, R.L.; Ravussin, E.; Ryan, D.H.; Katzmarzyk, P.T. Trunk Versus Extremity Adiposity and Cardiometabolic Risk Factors in White and African American Adults. Diabetes Care 2011, 34, 1415–1418. [Google Scholar] [CrossRef] [Green Version]
- Sakai, Y.; Ito, H.; Egami, Y.; Ohoto, N.; Hijii, C.; Yanagawa, M.; Satoh, S.; Jingu, S. Favourable association of leg fat with cardiovascular risk factors. J. Intern. Med. 2005, 257, 194–200. [Google Scholar] [CrossRef]
- Wildman, R.P.; Janssen, I.; I Khan, U.; Thurston, R.; Barinas-Mitchell, E.; El Khoudary, S.R.; Everson-Rose, S.A.; Kazlauskaite, R.; A Matthews, K.; Sutton-Tyrrell, K. Subcutaneous adipose tissue in relation to subclinical atherosclerosis and cardiometabolic risk factors in midlife women. Am. J. Clin. Nutr. 2011, 93, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Qi, Q.; Yu, Z.; Sun, Q.; Wang, J.; Franco, O.H.; Sun, L.; Li, H.; Liu, Y.; Hu, F.B.; et al. Independent and Opposite Associations of Trunk and Leg Fat Depots with Adipokines, Inflammatory Markers, and Metabolic Syndrome in Middle-Aged and Older Chinese Men and Women. J. Clin. Endocrinol. Metab. 2010, 95, 4389–4398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Chan, J.S.Y.; Ren, L.; Yan, J.H. Obesity Reduces Cognitive and Motor Functions across the Lifespan. Neural Plast. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The biomechanics of restricted movement in adult obesity. Obes. Rev. 2006, 7, 13–24. [Google Scholar] [CrossRef]
- Smith, E.; Hay, P.; Campbell, L.; Trollor, J.N. A review of the association between obesity and cognitive function across the lifespan: Implications for novel approaches to prevention and treatment. Obes. Rev. 2011, 12, 740–755. [Google Scholar] [CrossRef]
- Luppino, F.S.; De Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.J.H.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Willoughby, D.; Hewlings, S.; Kalman, D. Body composition changes in weight loss: Strategies and supplementation for maintaining lean body mass, a brief review. Nutrients 2018, 10, 1876. [Google Scholar] [CrossRef] [Green Version]
- Martín-Moraleda, E.; Delisle, C.; Collado Mateo, D.; Aznar-Lain, S. Cambios en la pérdida de peso y la composición corporal con dieta cetogénica y práctica de actividad física: Revisión narrativa, metodológica y sistemática. Nutricion Hospalaria 2019, 36, 1196–1204. [Google Scholar] [CrossRef] [Green Version]
- Bhutani, S.; Klempel, M.C.; Kroeger, C.M.; Trepanowski, J.F.; Varady, K.A. Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity 2013, 21, 1370–1379. [Google Scholar] [CrossRef]
- Byrd, B.R.; Keith, J.; Keeling, S.M.; Weatherwax, R.M.; Nolan, P.B.; Ramos, J.S.; Dalleck, L.C. Personalized Moderate-Intensity Exercise Training Combined with High-Intensity Interval Training Enhances Training Responsiveness. Int. J. Environ. Res. Public Health 2019, 16, 2088. [Google Scholar] [CrossRef] [Green Version]
- Oh, M.; Kim, S.; An, K.Y.; Min, J.; Yang, H.I.; Lee, J.; Lee, M.K.; Kim, D.I.; Lee, H.S.; Lee, J.W.; et al. Effects of alternate day calorie restriction and exercise on cardio-metabolic risk factors in overweight and obese adults: An exploratory randomized controlled study. BMC Public Health 2018, 18, 1124. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.S.; Dhaliwal, S.S.; Hills, A.P.; Pal, S. The effect of 12 weeks of aerobic, resistance or combination exercise training on cardiovascular risk factors in the overweight and obese in a randomized trial. BMC Public Health 2012, 12, 704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadi, H.R.; Khoshnam, M.S.; Khoshnam, E. Effects of different modes of exercise training on body composition and risk factors for cardiovascular disease in middle-aged men. Int. J. Prev. Med. 2018, 9. [Google Scholar] [CrossRef]
- Ross, R.; Goodpaster, B.H.; Koch, L.G.; Sarzynski, M.A.; Kohrt, W.M.; Johannsen, N.M.; Skinner, J.S.; Castro, A.; Irving, B.A.; Noland, R.C.; et al. Precision exercise medicine: Understanding exercise response variability. Br. J. Sports Med. 2019, 53, 1141–1153. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, C.; Ramírez-Campillo, R.; Ramírez-Vélez, R.; Izquierdo, M. Prevalence of non-responders for glucose control markers after 10 weeks of high-intensity interval training in adult women with higher and lower insulin resistance. Front. Physiol. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, C.; Ramírez-Campillo, R.; Ramírez-Vélez, R.; Izquierdo, M. Effects and prevalence of nonresponders after 12 weeks of high-intensity interval or resistance training in women with insulin resistance: A randomized trial. J. Appl. Physiol. 2017, 122, 985–996. [Google Scholar] [CrossRef]
- Álvarez, C.; Ramírez-Campillo, R.; Cristi-Montero, C.; Ramírez-Vélez, R.; Izquierdo, M. Prevalence of non-responders for blood pressure and cardiometabolic risk factors among prehypertensive women after long-term high-intensity interval training. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Gurd, B.J.; Giles, M.D.; Bonafiglia, J.T.; Raleigh, J.P.; Boyd, J.C.; Ma, J.K.; Zelt, J.G.E.; Scribbans, T.D. Incidence of nonresponse and individual patterns of response following sprint interval training. Appl. Physiol. Nutr. Metab. 2016, 41, 229–234. [Google Scholar] [CrossRef]
- Turner, R.M.; Park, B.K.; Pirmohamed, M. Parsing interindividual drug variability: An emerging role for systems pharmacology. Wiley Interdiscip. Rev. Syst. Biol. Med. 2015, 7, 221–241. [Google Scholar] [CrossRef]
- Healey, G.; Murphy, R.; Brough, L.; Butts, C.; Coad, J. Interindividual Variability in Gut Microbiota and Host Response to Dietary Interventions—PubMed. Nutr. Rev. 2017, 75, 1059–1080. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Vélez, R.; Izquierdo, M. Editorial: Precision physical activity and exercise prescriptions for disease prevention: The effect of interindividual variability under different training approaches. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Lobelo, F.; Izquierdo, M. Exercise for Disease Prevention and Management: A Precision Medicine Approach. J. Am. Med. Dir. Assoc. 2017, 18, 633–634. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.J.; Allison, M.; Daviglus, M.L.; Isasi, C.R.; Keller, C.; Leira, E.C.; Palaniappan, L.; Piña, I.L.; Ramirez, S.M.; Rodriguez, B.; et al. Status of cardiovascular disease and stroke in hispanics/latinos in the united states: A science advisory from the american heart association. Circulation 2014, 130, 593–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, N.A.; Hopkins, M.; Caudwell, P.; Stubbs, R.J.; Blundell, J.E. Individual variability following 12 weeks of supervised exercise: Identification and characterization of compensation for exercise-induced weight loss. Int. J. Obes. 2008, 32, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Church, T.S.; Martin, C.K.; Thompson, A.M.; Earnest, C.P.; Mikus, C.R.; Blair, S.N. Changes in weight, waist circumference and compensatory responses with different doses of exercise among sedentary, overweight postmenopausal women. PLoS ONE 2009, 4. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hill, J.O.; Jacobsen, D.J.; Potteiger, J.; Sullivan, D.K.; Johnson, S.L.; Heelan, K.; Hise, M.; Fennessey, P.V.; Sonko, B.; et al. Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: The midwest exercise trial. Arch. Intern. Med. 2003, 163, 1343–1350. [Google Scholar] [CrossRef]
- Hammond, B.P.; Stotz, P.J.; Brennan, A.M.; Lamarche, B.; Day, A.G.; Ross, R. Individual Variability in Waist Circumference and Body Weight in Response to Exercise. Med. Sci. Sports Exerc. 2019, 51, 315–322. [Google Scholar] [CrossRef]
- O’Donoghue, G.; Kennedy, A.; Andersen, G.S.; Carr, B.; Cleary, S.; Durkan, E.; Davis, H.; Færch, K.; Fitzpatrick, P.; Kenny, H.; et al. Phenotypic Responses to a Lifestyle Intervention Do Not Account for Inter-Individual Variability in Glucose Tolerance for Individuals at High Risk of Type 2 Diabetes. Front. Physiol. 2019, 10, 317. [Google Scholar] [CrossRef] [Green Version]
- Galani, C.; Schneider, H. Prevention and treatment of obesity with lifestyle interventions: Review and meta-analysis. Int. J. Public Health 2007, 52, 348–359. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Castro-Astudillo, K.; Correa-Bautista, J.E.; González-Ruíz, K.; Izquierdo, M.; García-Hermoso, A.; Álvarez, C.; Ramírez-Campillo, R.; Correa-Rodríguez, M. The Effect of 12 Weeks of Different Exercise Training Modalities or Nutritional Guidance on Cardiometabolic Risk Factors, Vascular Parameters, and Physical Fitness in Overweight Adults. J. Strength Cond. Res. 2020, 1. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Hernandez, A.; Castro, K.; Tordecilla-Sanders, A.; González-Ruíz, K.; Correa-Bautista, J.E.; Izquierdo, M.; García-Hermoso, A. High Intensity Interval—Vs. Resistance or Combined- Training for Improving Cardiometabolic Health in Overweight Adults (Cardiometabolic HIIT-RT Study): Study protocol for a randomised controlled trial. Trials 2016, 17, 298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewiecki, E.M.; Binkley, N.; Morgan, S.L.; Shuhart, C.R.; Camargos, B.M.; Carey, J.J.; Gordon, C.M.; Jankowski, L.G.; Lee, J.K.; Leslie, W.D. Best Practices for Dual-Energy X-ray Absorptiometry Measurement and Reporting: International Society for Clinical Densitometry Guidance. J. Clin. Densitom. 2016, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.A.; Bray, G.A.; Ryan, D.H. Is 5% weight loss a satisfactory criterion to define clinically significant weight loss? Obesity 2015, 23, 2319–2320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackburn, G. Effect of Degree of Weight Loss on Health Benefits. Obes. Res. 1995, 3, 211s–216s. [Google Scholar] [CrossRef]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [Green Version]
- Bouchard, C.; Blair, S.N.; Church, T.S.; Earnest, C.P.; Hagberg, J.M.; Häkkinen, K.; Jenkins, N.T.; Karavirta, L.; Kraus, W.E.; Leon, A.S.; et al. Adverse metabolic response to regular exercise: Is it a rare or common occurrence? PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Kerr, A.; Slater, G.J.; Byrne, N.; Nana, A. Reliability of 2 Different Positioning Protocols for Dual-Energy X-ray Absorptiometry Measurement of Body Composition in Healthy Adults. J. Clin. Densitom. 2016, 19, 282–289. [Google Scholar] [CrossRef]
- Hopkins, W.G. Measures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Manthou, E.; Gill, J.M.R.; Wright, A.; Malkova, D. Behavioural Compensatory Adjustments to Exercise Training In Overweight Women. Med. Sci. Sports Exerc. 2009, 42, 1. [Google Scholar] [CrossRef] [Green Version]
- Gremeaux, V.; Drigny, J.; Nigam, A.; Juneau, M.; Guilbeault, V.; Latour, E.; Gayda, M. Long-term lifestyle intervention with optimized high-intensity interval training improves body composition, Cardiometabolic risk, and exercise parameters in patients with abdominal obesity. Am. J. Phys. Med. Rehabil. 2012, 91, 941–950. [Google Scholar] [CrossRef]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.P.; Church, T.S. The role of exercise and physical activity in weight loss and maintenance. Prog. Cardiovasc. Dis. 2014, 56, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Willis, L.H.; Slentz, C.A.; Bateman, L.A.; Shields, A.T.; Piner, L.W.; Bales, C.W.; Houmard, J.A.; Kraus, W.E. Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. J. Appl. Physiol. 2012, 113, 1831–1837. [Google Scholar] [CrossRef] [PubMed]
- Villareal, D.T.; Aguirre, L.; Gurney, A.B.; Waters, D.L.; Sinacore, D.R.; Colombo, E.; Armamento-Villareal, R.; Qualls, C. Aerobic or Resistance Exercise, or Both, in Dieting Obese Older Adults. N. Engl. J. Med. 2017, 376, 1943–1955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keating, S.E.; Machan, E.A.; O’Connor, H.T.; Gerofi, J.A.; Sainsbury, A.; Caterson, I.D.; Johnson, N.A. Continuous exercise but not high intensity interval training improves fat distribution in overweight adults. J. Obes. 2014, 2014, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Tong, T.K.; Qiu, W.; Zhang, X.; Zhou, S.; Liu, Y.; He, Y. Comparable Effects of High-Intensity Interval Training and Prolonged Continuous Exercise Training on Abdominal Visceral Fat Reduction in Obese Young Women. J. Diabetes Res. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.; van den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Schumann, M.; Yli-Peltola, K.; Abbiss, C.; Häkkinen, K. Cardiorespiratory Adaptations during Concurrent Aerobic and Strength Training in Men and Women. PLoS ONE 2015, 10, e0139279. [Google Scholar] [CrossRef] [Green Version]
- Fyfe, J.J.; Loenneke, J. Interpreting Adaptation to Concurrent Compared with Single-Mode Exercise Training: Some Methodological Considerations. Sports Med. 2017, 48, 289–297. [Google Scholar] [CrossRef]
- Hennessy, L.; Watson, A. The interference effects of training for strength and endurance simultaneously. J. Strength Cond. Res. 1994, 8, 12–19. [Google Scholar]
- Hunter, G.; Demment, R.; Miller, D. Development of strength and maximum oxygen uptake during simultaneous training for strength and endurance. J. Sports Med. Phys. Fit. 1987, 27, 269–275. [Google Scholar]
- Methenitis, S. A Brief Review on Concurrent Training: From Laboratory to the Field. Sports 2018, 6, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Bonafiglia, J.T.; Nelms, M.W.; Preobrazenski, N.; LeBlanc, C.; Robins, L.; Lu, S.; Lithopoulos, A.; Walsh, J.J.; Gurd, B.J. Moving beyond threshold-based dichotomous classification to improve the accuracy in classifying non-responders. Physiol. Rep. 2018, 6, e13928. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | NG (n= 15) | HIIT (n= 14) | RT (n= 12) | CT (n= 14) | p Value |
|---|---|---|---|---|---|
| Anthropometric parameters | |||||
| Age, years | 41.2 (7.6) | 43.6 (7.2) | 38.7 (6.0) | 39.2 (6.8) | 0.237 |
| Body mass, kg | 82.4 (16.4) | 75.1 (10.8) | 84.2 (11.5) | 77.2 (23.1) | 0.169 |
| Body mass index, kg/m2 | 29.3 (3.9) | 29.7 (2.7) | 31.3 (3.7) | 30.2 (3.8) | 0.531 |
| Waist circumference, cm | 95.1 (12.4) | 90.0 (8.6) | 94.7 (8.3) | 91.2 (7.3) | 0.367 |
| Educational level, n (%)a | |||||
| High school | 2 (13) | 1 (13) | 2 (17) | 1 (7) | 0.188 |
| Technician | 8 (53) | 5 (36) | 0 (0) | 4 (27) | |
| University | 5 (33) | 8 (57) | 10 (83) | 9 (64) | |
| Level of occupation, n (%)a | |||||
| Full timer | 7 (47) | 7 (44) | 8 (50) | 10 (71) | 0.495 |
| Half timer | 1 (7) | 2 (13) | 0 (0) | 1 (7) | |
| Independent | 5 (33) | 5 (31) | 2 (13) | 3 (21) | |
| Housewife | 1 (7) | 0 (0) | 0 (0) | 0 (0) | |
| Unemployed | 1 (7) | 0 (0) | 2 (13) | 0 (0) | |
| Socioeconomic status, n (%)a | |||||
| Low | 1 (7) | 1 (7) | 2 (17) | 1 (7) | 0.651 |
| Mid | 14 (93) | 13 (93) | 8 (67) | 11 (79) | |
| High | 0 (0) | 0 (0) | 2 (17) | 2 (14) | |
| Caloric distribution by nutrients | |||||
| Daily caloric intake, mean (SD) | 1441 (471) | 1595 (279) | 1791 (439) | 1811 (439) | 0.060 |
| Protein, % | 19.8 (5.1) | 17.4 (5.5) | 18.2 (4.2) | 18.4 (3.1) | 0.221 |
| Fat, % | 37.7 (7.7) | 35.4 (3.6) | 38.1 (5.5) | 35.2 (5.6) | 0.435 |
| Carbohydrate, % | 42.7 (8.0) | 47.3 (8.4) | 43.7 (5.6) | 46.8 (8.4) | 0.195 |
| Variable | Baseline | 12 Weeks | Within-Group Change from | Intergroup Difference in Change | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline to 12 Weeks | from Baseline to 12 Weeks | |||||||||
| Mean (standard deviation) | Mean (95% Confidence Interval) | |||||||||
| Primary endpoint | ||||||||||
| Weight (kg) | ||||||||||
| HIIT group | 75.1 | 10.8 | 70.6 | 11.2 | −4.5 | −7.0 | −1.9 * | N.A | ||
| RT group | 84.2 | 11.5 | 79.4 | 13.2 | −4.8 | −8.0 | −1.6 ** | N.A | ||
| CT group | 77.2 | 23.1 | 75.6 | 22.7 | −1.7 | −3.4 | 0.0 * | N.A | ||
| NG group | 82.4 | 16.4 | 81.3 | 18.6 | −1.1 | −3.0 | 0.7 | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | −3.3 | −6.4 | −0.3 † | ||||
| RT group vs. NG group | N.A | N.A | N.A | −3.6 | −7.0 | −0.3 † | ||||
| CT group vs. NG group | N.A | N.A | N.A | 0.6 | −3.0 | −1.8 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 2.8 | −1.0 | 5.6 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 3.1 | −0.1 | 6.3 | ||||
| Secondary endpoints | ||||||||||
| Arms fat mass (%) | ||||||||||
| HIIT group | 40.2 | 7.4 | 38.3 | 7.3 | −2.1 | −3.2 | −0.9 ** | N.A | ||
| RT group | 37.8 | 10.4 | 35.1 | 9.8 | −2.6 | −4.2 | −1.1 ** | N.A | ||
| CT group | 40.4 | 8.6 | 38.6 | 8.7 | −1.8 | −3.2 | −0.4 * | N.A | ||
| NG group | 33 | 6.4 | 31.8 | 7.3 | −1.2 | −2.2 | −0.2 * | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | −0.9 | −2.3 | 0.6 | ||||
| RT group vs. NG group | N.A | N.A | N.A | −1.4 | −3.1 | 0.3 | ||||
| CT group vs. NG group | N.A | N.A | N.A | −0.6 | −3.1 | 1.9 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 0.4 | −1.6 | 2.3 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 0.9 | −1.3 | 3.1 | ||||
| Trunk fat mass (%) | ||||||||||
| HIIT group | 42.7 | 5.4 | 39.4 | 6.3 | −3.4 | −5.0 | −1.8 *** | N.A | ||
| RT group | 43.1 | 5.6 | 39.1 | 7.3 | −4.0 | −6.5 | −1.4 ** | N.A | ||
| CT group | 44.3 | 6.9 | 42.1 | 7.7 | −1.8 | −3.1 | −0.5 * | N.A | ||
| NG group | 41.7 | 3.8 | 40 | 5.4 | -1.3 | −2.8 | 0.3 | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | −2.3 | −4.4 | −0.1 † | ||||
| RT group vs. NG group | N.A | N.A | N.A | −2.9 | −5.6 | −0.1 † | ||||
| CT group vs. NG group | N.A | N.A | N.A | −0.7 | −2.7 | 1.3 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 1.6 | −0.4 | 3.6 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 2.2 | 0.4 | 4.8 | ||||
| Legs fat mass (%) | ||||||||||
| HIIT group | 37.5 | 7.4 | 35 | 7.2 | −2.4 | −3.2 | −1.5 *** | |||
| RT group | 35.8 | 10.7 | 33.7 | 10.7 | −2.1 | −3.9 | −0.3 * | |||
| CT group | 36.4 | 10 | 35.6 | 9.5 | −0.7 | −2.4 | 0.9 | |||
| NG group | 30.8 | 7.3 | 29.6 | 7.5 | −1.3 | −2.2 | −0.5 ** | |||
| HIIT group vs. NG group | N.A | N.A | N.A | −1.0 | 2.2 | 0.2 | ||||
| RT group vs. NG group | N.A | N.A | N.A | −0.8 | −2.5 | 1.0 | ||||
| CT group vs. NG group | N.A | N.A | N.A | 0.6 | −1.2 | 2.3 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 1.6 | −0.2 | 3.4 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 1.4 | −1.0 | 3.7 | ||||
| Arms lean mass (g) | ||||||||||
| HIIT group | 4734.9 | 1131.8 | 4593.1 | 1179.4 | −115.8 | −295.4 | 63.8 | N.A | ||
| RT group | 5608.7 | 1616.8 | 5553.3 | 1330.7 | −55.4 | −353.1 | 242.3 | N.A | ||
| CT group | 4608.5 | 863.0 | 4707.2 | 1013.7 | 66.8 | −139.9 | 273.5 | N.A | ||
| NG group | 5976.6 | 1740.1 | 5753.3 | 1652.2 | −88.9 | −275.1 | 97.2 | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | −26.9 | −274.1 | 220.4 | ||||
| RT group vs. NG group | N.A | N.A | N.A | 33.5 | −285.4 | 352.4 | ||||
| CT group vs. NG group | N.A | N.A | N.A | 155.7 | −108.7 | 420.2 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 182.6 | −77.9 | 442.1 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 122.2 | −212.6 | 457.0 | ||||
| Trunk lean mass (g) | ||||||||||
| HIIT group | 20,205.40 | 2990.6 | 20,619.90 | 2952.6 | 321.7 | −5.5 | 648.9 | N.A | ||
| RT group | 22,571.50 | 4144.4 | 22,672.60 | 4007.6 | 101.1 | −362.8 | 565.0 | N.A | ||
| CT group | 20,583.00 | 2221.1 | 20,759.10 | 2327.6 | 137.7 | −200.0 | 475.4 | N.A | ||
| NG group | 23,380.70 | 4727.9 | 23,141.60 | 4725.9 | 171.7 | −187.4 | 530.7 | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | 150.0 | −315.4 | 615.5 | ||||
| RT group vs. NG group | N.A | N.A | N.A | −70.6 | −617.4 | 476.2 | ||||
| CT group vs. NG group | N.A | N.A | N.A | −34.0 | −505.6 | 437.7 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | −184.0 | −631.4 | 263.4 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 36.5 | −495.5 | 568.8 | ||||
| Legs lean mass (g) | ||||||||||
| HIIT group | 14,589.40 | 2723.2 | 14,452.40 | 2859.7 | −129.0 | −534.9 | 276.9 | N.A | ||
| RT group | 17,128.30 | 3123.8 | 17,065.80 | 3441.3 | −62.4 | −542.4 | 417.6 | N.A | ||
| CT group | 15,427.20 | 2717.7 | 15,578.90 | 3088.9 | 51.7 | −241.3 | 344.7 | N.A | ||
| NG group | 17,268.90 | 3936.2 | 16,995.20 | 3993.5 | 75.4 | −292.0 | 442.8 | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | −204.4 | −725.0 | 316.2 | ||||
| RT group vs. NG group | N.A | N.A | N.A | −137.8 | −700.5 | 424.9 | ||||
| CT group vs. NG group | N.A | N.A | N.A | −23.7 | −476.2 | 428.8 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 180.7 | −295.6 | 657.0 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 114.1 | −400.8 | 628.3 | ||||
| Distribution indices | ||||||||||
| Android fat mass (%) | ||||||||||
| HIIT group | 44.9 | 6.9 | 41.0 | 7.7 | −4.0 | −5.8 | −2.1 *** | N.A | ||
| RT group | 46.2 | 5.1 | 42.0 | 7.4 | −4.1 | −7.2 | −1.1 ** | N.A | ||
| CT group | 46.9 | 7.3 | 44.4 | 8.6 | −2.1 | −3.6 | −0.7 ** | N.A | ||
| NG group | 44.6 | 4.1 | 42.2 | 6.2 | −1.8 | −3.7 | 0.2 | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | −2.2 | −4.8 | 0.4 | ||||
| RT group vs. NG group | N.A | N.A | N.A | −2.3 | −5.6 | 1.0 | ||||
| CT group vs. NG group | N.A | N.A | N.A | 0.3 | −2.7 | 2.0 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | −1.9 | −0.4 | 4.1 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 2.0 | −1.0 | 5.1 | ||||
| Gynecoid fat mass (%) | ||||||||||
| HIIT group | 40.0 | 6.4 | 37.2 | 6.6 | −2.6 | −3.9 | −1.3 *** | N.A | ||
| RT group | 38.9 | 10.8 | 36.1 | 11.1 | −2.8 | −4.7 | −1.0 ** | N.A | ||
| CT group | 40.7 | 9.1 | 38.9 | 9.2 | −1.7 | −2.7 | −0.6 ** | N.A | ||
| NG group | 35.0 | 7.1 | 33.9 | 7.7 | −1.1 | −2.0 | −0.2 * | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | −1.6 | 3.1 | 0.0 | ||||
| RT group vs. NG group | N.A | N.A | N.A | −1.7 | −3.6 | 0.1 | ||||
| CT group vs. NG group | N.A | N.A | N.A | −0.6 | −1.9 | 0.8 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 1.0 | −0.6 | 2.6 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 1.2 | −0.8 | 3.1 | ||||
| Android/Gynecoid ratio (%) | ||||||||||
| HIIT group | 1.1 | 0.2 | 1.1 | 0.2 | 0 | −0.1 | 0 | N.A | ||
| RT group | 1.3 | 0.3 | 1.2 | 0.4 | 0 | −0.1 | 0 | N.A | ||
| CT group | 1.2 | 0.2 | 1.2 | 0.2 | 0 | 0 | 0 | N.A | ||
| NG group | 1.3 | 0.3 | 1.3 | 0.3 | 0 | −0.1 | 0 | N.A | ||
| HIIT group vs. NG group | N.A | N.A | N.A | 0 | −0.1 | 0 | ||||
| RT group vs. NG group | N.A | N.A | N.A | 0 | −0.1 | 0 | ||||
| CT group vs. NG group | N.A | N.A | N.A | 0 | 0 | 0.1 | ||||
| CT group vs. HIIT group | N.A | N.A | N.A | 0 | 0 | 0.1 | ||||
| CT group vs. RT group | N.A | N.A | N.A | 0 | 0 | 0.1 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Vélez, R.; Izquierdo, M.; Castro-Astudillo, K.; Medrano-Mena, C.; Monroy-Díaz, A.L.; Castellanos-Vega, R.d.P.; Triana-Reina, H.R.; Correa-Rodríguez, M. Weight Loss after 12 Weeks of Exercise and/or Nutritional Guidance Is Not Obligatory for Induced Changes in Local Fat/Lean Mass Indexes in Adults with Excess of Adiposity. Nutrients 2020, 12, 2231. https://doi.org/10.3390/nu12082231
Ramírez-Vélez R, Izquierdo M, Castro-Astudillo K, Medrano-Mena C, Monroy-Díaz AL, Castellanos-Vega RdP, Triana-Reina HR, Correa-Rodríguez M. Weight Loss after 12 Weeks of Exercise and/or Nutritional Guidance Is Not Obligatory for Induced Changes in Local Fat/Lean Mass Indexes in Adults with Excess of Adiposity. Nutrients. 2020; 12(8):2231. https://doi.org/10.3390/nu12082231
Chicago/Turabian StyleRamírez-Vélez, Robinson, Mikel Izquierdo, Karem Castro-Astudillo, Carolina Medrano-Mena, Angela Liliana Monroy-Díaz, Rocío del Pilar Castellanos-Vega, Héctor Reynaldo Triana-Reina, and María Correa-Rodríguez. 2020. "Weight Loss after 12 Weeks of Exercise and/or Nutritional Guidance Is Not Obligatory for Induced Changes in Local Fat/Lean Mass Indexes in Adults with Excess of Adiposity" Nutrients 12, no. 8: 2231. https://doi.org/10.3390/nu12082231