Carbohydrates, Starch, Total Sugar, Fiber Intakes and Food Sources in Spanish Children Aged One to <10 Years—Results from the EsNuPI Study †

 , ,
, ,  ,
,  ,
,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
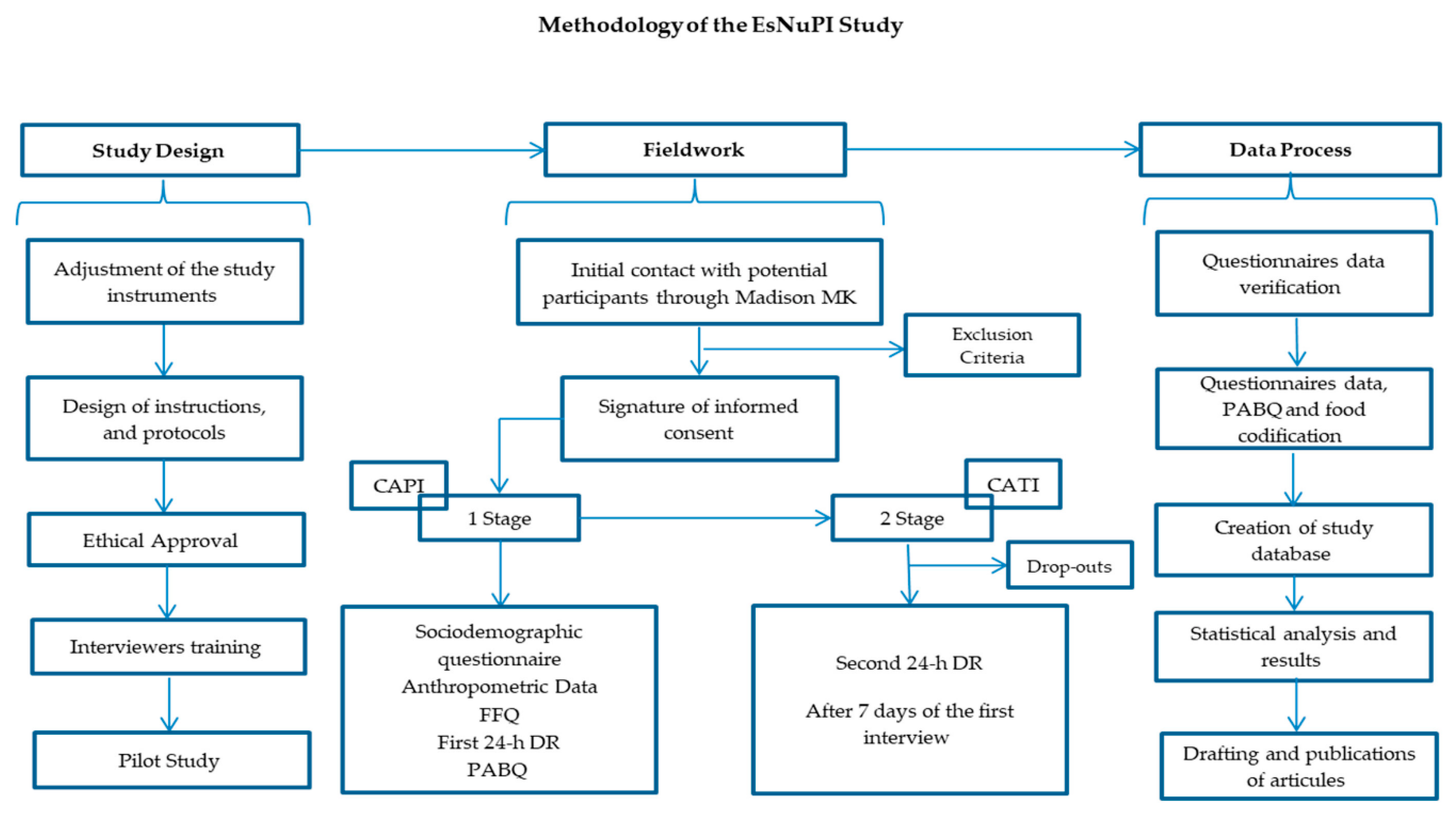
2.1. Study Design and Sample
2.2. Procedures and Data Collection
2.2.1. Socio-Demographic and Anthropometric Information
2.2.2. Physical Activity and Sedentary Behavior Questionnaire
2.3. Procedures, Dietary Survey and Data Collection
2.4. Statistical Analysis
3. Results
3.1. Total Carbohydrates, Starch, Total Sugar and Fiber Usual Intake in Children
3.2. Contribution of Food and Beverage Groups to Total Carbohydrates, Starch, Total Sugar and Fiber Reported Intakes
3.3. Total Carbohydrates, Starch, Total Sugar, and Fiber Intake in Children by Nielsen Geographical Area, Body Composition, and Income Level
4. Discussion
4.1. Total Carbohydrate Intakes and Sources
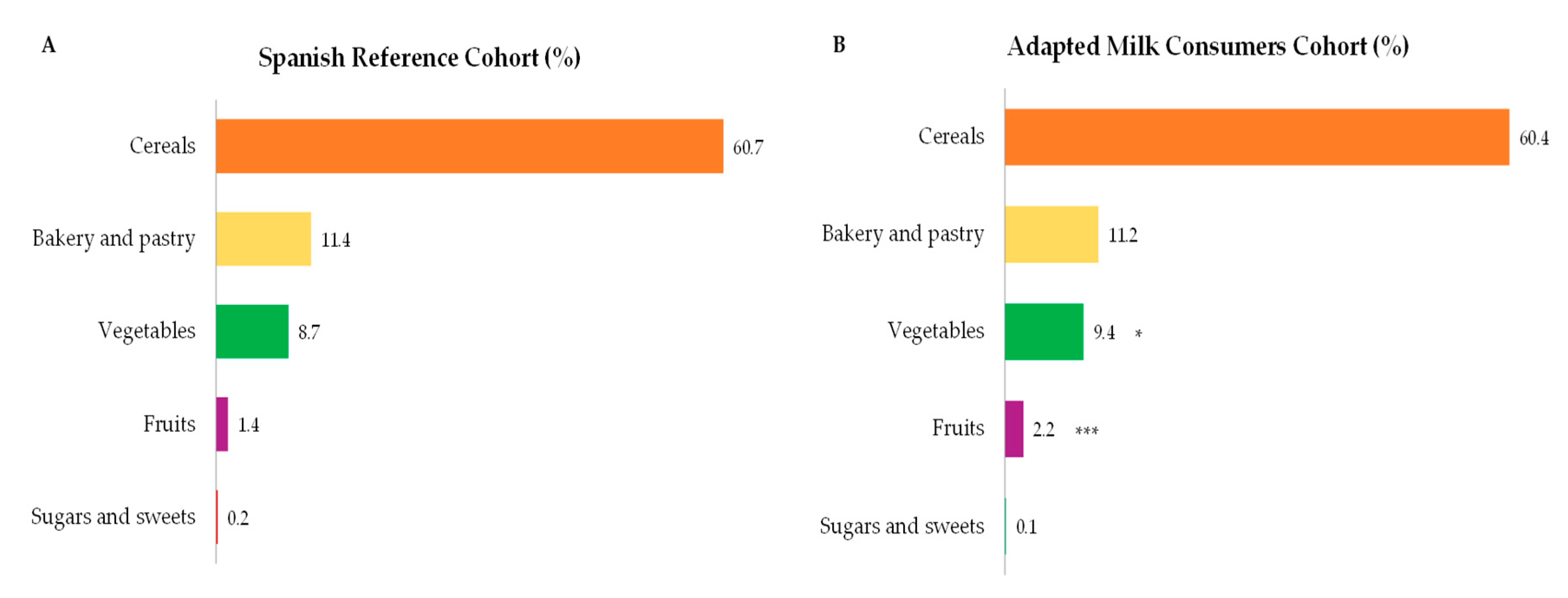
4.2. Starch Intakes and Sources
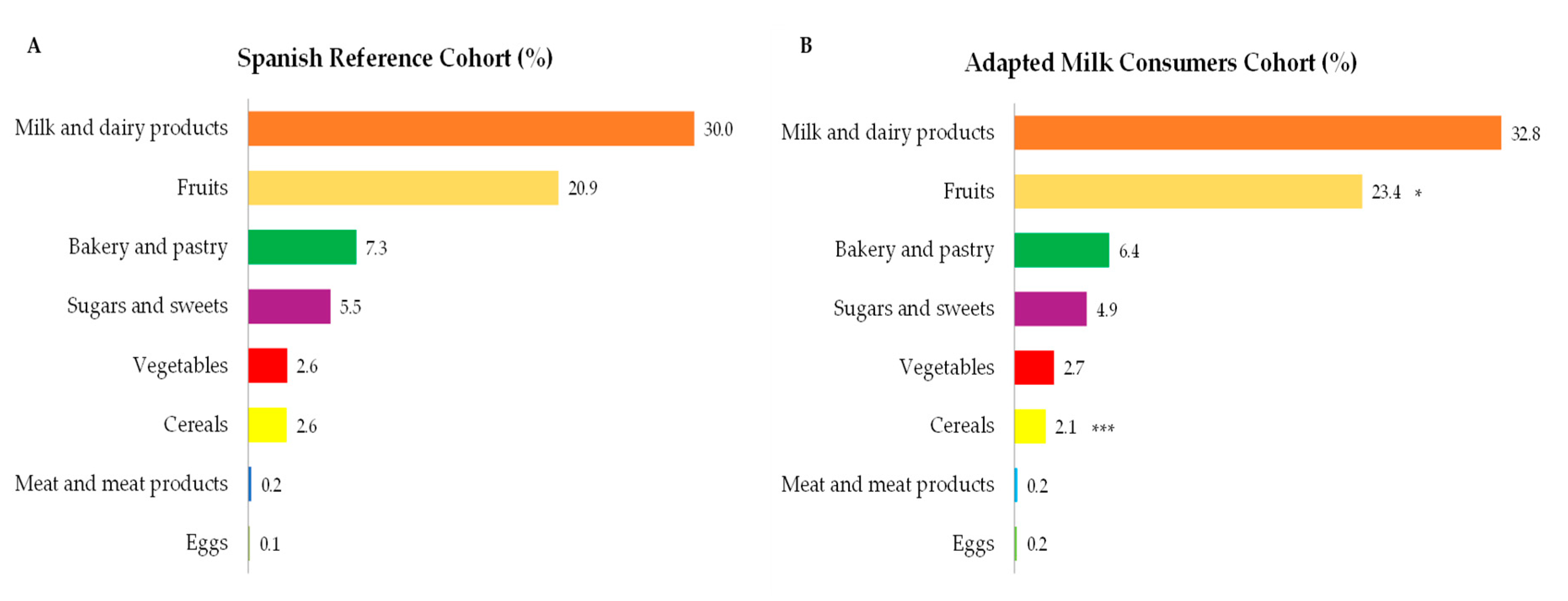
4.3. Total Sugar Intakes and Sources
4.4. Dietary Fiber Intakes and Sources
4.5. Body Composition, Socioeconomic and Geographical Factors
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Clark, H.; Coll-Seck, A.M.; Banerjee, A.; Peterson, S.; Dalglish, S.L.; Ameratunga, S.; Balabanova, D.; Bhan, M.K.; Bhutta, Z.A.; Borrazzo, J.; et al. A future for the world's children? A WHO–UNICEF–Lancet Commission. Lancet 2020, 395, 605–658. [Google Scholar] [CrossRef] [Green Version]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health. Childhood Overweight and Obesity. Available online: https://www.who.int/dietphysicalactivity/childhood/en/ (accessed on 18 June 2020).
- Ministerio de Sanidad, Consumo, Igualdad y Servicios Sociales. Encuesta Nacional de Salud 2017; Ministerio de Sanidad, Consumo, Igualdad y Servicios Sociales: Madrid, Spain, 2018.
- Ministerio de Sanidad, Consumo y Bienestar Social. Agencia Española de Seguridad Alimentaria y Nutrición. Prevalencia de Sobrepeso y Obesidad en España en El Informe “The Heavy Burden of Obesity” de la OCDE 2019 y en Otras Fuentes de Datos. 2019. Available online: http://www.aecosan.msssi.gob.es/ca/AECOSAN/web/nutricion/subseccion/documentos.htm (accessed on 16 May 2020).
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 1462. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, E.; Ávila, J.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; et al. Macronutrient Distribution and Dietary Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2016, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- López-Sobaler, A.M.; Aparicio, A.; Rubio, J.; Marcos, V.; Sanchidrián, R.; Santos, S.; Pérez-Farinós, N.; Dal-Re, M.Á.; Villar-Villalba, C.; Yusta-Boyo, M.J.; et al. Adequacy of usual macronutrient intake and macronutrient distribution in children and adolescents in Spain: A National Dietary Survey on the Child and Adolescent Population, ENALIA 2013–2014. Eur. J. Nutr. 2019, 58, 705–719. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, E.; Ávila, J.M.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; et al. Energy Intake, Profile, and Dietary Sources in the Spanish Population: Findings of the ANIBES Study. Nutrients 2015, 7, 4739–4762. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Dietary Reference Values for Nutrients Summary Report. EFSA Support. Publ. 2017, 14, e15121E. [Google Scholar] [CrossRef] [Green Version]
- WHO. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [Green Version]
- Aggett, P.J.; Agostoni, C.; Axelsson, I.; Edwards, C.A.; Goulet, O.; Hernell, O.; Koletzko, B.; Lafeber, H.N.; Micheli, J.-L.; Michaelsen, K.F.; et al. Nondigestible carbohydrates in the diets of infants and young children: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2003, 36, 329–337. [Google Scholar] [CrossRef] [Green Version]
- Madrigal, C.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Ruiz, E.; Valero, T.; Ávila, J.M.; Lara-Villoslada, F.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Dietary and Lifestyle Patterns in the Spanish Pediatric Population (One to <10 Years Old): Design, Protocol, and Methodology of the EsNuPI Study. Nutrients 2019, 11, 3050. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The WHO Child Growth Standards. Available online: http://www.who.int/childgrowth/en (accessed on 14 June 2020).
- Onis, M.D.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Camargo, D.M.; Santisteban, S.; Paredes, E.; Flórez, M.A.; Bueno, D. Confiabilidad de un cuestionario para medir la actividad física y los comportamientos sedentarios en niños desde preescolar hasta cuarto grado de primaria. Biomédica 2015, 35, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Madrigal, C.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Valero, T.; Ávila, J.M.; Ruiz, E.; Lara Villoslada, F.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Energy Intake, Macronutrient Profile and Food Sources of Spanish Children Aged One to <10 Years—Results from the EsNuPI Study. Nutrients 2020, 12, 893. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority (EFSA). Example of a Protocol for Identification of Misreporting (Underand Overreporting of Energy Intake) Based on the PILOT-PANEU Project. Available online: http://www.efsa.europa.eu/sites/default/files/efsa_rep/blobserver_assets/3944A-8-2-1.pdf (accessed on 1 November 2019).
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. 1), 5–41. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L. Ingestas Diarias Recomendadas de Energía y Nutrientes para la Población Española. In Tablas de Composición de Alimentos, 19th ed.; Ediciones Pirámide (Grupo Anaya, SA): Madrid, Spain, 2018. [Google Scholar]
- Fundación Española de la Nutrición (FEN) Software VD-FEN 2. 1 Programa de Valoración Dietética de la FEN; Fundación Española de la Nutrición (FEN): Madrid, Spain, 2013. [Google Scholar]
- Ruiz-López, M.D.; de Martínez Victoria, E.; Gil, A. Guía Fotográfica de Porciones de Alimentos Consumidos en España; Fundación Iberoamericana de Nutrición: Granada, Spain, 2019. [Google Scholar]
- European Food Safety Authority (EFSA). Dietary Reference Values for the Eupean Union. 2019. Available online: https://www.efsa.europa.eu/en/topics/topic/dietary-reference-values (accessed on 1 May 2020).
- Nusser, S.M.; Carriquiry, A.L.; Dodd, K.W.; Fuller, W.A. A semiparametric transformation approach to estimating usual daily intake distributions. J. Am. Stat. Assoc. 1996, 91, 1440–1449. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas-Barba, L.; Pérez-Rodrigo, C.; Bartrina, J.A. Nutrient adequacy in Spanish children and adolescents. Br. J. Nutr. 2006, 96, S49–S57. [Google Scholar] [CrossRef]
- Cuadrado-Soto, E.; López-Sobaler, A.M.; Jiménez-Ortega, A.I.; Aparicio, A.; Bermejo, L.M.; Hernández-Ruiz, Á.; Lara Villoslada, F.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Usual Dietary Intake, Nutritional Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D of Spanish Children Aged One to <10 Years. Findings from the EsNuPI Study. Nutrients 2020, 12, 1787. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on nutrient requirements and dietary intakes of infants and young children in the European Union. EFSA J. 2013, 11, 3408. [Google Scholar]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef]
- Börnhorst, C.; Huybrechts, I.; Hebestreit, A.; Krogh, V.; De Decker, A.; Barba, G.; Moreno, L.A.; Lissner, L.; Tornaritis, M.; Loit, H.M.; et al. Usual energy and macronutrient intakes in 2–9-year-old European children. Int. J. Obes. 2014, 38, S115–S123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Pozo, S.; García, V.; Cuadrado, C.; Ruiz, E.; Valero, T.; Ávila, J.; Varela-Moreiras, G. Valoración Nutricional de la Dieta Española de Acuerdo al Panel de Consumo Alimentario; Fundación Española de la Nutrición (FEN): Madrid, Spain, 2012. [Google Scholar]
- Ruiz, E.; Rodriguez, P.; Valero, T.; Ávila, J.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; Varela-Moreiras, G. Dietary Intake of Individual (Free and Intrinsic) Sugars and Food Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 275. [Google Scholar] [CrossRef] [Green Version]
- Van Dam, R.; Seidell, J. Carbohydrate intake and obesity. Eur. J. Clin. Nutr. 2007, 61, S75–S99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephen, A.M.; Champ, M.M.-J.; Cloran, S.J.; Fleith, M.; Van Lieshout, L.; Mejborn, H.; Burley, V.J. Dietary fibre in Europe: Current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr. Res. Rev. 2017, 30, 149–190. [Google Scholar] [CrossRef]
- Bartrina, J.A.; Majem, L.S. Objetivos nutricionales para la población española: Consenso de la Sociedad Española de Nutrición Comunitaria 2011. Rev. Española De Nutr. Comunitaria (Span. J. Community Nutr.) 2011, 17, 178–199. [Google Scholar]
- Aranceta-Bartrina, J.; Partearroyo, T.; López-Sobaler, A.M.; Ortega, R.M.; Varela-Moreiras, G.; Serra-Majem, L.; Pérez-Rodrigo, C. Updating the Food-Based Dietary Guidelines for the Spanish Population: The Spanish Society of Community Nutrition (SENC) Proposal. Nutrients 2019, 11, 2675. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Ribas-Barba, L.; Salvador, G.; Jover, L.; Raidó, B.; Ngo, J.; Plasencia, A. Trends in energy and nutrient intake and risk of inadequate intakes in Catalonia, Spain (1992–2003). Public Health Nutr. 2007, 10, 1354–1367. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Alvira, J.M.; Bammann, K.; Pala, V.; Krogh, V.; Barba, G.; Eiben, G.; Hebestreit, A.; Veidebaum, T.; Reisch, L.; Tornaritis, M.; et al. Country-specific dietary patterns and associations with socioeconomic status in European children: The IDEFICS study. Eur. J. Clin. Nutr. 2014, 68, 811–821. [Google Scholar] [CrossRef]
- Kovács, E.; Siani, A.; Konstabel, K.; Hadjigeorgiou, C.; De Bourdeaudhuij, I.; Eiben, G.; Lissner, L.; Gwozdz, W.; Reisch, L.; Pala, V. Adherence to the obesity-related lifestyle intervention targets in the IDEFICS study. Int. J. Obes. 2014, 38, S144–S151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranceta, J.; Pérez-Rodrigo, C.; Ribas, L.; Serra-Majem, L. Sociodemographic and lifestyle determinants of food patterns in Spanish children and adolescents: The enKid study. Eur. J. Clin. Nutr. 2003, 57, S40–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ocké, M.; de Boer, E.; Brants, H.; van der Laan, J.; Niekerk, M.; van Rossum, C.; Temme, L.; Freisling, H.; Nicolas, G.; Casagrande, C.; et al. PANCAKE—Pilot study for the Assessment of Nutrient intake and food Consumption Among Kids in Europe. EFSA Support. Publ. 2012, 9, 339E. [Google Scholar] [CrossRef]
- Livingstone, M.B.E.; Robson, P.J.; Wallace, J.M.W. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, S213–S222. [Google Scholar] [CrossRef] [PubMed]
- EU. European Union. Regulation (EU) 1169/2011 of the European parliament and of the Council of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and(EC) No 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004 (Text with EEA relevance). Off. J. Eur. Union 2011, 304, 18–63. [Google Scholar]
- Yusta-Boyo, M.J.; Bermejo, L.M.; García-Solano, M.; López-Sobaler, A.M.; Ortega, R.M.; García-Pérez, M.; Dal-Re Saavedra, M.Á. Sugar Content in Processed Foods in Spain and a Comparison of Mandatory Nutrition Labelling and Laboratory Values. Nutrients 2020, 12, 1078. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spanish Reference Cohort (SRS) | Adapted Milk Consumers Cohort (AMS) | ||||||
|---|---|---|---|---|---|---|---|
| Total | Boys | Girls | Total | Boys | Girls | ||
| Total population, n (%) | n | 707 (48.8%) | 357 (50.5%) | 350 (49.5) | 741 (51.2%) | 371 (50.1%) | 370 (49.9%) |
| Age group, n (%) | 1 to <3 years | 162 (22.9%) | 84 (23.5%) | 78 (22.3%) | 294 (39.7%) | 144 (38.8%) | 150 (40.5%) |
| 3 to <6 years | 244 (34.5%) | 122 (34.2%) | 122 (34.9%) | 262 (35.4%) | 128 (34.5%) | 134 (36.2%) | |
| 6 to <10 years | 301 (42.6%) | 151 (42.3%) | 150 (42.9%) | 185 (25%) | 99 (26.7%) | 86 (23.2%) | |
| Anthropometric characteristics, median (interquartile range) | Weight (kg) | 19.0 (14.6–26.0) | 19.0 (15.0–26.6) | 19.0 (14.0–26.0) | 15.0 *** (12.0–20.0) | 16.0 *** (12.0–22.0) | 15.0 *** (12.0–20.0) |
| Height (cm) | 110.0 (95.0–126.0) | 110.0 (95.0–127.0) | 110.0 (94.0–126.0) | 98.0 *** (86.0–115.0) | 98.0 *** (87.0–118.0) | 98.0 *** (95.0–110.0) | |
| BMI (kg/m2) | 16.5 (15.2–18.0) | 16.5 (15.3–18.0) | 16.5 (15.1–18.0) | 16.3 (15.1–18.0) | 16.4 (15.3–17.9) | 16.3 (14.9–18.0) | |
| Z-BMI/Age | 0.6 (−0.3–1.5) | 0.6 (−0.3–1.5) | 0.6 (−0.3–1.4) | 0.5 (−0.3–1.4) | 0.45 (−0.3–1.4) | 0.5 (−0.3–1.4) | |
| Z-Weight/Age | 0.5 (−0.3–1.2) | 0.4 (−0.4–1.2) | 0.6 (−0.3–1.3) | 0.6 (−0.3–1.4) | 0.6 (−0.1–1.4) | 0.5 (−0.3–1.4) | |
| Z-Height/Age | −0.3 (−1.2–0.9) | −0.2 (−1.1–1.0) | −0.4 (−1.3–0.7) | −0.4 ** (−1.4–0.6) | −0.4 ** (−1.4–0.6) | −0.4 (−1.5–0.6) | |
| Physical Activity Level (PAL), median (interquartile range) | 1 to <3 years | 1.6 (1.3–1.8) | 1.6 (1.4–1.8) | 1.5 (1.3–1.8) | 1.5 (1.3–1.7) | 1.5 (1.3–1.8) | 1.5 (1.3–1.7) |
| 3 to <6 years | 1.6 (1.4–1.7) | 1.6 (1.4–1.7) | 1.5 (1.4–1.7) | 1.5 (1.4–1.7) | 1.5 (1.4–1.7) | 1.5 (1.4–1.7) | |
| 6 to <10 years | 1.6 (1.4–1.7) | 1.6 (1.4–1.8) | 1.6 (1.5–1.7) | 1.6 (1.5–1.7) | 1.6 (1.5–1.8) | 1.6 (1.5–1.7) | |
| Size of the municipality, n (%) | 50.001 a 300.000 people | 376 (53.2%) | 193 (54.1%) | 183 (52.3%) | 406 (54.8%) | 204 (55.0%) | 202 (54.6%) |
| >300.000 inhabitants | 331 (46.8%) | 164 (45.9%) | 167 (47.7%) | 335 (45.2%) | 167 (45.0%) | 168 (45.4%) | |
| Highest level of education achieved by one of the parents, n (%) | ≤10 years of education | 23 (3.3%) | 10 (2.9%) | 13 (3.8%) | 14 (1.9%) | 7 (1.9%) | 7 (1.9%) |
| Secondary education | 416 (60.5%) | 219 (62.9%) | 197 (57.9%) | 414 (57.0%) | 208 (57.5%) | 206 (56.6%) | |
| University studies | 249 (36.2%) | 119 (34.2%) | 130 (38.2%) | 298 (41.0%) | 147 (40.6%) | 151 (41.5%) | |
| Income Level (€/month), n (%) | Low (<1500 €) | 171 (24.2%) | 79 (22.1%) | 92 (26.3%) | 163 (22.0%) | 84 (22.6%) | 79 (21.4%) |
| Medium (1501 to 2000 €) | 126 (17.8%) | 67 (18.8) | 59 (16.9%) | 134 (18.1%) | 64 (17.3%) | 70 (18.9%) | |
| High (>2000 €) | 226 (32.0%) | 123 (34.5%) | 103 (29.4%) | 238 (32.1%) | 110 (29.6%) | 128 (34.6) | |
| No answer/Does not know | 184 (26.0%) | 88 (24.6%) | 96 (27.4%) | 206 (27.8%) | 113 (30.5%) | 93 (25.1%) | |
| Number of feeding bottles or glasses of milk per day, n (%) | Less than 2 | 222 (32.9%) | 110 (32.0%) | 115 (33.8%) | 178 (24.1%) | 92 (24.9%) | 86 (23.3%) |
| 2 or more | 459 (67.1%) | 234 (68.0%) | 225 (66.2%) | 561 (75.9%) | 278 (75.1%) | 283 (76.7%) | |
| Group | Group by Age | RI (%) | Boys | Girls | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | Median (P25–P75) | % between 45–60% RI | n | Median (P25–P75) | % between 45–60% RI | ||||
| Carbohydrates (g/day) | SRS | 1 to <3 years | 45–60 | 84 | 136.3 (108.4–172.9) a | 60.6 | 78 | 134.7 (112.3–166.3) a | 62.6 |
| 3 to <6 years | 45–60 | 122 | 166.2 (145.3–191.2) b | 58.1 | 122 | 158.1 (132.2–194.5) b | 51.6 | ||
| 6 to <10 years | 45–60 | 151 | 194.3 (150.3–227.7) c | 67.1 | 150 | 176.7 (143.2–217.5) b | 46.9 | ||
| AMS | 1 to <3 years | 45–60 | 144 | 137.7 (112.8–167.1) a | 90.6 | 150 | 138.2 (115.2–166.2) a | 82.7 | |
| 3 to <6 years | 45–60 | 128 | 166.1 (138.5–199.9) b | 57.2 | 134 | 170.6 (141.1–197.8) b | 63.3 | ||
| 6 to <10 years | 45–60 | 99 | 183.5 (149.6–215.4) b | 64.9 | 86 | 180.0 (148.0–209.4) b | 69.9 | ||
| Starch (g/day) | SRS | 1 to <3 years | - | 84 | 54.6 (34.7–79.2) a | - | 78 | 54.0 (32.8–78.5) a | - |
| 3 to <6 years | - | 122 | 86.0 (65.1–109.4) b | - | 122 | 77.9 (60.5–107.0) b | - | ||
| 6 to <10 years | - | 151 | 107.5 (76.4–132.1) c | - | 150 | 99.2 (75.0–127.1) c | - | ||
| AMS | 1 to <3 years | - | 144 | 42.1 (28.5–66.1) *,a | - | 150 | 47.3 (34.1–70.0) a | - | |
| 3 to <6 years | - | 128 | 77.4 (63.2–102.3) b | - | 134 | 79.4 (62.9–99.7) b | - | ||
| 6 to <10 years | - | 99 | 93.5 (73.3–121.6) c | - | 86 | 95.3 (73.6–108.1) b | - | ||
| Total sugar (g/day) | SRS | 1 to <3 years | - | 84 | 77.9 (61.5–89.8) a | - | 78 | 75.9 (57.5–91.6) | - |
| 3 to <6 years | - | 122 | 78.0 (60.9–97.2) a,b | - | 122 | 75.5 (64.5–94.0) | - | ||
| 6 to <10 years | - | 151 | 86.1 (67.5–106.6) b | - | 150 | 73.4 (58.4–91.3) | - | ||
| AMS | 1 to <3 years | - | 144 | 72.3 (55.7–91.4) a | - | 150 | 67.9 (56.5–84.0) a | - | |
| 3 to <6 years | - | 128 | 80.8 (64.7–95.8) a,b | - | 134 | 78.4 (64.3–95.6) b | - | ||
| 6 to <10 years | - | 99 | 84.3 (68.8–103.2) b | - | 86 | 86.6 (64.1–103.2) *,b | - | ||
| Group | Group by Age | Boys | Girls | |||
|---|---|---|---|---|---|---|
| n | Median (P25–P75) | n | Median (P25–P75) | |||
| Carbohydrates (%) | SRS | 1 to <3 years | 84 | 46.4 (41.8–50.7) a | 78 | 45.9 (39.9–51.3) |
| 3 to <6 years | 122 | 44.9 (41.1–49.5) b | 122 | 44.4 (39.3–49.4) | ||
| 6 to <10 years | 151 | 45.0 (41.2–48.6) b | 150 | 45.4 (40.6–49.5) | ||
| AMS | 1 to <3 years | 144 | 48.4 (43.6–52.5) *,a | 150 | 47.6 (43.6–53.0) * | |
| 3 to <6 years | 128 | 46.2 (41.6–50.1) b | 134 | 46.0 (41.3–50.0) | ||
| 6 to <10 years | 99 | 45.0 (41.2–49.3) b | 86 | 45.8 (41.9–49.2) | ||
| Starch (%) | SRS | 1 to <3 years | 84 | 16.4 (13.6–23.6) a | 78 | 17.8 (13.7–22.9) a |
| 3 to <6 years | 122 | 24.0 (19.0–28.1) b | 122 | 22.5 (18.1–26.6) b | ||
| 6 to <10 years | 151 | 24.7 (20.9–28.6) b | 150 | 24.8 (20.7–29.7) c | ||
| AMS | 1 to <3 years | 144 | 15.0 (10.6–20.0) *,a | 150 | 17.3 (12.7–22.3) a | |
| 3 to <6 years | 128 | 21.8 (18.7–25.5) *,b | 134 | 21.8 (17.6–26.5) b | ||
| 6 to <10 years | 99 | 23.2 (19.2–27.7) b | 86 | 23.1 (19.7–27.3) b | ||
| Total sugar (%) | SRS | 1 to <3 years | 84 | 25.7 (20.5–31.1) a | 78 | 25.5 (20.6–30.6) a |
| 3 to <6 years | 122 | 20.8 (17.5–24.6) b | 122 | 21.8 (18.3–25.4) b | ||
| 6 to <10 years | 151 | 20.1 (16.9–24.7) b | 150 | 19.3 (15.9–22.7) c | ||
| AMS | 1 to <3 years | 144 | 25.4 (21.3–30.8) a | 150 | 24.4 (19.8–29.4) a | |
| 3 to <6 years | 128 | 22.9 (19.1–25.8) b | 134 | 21.7 (18.4–24.6) b | ||
| 6 to <10 years | 99 | 21.1 (17.8–24.0) b | 86 | 22.0 (17.3–25.0) b | ||
| Group | Group by Age | AI (g/Day) | Boys | Girls | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | Median (P25–P75) | >AI (%) | n | Median (P25–P75) | >AI (%) | ||||
| Fiber (g/day) | SRS | 1–3 years | 10 | 135 | 11.3 (7.9–14.2) | 61.0 | 127 | 10.2 (7.7–13.9) | 67.2 |
| 4–6 years | 14 | 105 | 12.0 (8.6–15.5) | 45.1 | 106 | 11.2 (7.8–14.9) | 34.8 | ||
| 7–10 years | 16 | 117 | 12.1 (8.6–15.2) | 17.9 | 117 | 11.3 (9.0–14.3) | 11.3 | ||
| AMS | 1–3 years | 10 | 200 | 10.4 (7.5–13.7) a | 65.3 | 214 | 10.1 (7.8–13.4) | 65.2 | |
| 4–6 years | 14 | 94 | 11.9 (9.2–14.7) b | 38.1 | 92 | 10.9 (8.5–13.9) | 20.4 | ||
| 7–10 years | 16 | 77 | 11.0 (8.4–14.3) a,b | 0.0 | 64 | 9.6 (8.0–14.2) | 7.2 | ||
| Geographical Distribution Group (Nielsen Areas) | n | Carbohydrates (g/Day) | Starch (g/Day) | Total Sugar (g/Day) | Fiber (g/Day) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SRS | AMS | SRS | AMS | SRS | AMS | SRS | AMS | SRS | AMS | ||
| Barcelona (Metropolitan Area) | 55 | 61 | 151.5 (141.0–191.7) | 155.8 (134.9–185.0) | 88.9 (68.9–107.3) | 79.8 (61.5–105.9) | 69.7 (57.9–84.5) | 68.5 (58.3–87.7) | 11.5 (8.4–15.2) | 11.0 (8.9–14.2) | |
| Canary Islands | 29 | 42 | 1656.0 (136.9–201.2) | 153.8 (128.1–185.8) | 67.5 (55.2–107.9) | 68.8 (46.5–91.8) | 84.2 (77.4–106.4) | 78.1 (58.6–96.3) | 11.2 (9.7–14.4) | 9.7 * (7.0–13.3) | |
| Center | 44 | 77 | 177.2 (146.1–202.4) | 160.9 * (129.8–183.2) | 83.7 (65.6–105.2) | 67.6 ** (42.1–86.1) | 84.4 (71.2–104.0) | 82.0 (67.7–98.7) | 9.9 (7.8–13.4) | 9.7 (7.2–13.4) | |
| East | 111 | 80 | 204.6 (156.5–232.9) | 167.6 *** (133.9–200.7) | 114.0 (78.1–139.1) | 86.9 *** (53.3–112.8) | 82.3 (62.6–100.2) | 69.5 ** (56.5–87.4) | 11.5 (9.9–15.0) | 9.9 ** (7.7–13.6) | |
| Madrid (Metropolitan Area) | 130 | 152 | 153.2 (128.3–183.8) | 150.2 (118.9–174.8) | 74.6 (52.3–96.6) | 68.2 * (39.0–91.3) | 74.4 (60.3–91.9) | 74.7 (57.7–89.3) | 10.8 (7.8–14.1) | 11.1 (8.1–14.0) | |
| Northeast | 57 | 74 | 145.9 (122.3–189.1) | 142.1 (116.6–173.7) | 79.2 (62.3–114.9) | 60.7 ** (41.1–93.3) | 67.6 (52.4–81.8) | 68.7 (54.7–82.5) | 12.2 (9.1–16.3) | 11.1 (8.8–13.3) | |
| Northwest | 94 | 86 | 153.3 (123.7–190.4) | 149.5 (125.8–184.5) | 72.5 (49.3–108.5) | 62.9 * (41.7–85.5) | 77.1 (58.8–96.5) | 77.3 (61.5–95.5) | 11.5 (7.1–14.9) | 10.4 (8.1–13.8) | |
| North Central | 68 | 62 | 178.3 (147.3–240.9) | 196.4 (153.1–264.7) | 89.6 (72.3–136.0) | 90.3 (56.2–130.8) | 82.4 (68.8–106.9) | 90.9 * (77.4–131.1) | 13.1 (10.4–17.5) | 13.2 (10.1–15.9) | |
| South | 119 | 107 | 158.3 (123.9–194.2) | 168.7 (132.4–198.4) | 77.5 (48.8–108.1) | 71.2 (45.2–93.8) | 80.5 (62.2–98.8) | 86.2 (66.0–105.8) | 9.7 (6.9–13.2) | 10.3 (7.8–13.4) | |
| n | Carbohydrates (g/Day) | Starch (g/Day) | Total Sugar (g/Day) | Fiber (g/Day) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | SRS | AMS | SRS | AMS | SRS | AMS | SRS | AMS | SRS | AMS | |
| BMI-for-age percentile | Severe underweight | 11 | 17 | 135.6 a (109.8–257.1) | 130.1 (108.3–165.9) | 65.3 (39.1–145.2) | 53.8 a,b (25.8–85.7) | 86.5 (41.7–111.9) | 70.3 (52.8–82.8) | 12.1 (10.1–15.7) | 9.7 (7.6–14.6) |
| Underweight | 80 | 83 | 125.4 a,b (125.4–184.1) | 158.3 (130.0–197.1) | 76.4 (52.8–104.5) | 74.6 b (53.0–99.5) | 74.9 (58.3–96.9) | 75.0 (63.2–89.9) | 10.4 (7.4–13.2) | 10.8 (8.0–14.1) | |
| Normal | 359 | 391 | 167.23 b (139.3–204.7) | 159.6 * (128.0–193.4) | 84.5 (63.2–113.1) | 75.3 ***,b (47.4–97.8) | 78.0 (62.6–93.8) | 75.2 (58.8–93.0) | 11.8 (8.5–14.9) | 10.5 *** (8.0–13.8) | |
| Overweight | 153 | 133 | 165.9 a,b (127.0–203.7) | 165.5 (132.7–197.6) | 84.6 (54.6–116.8) | 67.7 ***,a,b (40.0–92.4) | 76.0 (59.3–98.5) | 84.5 (65.0–99.9) | 11.3 (7.5–14.5) | 11.4 (8.7–14.1) | |
| Obesity | 104 | 117 | 165.6 a,b (135.6–206.9) | 153.7 * (126.2–182.7) | 86.4 (63.5–112.2) | 62.0 ***,a (37.5–89.6) | 80.1 (65.5–95.3) | 79.4 (61.9 – 94.0) | 11.0 (8.5–14.9) | 10.8 (7.7–13.6) | |
| n | Carbohydrates (g/Day) | Starch (g/Day) | Total Sugar (g/Day) | Fiber (g/Day) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | SRS | AMS | SRS | AMS | SRS | AMS | SRS | AMS | SRS | AMS | |
| Income Level (€/month) | Low (<1500 €) | 171 | 163 | 150.9 a (123.3–189.9) | 157.7 (128.9–187.7) | 77.2 a (50.0–106.6) | 74.5 a (54.1–98.2) | 76.9 (61.5–91.3) | 76.0 (57.9–92.6) | 10.7 a (7.4–14.3) | 9.6 a (7.7–13.2) |
| Medium (1501 to 2000 €) | 126 | 134 | 173.5 b (148.8–215.5) | 153.9 *** (122.5–178.9) | 89.7 b (66.6–117.5) | 59.7 ***,b (42.0–84.6) | 84.3 (62.8–108.1) | 74.6 (61.3–94.5) | 11.2 a,b (8.5–14.2) | 9.7 **,a (7.4–12.6) | |
| High (>2000 €) | 226 | 238 | 177.8 b (136.8–217.9) | 162.8 * (129.1–201.4) | 93.4 b (65.0–130.3) | 75.1 ***,a (44.3–103.1) | 78.5 (60.0–94.6) | 79.3 (61.5–93.6) | 11.8 b (8.8–15.2) | 11.4 b (8.5–14.1) | |
| No answer/ doesn’t know | 184 | 206 | 158.8 a (132.2–188.8) | 159.6 (127.9–191.1) | 81.1 a (56.1–104.2) | 73.2 *,a,b (42.7–96.1) | 75.4 (62.1–92.8) | 77.7 (63.6–96.5) | 11.5 a,b (7.8–14.4) | 11.2 b (8.6–14.5) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samaniego-Vaesken, M.d.L.; Partearroyo, T.; Valero, T.; Rodriguez, P.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Lara Villoslada, F.; Leis, R.; Victoria, E.M.d.; Moreno, J.M.; et al. Carbohydrates, Starch, Total Sugar, Fiber Intakes and Food Sources in Spanish Children Aged One to <10 Years—Results from the EsNuPI Study. Nutrients 2020, 12, 3171. https://doi.org/10.3390/nu12103171
Samaniego-Vaesken MdL, Partearroyo T, Valero T, Rodriguez P, Soto-Méndez MJ, Hernández-Ruiz Á, Lara Villoslada F, Leis R, Victoria EMd, Moreno JM, et al. Carbohydrates, Starch, Total Sugar, Fiber Intakes and Food Sources in Spanish Children Aged One to <10 Years—Results from the EsNuPI Study. Nutrients. 2020; 12(10):3171. https://doi.org/10.3390/nu12103171
Chicago/Turabian StyleSamaniego-Vaesken, Maria de Lourdes, Teresa Partearroyo, Teresa Valero, Paula Rodriguez, María José Soto-Méndez, Ángela Hernández-Ruiz, Federico Lara Villoslada, Rosaura Leis, Emilio Martínez de Victoria, José Manuel Moreno, and et al. 2020. "Carbohydrates, Starch, Total Sugar, Fiber Intakes and Food Sources in Spanish Children Aged One to <10 Years—Results from the EsNuPI Study" Nutrients 12, no. 10: 3171. https://doi.org/10.3390/nu12103171