Effect of Omega-3 Long Chain Polyunsaturated Fatty Acids (n-3 LCPUFA) Supplementation on Cognition in Children and Adolescents: A Systematic Literature Review with a Focus on n-3 LCPUFA Blood Values and Dose of DHA and EPA



Abstract
:1. Introduction
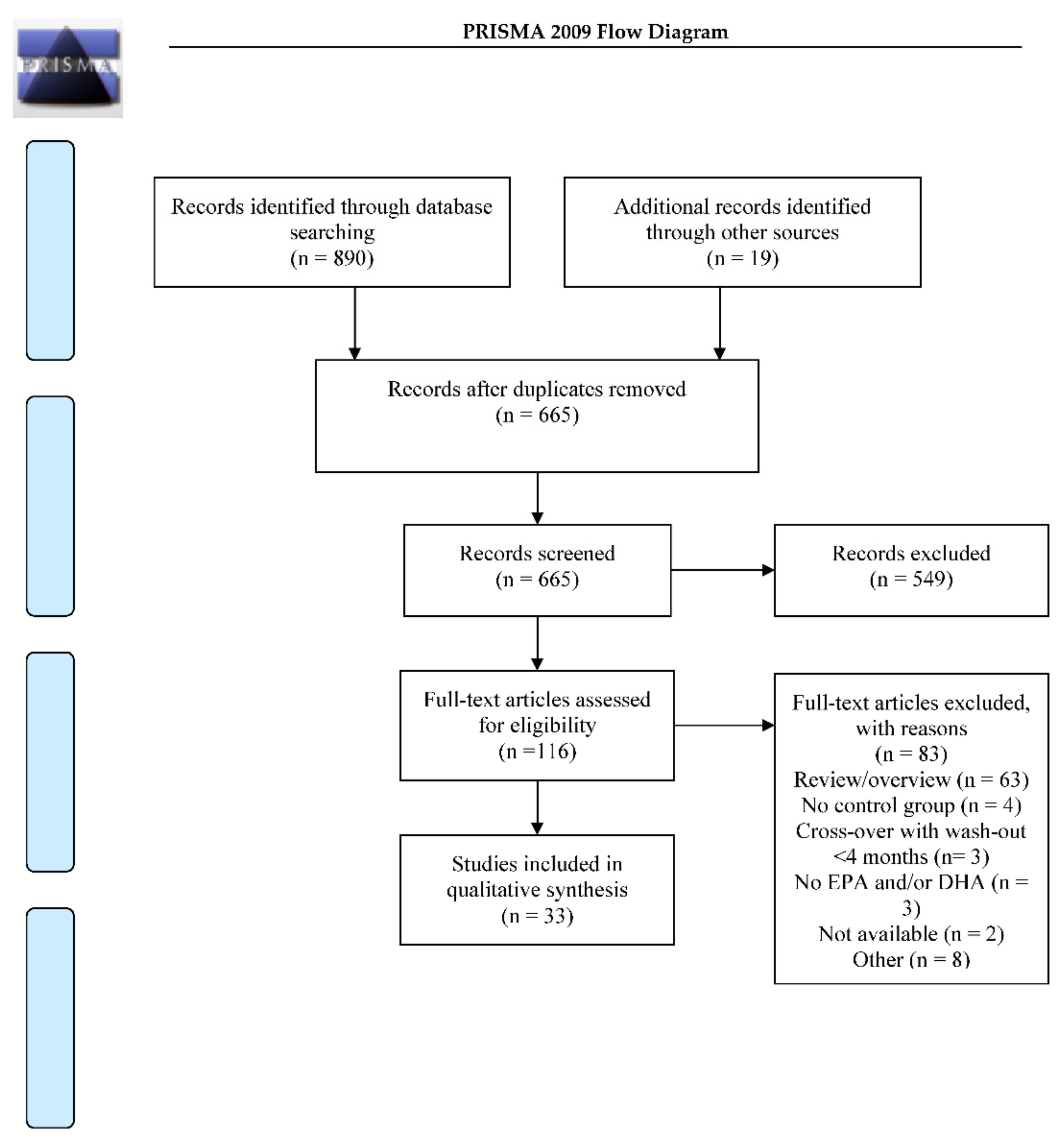
2. Materials and Methods
3. Results
3.1. Included Studies
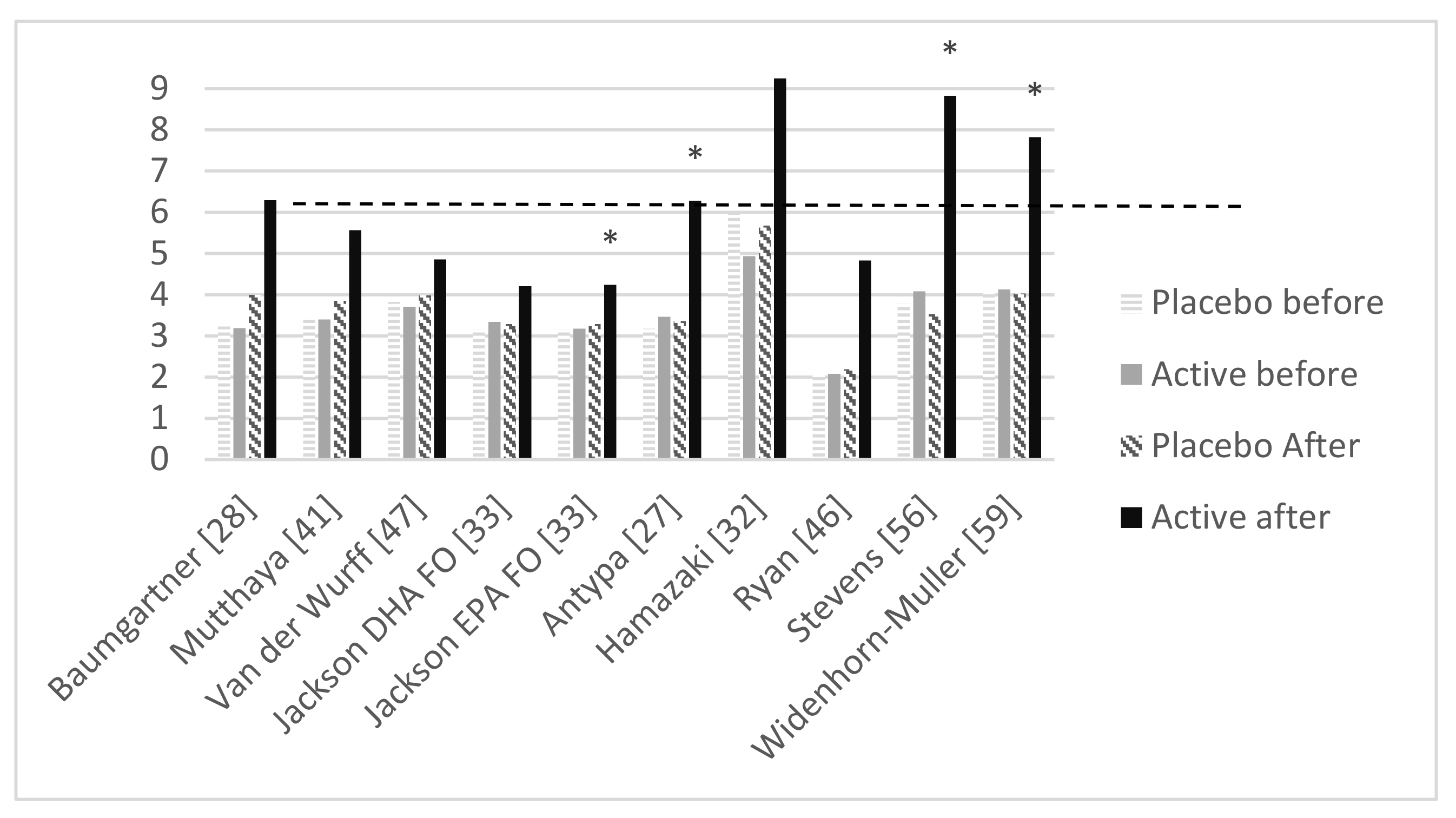
3.2. Omega-3 Index Equivalence
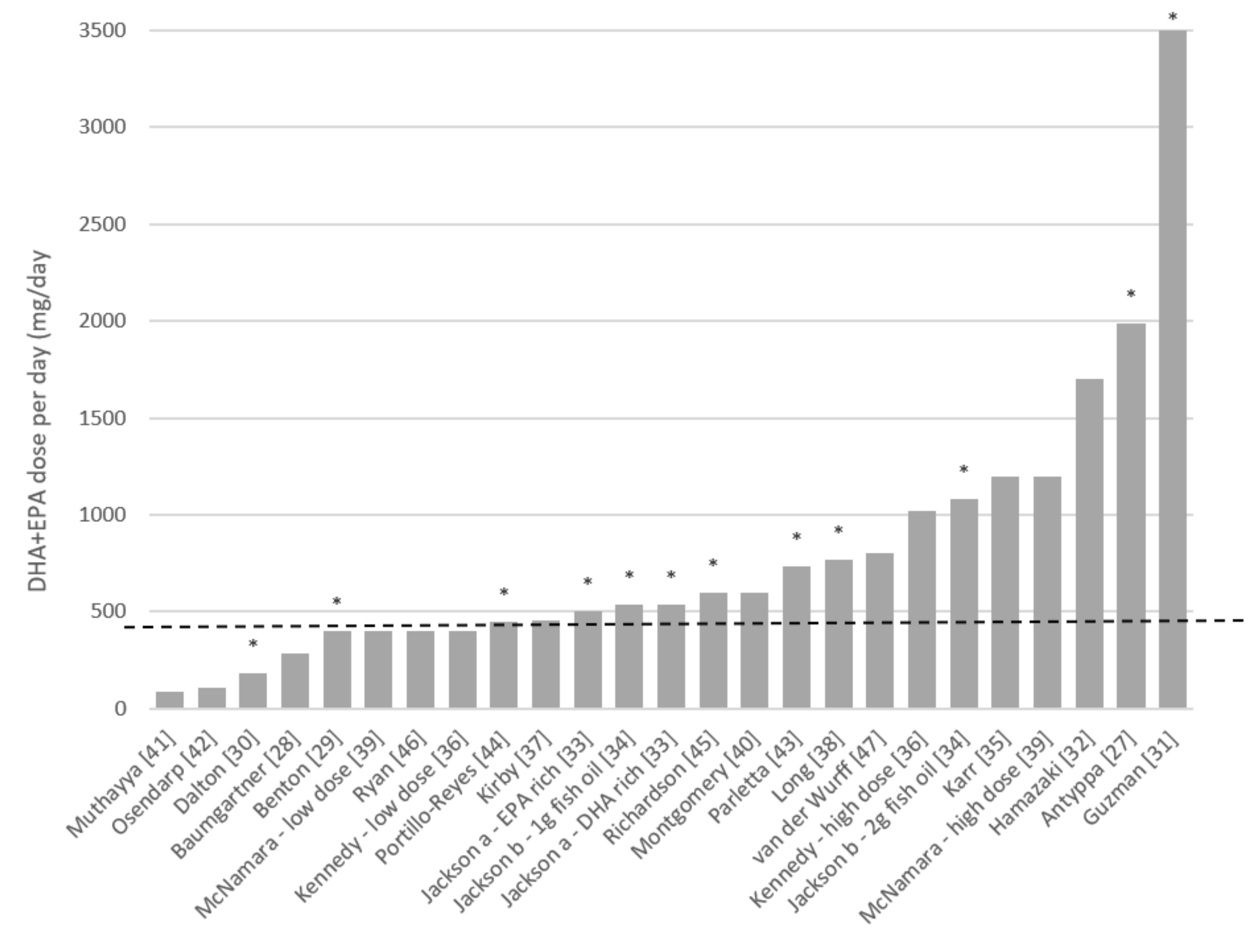
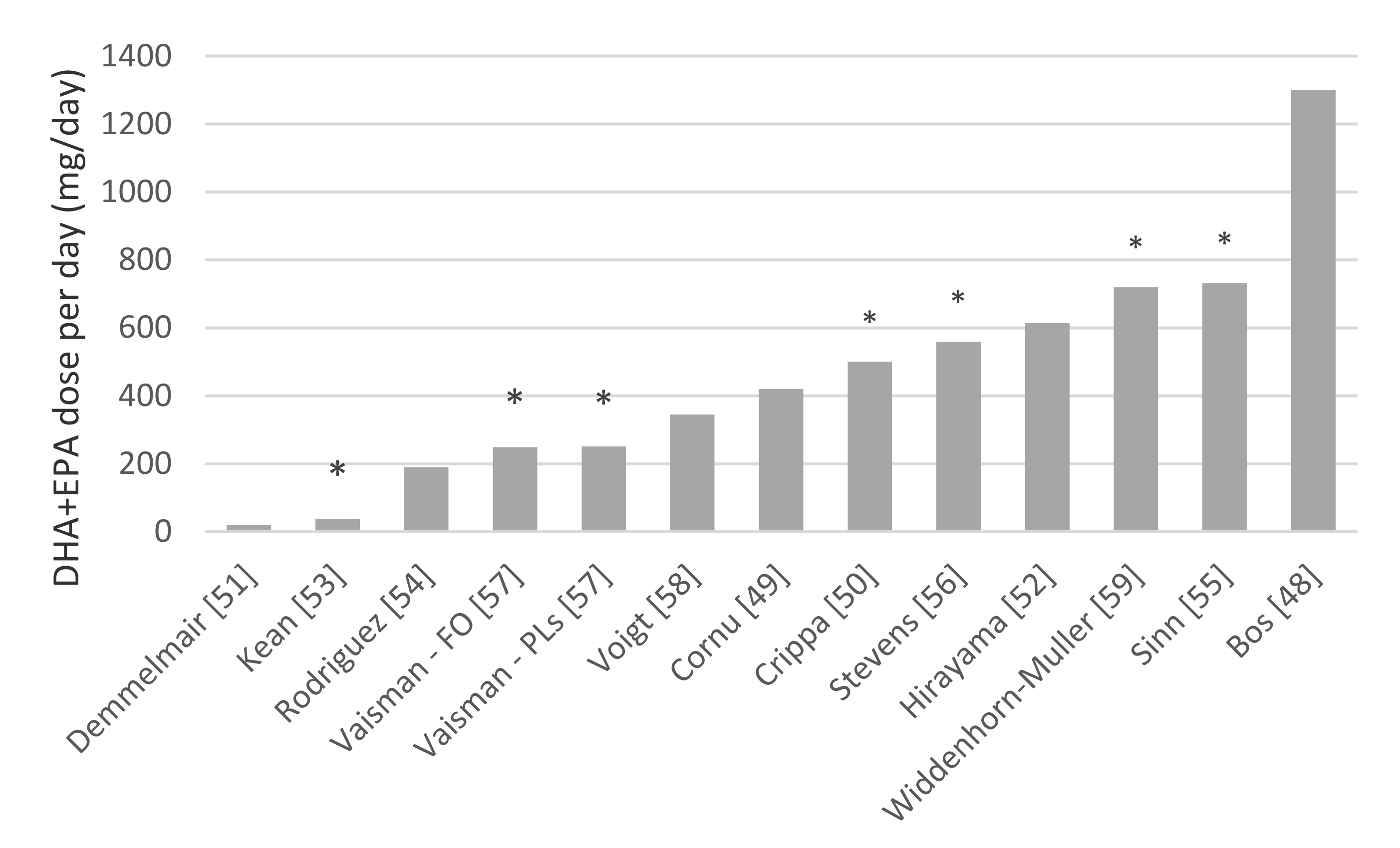
3.3. Supplementation Dose
3.4. Children and Adolescents with a Disease or Disorder
4. Discussion
4.1. Omega-3 Index Equivalence
4.2. Supplementation Dose in Typically Developing Children and Adolescents
4.3. Supplementation Dose in Children and Adolescents with a Disease or Disorder
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PUBMED Search Strategy | (((“fatty acid”[Title/Abstract]) OR “fatty acids”[Title/Abstract]) OR “omega-3”[Title/Abstract]) OR “omega-6”[Title/Abstract]) OR pufa[Title/Abstract]) OR lcpufa[Title/Abstract]) OR mufa[Title/Abstract]) OR fish oil*[Title/Abstract]))) AND ((child [Title/Abstract] OR children [Title/Abstract] OR childhood [Title/Abstract] OR kid [Title/Abstract] or kids [Title/Abstract] OR girl* [Title/Abstract] OR boy* [Title/Abstract] OR teenage* [Title/Abstract] OR youth* [Title/Abstract] OR youngster* [Title/Abstract] OR preschool* [Title/Abstract] OR pre-school* [Title/Abstract] OR kindergarten* [Title/Abstract] OR “elementary school” [Title/Abstract] OR elementary-school [Title/Abstract] OR juvenile* [Title/Abstract] OR minors [Title/Abstract] OR minor [Title/Abstract] OR pediatric* [Title/Abstract] OR paediatric* [Title/Abstract] OR schoolchild*[Title/Abstract] OR toddler*[Title/Abstract] OR teen [Title/Abstract] OR teens [Title/Abstract] OR child, preschool [MeSH terms] OR child [MeSH terms])) AND (cognit*)Searched 03–07-2019–421 hits | |
| Web of Science Search Strategy | #1 | (TS = (“fatty acid” OR “fatty acids” OR “omega-3” OR “omega-6” or pufa OR lcpufa OR mufa OR “fish oil*”)) Indexes = SCI-EXPANDED, SSCI, A&HCI, ESCI Timespan = All years |
| #2 | (TS = (child OR children OR childhood OR kid OR kids OR girl* OR boy* OR teenage* OR youth* OR youngster* OR preschool* OR pre-school* OR kindergarten* OR “elementary school” OR elementary-school OR juvenile* OR minors OR minor OR childhood OR pediatric* OR paediatric* OR schoolchild OR toddler* OR teen OR teens)) Indexes = SCI-EXPANDED, SSCI, A&HCI, ESCI Timespan = All years | |
| #3 | (TS = (cognit*)) Indexes = SCI-EXPANDED, SSCI, A&HCI, ESCI Timespan = All years #3 AND #2 AND #1 Indexes = SCI-EXPANDED, SSCI, A&HCI, ESCI Timespan = All years Searched 03-07-2019-469 hits | |
References
- Hu, Y.; Hu, F.B.; Manson, J.E. Marine Omega-3 Supplementation and Cardiovascular Disease: An Updated Meta-Analysis of 13 Randomized Controlled Trials Involving 127 477 Participants. J. Am. Heart Assoc. 2019, 8, e013543. [Google Scholar] [CrossRef] [PubMed]
- Appleton, K.M.; Rogers, P.J.; Ness, A.R. Updated Systematic Review and Meta-Analysis of the Effects of N-3 Long-Chain Polyunsaturated Fatty Acids on Depressed Mood. Am. J.Clin. Nutr. 2010, 91, 757–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, P.; Gomersall, J.C.; Gould, J.F.; Shepherd, E.; Olsen, S.F.; Makrides, M. Omega-3 Fatty Acid Addition During Pregnancy. Cochrane Database Syst. Rev. 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- Sydenham, E.; Dangour Alan, D.; Lim, W.-S. Omega 3 Fatty Acid for the Prevention of Cognitive Decline and Dementia. Cochrane Database Syst. Rev. 2012, 6. [Google Scholar] [CrossRef] [Green Version]
- Stonehouse, W. Does Consumption of LC Omega-3 Pufa Enhance Cognitive Performance in Healthy School-Aged Children and Throughout Adulthood? Evidence From Clinical Trials. Nutrients 2014, 6, 2730–2758. [Google Scholar] [CrossRef] [Green Version]
- Agostoni, C.; Nobile, M.; Ciappolino, V.; Delvecchio, G.; Tesei, A.; Turolo, S.; Crippa, A.; Mazzocchi, A.; Altamura, C.A.; Brambilla, P. The Role of Omega-3 Fatty Acids in Developmental Psychopathology: A Systematic Review on Early Psychosis, Autism, and ADHD. Int. J. Mol. Sci. 2017, 18, 2608. [Google Scholar] [CrossRef] [Green Version]
- Parletta, N.; Milte, C.M.; Meyer, B.J. Nutritional Modulation of Cognitive Function and Mental Health. J. Nutr. Biochem. 2013, 24, 725–743. [Google Scholar] [CrossRef] [Green Version]
- Bazinet, R.P.; Layé, S. Polyunsaturated Fatty Acids and Their Metabolites in Brain Function and Disease. Nat. Rev. Neurosci. 2014, 15, 771–785. [Google Scholar] [CrossRef]
- Dyall, S.C. Long-Chain Omega-3 Fatty Acids and the Brain: A Review of the Independent and Shared Effects of EPA, DPA and DHA. Front. Aging Neurosci. 2015, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Kuratko, C.N.; Barrett, E.C.; Nelson, E.B.; Salem, N. The Relationship of Docosahexaenoic Acid (DHA) with Learning and Behavior in Healthy Children: A review. Nutrients 2013, 5, 2777–2810. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.; Connock, M. Effects of Oily Fish/Omega-3 Fatty Acids on Behavioural, Cogitative and Educational Outcomes of Normal School Children: A Systematic Review. Dep. Public Health Epidemiol. Rep. 2007, 58. [Google Scholar]
- Frensham, L.J.; Bryan, J.; Parletta, N. Influences of Micronutrient and Omega-3 Fatty Acid Supplementation on Cognition, Learning, and Behavior: Methodological Considerations and Implications for Children and Adolescents in Developed Societies. Nutr. Rev. 2012, 70, 594–610. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.S.; Astwood, J.D.; Gautier, S.; Kuratko, C.N.; Nelson, E.B.; Salem, N., Jr. Effects of Long-Chain Polyunsaturated Fatty Acid Supplementation on Neurodevelopment in Childhood: A Review of Human Studies. Prostaglandins Leukot. Essent. Fat. Acids 2010, 82, 305–314. [Google Scholar] [CrossRef] [PubMed]
- McCann, J.; Ames, B.N. Is Docosahexaenoic Acid, an N-3 Long-Chain Polyunsaturated Fatty Acid, Required for Development of Normal Brain Function? an Overview of Evidence From Cognitive and Behavioral Tests in Humans and Animals. Am. J. Clin. Nutr. 2005, 82, 281–295. [Google Scholar] [CrossRef] [PubMed]
- Eilander, A.; Hundscheid, D.C.; Osendarp, S.J.; Transler, C.; Zock, P.L. Effects of N-3 Long Chain Polyunsaturated Fatty Acid Supplementation on Visual and Cognitive Development Throughout Childhood: A Review of Human Studies. Prostaglandins Leukot. Essent. Fat. Acids 2007, 76, 189–203. [Google Scholar] [CrossRef] [PubMed]
- Karr, J.E.; Alexander, J.E.; Winningham, R.G. Omega-3 Polyunsaturated Fatty Acids and Cognition Throughout the Lifespan: A Review. Nutr. Neurosci. 2011, 14, 216–225. [Google Scholar] [CrossRef]
- Cooper, R.E.; Tye, C.; Kuntsi, J.; Vassos, E.; Asherson, P. Omega-3 Polyunsaturated Fatty Acid Supplementation and Cognition: A Systematic Review and Meta-Analysis. J. Psychopharmacol. 2015, 29, 753–763. [Google Scholar] [CrossRef]
- Jiao, J.; Li, Q.; Chu, J.; Zeng, W.; Yang, M.; Zhu, S. Effect of N- 3 Pufa Supplementation on Cognitive Function Throughout the Life Span From Infancy to Old Age: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2014, 100, 1422–1436. [Google Scholar] [CrossRef] [Green Version]
- Kirby, A.; Woodward, A.; Jackson, S. Benefits of Omega-3 Supplementation for Schoolchildren: Review of the Current Evidence. Br. Educ. Res. J. 2010, 36, 699–732. [Google Scholar] [CrossRef]
- Meyer, B.J.; De Groot, R.H. Effects of Omega-3 Long Chain Polyunsaturated Fatty Acid Supplementation on Cardiovascular Mortality: The Importance of the Dose of DHA. Nutrients 2017, 9, 1305. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.S.; Von Schacky, C. The Omega-3 Index: A New Risk Factor for Death From Coronary Heart Disease? Prev. Med. 2004, 39, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Milte, C.M.; Sinn, N.; Howe, P.R.C. Polyunsaturated Fatty Acid Status in Attention Deficit Hyperactivity Disorder, Depression, and Alzheimer’s Disease: Towards an Omega-3 Index for Mental Health? Nutr. Rev. 2009, 67, 573–590. [Google Scholar] [CrossRef] [PubMed]
- Emery, S.; Häberling, I.; Berger, G.; Walitza, S.; Schmeck, K.; Albert, T.; Baumgartner, N.; Strumberger, M.; Albermann, M.; Drechsler, R. Omega-3 And Its Domain-Specific Effects on Cognitive Test Performance in Youths: A Meta-Analysis. Neurosci. Biobehav. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Griffith, L.; van den Heuvel, E.; Fortier, I.; Hofer, S.; Raina, P.; Sohel, N.; Payette, H.; Wolfson, C.; Belleville, S. Harmonization of Cognitive Measures in Individual Participant Data and Aggregate Data Meta-Analysis; Agency for Healthcare Research and Quality: Washington, DC, USA, 2013. [Google Scholar]
- Gogtay, N.; Giedd, J.N.; Lusk, L.; Hayashi, K.M.; Greenstein, D.; Vaituzis, A.C.; Nugent, T.F.; Herman, D.H.; Clasen, L.S.; Toga, A.W.; et al. Dynamic Mapping of Human Cortical Development During Childhood Through Early Adulthood. Proc. Natl. Acad. Sci. USA 2004, 101, 8174–8179. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta Analyses: The Prisma Statement. PLoS Med. 2009, 6, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Antypa, N.; Van der Does, A.; Smelt, A.; Rogers, R. Omega-3 Fatty Acids (Fish-Oil) and Depression-Related Cognition in Healthy Volunteers. J. Psychopharmacol. 2009, 23, 831–840. [Google Scholar] [CrossRef]
- Baumgartner, J.; Smuts, C.M.; Malan, L.; Kvalsvig, J.; van Stuijvenberg, M.E.; Hurrell, R.F.; Zimmermann, M.B. Effects of Iron and N-3 Fatty Acid Supplementation, Alone and in Combination, on Cognition in School Children: A Randomized, Double-Blind, Placebo-Controlled Intervention in South Africa. Am. J. Clin. Nutr. 2012, 96, 1327–1338. [Google Scholar] [CrossRef] [Green Version]
- Benton, D.; Donohoe, R.; Clayton, D.; Long, S. Supplementation with DHA and the Psychological Functioning of Young Adults. Br. J. Nutr. 2013, 109, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Dalton, A.; Wolmarans, P.; Witthuhn, R.C.; van Stuijvenberg, M.E.; Swanevelder, S.A.; Smuts, C.M. A Randomised Control Trial in Schoolchildren Showed Improvement in Cognitive Function After Consuming a Bread Spread, Containing Fish Flour From a Marine Source. Prostaglandins Leukot. Essent. Fatty Acids 2009, 80, 143–149. [Google Scholar] [CrossRef]
- Guzmán, J.F.; Esteve, H.; Pablos, C.; Pablos, A.; Blasco, C.; Villegas, J.A. Dha-Rich Fish Oil Improves Complex Reaction Time in Female Elite Soccer Players. J. Sports Sci. Med. 2011, 10, 301. [Google Scholar]
- Hamazaki, T.; Sawazaki, S.; Itomura, M.; Asaoka, E.; Nagao, Y.; Nishimura, N.; Yazawa, K.; Kuwamori, T.; Kobayashi, M. The Effect of Docosahexaenoic Acid on Aggression in Young Adults. a Placebo-Controlled Double-Blind Study. J. Clin. Investig. 1996, 97, 1129–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, P.A.; Deary, M.E.; Reay, J.L.; Scholey, A.B.; Kennedy, D.O. No Effect of 12 Weeks’ Supplementation with 1 G DHA-Rich or EPA-Rich Fish Oil on Cognitive Function or Mood in Healthy Young Adults Aged 18–35 Years. Br. J. Nutr. 2012, 107, 1232–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, P.A.; Reay, J.L.; Scholey, A.B.; Kennedy, D.O. Docosahexaenoic Acid-Rich Fish Oil Modulates the Cerebral Hemodynamic Response to Cognitive Tasks in Healthy Young Adults. Biol. Psychol. 2012, 89, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Karr, J.E.; Grindstaff, T.R.; Alexander, J.E. Omega-3 Polyunsaturated Fatty Acids and Cognition in a College-Aged Population. Exp. Clin. Psychopharmacol. 2012, 20, 236–242. [Google Scholar] [CrossRef]
- Kennedy, D.O.; Jackson, P.A.; Elliott, J.M.; Scholey, A.B.; Robertson, B.C.; Greer, J.; Tiplady, B.; Buchanan, T.; Haskell, C.F. Cognitive and Mood Effects of 8 Weeks’ Supplementation with 400 mg or 1000 mg of the Omega-3 Essential Fatty Acid Docosahexaenoic Acid (DHA) in Healthy Children Aged 10-12 Years. Nutr. Neurosci. 2009, 12, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Kirby, A.; Woodward, A.; Jackson, S.; Wang, Y.; Crawford, M.A. A Double-Blind, Placebo-Controlled Study Investigating the Effects of Omega-3 Supplementation in Children Aged 8-10 Years From a Mainstream School Population. Res. Dev. Disabil. 2010, 31, 718–730. [Google Scholar] [CrossRef]
- Long, S.J.; Benton, D. A Double-Blind Trial of the Effect of Docosahexaenoic Acid and Vitamin and Mineral Supplementation on Aggression, Impulsivity, and Stress. Hum. Psychopharmacol. Clin. Exp. 2013, 28, 238–247. [Google Scholar] [CrossRef]
- McNamara, R.K.; Able, J.; Jandacek, R.; Rider, T.; Tso, P.; Eliassen, J.C.; Alfieri, D.; Weber, W.; Jarvis, K.; DelBello, M.P.; et al. Docosahexaenoic Acid Supplementation Increases Prefrontal Cortex Activation During Sustained Attention in Healthy Boys: A Placebo-Controlled, Dose-Ranging, Functional Magnetic Resonance Imaging Study. Am. J. Clin. Nutr. 2010, 91, 1060–1067. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, P.; Spreckelsen, T.F.; Burton, A.; Burton, J.R.; Richardson, A.J. Docosahexaenoic Acid for Reading, Working Memory and Behavior in UK Children Aged 7-9: A Randomized Controlled Trial for Replication (the Dolab II Study). PLoS ONE 2018, 13, e0192909. [Google Scholar] [CrossRef] [Green Version]
- Muthayya, S.; Eilander, A.; Transler, C.; Thomas, T.; van der Knaap, H.C.; Srinivasan, K.; van Klinken, B.J.; Osendarp, S.J.; Kurpad, A.V. Effect of Fortification With Multiple Micronutrients and N-3 Fatty Acids on Growth and Cognitive Performance in Indian Schoolchildren: The Champion (Children’s Health and Mental Performance Influenced by Optimal Nutrition) Study. Am. J. Clin. Nutr. 2009, 89, 1766–1775. [Google Scholar] [CrossRef] [Green Version]
- Osendarp, S.J.; Baghurst, K.I.; Bryan, J.; Calvaresi, E.; Hughes, D.; Hussaini, M.; Karyadi, S.J.; van Klinken, B.J.; van der Knaap, H.C.; Lukito, W.; et al. Effect of a 12-MO Micronutrient Intervention on Learning and Memory in Well-Nourished and Marginally Nourished School-Aged Children: 2 Parallel, Randomized, Placebo-Controlled Studies in Australia and Indonesia. Am. J. Clin. Nutr. 2007, 86, 1082–1093. [Google Scholar] [PubMed] [Green Version]
- Parletta, N.; Cooper, P.; Gent, D.N.; Petkov, J.; O’Dea, K. Effects of Fish Oil Supplementation on Learning and Behaviour of Children From Australian Indigenous Remote Community Schools: A Randomised Controlled Trial. Prostaglandins Leukot. Essent. Fatty Acids 2013, 89, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Portillo-Reyes, V.; Perez-Garcia, M.; Loya-Mendez, Y.; Puente, A.E. Clinical Significance of Neuropsychological Improvement After Supplementation With Omega-3 in 8-12 Years Old Malnourished Mexican Children: A Randomized, Double-Blind, Placebo and Treatment Clinical Trial. Res. Dev. Disabil. 2014, 35, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.J.; Burton, J.R.; Sewell, R.P.; Spreckelsen, T.F.; Montgomery, P. Docosahexaenoic Acid for Reading, Cognition and Behavior in Children Aged 7-9 Years: A Randomized, Controlled Trial (the Dolab Study). PLoS ONE 2012, 7, e43909. [Google Scholar] [CrossRef]
- Ryan, A.S.; Nelson, E.B. Assessing the Effect of Docosahexaenoic Acid on Cognitive Functions in Healthy, Preschool Children: A Randomized, Placebo-Controlled, Double-Blind Study. Clin. Pediatrics 2008, 47, 355–362. [Google Scholar] [CrossRef]
- van der Wurff, I.S.; von Schacky, C.; Bergeland, T.; Leontjevas, R.; Zeegers, M.P.; Jolles, J.; Kirschner, P.A.; de Groot, R.H. Effect of 1 Year Krill Oil Supplementation on Cognitive Achievement of Dutch Adolescents: A Double-Blind Randomized Controlled Trial. Nutrients 2019, 11, 1230. [Google Scholar] [CrossRef] [Green Version]
- Bos, D.J.; Oranje, B.; Veerhoek, E.S.; Van Diepen, R.M.; Weusten, J.M.; Demmelmair, H.; Koletzko, B.; de Sain-van der Velden, M.G.; Eilander, A.; Hoeksma, M.; et al. Reduced Symptoms of Inattention After Dietary Omega-3 Fatty Acid Supplementation in Boys with and without Attention Deficit/Hyperactivity Disorder. Neuropsychopharmacology 2015, 40, 2298–2306. [Google Scholar] [CrossRef] [Green Version]
- Cornu, C.; Mercier, C.; Ginhoux, T.; Masson, S.; Mouchet, J.; Nony, P.; Kassai, B.; Laudy, V.; Berquin, P.; Franc, N. A Double-Blind Placebo-Controlled Randomised Trial of Omega-3 Supplementation in Children with Moderate ADHD Symptoms. Eur. Child Adolesc. Psychiatry 2018, 27, 377–384. [Google Scholar] [CrossRef]
- Crippa, A.; Tesei, A.; Sangiorgio, F.; Salandi, A.; Trabattoni, S.; Grazioli, S.; Agostoni, C.; Molteni, M.; Nobile, M. Behavioral and Cognitive Effects of Docosahexaenoic Acid in Drug-Naive Children with Attention-Deficit/Hyperactivity Disorder: A Randomized, Placebo-Controlled Clinical Trial. Eur. Child Adolesc. Psychiatry 2019, 28, 571–583. [Google Scholar] [CrossRef]
- Demmelmair, H.; MacDonald, A.; Kotzaeridou, U.; Burgard, P.; Gonzalez-Lamuno, D.; Verduci, E.; Ersoy, M.; Gokcay, G.; Alyanak, B.; Reischl, E.; et al. Determinants of Plasma Docosahexaenoic Acid Levels and Their Relationship to Neurological and Cognitive Functions in Pku Patients: A Double Blind Randomized Supplementation Study. Nutrients 2018, 10, 1944. [Google Scholar] [CrossRef] [Green Version]
- Hirayama, S.; Hamazaki, T.; Terasawa, K. Effect of Docosahexaenoic Acid-Containing Food Administration on Symptoms of Attention-Deficit/Hyperactivity Disorder—A Placebo-Controlled Double-Blind Study. Eur. J. Clin. Nutr. 2004, 58, 467. [Google Scholar] [CrossRef] [PubMed]
- Kean, J.D.; Sarris, J.; Scholey, A.; Silberstein, R.; Downey, L.A.; Stough, C. Reduced Inattention and Hyperactivity and Improved Cognition After Marine Oil Extract (Pcso-524a (R)) Supplementation in Children and Adolescents With Clinical and Subclinical Symptoms of Attention-Deficit Hyperactivity Disorder (ADHD): A Randomised, Double-Blind, Placebo-Controlled Trial. Psychopharmacology 2017, 234, 403–420. [Google Scholar] [PubMed] [Green Version]
- Rodriguez, C.; Garcia, T.; Areces, D.; Fernandez, E.; Garcia-Noriega, M.; Domingo, J.C. Supplementation with High-Content Docosahexaenoic Acid Triglyceride in Attention-Deficit Hyperactivity Disorder: A Randomized Double-Blind Placebo-Controlled Trial. Neuropsychiatr. Dis. Treat. 2019, 15, 1193–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinn, N.; Bryan, J.; Wilson, C. Cognitive Effects of Polyunsaturated Fatty Acids in Children With Attention Deficit Hyperactivity Disorder Symptoms: A Randomised Controlled Trial. Prostaglandins Leukot. Essent. Fatty Acids 2008, 78, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.; Zhang, W.; Peck, L.; Kuczek, T.; Grevstad, N.; Mahon, A.; Zentall, S.S.; Eugene Arnold, L.; Burgess, J.R. EFA Supplementation in Children with Inattention, Hyperactivity, and Other Disruptive Behaviors. Lipids 2003, 38, 1007–1021. [Google Scholar] [CrossRef] [PubMed]
- Vaisman, N.; Kaysar, N.; Zaruk-Adasha, Y.; Pelled, D.; Brichon, G.; Zwingelstein, G.; Bodennec, J. Correlation Between Changes in Blood Fatty Acid Composition and Visual Sustained Attention Performance in Children with Inattention: Effect of Dietary N−3 Fatty Acids Containing Phospholipids. Am. J. Clin. Nutr. 2008, 87, 1170–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voigt, R.G.; Llorente, A.M.; Jensen, C.L.; Fraley, J.K.; Berretta, M.C.; Heird, W.C. A Randomized, Double-Blind, Placebo-Controlled Trial of Docosahexaenoic Acid Supplementation in Children with Attention-Deficit/Hyperactivity Disorder. J. Pediatrics 2001, 139, 189–196. [Google Scholar] [CrossRef] [Green Version]
- Widenhorn-Muller, K.; Schwanda, S.; Scholz, E.; Spitzer, M.; Bode, H. Effect of Supplementation With Long-Chain Omega-3 Polyunsaturated Fatty Acids on Behavior and Cognition in Children with Attention Deficit/Hyperactivity Disorder (ADHD): A Randomized Placebo-Controlled Intervention Trial. Prostaglandins Leukot. Essent. Fatty Acids 2014, 91, 49–60. [Google Scholar] [CrossRef]
- Stark, K.D.; Aristizabal Henao, J.J.; Metherel, A.H.; Pilote, L. Translating Plasma and Whole Blood Fatty Acid Compositional Data Into the Sum of Eicosapentaenoic and Docosahexaenoic Acid in Erythrocytes. Prostaglandins Leukot. Essent. Fatty Acids 2016, 104, 1–10. [Google Scholar] [CrossRef]
- Jáuregui-Lobera, I. Iron Deficiency and Cognitive Functions. Neuropsychiatr. Dis. Treat. 2014, 10, 2087. [Google Scholar] [CrossRef] [Green Version]
- Grantham-McGregor, S.; Ani, C. A Review of Studies on the Effect of Iron Deficiency on Cognitive Development in Children. J. Nutr. 2001, 131, 649S–668S. [Google Scholar] [CrossRef] [PubMed]
- Grantham-McGregor, S.; Baker-Henningham, H. Review of the Evidence Linking Protein and Energy to Mental Development. Public Health Nutr. 2005, 8, 1191–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Schacky, C. Omega-3 Fatty Acids in Cardiovascular Disease–An Uphill Battle. Prostaglandins Leukot. Essent. Fatty Acids 2015, 92, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Van Der Burg, K.P.; Cribb, L.; Firth, J.; Karmacoska, D.; Sarris, J. Nutrient and Genetic Biomarkers of Nutraceutical Treatment Response in Mood and Psychotic Disorders: A Systematic Review. Nutr. Neurosci. 2019, 1–17. [Google Scholar] [CrossRef]
- Carney, R.M.; Steinmeyer, B.C.; Freedland, K.E.; Rubin, E.H.; Rich, M.W.; Harris, W.S. Baseline Blood Levels of Omega-3 and Depression Remission: A Secondary Analysis of Data From a Placebo-Controlled Trial of Omega-3 Supplements. J. Clin. Psychiatry 2016, 77, e138. [Google Scholar] [CrossRef] [Green Version]
- de Groot, R.H.; Meyer, B.J. Issfal Official Statement Number 6: The Importance of Measuring Blood Omega-3 Long Chain Polyunsaturated Fatty Acid Levels in Research. Prostaglandins Leukot. Essent. Fatty Acids 2019, 157, 102029. [Google Scholar] [CrossRef]
- de Groot, R.H.; Emmett, R.; Meyer, B.J. Non-Dietary Factors Associated with N-3 Long-Chain Pufa Levels in Humans–a Systematic Literature Review. Br. J. Nutr. 2019, 121, 793–808. [Google Scholar] [CrossRef] [Green Version]
- Umhau, J.C.; Zhou, W.; Carson, R.E.; Rapoport, S.I.; Polozova, A.; Demar, J.; Hussein, N.; Bhattacharjee, A.K.; Ma, K.; Esposito, G.; et al. Imaging Incorporation of Circulating Docosahexaenoic Acid Into the Human Brain Using Positron Emission Tomography. J. Lipid Res. 2009, 50, 1259–1268. [Google Scholar] [CrossRef] [Green Version]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the Executive Function Theory of Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. Biol. Psychiatry 2005, 57, 1336–1346. [Google Scholar] [CrossRef]
- Stevens, L.J.; Zentall, S.S.; Deck, J.L.; Abate, M.L.; Watkins, B.A.; Lipp, S.R.; Burgess, J.R. Essential Fatty Acid Metabolism in Boys with Attention-Deficit Hyperactivity Disorder. Am. J. Clin. Nutr. 1995, 62, 761–768. [Google Scholar] [CrossRef]
- Anand, D.; Colpo, G.D.; Zeni, G.; Zeni, C.P.; Teixeira, A.L. Attention-Deficit/Hyperactivity Disorder and Inflammation: What Does Current Knowledge Tell Us? A Systematic Review. Front. Psychiatry 2017, 8, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Létondor, A.; Buaud, B.; Vaysse, C.; Fonseca, L.; Herrouin, C.; Servat, B.; Layé, S.; Pallet, V.; Alfos, S. Erythrocyte DHA Level as a Biomarker of Dha Status in Specific Brain Regions of N-3 Long-Chain Pufa-Supplemented Aged Rats. Br. J. Nutr. 2014, 112, 1805–1818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkadi-Nagy, E.; Wijendran, V.; Diau, G.Y.; Chao, A.C.; Hsieh, A.T.; Turpeinen, A.; Lawrence, P.; Nathanielsz, P.W.; Brenna, J.T. Formula Feeding Potentiates Docosahexaenoic and Arachidonic Acid Biosynthesis in Term and Preterm Baboon Neonates. J. Lipid Res. 2004, 45, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Sugasini, D.; Yalagala, P.C.; Subbaiah, P.V. Plasma BDNF Is a More Reliable Biomarker Than Erythrocyte Omega-3 Index for the Omega-3 Fatty Acid Enrichment of Brain. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]




| Author, n 1 | Mean Age in Years (SD) and Any Specifics | DHA, EPA Dosage Per day Active Group | Other Constituents Active As Specified in Manuscript | Placebo as Specified in Manuscript | Duration (in Weeks) | Cognitive Tests | Adherence | Effect on Cognition? |
|---|---|---|---|---|---|---|---|---|
| Antypa n 54 [27] | A: 22.2 P: 22.6 | 250 mg DHA, 1740 mg EPA, | 310 mg other n-3 PUFA | Olive oil | 4 | Affective Go/No-Go task, attentional Go/No-Go task, 15 word test, decision-making (gambling) task. | OS | Y, in gains only trials of gambling task the n-3 group showed sig. more risk-seeking decision-making behavior than the placebo group. |
| Baumgartner n 321 [28] | 6–11 iron deficient | 240 mg DHA 46 mg EPA 1,3 | 28.6 mg iron sulfate 2,3 | Medium chain triglycerides 3 | 15 | The Atlantis test, Atlantis Delayed test, The Hand Movement test, the Triangles test, The Hopkins Verbal Learning Test | 95.4% | N |
| Benton n 305 [29] | 21.8 | 400 mg DHA | 10:0 5 mg, 12:0 38 mg, 14:0 121 mg, 16:0 78 mg, 18:0 10 mg, 18:1 312 mg, 18:2 15 mg, 22:0 3 mg | Maize/soya oil: 16:0 110 mg, 18:0 30 mg, 18:1 233 mg, 18: 2 567 mg, 18:5 41 mg, 20:0 4 mg, 20:1 3 mg, 22:0 2 mg | 7.1 | Recall of word list (immediate and delayed), recall of capitals, reaction time test, rapid information processing task | NR | Y, those taking DHA sig. forgot more than the placebo group on the recall of word list after 50 days. |
| Dalton n 183 [30] | 7–9 some underweight, wasted or stunted | 127.3 mg DHA, 54.6 mg EPA 4,5 | 222.55 mg ALA, 1041.2 mg LA, 15.4 mg AA 6 | 55.8 mg ALA, 9.8 mg EPA, 23.7 mg DHA, 1668.2 mg LA, 4.5 mg AA 7 | 14.9 | Hopkins Verbal Learning Test | A: 94.8% P: 94.5% | Y, sig. intervention effect for recall 1 and recall 3, recognition and discrimination index score |
| Guzman n 34 [31] | 23.58 female elite soccer players | 3500 g DHA | - | Olive oil | 4 | Multiple reaction times | NR | Y, those taking DHA showed sig. improvement in complex reaction time and complex reaction efficiency |
| Hamazaki n 42 [32] | Two groups: (1) 19–20 (2) 22 | 1500–1800 mg DHA, 200–240 mg EPA dependent on bodyweight | palmitic acid 270–324 mg, oleic acid 219–263 mg, AA 99–119 mg, palmitoleic acid 96–115 mg, stearic acid and others 69–83 mg | Soybean oil + partly deodorized fish oil: LA 1623–1948 mg, oleic acid 669–803 mg, palmitic acid 324–389 mg, ALA 204–245 mg, stearic acid 111–133 mg, DHA and others 15–18 mg | 12 | Adapted Stroop test, dementia-detecting test (to assess higher functions of brain) | NR | N |
| Jackson n 140 [33] | DHA rich group 21.96 (0.54), EPA rich group 22.74 (0.61) P: 21.94 (0.50) | I: DHA rich group: 450 mg DHA, 90 mg EPA II: EPA rich group: 300 mg EPA, 200 mg DHA | I: NS II: NS | 1 g olive oil | 12 | Immediate Word Recall, Simple RT, Choice RT, Four Choice RT, Stroop Task, Verbal Fluency, Alphabetic Working Memory, Corsi Block Task, Three Block Task, Telephone Number Working Memory Task, Delay Word Recall, Delayed Word Recognition, Delayed Picture Recognition, Names-To-Faces Recall, Cognitive Demand Battery (Serial 3 Subtractions, Serial 7 Subtractions, Rapid Visual Information Processing). | DHA: 91% EPA: 90% P: 92% | Y, DHA group had sig faster reaction time on Stroop Task compared to placebo group. Both DHA and EPA group matched sig. fewer items on the Names-To-Faces-task than the placebo group. |
| Jackson n 64 [34] | 20.58 | 1 g fish oil (FO) group: 450 mg DHA, 90 mg EPA, oil. 2 g FO group: 900 mg DHA, 180 mg EPA, | 1 g FO: 1 g olive 2 g FO: NS | 2 g olive oil | 12 | Corsi blocks task, Numeric Working Memory, 3-Back Task, Simple Reaction time, Choice Reaction Time, Four Choice Reaction Time, Stroop Task, Rapid Visual Information Processing Task, Serial 7 Subtractions while near-infra red spectroscopy was executed. | 1 g: 91% 2 g: 92% P: 96% | Y, sig. treatment effect on reaction time for Choice Reaction Time task, reaction time in both treatment groups faster. Sig. effect of treatment on Rapid Visual Information Processing Task, reaction time sig faster in 2 g FO group compared to placebo. |
| Karr n 41 [35] | FO: 19.9 (1.8) P: 20.4 (1.6) | 480 mg DHA, 720 mg EPA | NS | 1 g coconut oil | 4 | Rey Auditory Verbal Learning Test, Stroop Color and Word Test and Trail Making Test | 99% | Y, interaction condition x test moment sign. for Rey auditory Verbal Learning Test stage 6, stage 7 and summary 7–5 (FO improved from baseline, placebo not) but main effect cognition not sign. Placebo condition improved sig. over FO group on Trial Making Test. |
| Kennedy n 90 [36] | 10–12 | Low dose: 400 mg DHA, 8 mg EPA High dose: 1000 mg DHA, 20 mg EPA | Low dose: 2092 mg vegetable oil High dose: 1480 mg vegetable oil 8 | 2.5 g vegetable oil containing 75 mg ALA and 1250 mg LA | 8 | Internet Battery (Word Presentation, Picture Presentation, Arrow Reaction Time Test, Arrow Flanker Test, Paired Associate Learning, Sentence Verification, Delayed Word Recognition, Delayed Picture Recognition) and Cognitive Drug Research Battery (Picture Presentation, Word Presentation/Immediate Word Recall, Simple RT, Digit Vigilance Task: Choice RT, Spatial Working Memory, Numeric Working Memory, Delayed Word Recall, Delayed Word Recognition, Delayed Picture Recognition | >80% | N, sig. main treatment effect on speed of Word Recognition of the Cognitive Drug Research Battery. Post-hoc analysis: the low dose group was sig. faster than the placebo group. However, the high dose group was sig. slower than placebo group. |
| Kirby n 348 [37] | 8–10 | 400 mg DHA, 56 mg EPA, | 64 mg other n-3 fatty acids, vitamin A 800 mg RE, vitamin C 60 mg, vitamin D 5 mg, and vitamin E 3 mg | Olive oil | 16 | Working Memory Test Battery for Children (digit recall, block recall and backward digit recall), TEA-Ch (Creature Counting), Matching Familiar Figures Task | OS | Y, in intention to treat analysis no sig. effects. In per protocol analysis PUFA group had higher number of first correct responses on matching familiar figures task in comparison to baseline, the change for placebo group was not sig. |
| Long n 202 [38] | 20.9 | 672 mg DHA, 93.3 mg EPA 9 | 14:0 4.5 mg, 16:0 13.8 mg, 16:1 5.4 mg, 17:0 3 mg, 18:0 39.3 mg, 18:1 70.2 mg, 18:0 12.6 mg, 18:2 10.2 mg, 18:3 4.2 mg, 18:4 5.1 mg, 20:0 8.4 mg, 20:1 34.8 mg, 20:2 (n-9) 5.4 mg, 20:3 (n-6) 2.7 mg, 20:4 (n-6) 27.9 mg, 20:3 (n-3) 3.3 mg, 20:4 (n-3) 8.4 mg, 22:0 (n-3) 5.1 mg, 22:1 (n-11) 27.9 mg, 22:1 (n-9) 6.3 mg, 22:4 (n-6) 6 mg, 22:5 (n-6) 50.7 mg, 22:5 (n-3) 35.7 mg, 24:0 4.5 mg, 24:1 20.4 mg, minor components 4.9%, alpha tocopheryl acetate (2.25 mg), and mixed tocopherols (4.5 mg). multi vitamin and mineral supplement | 14:0 9.0 mg, 16:0 392.1 mg, 16:1 2.1 mg, 18:0 50.1 mg, 18:1 562.5 mg, 18:1 (n-7) 16.5 mg, 18:2 289.5 mg, 18:3 29.1 mg, 20:0 5.4 mg, 20:1 5.4 mg, 22:0 (n-3) 3.3 mg, 22:1 1.5 mg, 24:0 1.5 mg, minor components (0.4%), alpha tocopheryl acetate (2.28 mg), and mixed tocopherols (4.5 mg) | 12 | Go Stop Impulsivity Paradigm | NR | Y, only for participants with high impulsivity at baseline: the % of inhibited responses was sig. greater if they had consumed DHA rather than a placebo. For participants with low impulsivity no effect of supplementation was shown. |
| McNamara n 38 [39] | 8–10 | Low dose: 400 mg DHA High dose: 1200 mg DHA, | Low dose: 2 g corn oil High dose: - | 3 g corn oil | 8 | The identical-pairs version of the Continuous Performance task (CPT-IP). | NR | N |
| Montgomery n 376 [40] | 7–9 underperforming on reading | 600 mg DHA 22.5 mg EPA | 14:0 72.4 mg, 16:0 222 mg, 18:0 14.5 mg, 18:1 n-9 242.9 mg, 18:2 n-6 16.1 mg, 22:5 n-6 252.5 mg | 1500 mg corn/soy bean oil | 16 | Recall of digits Forward and Recall of Digits Backwards | 75% | N |
| Muthayya n 598 [41] | 6–10 marginally nourished | High n-3: 86 mg DHA 10,11 | High n-3: 800 mg ALA + high or low micronutrient 12,13 | Low n-3: 120 mg ALA + high or low micronutrient 13,14 | 52 | Kaufman Assessment Battery for Children (pattern reasoning, triangles, rover, number recall, word order and Atlantis), Wechsler Intelligence Scales for Children (picture arrangement and coding), Rey Auditory Verbal Learning test (auditory-verbal learning test), Neuropsychological Assessment Tool (verbal fluency) and number cancellation | 70% | N |
| Osendarp n 780 [42] | 6–10 Some marginally nourished | 88 mg DHA 22 mg EPA 15,16 | Multivitamin 17 | Base powder | 52 | Digits Backwards, Visual Attention 2, Coding, Block Design, Fluency Structured and Random, Rey Auditory Verbal Learning Test. | 73–87% | N |
| Parletta n 408 [43] | 3–13 18 | 174 mg DHA 558 mg EPA | 60 mg GLA, 10.8 mg vitamin E | Palm oil + fraction of fish oil | 28.6 | Draw-A-Person | Y, sig. treatment by group interaction whereby the treatment group improved compared to placebo. | |
| Portillo-Reyes n 55 [44] | 8–12 Malnourished | 180 mg DHA 270 mg EPA | Not reported | Soy bean oil | 12 | Symbol Search, Embedded Figures Test, Visual Closure, Block Design, TMT A, Letter Cancellation, Rey Complex Figure, Word List, Semantic Fluency, Matrix Reasoning, Letter-Number Sequencing, Stroop Color and Word test, TMT-B: Shifting. | NR | Y, only the treatment group improved sig. in Symbol Search, Embedded Figures, Visual Closure, Block Design, Stroop-Color, Stroop Color-Word and Matrix Reasoning. |
| Richardson n 362 [45] | 7–9 underperforming on reading | 600 mg DHA | NS | 1500 mg corn/soy bean oil | 16 | Recall of Digits Forward and Recall of Digits Backwards | 75% | Y, post intervention score for Recall of Digits Forwards sig. higher in active treatment group. |
| Ryan n 202 [46] | 4 | 400 mg DHA | high-oleic sunflower oil | 16 | Leiter-R Test of Sustained Attention, Day-Night Stroop Test, and Conners’ Kiddie Continuous Performance Test, Peabody Picture Vocabulary Test. | Nearly 100% | N | |
| Van der Wurff n 267 [47] | 13–15 | 280 mg DHA, 520 mg EPA | NS | Capsules with a fatty acid profile comparable to the fatty acid composition of the average European diet: mix of olive oil, corn oil, palm oil and medium chain triglycerides: (16:0 26%, 18:0 4.6%, 18: 1–9 35.8%, 18:2–6 16.7%, 18:3–32.1%, 20:4–6 0% and other compounds 14.8%) | 52 | Letter Digit Substitution Task, Concept Shifting Task, Digit Span Forwards and Backwards, D2 test of Attention. | OS | N |
| Author, n, Reference | Mean Age in Years (Sd) and Any Specifics | DHA, EPA Dosage per Day Active Group | Other Constituents Active as Specified in Manuscript | Placebo as Specified in Manuscript | Duration (in Weeks) | Cognitive Measure | Adherence | Effect on Cognition? |
|---|---|---|---|---|---|---|---|---|
| Bos n 79 [48] | ADHD: 10.3 Typically developing: 10.9 | 650 mg DHA, 650 mg EPA | 70 mg ALA, 30 mg AA, 1 g LA, 2.66 g saturated FA, 2.08 g MUFA, 6.4 mg vitamin E | 60 mg ALA, 1 g LA, 2.59 g saturated FA, 4.32 g MUFA, 0.52 mg vitamin E | 16 | Go-No Go task | ADHD: 92.2% TD: 91.4% | N |
| Cornu n 162 [49] | A: 10.2 P: 9.7 ADHD | 84 mg-168 mg DHA, 336–672 mg EPA1 | 100μg vitamin A, 1.25 μg vitamin D, 3.5 mg vitamin E | Olive oil + marine lipid concentrate containing 4.83 mg EPA + DHA, 100μg vitamin A, 1.25μg vitamin D, 3.5 mg vitamin E | 12 | KiTAP (6–10 yr) and TAP (11–15 yr): Distractibility, Flexibility and Go/NoGo | OS | N |
| Crippa n 50 [50] | 7–14 ADHD drug-naïve | 500 mg DHA | wheat germ oil, low concentration vitamin E. | 24 | Abbreviated ANT: Focused Attention 4 letters, Shifting Attentional Set-Visual and Sustained Attention. | 83.2% | Y, DHA group showed a decrease in misses in Focused Attention 4 letters task at 6 mo, placebo group showed decrease at 4 mo but not at 6 mo. DHA group showed reduction in false alarms irrelevant target in Focused Attention 4-letters task at 6 mo. | |
| Demmelmair n 109 [51] | 5–13 PKU | Between 20 and 254 mg DHA2 | 14:0 5–64 mg, 14:1 0–1 mg, 16:0 37–61 mg, 16:1 1.5–14 mg 18:0 15.5–20 mg, 18:1 403–536 mg, 18:2 n-6 29–35, 18:n3–3 0.5–1 mg, 20:0 1.5–2 mg, 20:1 n-9 1–2 mg, 22:0 3.5–5 mg, 24:1 n-9 1–2 mg, 22:5 n-3 0–3 mg3 | 16:0 16.5–33 mg, 16.1 0.5–1 mg, 18:0 16–32 mg, 18:1 428.5–857 mg, 18:2 n-6 29–58 mg, 18:3 n-3 0.5–1 mg, 20:0 1.5–3 mg, 20:1 n-9 1.5–3 mg, 22:0 4–8 mg, 24:1 n-9 1.5–3 mg4 | 24 | Raven Progressive Matrices (standard or coloured) | 96–102% | N |
| Hirayama n 40 [52] | 6–12 ADHD | 514 mg DHA, 100 mg EPA5 | - | Olive oil | 16 | Adapted Test of Visual Perception, Visual and Auditory Short-Term Memory, Developmental Test of Visual–Motor Integration, Continuous Performance Test | NR | Y, Visual Short Term Memory and number of errors of commission on Continuous Performance Test improved sig. in control group. |
| Kean n 112 [53] | 6–14, mean 8.7 ADHD rating score >15 | 16.5–22 mg DHA, 21.9–29.2 mg EPA 6 | 300–400 mg olive oil, 0.68–0.90 mg vitamin E, diverse sterol esters (amounts not specified) | Olive oil, lecithin, coconut oil and beta-carotene | 14 | COMPASS cognitive battery: Word Presentation, Immediate Word Recall, Picture Presentation, Simple Reaction Time, Choice Reaction Time, Numeric Working Memory, Delayed Word Recall, Delayed Word Recognition, Delayed Picture Recognition. TOVA | 96.7% | Y, improved memory accuracy score in active group for recalled target and non-target pictures correctly and sig. overall picture recognition accuracy only at 8 weeks not at 14 weeks. No sig. differences in TOVA. Additionally subgroup differences showed difference between diagnosed and non-diagnosed participants in response to supplement. |
| Rodriguez n 95 [54] | 6–19 ADHD | 1000–2000 mg DHA, 90–180 mg EPA 7 | 150–300 mg n-3 DPA, 4.5–9 mg vitamin E | Olive oil | 24 | AULA Nesplora test, d2 test of attention | OS | N |
| Sinn n 167 [55] | 7–12 ADHD symptoms no stimulant medication | 174 mg DHA, 558 mg EPA 8 | 60 mg GLA, 10.8 mg vitamin E, multivitamin 9 | Palm oil: 44.3% palmitic acid C16, 4.6% stearic acid C18, 1% myristic acid C14, 38.7% oleic acid C18, and 10.5% LA | 15w–one way CO 15w | Digit-Symbol Coding, Inspection Time, Rey Auditory-Verbal Learning Test, Creature Counting, DSB, Knock and Tap, Stroop Colour-Word Test. | OS | Y, PUFA group had sig improvement compared to placebo on Creature Counting with large effect. |
| Stevens n 50 [56] | P: 10.1 A: 9.5 ADHD + high thirst/ skin symptom score | 480 mg DHA, 80 mg EPA | 40 mg AA, 96 mg GLA, 24 mg vitamin E | Olive oil | 16 | Conners’ Continuous Performance Test, Woodcock-Johnson Psycho-Educational Battery-Revised | 88% | Y, hit reaction time on Conner’s Continuous Performance Test showed a treatment effect in favor of treatment group. Auditory processing showed improvement in treatment group only (no significant difference between groups). |
| Vaisman n 83 [57] | 8–13 ADHD and impaired visual sustained attention performance | FO: 96 mg DHA, 153 mg EPA or n-3 LCPUFA containing PLs: 95 mg DHA, 156 mg EPA | FO: 14:0 63 mg, 16:0 147 mg, 18:0 31 mg, 20:0 2 mg, 22:0 2 mg, 24:0 4 mg, 16:1 n-7 68 mg, 18:1 n-9 95 mg, 18:1 n-7 25 mg, 20:1 n-9 12 mg, 22:1 n-9 7 mg, 18:2 n-6 18 mg, 18:3 n-6 2 mg, 20:4 n-6 7 mg, 18:3 n-3 25 mg LC-PUFA containing PLs: 14:0 19 mg, 16:0 141 mg, 18:0 7 mg, 22:0 1 mg, 16:1 n-7 19 mg, 18:1 n-9 37 mg, 18:1 n-7 44 mg, 20:1 n-9 5 mg, 22:1 n-9 5 mg, 18:2 n-6 11 mg, 18:3 n-6 1 mg, 20:4 n-6 4 mg, 18:3 n-3 7 mg, 22:5 n-3: 4 mg 10 | 16:0 30 mg, 18:0 13 mg, 20:0 5 mg, 22:0 3 mg, 24:0 1 mg, 16:1 n-7 1 mg, 18:1 n-9 415 mg, 20:1 n-9 12 mg, 22:1 n-9 4 mg, 18:2 n-6 150 mg, 18:3 n-3 69 mg | 12 | TOVA | OS | Y, The PL-n3 and, to a limited extent, the FO treatment significantly improved errors of commission, response time, and response time variability as compared with placebo intervention |
| Voigt n 63 [58] | 6–12 ADHD | 345 mg DHA | - | Not specified | 16 | TOVA, The Children’s Color Trails test | OS | N |
| Widdenhorn-Muller n 110 [59] | 6–12 ADHD | 120 mg DHA, 600 mg EPA | 15 mg vitamin E | Olive oil | 16 | DSF, DSB, Letter Number Sequencing, HAWIK Number-Symbol, Symbol Search Test, KITAP or TAP (dependent on age participant) | OS | Y, sig. improvement on working memory index score, Digit Span subtest and DSB. |
| O3I Equivalence Before | O3I Equivalence After | O3I Equivalence Change | Significant Effect on Cognition? | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| DHA, EPA Dose per Day | Blood Fraction | Formulae Used 1 | Intervention | Placebo | Intervention | Placebo | Intervention | Placebo | ||
| Typically developing | ||||||||||
| Antypa [27] | 250 mg DHA, 1740 mg EPA | Plasma FA | 0.94 x + 1.17 | 3.46 | 3.18 | 6.28 | 3.36 | 2.82 | 0.18 | Y |
| Baumgartner 2 [28] | 240 mg DHA, 46 mg EPA | Total PP fraction of erythr membranes | 3.20 a 3.17 b | 3.22 c 3.24 d | 6.27 a 6.33 b | 4.03 c 3.97 d | 3.07 3.16 | 0.81 0.73 | N | |
| Jackson 3 [33] | DHA rich group: 450 mg DHA, 90 mg EPA EPA rich group: 300 mg EPA, 200 mg DHA | Serum FA | 0.94 x + 1.17 | 3.34 e 3.31 f | 3.16 | 4.21 e 4.24 f | 3.29 | 0.87 0.93 | 0.13 | Y |
| Muthayya [41] | 86 mg DHA | Erythr membranes in PP fraction | - | 3.37 3.38 | 3.37 3.48 | 5.55 5.59 | 3.85 3.86 | 2.18 2.21 | 0.48 0.38 | N |
| Hamazaki [32] | 1500–1800 mg DHA, 200–240 mg EPA4 | Total serum FA | 0.94 x + 1.17 | 4.93 | 5.96 | 9.25 | 5.68 | 4.32 | −0.28 | N |
| Ryan [46] | 400 mg DHA | Capillary WB | 1.10 x + 0.65 | 2.08 | 2.08 | 4.83 | 2.19 | 2.75 | 0.11 | N |
| Van der Wurff [47] | 280 mg DHA, 520 mg EPA | Capillary WB | - | 3.72 | 3.83 | 4.86 | 3.98 | 1.03 | 0.15 | N |
| With disorder/disease | ||||||||||
| Stevens [56] | 480 mg DHA, 80 mg EPA | Eryth membranes | - | 4.08 | 3.78 | 8.83 | 3.53 | 4.75 | −0.25 | Y |
| Widdenhorn-Muller [59] | 120 mg DHA, 600 mg EPA | Eryth membranes | - | 4.13 | 4.05 | 7.82 | 4.03 | 3.69 | −0.02 | Y |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Wurff, I.S.M.; Meyer, B.J.; de Groot, R.H.M. Effect of Omega-3 Long Chain Polyunsaturated Fatty Acids (n-3 LCPUFA) Supplementation on Cognition in Children and Adolescents: A Systematic Literature Review with a Focus on n-3 LCPUFA Blood Values and Dose of DHA and EPA. Nutrients 2020, 12, 3115. https://doi.org/10.3390/nu12103115
van der Wurff ISM, Meyer BJ, de Groot RHM. Effect of Omega-3 Long Chain Polyunsaturated Fatty Acids (n-3 LCPUFA) Supplementation on Cognition in Children and Adolescents: A Systematic Literature Review with a Focus on n-3 LCPUFA Blood Values and Dose of DHA and EPA. Nutrients. 2020; 12(10):3115. https://doi.org/10.3390/nu12103115
Chicago/Turabian Stylevan der Wurff, Inge S.M., Barbara J. Meyer, and Renate H.M. de Groot. 2020. "Effect of Omega-3 Long Chain Polyunsaturated Fatty Acids (n-3 LCPUFA) Supplementation on Cognition in Children and Adolescents: A Systematic Literature Review with a Focus on n-3 LCPUFA Blood Values and Dose of DHA and EPA" Nutrients 12, no. 10: 3115. https://doi.org/10.3390/nu12103115