Clustering of Dietary Patterns and Lifestyles Among Spanish Children in the EsNuPI Study † †

 ,
,  ,
,  , ,
, ,  ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Samples
2.1.1. Dietary Survey and Data Collection
2.1.2. Physical Activity and Sedentary Behavior Questionnaire
2.1.3. Anthropometric Data
2.1.4. Covariates
Parental Education
Household income (HI)
2.2. Data Analysis
2.2.1. Dietary Patterns
2.2.2. Lifestyle Patterns with Clustering Analysis
3. Results
3.1. Description of the Sample
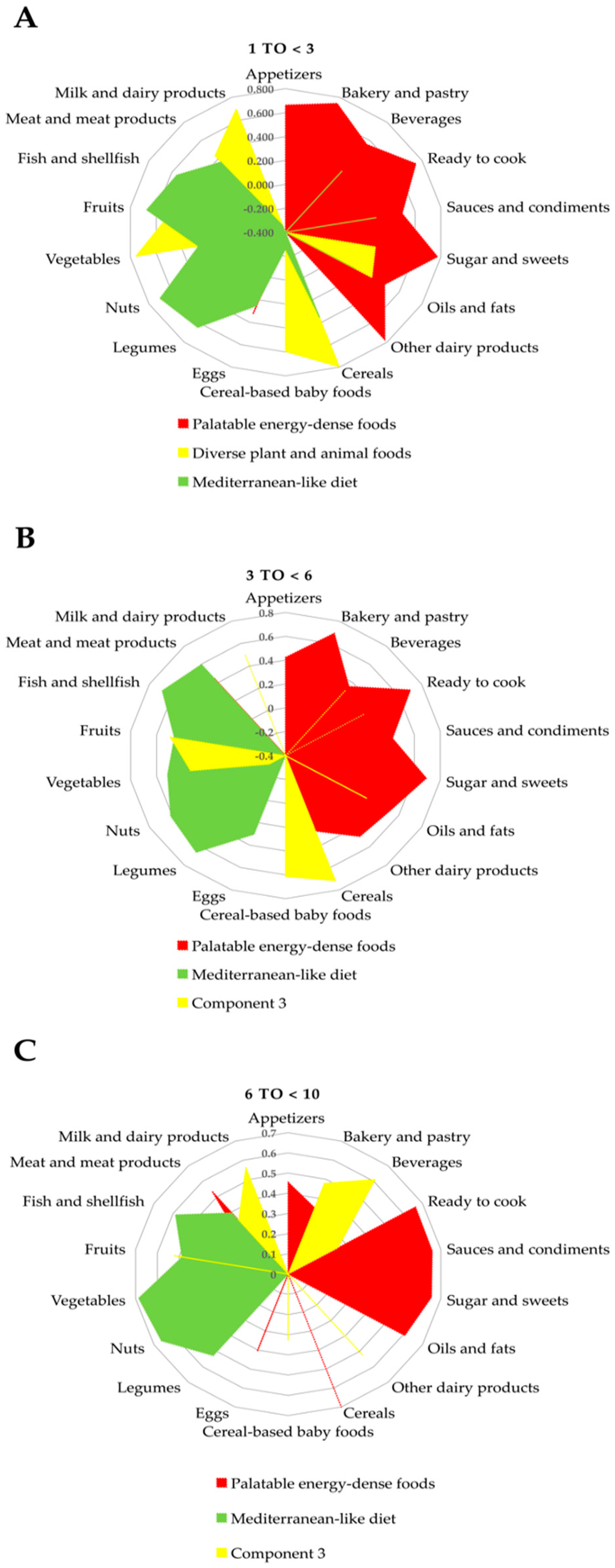
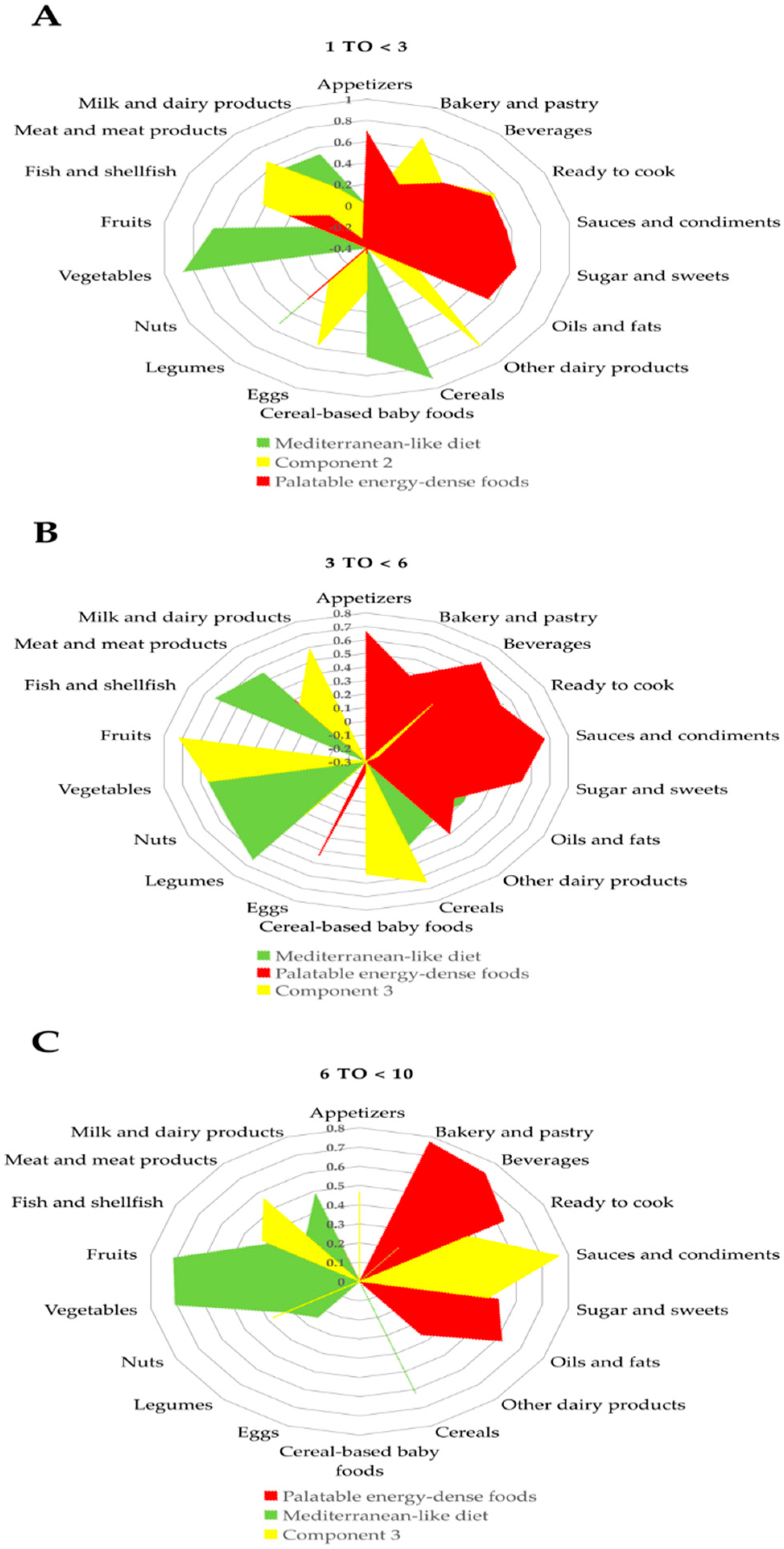
3.2. Dietary Patterns
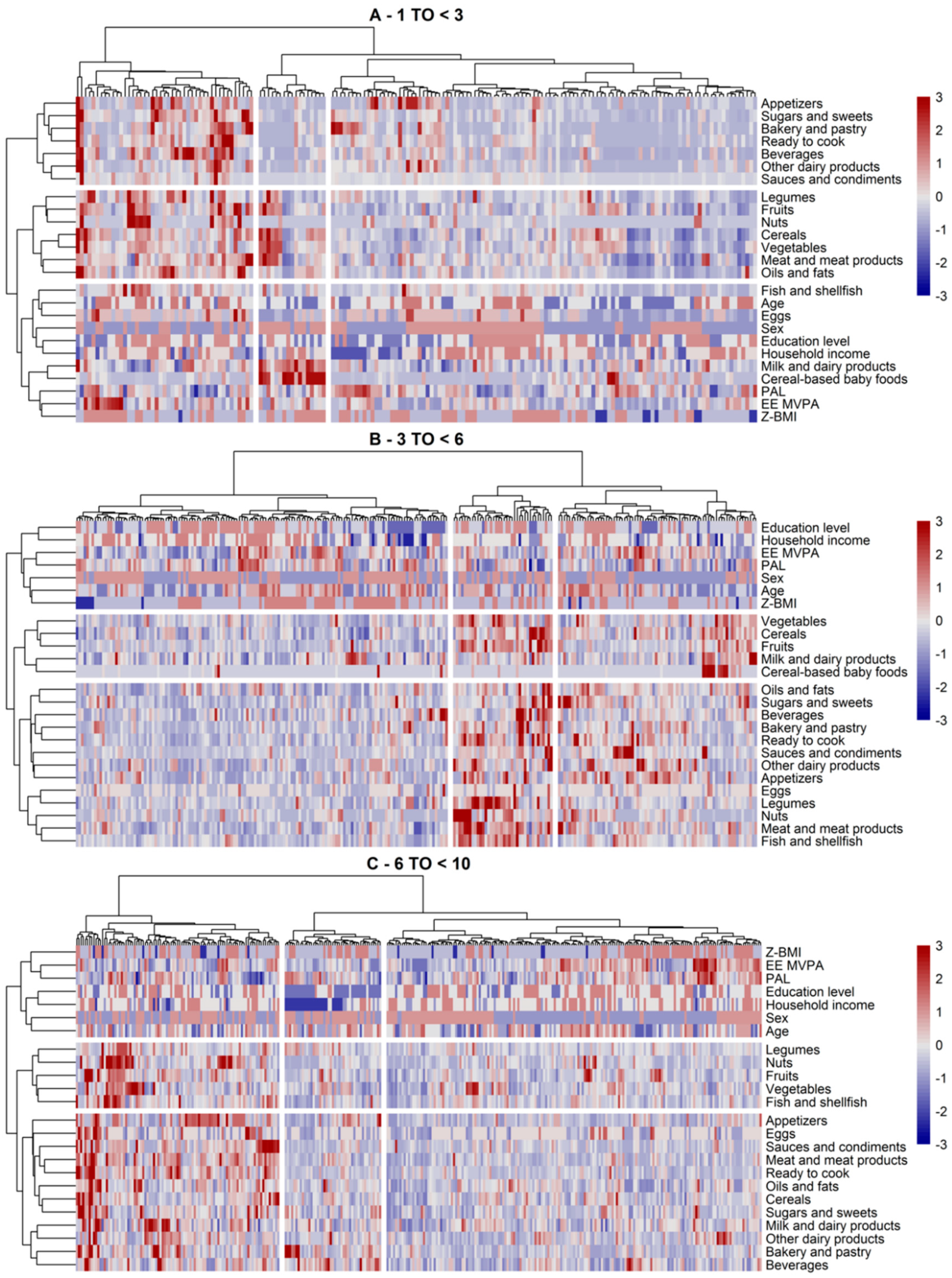
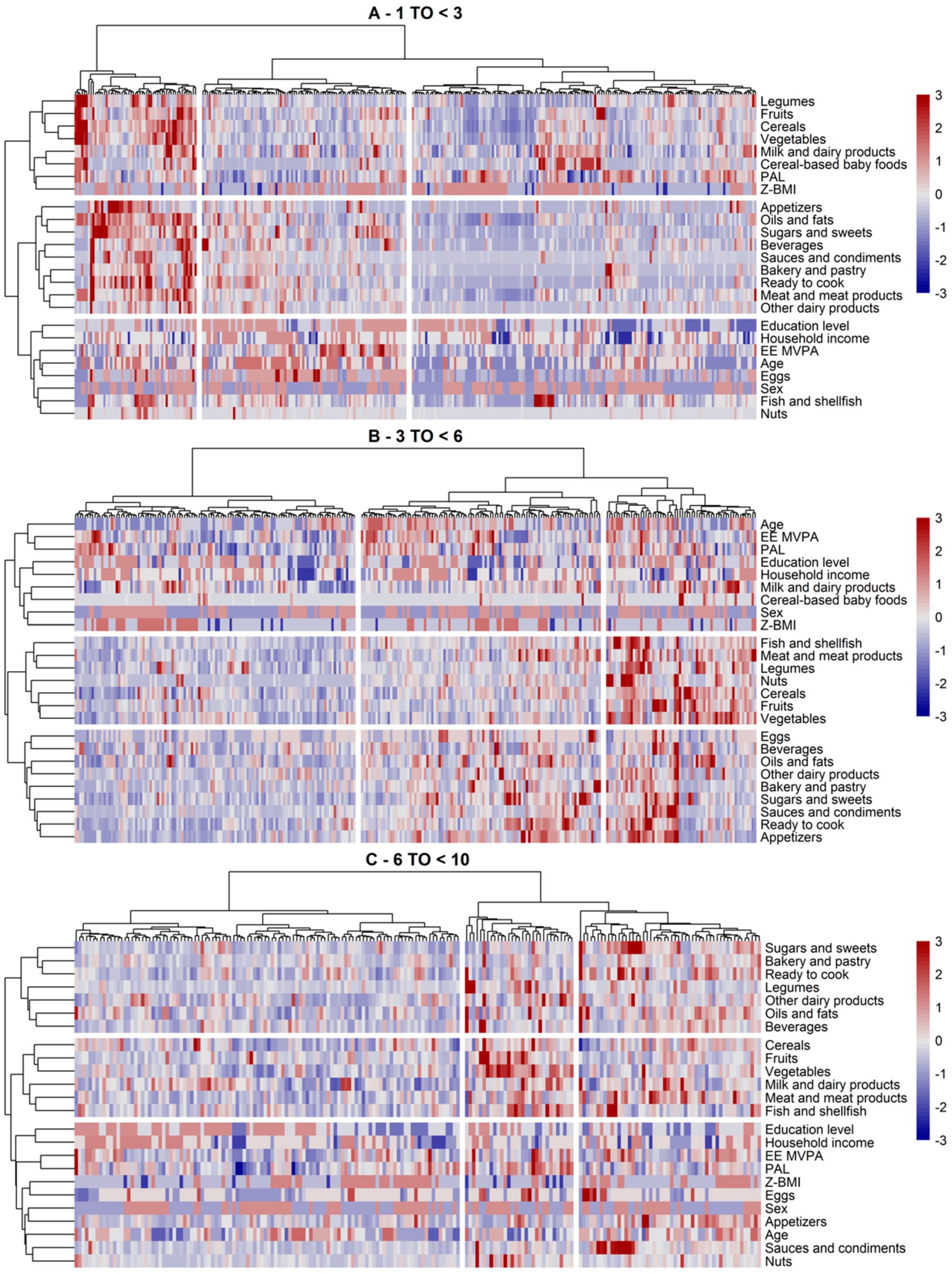
3.3. Dietary and Lifestyle Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ahluwalia, N. Nutrition Monitoring of Children Aged Birth to 24 Mo (B-24): Data Collection and Findings from the NHANES. Adv. Nutr. 2020, 11, 113–127. [Google Scholar] [CrossRef] [Green Version]
- Northstone, K.; Emmett, P.M. Are dietary patterns stable throughout early and mid-childhood? A birth cohort study. Br. J. Nutr. 2008, 100, 1069–1076. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pr. Res. 2007, 68, s1–s56. [Google Scholar]
- Murray, C.J. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis forthe Global Burden of Disease Study. Lancet 2019, 393, 1958–1972. [Google Scholar]
- Biddle, S.J.; Pearson, N.; Ross, G.M.; Braithwaite, R. Tracking of sedentary behaviours of young people: A systematic review. Prev. Med. 2010, 51, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Maynard, M.; Gunnell, D.; Ness, A.R.; Abraham, L.; Bates, C.J.; Blane, D. What influences diet in early old age? Prospective and cross-sectional analyses of the Boyd Orr cohort. Eur. J. Public Health 2006, 16, 316–324. [Google Scholar] [CrossRef] [Green Version]
- Pearson, N.; Biddle, S.J.H.; Griffiths, P.; Johnston, J.P.; Haycraft, E. Clustering and correlates of screen-time and eating behaviours among young children. BMC Public Health 2018, 18, 753. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Santos-Beneit, G.; Pocock, S.; Redondo, J.; Fuster, V.; Penalvo, J.L. Parental and self-reported dietary and physical activity habits in pre-school children and their socio-economic determinants. Public Health Nutr. 2015, 18, 275–285. [Google Scholar] [CrossRef] [Green Version]
- Aranceta, J. Guía de la Alimentación Saludable para Atención Primaria y Colectivos Ciudadanos; SENC-Planeta: Madrid, Spain, 2018. [Google Scholar]
- Health Canada. Canada’s Dietary Guidelines for Health Professionals and Policy Makers. Available online: https://food-guide.canada.ca/static/assets/pdf/CDG-EN-2018.pdf (accessed on 16 August 2020).
- Dietary Guidelines Advisory Committee. Dietary Guidelines for Americans 2015–2020; Government Printing Office: Washington, DC, USA, 2015.
- Gil, A.; Ortega, R.M. Introduction and Executive Summary of the Supplement, Role of Milk and Dairy Products in Health and Prevention of Noncommunicable Chronic Diseases: A Series of Systematic Reviews. Adv. Nutr. 2019, 10, S67–S73. [Google Scholar] [CrossRef]
- Hirahatake, K.M.; Astrup, A.; Hill, J.O.; Slavin, J.L.; Allison, D.B.; Maki, K.C. Potential Cardiometabolic Health Benefits of Full-Fat Dairy: The Evidence Base. Adv. Nutr. 2020, 11, 533–547. [Google Scholar] [CrossRef]
- De Lamas, C.; De Castro, M.J.; Gil-Campos, M.; Gil, A.; Couce, M.L.; Leis, R. Effects of Dairy Product Consumption on Height and Bone Mineral Content in Children: A Systematic Review of Controlled Trials. Adv. Nutr. 2019, 10, S88–S96. [Google Scholar] [CrossRef]
- Ortega, R.; González-Rodríguez, L.; Jiménez Ortega, A.; Perea Sánchez, J.; Bermejo López, L. Implicación del consumo de lácteos en la adecuación de la dieta y de la ingesta de calcio y nutrientes en niños españoles. Abandon. Colest. 2012, 32, 28–36. [Google Scholar]
- Santaliestra-Pasias, A.M.; Gonzalez-Gil, E.M.; Pala, V.; Intemann, T.; Hebestreit, A.; Russo, P.; Van Aart, C.; Rise, P.; Veidebaum, T.; Molnar, D.; et al. Predictive associations between lifestyle behaviours and dairy consumption: The IDEFICS study. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 514–522. [Google Scholar] [CrossRef]
- Lopez-Sobaler, A.M.; Aparicio, A.; Gonzalez-Rodriguez, L.G.; Cuadrado-Soto, E.; Rubio, J.; Marcos, V.; Sanchidrian, R.; Santos, S.; Perez-Farinos, N.; Dal Re, M.A.; et al. Adequacy of Usual Vitamin and Mineral Intake in Spanish Children and Adolescents: ENALIA Study. Nutrients 2017, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- Olza, J.; Aranceta-Bartrina, J.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, A. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 168. [Google Scholar] [CrossRef]
- Vieux, F.; Brouzes, C.M.; Maillot, M.; Briend, A.; Hankard, R.; Lluch, A.; Darmon, N. Role of Young Child Formulae and Supplements to Ensure Nutritional Adequacy in U.K. Young Children. Nutrients 2016, 8, 539. [Google Scholar] [CrossRef] [Green Version]
- Eussen, S.R.; Pean, J.; Olivier, L.; Delaere, F.; Lluch, A. Theoretical Impact of Replacing Whole Cow’s Milk by Young-Child Formula on Nutrient Intakes of UK Young Children: Results of a Simulation Study. Ann. Nutr. Metab. 2015, 67, 247–256. [Google Scholar] [CrossRef]
- Madrigal, C.; Soto-Mendez, M.J.; Hernandez-Ruiz, A.; Ruiz, E.; Valero, T.; Avila, J.M.; Lara-Villoslada, F.; Leis, R.; Victoria, E.M.; Moreno, J.M.; et al. Dietary and Lifestyle Patterns in the Spanish Pediatric Population (One to <10 Years Old): Design, Protocol, and Methodology of the EsNuPI Study. Nutrients 2019, 11, 3050. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Moeller, S.M.; Reedy, J.; Millen, A.E.; Dixon, L.B.; Newby, P.K.; Tucker, K.L.; Krebs-Smith, S.M.; Guenther, P.M. Dietary patterns: Challenges and opportunities in dietary patterns research an Experimental Biology workshop, April 1, 2006. J. Am. Diet. Assoc. 2007, 107, 1233–1239. [Google Scholar] [CrossRef]
- Rodrigues, D.; Muc, M.; Rodrigues, P.R.; Pinto, A.M.; Padez, C. Dietary Patterns and Their Socioeconomic and Behavioral Determinants in 6- to 8-Year-Old Portuguese Children. Ecol. Food Nutr. 2016, 55, 428–441. [Google Scholar] [CrossRef] [Green Version]
- Edefonti, V.; De Vito, R.; Dalmartello, M.; Patel, L.; Salvatori, A.; Ferraroni, M. Reproducibility and Validity of A Posteriori Dietary Patterns: A Systematic Review. Adv. Nutr. 2020, 11, 293–326. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Edefonti, V.; Randi, G.; La Vecchia, C.; Ferraroni, M.; Decarli, A. Dietary patterns and breast cancer: A review with focus on methodological issues. Nutr. Rev. 2009, 67, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Boone-Heinonen, J.; Gordon-Larsen, P.; Adair, L.S. Obesogenic clusters: Multidimensional adolescent obesity-related behaviors in the U.S. Ann. Behav. Med. 2008, 36, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Cameron, A.J.; Crawford, D.A.; Salmon, J.; Campbell, K.; McNaughton, S.A.; Mishra, G.D.; Ball, K. Clustering of obesity-related risk behaviors in children and their mothers. Ann. Epidemiol. 2011, 21, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Alvira, J.M.; Bammann, K.; Pala, V.; Krogh, V.; Barba, G.; Eiben, G.; Hebestreit, A.; Veidebaum, T.; Reisch, L.; Tornaritis, M.; et al. Country-specific dietary patterns and associations with socioeconomic status in European children: The IDEFICS study. Eur. J. Clin. Nutr. 2014, 68, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; Goldbohm, R.A.; De Vries, N.K.; Thijs, C. Clustering of energy balance-related behaviors in 5-year-old children: Lifestyle patterns and their longitudinal association with weight status development in early childhood. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 77. [Google Scholar] [CrossRef] [Green Version]
- Huh, J.; Riggs, N.R.; Spruijt-Metz, D.; Chou, C.P.; Huang, Z.; Pentz, M. Identifying patterns of eating and physical activity in children: A latent class analysis of obesity risk. Obesity 2011, 19, 652–658. [Google Scholar] [CrossRef] [Green Version]
- Santos, L.P.; Assuncao, M.C.F.; Matijasevich, A.; Santos, I.S.; Barros, A.J.D. Dietary intake patterns of children aged 6 years and their association with socioeconomic and demographic characteristics, early feeding practices and body mass index. BMC Public Health 2016, 16, 1055. [Google Scholar] [CrossRef] [Green Version]
- Kudlova, E.; Schneidrova, D. Dietary patterns and their changes in early childhood. Cent. Eur. J. Public Health 2012, 20, 126–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iguacel, I.; Fernandez-Alvira, J.M.; Bammann, K.; De Clercq, B.; Eiben, G.; Gwozdz, W.; Molnar, D.; Pala, V.; Papoutsou, S.; Russo, P.; et al. Associations between social vulnerabilities and dietary patterns in European children: The Identification and prevention of Dietary- and lifestyle-induced health EFfects In Children and infantS (IDEFICS) study. Br. J. Nutr. 2016, 116, 1288–1297. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef] [PubMed]
- Perez-Rodrigo, C.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients 2015, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Leis, R.; Jurado-Castro, J.M.; Llorente-Cantarero, F.J.; Anguita-Ruiz, A.; Iris-Ruperez, A.; Bedoya-Carpente, J.J.; Vazquez-Cobela, R.; Aguilera, C.M.; Bueno, G.; Gil-Campos, M. Cluster Analysis of Physical Activity Patterns, and Relationship with Sedentary Behavior and Healthy Lifestyles in Prepubertal Children: Genobox Cohort. Nutrients 2020, 12, 1288. [Google Scholar] [CrossRef]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, C.P.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Métodos de Frecuencia de consumo alimentario. Rev. Española Nutr. Comunitaria 2015, 21, 45–52. [Google Scholar]
- Madrigal, C.; Soto-Mendez, M.J.; Hernandez-Ruiz, A.; Valero, T.; Avila, J.M.; Ruiz, E.; Villoslada, F.L.; Leis, R.; Martinez de Victoria, E.; Moreno, J.M.; et al. Energy Intake, Macronutrient Profile and Food Sources of Spanish Children Aged One to <10 Years-Results from the EsNuPI Study. Nutrients 2020, 12, 893. [Google Scholar] [CrossRef] [Green Version]
- Camargo, D.M.; Santisteban, S.; Paredes, E.; Florez, M.A.; Bueno, D. Reliability of a questionnaire for measuring physical activity and sedentary behavior in children from preschool to fourth grade. Biomedica 2015, 35, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Butte, N.F.; Watson, K.B.; Ridley, K.; Zakeri, I.F.; McMurray, R.G.; Pfeiffer, K.A.; Crouter, S.E.; Herrmann, S.D.; Bassett, D.R.; Long, A. A youth compendium of physical activities: Activity codes and metabolic intensities. Med. Sci. sports Exerc. 2018, 50, 246. [Google Scholar] [CrossRef]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R.; Group, P.N.G.W. 1. Guidelines on paediatric parenteral nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), supported by the European Society of Paediatric Research (ESPR). J. Pediatr. Gastroenterol. Nutr. 2005, 41, S1–S4. [Google Scholar] [PubMed] [Green Version]
- Schofield, W. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar] [PubMed]
- WHO. Good Maternal Nutrition: The Best Start in Life; World Health Organization: Copenhagen, Denmark, 2016. [Google Scholar]
- Hardwick, J.; Sidnell, A. Infant nutrition–diet between 6 and 24 months, implications for paediatric growth, overweight and obesity. Nutr. Bull. 2014, 39, 354–363. [Google Scholar] [CrossRef] [Green Version]
- Pařízková, J. Dietary habits and nutritional status in adolescents in Central and Eastern Europe. Eur. J. Clin. Nutr. 2000, 54, S36–S40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castetbon, K.; Vernay, M.; Malon, A.; Salanave, B.; Deschamps, V.; Roudier, C.; Oleko, A.; Szego, E.; Hercberg, S. Dietary intake, physical activity and nutritional status in adults: The French nutrition and health survey (ENNS, 2006–2007). Br. J. Nutr. 2009, 102, 733–743. [Google Scholar] [CrossRef] [Green Version]
- Diethelm, K.; Jankovic, N.; Moreno, L.A.; Huybrechts, I.; De Henauw, S.; De Vriendt, T.; Gonzalez-Gross, M.; Leclercq, C.; Gottrand, F.; Gilbert, C.C. Food intake of European adolescents in the light of different food-based dietary guidelines: Results of the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr. 2012, 15, 386–398. [Google Scholar] [CrossRef] [Green Version]
- Wilson, T.A.; Adolph, A.L.; Butte, N.F. Nutrient adequacy and diet quality in non-overweight and overweight Hispanic children of low socioeconomic status: The Viva la Familia Study. J. Am. Diet. Assoc. 2009, 109, 1012–1021. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Bell, L.K.; Golley, R.K.; Daniels, L.; Magarey, A.M. Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity. Eur. J. Clin. Nutr. 2013, 67, 638–645. [Google Scholar] [CrossRef] [Green Version]
- Pereira-da-Silva, L.; Rêgo, C.; Pietrobelli, A. The diet of preschool children in the Mediterranean countries of the European Union: A systematic review. Int. J. Environ. Res. Public Health 2016, 13, 572. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, L.; Shatila, H.; Itani, L.; Hwalla, N.; Jomaa, L.; Naja, F. A traditional dietary pattern is associated with lower odds of overweight and obesity among preschool children in Lebanon: A cross-sectional study. Eur. J. Nutr. 2019, 58, 91–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kafatos, A.; Verhagen, H.; Moschandreas, J.; Apostolaki, I.; Van Westerop, J.J. Mediterranean diet of Crete: Foods and nutrient content. J. Am. Diet. Assoc. 2000, 100, 1487–1493. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Gotsis, E.; Anagnostis, P.; Mariolis, A.; Vlachou, A.; Katsiki, N.; Karagiannis, A. Health benefits of the Mediterranean diet: An update of research over the last 5 years. Angiology 2015, 66, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Delgado, F.; Katsiki, N.; Lopez-Miranda, J.; Perez-Martinez, P. Dietary habits, lipoprotein metabolism and cardiovascular disease: From individual foods to dietary patterns. Crit. Rev. Food Sci. Nutr. 2020, in press. [Google Scholar] [CrossRef]
- Costarelli, V.; Michou, M.; Panagiotakos, D.B.; Lionis, C. Adherence to the Mediterranean diet and weight status in children: The role of parental feeding practices. Int. J. Food Sci. Nutr. 2020, in press. [Google Scholar] [CrossRef]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Gallardo, L.; Garcia-Unanue, J. Weight Status, Adherence to the Mediterranean Diet, and Physical Fitness in Spanish Children and Adolescents: The Active Health Study. Nutrients 2020, 12, 1680. [Google Scholar] [CrossRef]
- Fallani, M.; Amarri, S.; Uusijarvi, A.; Adam, R.; Khanna, S.; Aguilera, M.; Gil, A.; Vieites, J.M.; Norin, E.; Young, D.; et al. Determinants of the human infant intestinal microbiota after the introduction of first complementary foods in infant samples from five European centres. Microbiology 2011, 157, 1385–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arenaza, L.; Medrano, M.; Oses, M.; Huybrechts, I.; Díez, I.; Henriksson, H.; Labayen, I. Dietary determinants of hepatic fat content and insulin resistance in overweight/obese children: A cross-sectional analysis of the Prevention of Diabetes in Kids (PREDIKID) study. Br. J. Nutr. 2019, 121, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Touvier, M.; Lafay, L.; Volatier, J.-L.; Maire, B. Dietary and physical activity patterns in French children are related to overweight and socioeconomic status. J. Nutr. 2008, 138, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Sabbe, D.; De Bourdeaudhuij, I.; Legiest, E.; Maes, L. A cluster-analytical approach towards physical activity and eating habits among 10-year-old children. Health Educ. Res. 2008, 23, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Emmett, P.M.; Newby, P.K.; Northstone, K. Dietary patterns obtained through principal components analysis: The effect of input variable quantification. Br. J. Nutr. 2013, 109, 1881–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Population (n = 1512) | Spanish Reference Cohort (SRS) (n = 740) | Adapted Milk Consumers Cohort (AMS) (n = 772) | ||
|---|---|---|---|---|
| Sex | Boys | 757 | 372 | 385 |
| Girls | 755 | 368 | 387 | |
| Age (years) | 1 to <3 | 471 | 169 | 302 |
| 3 to <6 | 533 | 256 | 277 | |
| 6 to <10 | 508 | 315 | 193 | |
| Food Groups | Spanish Reference Cohort (SRS) | Adapted Milk Consumers Cohort (AMS) | ||||||
|---|---|---|---|---|---|---|---|---|
| Total | 1 to <3 Years | 3 to <6 Years | 6 to <10 Years | Total | 1 to <3 Years | 3 to <6 Years | 6 to <10 Years | |
| (n = 740) | (n = 169) | (n = 256) | (n = 315) | (n = 772) | (n = 302) | (n = 277) | (n = 193) | |
| Milk and dairy products (g/day) | 608.9 ± 308.2 | 738.8 ± 368.6 a | 588.9 ± 275.2 b | 555.5 ± 277.5 b | 682.6 ± 320.6 * | 820.5 ± 342.6 a,* | 604.1 ± 267.7 b | 579.6 ± 276.4 b |
| Cereals (g/day) | 138.5 ± 77.6 | 145.2 ± 84.6 | 134.1 ± 63.7 | 138.5 ± 83.7 | 143.3 ± 80.4 | 158.0 ± 102.5 a | 133.9 ± 64.2 b | 133.9 ± 54.8a b |
| Meat and meat products (g/day) | 94.5 ± 58.1 | 74.3 ± 45.9 a | 93.5 ± 51.6 b | 106.2 ± 65.5 b | 88.6 ± 57.0 * | 74.9 ± 59.1 a | 93.3 ± 52.4 b | 103.1 ± 55.5 b |
| Oils and fats (g/day) | 24.2 ± 19.8 | 21.7 ± 19.8 a | 24.2 ± 18.9 b | 25.7 ± 20.4 b | 23.6 ± 16.6 | 20.8 ± 15.5 a | 23.2 ± 15.0 a | 28.6 ± 19.2 b,* |
| Bakery and pastry (g/day) | 21.4 ± 26.6 | 12.4 ± 20.1 a | 20.8 ± 26.2 b | 26.6 ± 28.6 c | 17.4 ± 26.0 * | 9.7 ± 18.7 a | 18.9 ± 24.3 b | 27.4 ± 33.5 c |
| Fruits (g/day) | 253.1 ± 196.1 | 293.6 ± 216.6 a | 256.5 ± 209.8 ab | 228.5 ± 168.0 b | 264.6 ± 207.9 | 302.4 ± 226.6 a | 243.0 ± 200.1 b | 236.4 ± 178.3 b |
| Vegetables (g/day) | 130.9 ± 106.6 | 177.0 ± 146.5 a | 128.0 ± 97.4 b | 108.6 ± 76.8 c | 149.7 ± 120.7 * | 190.5 ± 153.1 a | 128.4 ± 87.7 b | 116.3 ± 79.1 b |
| Other dairy products (g/day) | 73.5 ± 79.7 | 51.3 ± 85.4 a | 73.2 ± 66.6 b | 85.7 ± 84.0 b | 61.3 ± 77.0 * | 38.5 ± 79.7 a | 71.1 ± 74.9 b | 83.2 ± 65.7 c |
| Sugars and sweets (g/day) | 40.9 ± 39.5 | 30.5 ± 40.8 a | 44.4 ± 42.2 b | 43.6 ± 35.5 b | 34.2 ± 31.8 * | 23.6 ± 25.8 a,* | 37.4 ± 30.6 b | 46.3 ± 36.7 c |
| Ready to cook (g/day) | 23.3 ± 23.8 | 11.8 ± 17.4 a | 22.6 ± 20.8 b | 30.1 ± 26.5 c | 19.4 ± 18.9 * | 9.6 ± 12.8 a | 21.5 ± 16.8 b | 31.5 ± 21.7 c |
| Eggs (g/day) | 23.3 ± 20.5 | 17.9 ± 18.0 a | 24.4 ± 24.3 b | 25.2 ± 17.7 b | 20.7 ± 15.8 * | 16.1 ± 14.0 a | 22.6 ± 16.9 b | 25.1 ± 15.0 b |
| Legumes (g/day) | 21.0 ± 17.6 | 21.1 ± 19.8 | 20.9 ± 14.5 | 21.0 ± 18.6 | 20.6 ± 17.6 | 19.6 ± 18.2 a | 20.1 ± 12.7 ab | 22.9 ± 22.1 b |
| Fish and shellfish (g/day) | 40.1 ± 37.8 | 28.6 ± 38.9 a | 38.9 ± 34.5 b | 47.2 ± 38.2 c | 33.7 ± 28.6 * | 25.8 ± 26.0 a | 36.5 ± 30.6 b | 41.9 ± 26.8 c |
| Beverages (g/day) | 171.9 ± 163.9 | 112.8 ± 138.3 a | 189.2 ± 178.6 b | 189.5 ± 157.1 b | 163.3 ± 181.6 * | 126.8 ± 163.6 a | 156.6 ± 144.3 b,* | 230.0 ± 232.0 c |
| Cereal-based baby foods (g/day) | 1.8 ± 6.3 | 5.9 ± 10.7 a | 1.1 ± 4.7 b | 0.08 ± 0.8 c | 3.4 ± 9.4 * | 7.6 ± 12.6 a,* | 1.2 ± 6.4 b | 0.02 ± 0.2 c |
| Appetizers (g/day) | 14.8 ± 16.0 | 9.3 ± 13.4 a | 16.0 ± 16.5 b | 16.8 ± 16.3 b | 14.0 ± 16.3 * | 9.1 ± 14.1 a | 15.0 ± 14.4 b | 20.5 ± 19.2 c,* |
| Sauces and condiments (g/day) | 4.3 ± 7.6 | 2.4 ± 9.5 a | 4.7 ± 7.7 b | 5.0 ± 6.2 c | 3.7 ± 6.5 * | 1.6 ± 3.9 a | 4.2 ± 6.6 b | 6.4 ± 8.4 c,* |
| Nuts (g/day) | 3.7 ± 5.8 | 1.7 ± 4.5 a | 3.3 ± 4.9 b | 5.1 ± 6.7 c | 3.1 ± 7.7 * | 1.2 ± 5.9 a | 3.2 ± 6.1 b | 5.7 ± 10.8 c |
| Variables | Spanish Reference Cohort (SRS) | Adapted Milk Consumers Cohort(AMS) | ||||||
|---|---|---|---|---|---|---|---|---|
| Total | 1 to <3 Years | 3 to <6 Years | 6 to <10 Years (n = 315) | Total | 1 to <3 Years | 3 to <6 Years | 6 to <10 Years | |
| (n = 740) | (n = 169) | (n = 256) | (n = 772) | (n = 302) | (n = 277) | (n = 193) | ||
| Energy expenditure Moderate–vigorous physical activity (minutes/day) | 402.9 ± 282.0 | 236.4 ± 226.0 a | 392.1 ± 238.5 b | 501.6 ± 298.1 c | 356.8 ± 273.1 * | 235.2 ± 199.1 a | 357.0 ± 196.3 b | 546.4 ± 350.1 c |
| PAL (per 24 h) | 1.6 ± 0.6 | 1.6 ± 0.3 | 1.6 ± 0.2 | 1.6 ± 0.2 | 1.6 ± 0.3 | 1.5 ± 0.3 a | 1.5 ± 0.2 a | 1.6 ± 0.2 b |
| BMI-for-age z-score | 0.6 ± 1.8 | 0.7 ± 1.7 | 0.7 ± 2.1 | 0.4 ± 1.7 | 0.6 ± 1.8 | 1.0 ± 2.1 a | 0.4 ± 1.7 b,* | 0.4 ± 1.4 b |
| Parental education | ||||||||
| a. Low (less than 10 years of education; the primary school or less) | 22.0% (163) | 26.6% (45) | 18.4% (47) | 22.5% (71) | 18.5% (143) | 18.5% (56) | 17.0% (47) | 20.7% (40) |
| b. Medium (12 years of education; higher secondary education) | 44.2% (327) | 36.7% (62) | 45.7% (117) | 47.0% (148) | 42.2% (326) | 39.4% (119) | 44.4% (123) | 43.5% (84) |
| c. High (13 years or more of education; higher vocational, college and university studies) | 33.8% (250) | 36.7% (62) | 35.9% (92) | 30.5% (96) | 39.3% (303) | 42.1% (127) | 38.6% (107) | 35.8% (69) |
| Household income | ||||||||
| a. Low | 9.6% (71) | 13.6% (23) | 6.3% (16) | 10.2% (32) | 9.0% (69) | 8.6% (26) *.* | 9.0% (25) | 9.3% (18) |
| b. Mid-low | 14.3% (106) | 15.4% (26) | 16.4% (42) | 12.1% (38) | 12.7% (98) | 8.9% (27) ** | 13.0% (36) | 18.1% (35) |
| c. High (mid-mid, mid-high and high) | 49.4% (366) | 43.8% (74) | 52.3% (134) | 50.1% (158) | 50.1% (387) | 53.0% (160) ** | 48.4% (134) | 48.2% (93) |
| d.- DK/NA/REF | 26.7% (197) | 27.2% (46) | 25.0% (64) | 27.6% (87) | 28.2% (218) | 29.5% (89) ** | 29.6% (82) | 24.4% (47) |
| SRS 1 to <3 years | AMS 1 to <3 years | ||||||||||||||
| CLU3 (n = 108) | CLU1 (n = 45) | CLU2 (n = 17) | p-Value | CLU3 (n = 155) | CLU 1 (n = 55) | CLU2 (n = 92) | p-Value | ||||||||
| EE-MVPA | 176 ± 152 | 370 ± 313 | 268 ± 197 | <0.001 | 182 ± 145 | 228 ± 188 | 328 ± 247 | <0.001 | |||||||
| PAL | 1.59 ± 0.31 | 1.51 ± 0.32 | 1.58 ± 0.29 | 0.341 | 1.57 ± 0.32 | 1.59 ± 0.27 | 1.44 ± 0.25 | 0.002 | |||||||
| Education | 0.283 | <0.001 | |||||||||||||
| Low | 32 | −29.60% | 9 | −20.00% | 5 | −29.40% | 47 | −30.30% | 4 | −7.27% | 5 | −5.43% | |||
| Medium | 37 | −34.30% | 16 | −35.60% | 9 | −52.90% | 61 | −39.40% | 34 | −61.80% | 24 | −26.10% | |||
| High | 39 | −36.10% | 20 | −44.40% | 3 | −17.60% | 47 | −30.30% | 17 | −30.90% | 63 | −68.50% | |||
| Household Income | 0.849 | . | <0.001 | ||||||||||||
| Low | 17 | −15.70% | 5 | −11.10% | 1 | −5.88% | 21 | −13.50% | 3 | −5.45% | 2 | −2.17% | |||
| Mid-low | 14 | −13.00% | 8 | −17.80% | 4 | −23.50% | 12 | −7.74% | 5 | −9.09% | 10 | −10.90% | |||
| High | 46 | −42.60% | 20 | −44.40% | 8 | −47.10% | 82 | −52.90% | 36 | −65.50% | 42 | −45.70% | |||
| DK/REF | 31 | −28.70% | 12 | −26.70% | 4 | −23.50% | 40 | −25.80% | 11 | −20.00% | 38 | −41.30% | |||
| Z-BMI-for-age | 2.28 ± 0.62 | 2.42 ± 0.54 | 2.65 ± 0.49 | 0.04 | 2.41 ± 0.60 | 2.33 ± 0.51 | 2.37 ± 0.61 | 0.675 | |||||||
| SRS 3 to <6 years | AMS 3 to <6 years | ||||||||||||||
| CLU1 (n = 142) | CLU3 (n = 76) | CLU2 (n = 38) | p-Value | CLU1 (n = 116) | CLU2 (n = 99) | CLU3 (n = 62) | p-Value | ||||||||
| EE MVPA | 372 ± 249 | 447 ± 233 | 356 ± 191 | 0.053 | 318 ± 186 | 387 ± 209 | 382 ± 185 | 0.017 | |||||||
| PAL | 1.6 ± 0.21 | 1.52 ± 0.22 | 1.49 ± 0.25 | 0.006 | 1.49 ± 0.22 | 1.56 ± 0.21 | 1.57 ± 0.23 | 0.014 | |||||||
| Education | 0.139 | 0.063 | |||||||||||||
| Low | 33 | −23.20% | 10 | −13.20% | 4 | −10.50% | 17 | −14.70% | 24 | −24.20% | 6 | −9.68% | |||
| Medium | 59 | −41.50% | 41 | −53.90% | 17 | −44.70% | 52 | −44.80% | 45 | −45.50% | 26 | −41.90% | |||
| High | 50 | −35.20% | 25 | −32.90% | 17 | −44.70% | 47 | −40.50% | 30 | −30.30% | 30 | −48.40% | |||
| Household Income | <0.001 | 0.168 | |||||||||||||
| Low | 11 | −7.75% | 4 | −5.26% | 1 | −2.63% | 12 | −10.30% | 6 | −6.06% | 7 | −11.30% | |||
| Mid-low | 19 | −13.40% | 18 | −23.70% | 5 | −13.20% | 11 | −9.48% | 13 | −13.10% | 12 | −19.40% | |||
| High | 63 | −44.40% | 43 | −56.60% | 28 | −73.70% | 62 | −53.40% | 43 | −43.40% | 29 | −46.80% | |||
| DK/REF | 49 | −34.50% | 11 | −14.50% | 4 | −10.50% | 31 | −26.70% | 37 | −37.40% | 14 | −22.60% | |||
| Z-BMI-for-age | 2.36 ± 0.59 | 2.21 ± 0.50 | 2.29 ± 0.46 | 0.158 | 2.23 ± 0.57 | 2.24 ± 0.52 | 2.11 ± 0.48 | 0.266 | |||||||
| SRS 6 to <10 years | AMS 6 to <10 years | ||||||||||||||
| CLU2 (n = 45) | CLU1 (n = 95) | CLU3 (n = 175) | p-Value | CLU1 (n = 110) | CLU3 (n = 52) | CLU2 (n = 31) | p-Value | ||||||||
| EE MVPA | 352 ± 173 | 474 ± 276 | 555 ± 320 | <0.001 | 484 ± 322 | 619 ± 347 | 644 ± 410 | 0.016 | |||||||
| PAL | 1.61 ± 0.21 | 1.55 ± 0.23 | 1.61 ± 0.21 | 0.051 | 1.58 ± 0.20 | 1.58 ± 0.17 | 1.75 ± 0.22 | <0.001 | |||||||
| Education | <0.001 | 0.01 | |||||||||||||
| Low | 34 | −75.60% | 15 | −15.80% | 22 | −12.60% | 21 | −19.10% | 14 | −26.90% | 5 | −16.10% | |||
| Medium | 8 | −17.80% | 51 | −53.70% | 89 | −50.90% | 39 | −35.50% | 29 | −55.80% | 16 | −51.60% | |||
| High | 3 | −6.67% | 29 | −30.50% | 64 | −36.60% | 50 | −45.50% | 9 | −17.30% | 10 | −32.30% | |||
| Household Income | <0.001 | 0.387 | |||||||||||||
| Low | 25 | −55.60% | 6 | −6.32% | 1 | −0.57% | 11 | −10.00% | 6 | −11.50% | 1 | −3.23% | |||
| Mid-low | 5 | −11.10% | 12 | −12.60% | 21 | −12.00% | 18 | −16.40% | 10 | −19.20% | 7 | −22.60% | |||
| High | 11 | −24.40% | 51 | −53.70% | 96 | −54.90% | 49 | −44.50% | 25 | −48.10% | 19 | −61.30% | |||
| DK/REF | 4 | −8.89% | 26 | −27.40% | 57 | −32.60% | 32 | −29.10% | 11 | −21.20% | 4 | −12.90% | |||
| Z-BMI-for-age | 2.42 ± 0.50 | 2.24 ± 0.61 | 2.29 ± 0.55 | 0.208 | 2.3 ± 0.57 | 2.42 ± 0.50 | 1.97 ± 0.60 | 0.002 | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plaza-Díaz, J.; Molina-Montes, E.; Soto-Méndez, M.J.; Madrigal, C.; Hernández-Ruiz, Á.; Valero, T.; Lara Villoslada, F.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Clustering of Dietary Patterns and Lifestyles Among Spanish Children in the EsNuPI Study †. Nutrients 2020, 12, 2536. https://doi.org/10.3390/nu12092536
Plaza-Díaz J, Molina-Montes E, Soto-Méndez MJ, Madrigal C, Hernández-Ruiz Á, Valero T, Lara Villoslada F, Leis R, Martínez de Victoria E, Moreno JM, et al. Clustering of Dietary Patterns and Lifestyles Among Spanish Children in the EsNuPI Study †. Nutrients. 2020; 12(9):2536. https://doi.org/10.3390/nu12092536
Chicago/Turabian StylePlaza-Díaz, Julio, Esther Molina-Montes, María José Soto-Méndez, Casandra Madrigal, Ángela Hernández-Ruiz, Teresa Valero, Federico Lara Villoslada, Rosaura Leis, Emilio Martínez de Victoria, José Manuel Moreno, and et al. 2020. "Clustering of Dietary Patterns and Lifestyles Among Spanish Children in the EsNuPI Study †" Nutrients 12, no. 9: 2536. https://doi.org/10.3390/nu12092536