
Herbal Remedies and Their Possible Effect on the GABAergic System and Sleep


1
Department of Developmental and Social Psychology, Sapienza University, 00185 Rome, Italy
2
Department of Neurology, Ospedale San Raffaele Turro, 20127 Milan, Italy
3
Sleep Disorders Center, Vita-Salute San Raffaele University, 20132 Milan, Italy
4
Department of Medical Affairs, Sanofi Consumer HealthCare, 20158 Milan, Italy
*
Author to whom correspondence should be addressed.
Nutrients 2021, 13(2), 530; https://doi.org/10.3390/nu13020530
Submission received: 13 January 2021
/
Revised: 29 January 2021
/
Accepted: 2 February 2021
/
Published: 6 February 2021
(This article belongs to the Section Phytochemicals and Human Health)
Abstract
:Sleep is an essential component of physical and emotional well-being, and lack, or disruption, of sleep due to insomnia is a highly prevalent problem. The interest in complementary and alternative medicines for treating or preventing insomnia has increased recently. Centuries-old herbal treatments, popular for their safety and effectiveness, include valerian, passionflower, lemon balm, lavender, and Californian poppy. These herbal medicines have been shown to reduce sleep latency and increase subjective and objective measures of sleep quality. Research into their molecular components revealed that their sedative and sleep-promoting properties rely on interactions with various neurotransmitter systems in the brain. Gamma-aminobutyric acid (GABA) is an inhibitory neurotransmitter that plays a major role in controlling different vigilance states. GABA receptors are the targets of many pharmacological treatments for insomnia, such as benzodiazepines. Here, we perform a systematic analysis of studies assessing the mechanisms of action of various herbal medicines on different subtypes of GABA receptors in the context of sleep control. Currently available evidence suggests that herbal extracts may exert some of their hypnotic and anxiolytic activity through interacting with GABA receptors and modulating GABAergic signaling in the brain, but their mechanism of action in the treatment of insomnia is not completely understood.
1. Introduction
Sleep is a fundamental physiological process required to maintain physical and emotional well-being. Healthy sleep is a crucial process for optimal cognitive performance, including attention, emotional reactivity, and learning and memory [1]. Sleep also contributes to a wide range of other physiological processes, e.g., metabolic and endocrine health and the strengthening of the immune system [2,3]. Chronic insomnia affects people across all geographies, socioeconomic levels, and cultures; because of this, sleeping pills are among the most frequently prescribed medicines worldwide [1,2].
It should be noted that multiple approved therapies for insomnia come with a safety warning, and some hypnotics (including, for example, barbiturates) have been abandoned because of unfavorable adverse event profiles or substance abuse [4]. In contrast, most herbal medicines for insomnia and anxiety offer an exceptional safety profile, sometimes with tenfold fewer adverse events than with pharmacotherapy [5,6,7]. Recent surveys suggest that almost two-thirds of individuals with sleep problems do not consult their doctor but search for treatment advice online, and herbal medicine remains a popular choice [8,9,10,11]. A number of recent studies demonstrate a steady increase in the uptake of complementary and alternative medicines for insomnia; the reasons for this increase may include dissatisfaction or concern for side effects with pharmacological treatment, previous positive experiences, and self-perceived effectiveness of alternative medicine [9,11,12].
Although their effectiveness is heavily debated, several herbal therapies for insomnia have been used for centuries, and many products, including valerian (Valeriana officinalis L.) and chamomile (Matricaria sp.), are still widely used today because of their good safety profile and their proposed anxiolytic and sedative proprieties [10,13,14,15,16,17].
Pharmacologically, herbal and traditional medicines represent complex mixtures of hundreds of constituents, making it difficult to isolate the active components and determine their exact mechanism of action [18]. Studies of several herbal remedies used for insomnia highlighted that changes in the central GABAergic neurotransmission could be responsible for the anxiolytic and the sedative properties of these remedies [13]. This is not surprising, as gamma-aminobutyric acid (GABA) is recognized as one of the main neurotransmitters responsible for sleep regulation. GABAA receptor modulation is one of the four key mechanisms of action of the approved pharmacological therapies for insomnia (the other three mechanisms are melatonin receptor agonism, histamine 1 receptor antagonism, and hypocretin/orexin antagonism) [1].
The aim of this review is to summarize the current knowledge of the GABA receptors in sleep regulation and to perform a systematic analysis of literature addressing the GABAergic mechanisms of action of herbal remedies for insomnia.
2. Stages of Sleep
Three distinct vigilance states can be identified on the basis of the level of arousal and electroencephalogram (EEG) activity: wakefulness, non-rapid eye movement (NREM), and rapid eye movement (REM) [2]. Healthy, young individuals usually experience several NREM and REM cycles during the night; the typical length of one NREM–REM cycle in humans is approximately 90 min [2,19].
The three vigilance states are regulated by wakefulness-promoting, NREM-promoting, and REM-promoting distinct neuronal groups (nuclei) located in the basal forebrain, thalamus, and brainstem [2,20]. Brain nuclei promoting different vigilance states exert reciprocally inhibitory activity and are involved in modulating the activity of numerous other structures of the central nervous system [2,20,21].
Wakefulness is regulated by a number of different neurotransmitter systems, including acetylcholine, serotonin, norepinephrine, histamine, orexins, neuropeptide S, dopamine, glutamate, and even GABA [2]. In the brainstem, the pontine locus coeruleus promotes wakefulness via excitatory connections to the cerebral cortex and inhibitory connections to sleep-promoting nuclei [22]. The alternation of NREM and REM sleep phases during the night is likely controlled by several mechanisms, including a reciprocal interaction of “REM-on” glutamatergic neurons in the pontine/mesencephalic reticular formation and “REM-off” norepinephrine/serotonin neurons in the dorsal raphe and the locus coeruleus [2,20]. Transition between vigilance states is orchestrated by the central pacemaker: the suprachiasmatic nucleus [20,23]. As the most widespread inhibitory neurotransmitter in the brain, GABA plays a role in inhibiting both “REM-on” and “REM-off” neurons in the brainstem and in regulating transitions between REM sleep and wakefulness or NREM sleep [2,23]. In addition, various groups of GABA neurons outside the brainstem are involved in the control of circadian timing and homeostatic regulation of sleep [2].
3. The Role of GABAergic Signaling in Sleep Physiology
As a major inhibitory neurotransmitter, GABA helps maintain the overall balance of neuronal excitation and inhibition in the central nervous system and plays one of the central roles in brain development and function [24]. Over 20% of all neurons in the brain are estimated to be GABAergic [25]. Three different GABA receptors, GABAA, GABAB, and GABAC, are involved in the regulation of sleep and arousal (albeit to different extents) [2,25]. The most commonly used hypnotics exert their effect on GABA systems, most notably through allosteric modulation of the benzodiazepine site [26,27,28]. Similarly, many herbal medicines have been proposed to enhance GABAergic signaling, many through interactions with the GABAA receptor [13].
3.1. GABAA Receptor
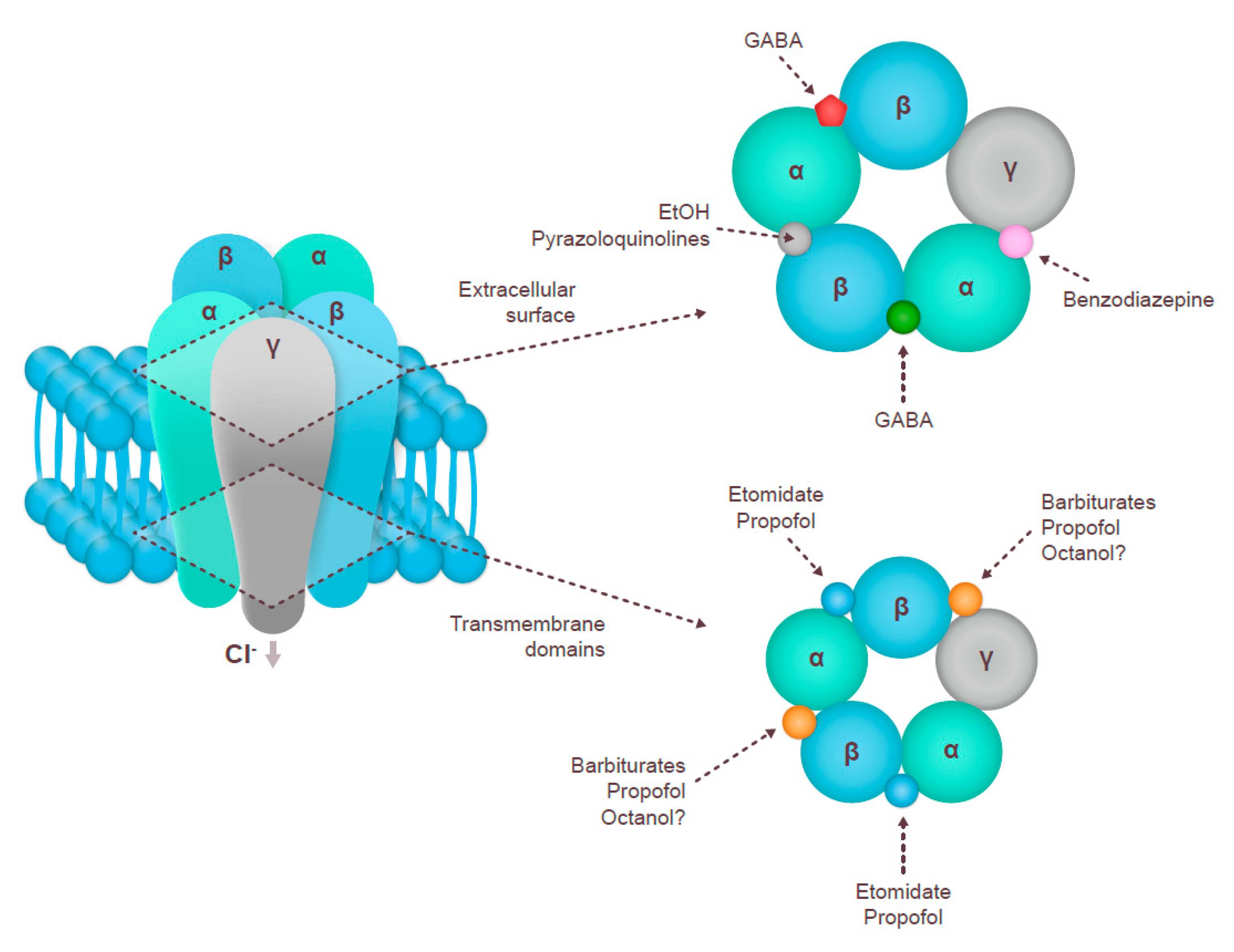
The fast-acting ionotropic GABAA receptors were the first to be discovered and have been the target of three generations of anxiolytics and hypnotics [1,2,29]. GABAA receptors are pentameric, ligand-gated Cl– ion channels; the classical synaptic subtypes are formed of two α, two β, and one γ or δ subunit, the α1β2γ2 receptor being the most abundant [29,30] (Figure 1).
Barbiturates were the first generation of sedative/hypnotic drugs introduced in the early 20th century. Their binding site on the GABAA receptor is different from that of GABA, and they act via direct activation of the receptor. Barbiturates do not show selective affinity to different receptor compositions of GABAA. Second-generation sleep aids (benzodiazepines) are GABAA allosteric modulators that bind to the interface between the α and the γ subunits across a range of receptor compositions [27,29,31]. Recently developed third-generation non-benzodiazepine hypnotics include, among others, zopiclone (a cyclopyrrolone), zolpidem (an imidazopyridine), and zaleplon (a pyrazolopyrimidine), which are sometimes collectively called the “Z drugs” [32]. All GABAA agonists help with entering and maintaining sleep by suppressing REM sleep and lower frequency waves while promoting high frequency waves [19]. The effects of GABAA agonists on sleep stages may vary; for example, eszopiclone does not have any effect on the length of NREM or REM sleep [33]. Reductions in theta and alpha frequencies have been observed in older, but not in young, adults with zolpidem; moreover, zolpidem decreased Stage 1 NREM in older adults, with no other age-related changes in sleep parameters [34].
3.2. GABAB Receptor
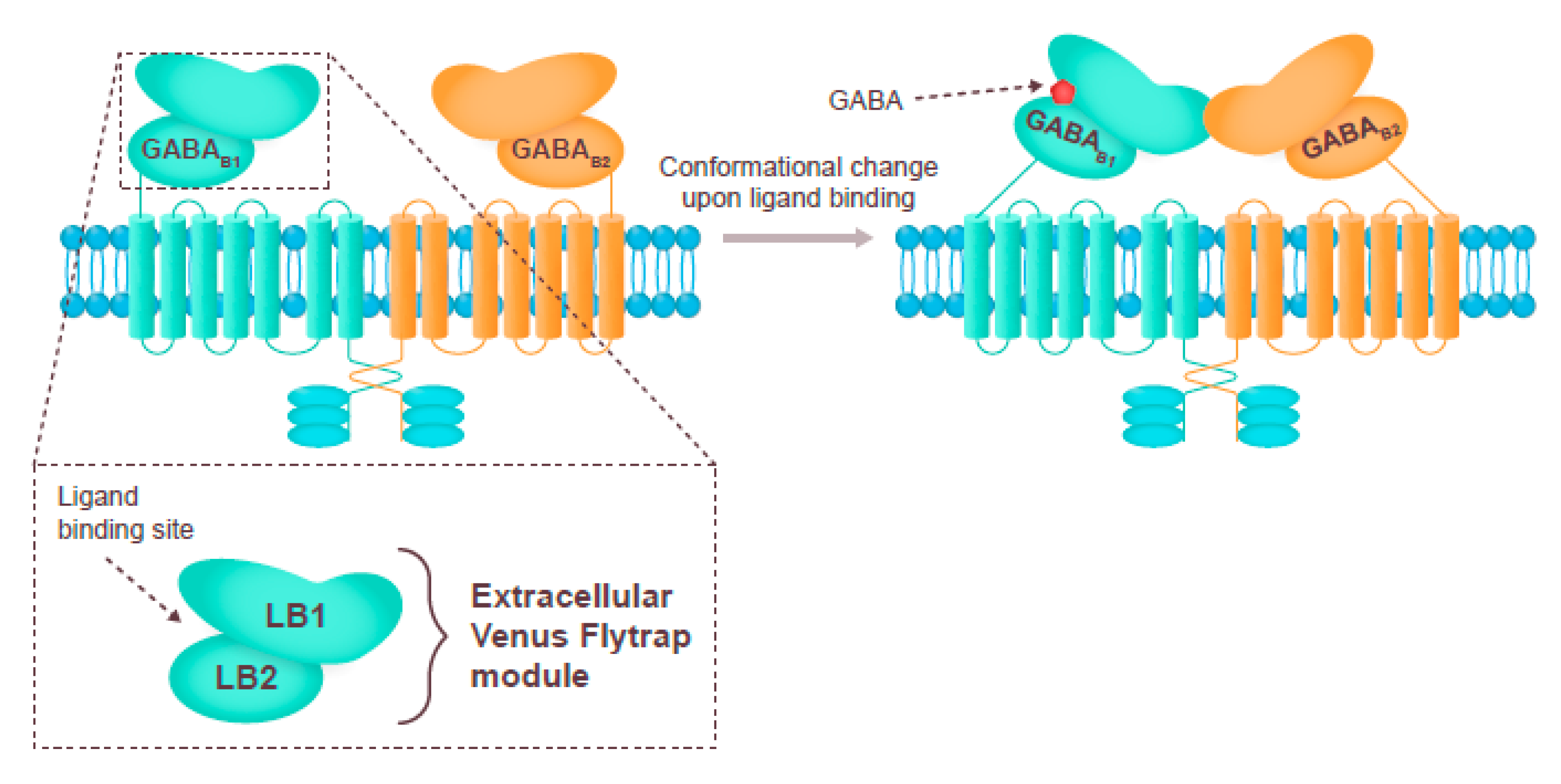
GABAB receptors are slow-acting metabotropic G-protein-linked dimers containing one GABAB1 (GABAB1a or GABAB1B) and one GABAB2 subunit [25,28,29] (Figure 2). Fewer drugs have been developed to target the GABAB receptor, baclofen being the most popular agonist, and there are less clinical data available than for the GABAA receptor [27,35]. Although GABAB agonists may promote sleep by increasing the duration of NREM and REM sleep, the effect is believed to be largely off-target [28,36]. Binding to the GABAB receptor may be responsible for the sleep-promoting effects of the drug gamma hydroxybutyrate. Activation of GABAB receptors on hypocretin/orexin neurons increases the power and duration of slow wave sleep and decreases the frequency of transitions between wakefulness and REM sleep [37,38].
3.3. GABAC Receptor
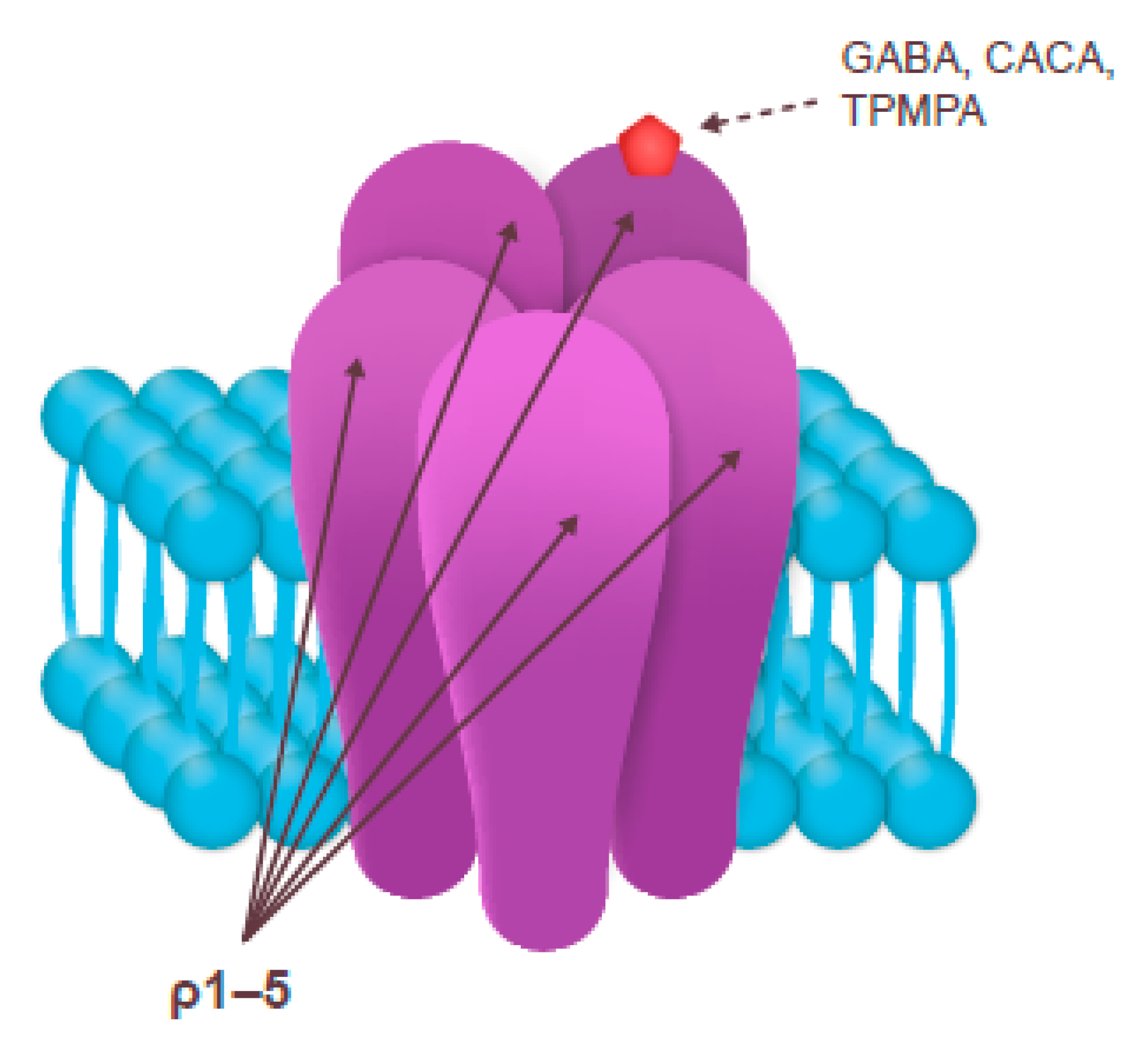
The subclass of GABAA receptors containing ρ subunits is often called GABAC or GABA-ρ; they belong to the same family of fast-acting pentameric, ligand-gated Cl– ion channels as GABAA [25,27,41] (Figure 3). Although both GABAA and GABAC receptors bind GABA, they have separate sets of agonists and antagonists. GABAC receptors are more sensitive to GABA than the other two receptor subclasses [25].
A selective GABAC antagonist (1,2,5,6-tetrahydropyridin-4-yl) methylphosphinic acid (TPMPA) has been shown to decrease the relative duration of NREM and REM sleep in rats [42]. In contrast, the selective partial GABAC agonist cis-4-aminocrotonic acid (CACA) does not have any effect on the relative duration of REM sleep [43].
A number of studies suggest that different classes of GABA receptors may play varying roles in sleep control, e.g., promoting different phases of sleep [25]. The expression pattern of each class and the cellular localization (synaptic or extrasynaptic) may play a role in the extent of the receptor involvement in sleep control [19]. This involvement may be influenced by other physiological and pathological conditions; for example, sleep deficits in slow wave sleep recorded in patients with schizophrenia may be specifically linked to the GABAB receptor [44]. Although most of the currently available hypnotics target GABAA, ongoing research on the physiology and pharmacology of the other two types of GABA receptors may lead to development of therapies for insomnia targeting GABAB or GABAC.
4. Herbal Remedies Acting on GABA Metabolism and Function
Herbal medicine, i.e., applications of plants or plant-derived materials for therapeutic purposes, has been used for centuries to treat a range of sleep disorders; notable examples include valerian (Valeriana officinalis L.), passionflower (Passiflora incarnata L.), lemon balm (Melissa officinalis L.), and Californian poppy (Eschscholzia californica Cham.) [13,16]. More recently, therapies being tested for efficacy in insomnia have included combinations of herbal extracts with melatonin and vitamin B6 [45]. A growing body of recent research has been dedicated to dissecting the content of naturally derived sleep aids and to determining the specific compounds responsible for their sedative properties. Multiple mechanisms of actions have been proposed, including those that promote GABAergic signaling, most commonly through an interaction of the active component with the GABAA receptor [6,13,46].
4.1. Systematic Literature Review
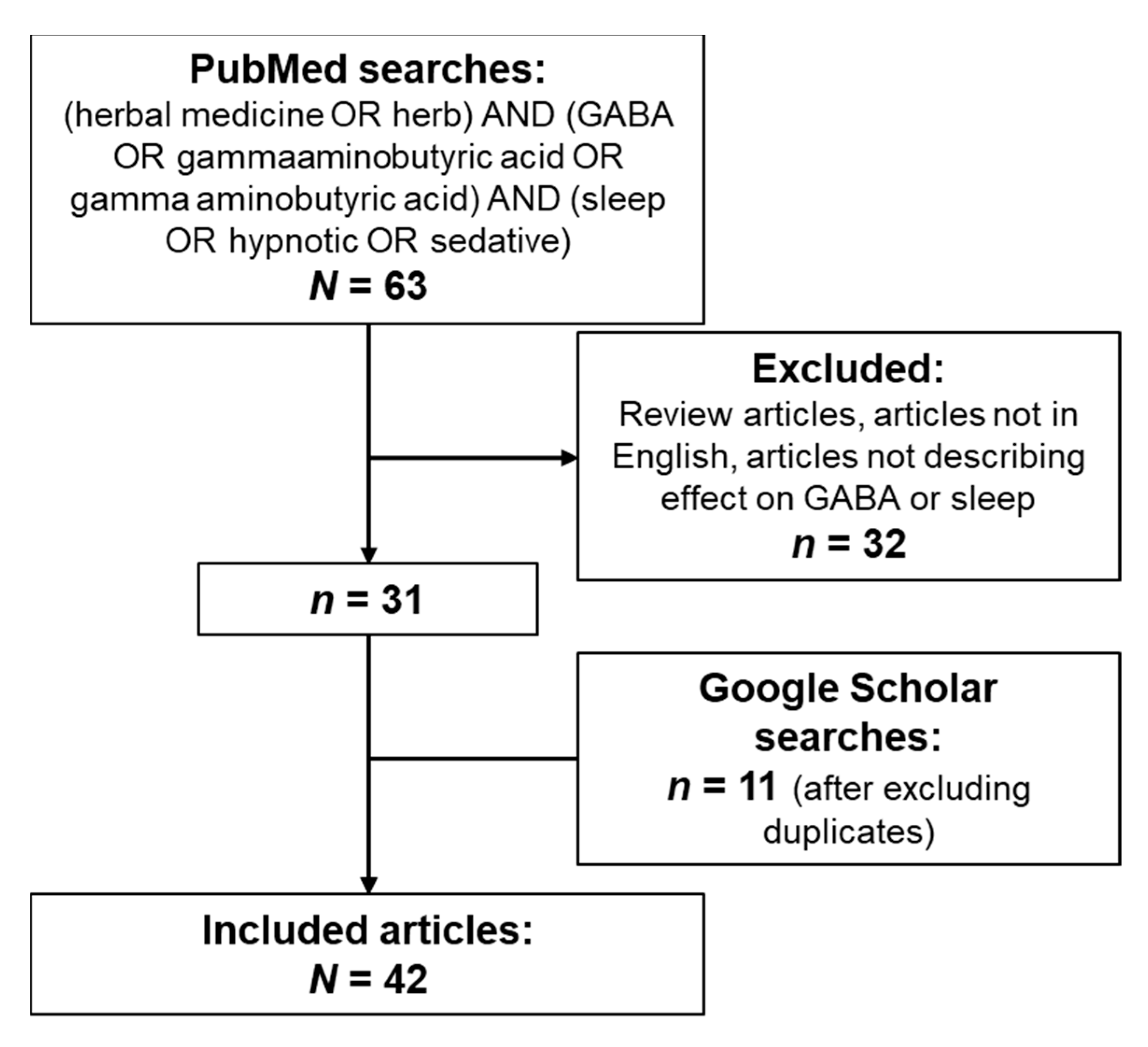
We have searched PubMed and Google Scholar for publications describing GABAergic effects of herbal medicines and their active components that could explain their mechanism of action in sleep regulation. The search terms included (“herbal medicine” OR “herb”) AND (“GABA” OR “gammaaminobutyric acid” OR “gamma aminobutyric acid”) AND (“sleep” OR “hypnotic” OR “sedative”).
The PubMed search returned 63 results; after removing reviews, articles not in English, and studies that did not assess GABAergic effects or sleep, 31 results were included. A number of additional publications were identified through Google Scholar searches; after removing duplicates, 11 additional articles were added to the reference library (Figure 4).
4.2. Natural Compounds Acting on GABAA, GABAB, and GABAC
We analyzed the articles identified in the literature search for the description of specific mechanisms of action targeting GABAergic signaling in sleep. The results of the literature analysis are shown in Table 1.
The vast majority of herbal medicines acted through the GABAA receptor (mostly via binding to the GABA or benzodiazepine sites) (Figure 1). The specific chemicals that serve as natural modulators of the GABAA receptor (alkanes and alkaloids, flavones, flavonoids and isoflavonoids, phenols, terpenes, coumarins, etc.) have been described in detail in a recent review that addressed the specific pharmacological features of their interactions with the receptor [46]. Here, we present a broader summary of herbal extracts that may be used to regulate sleep, possibly acting via GABAergic signaling.
The largest body of evidence for GABAA modulation is associated with valerian root (Valeriana officinalis L.), which is widely used to reduce the latency of sleep onset and increase sleep quality [13,79]. Valerian root extract contains over 150 chemical constituents including alkaloids, terpenes, organic acids and their derivatives, valepotriates and flavones [13,48]. GABA itself may be present in the valerian extracts, although its bioavailability is questionable [5]. Notably, small differences have been reported between extracts from plants grown in different conditions or processed in a different manner, and large-scale producers have standardized protocols of plant growth and extract preparation aimed at reducing variability [48]. Studies in tissue culture and animal models suggest that components of valerian extract (Valeriana officinalis L.) possess prominent dose-dependent GABAA agonistic activity [49,51]. 6-methylapigenin is a potent positive modulator of GABAA, possibly binding to the benzodiazepine site at the interface of α and γ subunits, whereas valerenic acid and valerenol have been shown to interact with the β subunit of the receptor [47,48].
Magnolia sp., Artemisia sp., Chinese magnolia vine (Schisandra chinensis), lotus (Nelumbo nucifera), and drumstick tree (Moringa oleifera) have all been shown to contain GABAA agonists that promote sleep in various animal models. A potent GABAergic effect via the GABAA receptor (benzodiazepine site) has been demonstrated for herbal mixes used in traditional medicine in Japan (yokukansan) and China (suanzaorentang); however, the specific herbs and compounds responsible for the effect remain to be identified [76,78]. A number of different approaches can be used to identify these compounds; for example, in one study, an in silico screen of a traditional Chinese medicine library was performed and found that 2-O-caffeoyl tartaric acid, 2-O-feruloyl tartaric acid, and mumefural are potent GABAA receptor agonists at both GABA and benzodiazepine binding sites [80]. Tartaric acid derivatives are present in various fruit syrups and juices, and mumeferal is derived from the processed fruit of Japanese apricot (Prunus mume Sieb. et Zucc.) (a traditional health food) [81].
Extract of dried flowers of chamomile (Matricaria sp.) has been used as a mild tranquilizer and sleep inducer for thousands of years and contains 28 terpenoids and 36 flavonoids [82,83]. Among them, apigenin has been shown to exhibit a hypnotic activity by activating the GABAA receptor at the benzodiazepine binding site [26,46,82]. Apigenin is an active component of several herbal sleep remedies such as passionflower (Passiflora incarnata L.), which is used to reduce sleep latency and increase sleep duration [13,46]. Other GABAA allosteric modulators acting at the benzodiazepine site include alkaloids isolated from the California poppy (Eschscholzia californica Cham.), which is used to induce relaxation and sleep [69].
There is much less evidence of herbal medicines interacting with the GABAB or the GABAC receptors. The extract of Passiflora incarnata has been shown to inhibit the binding of ligands to both GABAA and GABAB receptors in a concentration-dependent manner, suggesting that it contains antagonists of both receptor subtypes [65]. Notably, Passiflora incarnata L. extract contains a high amount of GABA and therefore has a potential to exert its hypnotic activity through all three types of GABA receptors, although its exact mechanism of action remains to be demonstrated [66]. The aqueous root extract of Indian ginseng (Withania somnifera L.) has been shown to act as a potent agonist of the GABAC receptor in addition to weakly activating GABAA [67]. Various natural compounds have been implicated in the plant’s mechanism of action, including withanone, withaferin A, and triethylene glycol [67,84].
4.3. Other Mechanisms of Action Related to GABA Signaling
Several indirect effects on GABA signaling have been reported for various medicinal plant extracts. Valerian root extract (Valeriana officinalis L.) may mediate inhibition of enzymatic destruction of GABA, increasing GABA availability [5]. Extract of Melissa officinalis L. decreases the level of GABA transaminase in hippocampal neurons [72]. Unidentified components of a Mexican tree Ternstroemia lineata DC. have been shown to promote GABA release in mouse brain slices [85]. Tenufolin, the active component of Polygala tenuifolia, increases the expression of GABA transporter 1 and GABA availability in animal models [70,71]. Activation of GABA synthesis through enhanced expression of glutamic acid decarboxylase (GAD) has been demonstrated for sanjoinine A, an alkaloid isolated from jujube (Zizyphus jujuba) [63]. Finally, although the Citrus aurantium essential oil exerts its anxiolytic effect via the serotonin receptor, an indirect effect on GABAergic system has been described as well [75,86]. These results suggest that herbal sleep medicines may have a plethora of direct and indirect effects on GABAergic signaling beyond direct interaction with GABA receptors.
5. Discussion and Conclusions
Insomnia is a widespread, often chronic, disorder that affects 5–15% of the general population and is associated with a great reduction in quality of life [1,2,87]. Among prescription medicines for insomnia, many therapies act via modulation of GABAergic signaling, including potent hypnotics such as benzodiazepines and “Z drugs” that bind to various sites on the GABAA receptor [1,27,30]. Although GABAB and GABAC receptors have distinct roles in controlling various stages of sleep, none of the currently approved prescription medicines target these receptor subtypes; however, ongoing research may lead to the development of such medicines in the future.
The ability of herbal extracts to reduce sleep latency, increase sleep duration, and improve sleep quality has been explored in numerous studies; however, robust clinical evidence supporting their use for the treatment of insomnia is currently lacking, emphasizing the need for research in this area [87,88]. Mechanistic studies have shown that herbal medicines used for the treatment of depression, anxiety, and insomnia may exert their effect through various mechanisms of action. Components of ginseng (Withania somnifera L.), Ginkgo biloba L., and St John’s Wort (Hypericum perforatum L.) have been shown to influence the reuptake of neurotransmitters, such as norepinephrine, dopamine, and serotonin [70,89,90]. Extracts of jujube seeds and valerian (Valeriana officinalis L.) directly interact with serotonin receptors [64,89], and Griffonia simplicifolia Baill. contains 5-hydroxytryptophan, a natural precursor of serotonin [91]. L-theanine, which is found in green tea, has been discovered to potentiate GABA, dopamine, and serotonin receptors and to inhibit glutamate reuptake [92]. Active components of lavender (Lavandula angustifolia Miller) can bind the glutamate N-methyl-D-aspartate receptors and serotonin transporters [93]. Finally, several herbal substances may interact with glutamic acid decarboxylase or modulate GABA and serotonin receptors [6,88,94]. Sleep-promoting GABAergic neurons represent the main cellular target of pharmacological therapies for insomnia, and GABA signaling appears to be the target of a large number of over-the-counter herbal sleep aids [1,2,13]. The exceptional safety profile of herbal medicines, especially when compared with pharmacotherapy for insomnia, and their wide acceptance by patients, serve as a strong argument in favor of further investigations that aim to define their mechanism of action more precisely and that aim to confirm their clinical efficacy in terms of specific sleep parameters.
In conclusion, despite the availability of multiple hypnotic drugs, side effects remain an issue, and there is ongoing demand for safer treatment options for insomnia. The evidence reviewed here suggests that multiple plant-derived substances may serve as sleep aids by modulating GABAergic signaling in the brain. The exceptional safety profile of herbal medicines and their wide acceptance by patients serve as a strong argument in favor of further investigations of their mechanism of action and identification of specific compounds that exert the hypnotic effect.
Author Contributions
All authors discussed and agreed on the concept of the review. P.P. and E.G. drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
Editorial support was provided by Olga Ucar and Ella Palmer of inScience Communications, Springer Healthcare Ltd., UK and was funded by Sanofi.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The study did not report any data; all references used in the review are included in the reference list.
Acknowledgments
The authors thank Claire Bertin and Lamia Achour of Sanofi Consumer HealthCare for providing helpful scientific insight throughout manuscript development.
Conflicts of Interest
O.B. and L.F.-S. declare no conflicts of interest. E.G. and P.P. are employees of Sanofi.
References
- Avidan, A.Y.; Neubauer, D.N. Chronic Insomnia Disorder. Continuum (Minneap Minn) 2017, 23, 1064–1092. [Google Scholar] [CrossRef] [Green Version]
- Brown, R.E.; Basheer, R.; McKenna, J.T.; Strecker, R.E.; McCarley, R.W. Control of Sleep and Wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leproult, R.; Van Cauter, E. Role of sleep and sleep loss in hormonal release and metabolism. Endocr. Dev. 2010, 17, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Kripke, D.F. Hypnotic drug risks of mortality, infection, depression, and cancer: But lack of benefit. F1000Research 2016, 5, 918. [Google Scholar] [CrossRef] [PubMed]
- Monograph. Valeriana officinalis. Altern. Med. Rev. 2004, 9, 438–441. [Google Scholar]
- Awad, R.; Levac, D.; Cybulska, P.; Merali, Z.; Trudeau, V.L.; Arnason, J.T. Effects of traditionally used anxiolytic botanicals on enzymes of the gamma-aminobutyric acid (GABA) system. Can. J. Physiol. Pharmacol. 2007, 85, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Schulz, V. Safety of St. John’s Wort extract compared to synthetic antidepressants. Phytomedicine 2006, 13, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Philips. The global pursuit of better sleep health. In Global Sleep Survey; Philips: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Welz, A.N.; Emberger-Klein, A.; Menrad, K. Why people use herbal medicine: Insights from a focus-group study in Germany. BMC Complementary Altern. Med. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, P.; Wu, X.; Zhang, Y.; Cong, D. Effectiveness of Chinese herbal medicine for patients with primary insomnia: A PRISMA-compliant meta-analysis. Medicine (Baltimore) 2019, 98, e15967. [Google Scholar] [CrossRef]
- Frass, M.; Strassl, R.P.; Friehs, H.; Mullner, M.; Kundi, M.; Kaye, A.D. Use and acceptance of complementary and alternative medicine among the general population and medical personnel: A systematic review. Ochsner J. 2012, 12, 45–56. [Google Scholar]
- Ashraf, M.; Saeed, H.; Saleem, Z.; Rathore, H.A.; Rasool, F.; Tahir, E.; Bhatti, T.; Khalid, J.; Bhatti, I.; Tariq, A. A cross-sectional assessment of knowledge, attitudes and self-perceived effectiveness of complementary and alternative medicine among pharmacy and non-pharmacy university students. BMC Complementary Altern. Med. 2019, 19, 95. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Dong, J.W.; Zhao, J.H.; Tang, L.N.; Zhang, J.J. Herbal Insomnia Medications that Target GABAergic Systems: A Review of the Psychopharmacological Evidence. Curr. Neuropharmacol. 2014, 12, 289–302. [Google Scholar] [CrossRef] [PubMed]
- Yeung, W.F.; Chung, K.F.; Poon, M.M.; Ho, F.Y.; Zhang, S.P.; Zhang, Z.J.; Ziea, E.T.; Wong, V.T. Chinese herbal medicine for insomnia: A systematic review of randomized controlled trials. Sleep Med. Rev. 2012, 16, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.L.; Gu, Y.; Wang, W.W.; Lu, L.; Fu, D.L.; Liu, A.J.; Li, H.Q.; Li, J.H.; Lin, Y.; Tang, W.J.; et al. Efficacy and safety of Suanzaoren decoction for primary insomnia: A systematic review of randomized controlled trials. BMC Complementary Altern. Med. 2013, 13, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegelhalder, K.; Nissen, C.; Riemann, D. Clinical Sleep—Wake Disorders II: Focus on Insomnia and Circadian Rhythm Sleep Disorders. In Sleep-Wake Neurobiology and Pharmacology; Landolt, H.-P., Dijk, D.-J., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 261–276. [Google Scholar] [CrossRef]
- Meolie, A.L.; Rosen, C.; Kristo, D.; Kohrman, M.; Gooneratne, N.; Aguillard, R.N.; Fayle, R.; Troell, R.; Townsend, D.; Claman, D.; et al. Oral nonprescription treatment for insomnia: An evaluation of products with limited evidence. J. Clin. Sleep Med. 2005, 1, 173–187. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. National Policy on Traditional Medicine and Regulation of Herbal Medicines; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Steiger, A. Sleep and Its Modulation by Substances That Affect GABAA Receptor Function. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 121–146. [Google Scholar] [CrossRef]
- Pal, D.; Mallick, B.N. GABA-ergic Modulation of Pontine Cholinergic and Noradrenergic Neurons for REM Sleep Generation. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 199–212. [Google Scholar] [CrossRef]
- Szabadi, E. Selective targets for arousal-modifying drugs: Implications for the treatment of sleep disorders. Drug Discov. Today 2014, 19, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Szabadi, E. Functional neuroanatomy of the central noradrenergic system. J. Psychopharmacol. 2013, 27, 659–693. [Google Scholar] [CrossRef] [PubMed]
- Reinoso-Suárez, F.; de la Roza, C.; Rodrigo-Angulo, M.L.; de Andrés, I.; Núñez, Á.; Garzón, M. GABAergic Mechanisms in the Ventral Oral Pontine Tegmentum: The REM Sleep—Induction Site—In the Modulation of Sleep—Wake States. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 233–252. [Google Scholar] [CrossRef]
- Möhler, H. Physiology and Pharmacology of the GABA System: Focus on GABA Receptors. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 3–23. [Google Scholar] [CrossRef]
- Gottesmann, C. Function of GABAB and ρ-Containing GABAA Receptors (GABAC Receptors) in the Regulation of Basic and Higher Integrated Sleep-Waking Processes. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 169–188. [Google Scholar] [CrossRef]
- Chebib, M.; Hanrahan, J.R.; Mewett, K.N.; Duke, R.K.; Johnston, G.A.R. Ionotropic GABA Receptors as Therapeutic Targets for Memory and Sleep Disorders. In Annual Reports in Medicinal Chemistry; Elsevier: Amsterdam, The Netherlands, 2004; pp. 13–23. [Google Scholar] [CrossRef]
- Vargas, R. The GABAergic System: An Overview of Physiology, Physiopathology and Therapeutics. Int. J. Clin. Pharmacol. Pharmacother. 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- Wisden, W.; Yu, X.; Franks, N.P. GABA Receptors and the Pharmacology of Sleep. In Sleep-Wake Neurobiology and Pharmacology; Landolt, H.-P., Dijk, D.-J., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 279–304. [Google Scholar] [CrossRef]
- Nutt, D. GABAA receptors: Subtypes, regional distribution, and function. J. Clin. Sleep Med. 2006, 2, S7–S11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharjee, A.; Wallner, M.; Lindemeyer, A.K.; Olsen, R.W. GABAA Receptor Physiology and Pharmacology. In The Oxford Handbook of Neuronal Ion Channels; Oxford University Press: Oxford, UK, 2018. [Google Scholar] [CrossRef]
- Uusi-Oukari, M.; Korpi, E.R. Regulation of GABAA Receptor Subunit Expression by Pharmacological Agents. Pharmacol. Rev. 2010, 62, 97–135. [Google Scholar] [CrossRef] [Green Version]
- Staner, L.; Cornette, F.; Otmani, S.; Nedelec, J.-F.; Danjou, P. Zolpidem in the Treatment of Adult and Elderly Primary Insomnia Patients. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 383–411. [Google Scholar] [CrossRef]
- Monti, J.M.; Pandi-Perumal, S.R. Eszopiclone: Its use in the treatment of insomnia. Neuropsychiatr. Dis. Treat. 2007, 3, 441–453. [Google Scholar] [PubMed]
- Chinoy, E.D.; Frey, D.J.; Kaslovsky, D.N.; Meyer, F.G.; Wright, K.P., Jr. Age-related changes in slow wave activity rise time and NREM sleep EEG with and without zolpidem in healthy young and older adults. Sleep Med. 2014, 15, 1037–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enna, S.J. GABAB receptor agonists and antagonists: Pharmacological properties and therapeutic possibilities. Expert Opin. Investig. Drugs 2005, 6, 1319–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vienne, J.; Bettler, B.; Franken, P.; Tafti, M. Differential effects of GABAB receptor subtypes, γ-hydroxybutyric Acid, and Baclofen on EEG activity and sleep regulation. J. Neurosci. 2010, 30, 14194–14204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wetter, T.C.; Beitinger, P.A.; Beitinger, M.E.; Wollweber, B. Pathophysiology of Sleep Disorders. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 325–361. [Google Scholar] [CrossRef]
- Landolt, H.-P.; Holst, S.C.; Valomon, A. Clinical and Experimental Human Sleep-Wake Pharmacogenetics. In Sleep-Wake Neurobiology and Pharmacology; Landolt, H.-P., Dijk, D.-J., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 207–241. [Google Scholar] [CrossRef] [Green Version]
- Benarroch, E.E. GABAB receptors: Structure, functions, and clinical implications. Neurology 2012, 78, 578–584. [Google Scholar] [CrossRef]
- Geng, Y.; Bush, M.; Mosyak, L.; Wang, F.; Fan, Q.R. Structural mechanism of ligand activation in human GABA(B) receptor. Nature 2013, 504, 254–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naffaa, M.M.; Hung, S.; Chebib, M.; Johnston, G.A.R.; Hanrahan, J.R. GABA-ρ receptors: Distinctive functions and molecular pharmacology. Br. J. Pharmacol. 2017, 174, 1881–1894. [Google Scholar] [CrossRef] [Green Version]
- Arnaud, C.; Gauthier, P.; Gottesmann, C. Study of a GABAC receptor antagonist on sleep-waking behavior in rats. Psychopharmacology (Berlin) 2001, 154, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Ulloor, J.; Mavanji, V.; Saha, S.; Siwek, D.F.; Datta, S. Spontaneous REM sleep is modulated by the activation of the pedunculopontine tegmental GABAB receptors in the freely moving rat. J. Neurophysiol. 2004, 91, 1822–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantrowitz, J.; Citrome, L.; Javitt, D. GABA(B) receptors, schizophrenia and sleep dysfunction: A review of the relationship and its potential clinical and therapeutic implications. CNS Drugs 2009, 23, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, P.; Bablon, J.-C.; Da Silva, C. A combination of melatonin, vitamin B6 and medicinal plants in the treatment of mild-to-moderate insomnia: A prospective pilot study. Complementary Ther. Med. 2019, 45, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Cicek, S.S. Structure-Dependent Activity of Natural GABA(A) Receptor Modulators. Molecules 2018, 23, 1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benke, D.; Barberis, A.; Kopp, S.; Altmann, K.H.; Schubiger, M.; Vogt, K.E.; Rudolph, U.; Mohler, H. GABA A receptors as in vivo substrate for the anxiolytic action of valerenic acid, a major constituent of valerian root extracts. Neuropharmacology 2009, 56, 174–181. [Google Scholar] [CrossRef] [Green Version]
- Patočka, J.; Jakl, J. Biomedically relevant chemical constituents of Valeriana officinalis. J. Appl. Biomed. 2010, 8, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Yuan, C.-S.; Mehendale, S.; Xiao, Y.; Aung, H.H.; Xie, J.-T.; Ang-Lee, M.K. The Gamma-Aminobutyric Acidergic Effects of Valerian and Valerenic Acid on Rat Brainstem Neuronal Activity. Anesth. Analg. 2004, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Mineo, L.; Concerto, C.; Patel, D.; Mayorga, T.; Paula, M.; Chusid, E.; Aguglia, E.; Battaglia, F. Valeriana officinalis Root Extract Modulates Cortical Excitatory Circuits in Humans. Neuropsychobiology 2017, 75, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Khom, S.; Baburin, I.; Timin, E.; Hohaus, A.; Trauner, G.; Kopp, B.; Hering, S. Valerenic acid potentiates and inhibits GABA(A) receptors: Molecular mechanism and subunit specificity. Neuropharmacology 2007, 53, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Alexeev, M.; Grosenbaugh, D.K.; Mott, D.D.; Fisher, J.L. The natural products magnolol and honokiol are positive allosteric modulators of both synaptic and extra-synaptic GABA(A) receptors. Neuropharmacology 2012, 62, 2507–2514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, W.M.; Yue, X.F.; Sun, Y.; Fan, K.; Chen, C.R.; Hou, Y.P.; Urade, Y.; Huang, Z.L. Honokiol promotes non-rapid eye movement sleep via the benzodiazepine site of the GABA(A) receptor in mice. Br. J. Pharmacol. 2012, 167, 587–598. [Google Scholar] [CrossRef] [Green Version]
- Squires, R.F.; Ai, J.; Witt, M.R.; Kahnberg, P.; Saederup, E.; Sterner, O.; Nielsen, M. Honokiol and magnolol increase the number of [3H] muscimol binding sites three-fold in rat forebrain membranes in vitro using a filtration assay, by allosterically increasing the affinities of low-affinity sites. Neurochem. Res. 1999, 24, 1593–1602. [Google Scholar] [CrossRef]
- Li, N.; Liu, J.; Wang, M.; Yu, Z.; Zhu, K.; Gao, J.; Wang, C.; Sun, J.; Chen, J.; Li, H. Sedative and hypnotic effects of Schisandrin B through increasing GABA/Glu ratio and upregulating the expression of GABA(A) in mice and rats. Biomed. Pharmacother. 2018, 103, 509–516. [Google Scholar] [CrossRef]
- Wang, M.; Li, N.; Jing, S.; Wang, C.; Sun, J.; Li, H.; Liu, J.; Chen, J. Schisandrin B exerts hypnotic effects in PCPA-treated rats by increasing hypothalamic 5-HT and γ-aminobutyric acid levels. Exp. Ther. Med. 2020, 20, 142. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhao, X.; Mao, X.; Liu, A.; Liu, Z.; Li, X.; Bi, K.; Jia, Y. Pharmacological evaluation of sedative and hypnotic effects of schizandrin through the modification of pentobarbital-induced sleep behaviors in mice. Eur. J. Pharmacol 2014, 744, 157–163. [Google Scholar] [CrossRef]
- Emadi, F.; Yassa, N.; Hadjiakhoondi, A.; Beyer, C.; Sharifzadeh, M. Sedative effects of Iranian Artemisia annua in mice: Possible benzodiazepine receptors involvement. Pharm. Biol. 2011, 49, 784–788. [Google Scholar] [CrossRef]
- Kavvadias, D.; Abou-Mandour, A.A.; Czygan, F.C.; Beckmann, H.; Sand, P.; Riederer, P.; Schreier, P. Identification of benzodiazepines in Artemisia dracunculus and Solanum tuberosum rationalizing their endogenous formation in plant tissue. Biochem. Biophys. Res. Commun. 2000, 269, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.Z.; Chang, Q.; Zhong, Y.; Xiao, B.X.; Feng, L.; Cao, F.R.; Pan, R.L.; Zhang, Z.S.; Liao, Y.H.; Liu, X.M. Lotus Leaf Alkaloid Extract Displays Sedative-Hypnotic and Anxiolytic Effects through GABAA Receptor. J. Agric. Food Chem. 2015, 63, 9277–9285. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.L.; Wu, B.F.; Shang, J.H.; Zhao, Y.L.; Huang, A.X. Moringa oleifera Lam Seed Oil Augments Pentobarbital-Induced Sleeping Behaviors in Mice via GABAergic Systems. J. Agric. Food Chem. 2020, 68, 3149–3162. [Google Scholar] [CrossRef]
- Shinomiya, K.; Inoue, T.; Utsu, Y.; Tokunaga, S.; Masuoka, T.; Ohmori, A.; Kamei, C. Effects of kava-kava extract on the sleep-wake cycle in sleep-disturbed rats. Psychopharmacology (Berlin) 2005, 180, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Han, H.; Eun, J.S.; Kim, H.C.; Hong, J.T.; Oh, K.W. Sanjoinine A isolated from Zizyphi Spinosi Semen augments pentobarbital-induced sleeping behaviors through the modification of GABA-ergic systems. Biol. Pharm. Bull. 2007, 30, 1748–1753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, P.L.; Lin, C.P.; Tsai, C.H.; Lin, J.G.; Chang, F.C. The involvement of serotonin receptors in suanzaorentang-induced sleep alteration. J. Biomed. Sci. 2007, 14, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Appel, K.; Rose, T.; Fiebich, B.; Kammler, T.; Hoffmann, C.; Weiss, G. Modulation of the gamma-aminobutyric acid (GABA) system by Passiflora incarnata L. Phytother. Res. 2011, 25, 838–843. [Google Scholar] [CrossRef]
- Elsas, S.M.; Rossi, D.J.; Raber, J.; White, G.; Seeley, C.A.; Gregory, W.L.; Mohr, C.; Pfankuch, T.; Soumyanath, A. Passiflora incarnata L. (Passionflower) extracts elicit GABA currents in hippocampal neurons in vitro, and show anxiogenic and anticonvulsant effects in vivo, varying with extraction method. Phytomedicine 2010, 17, 940–949. [Google Scholar] [CrossRef] [Green Version]
- Candelario, M.; Cuellar, E.; Reyes-Ruiz, J.M.; Darabedian, N.; Feimeng, Z.; Miledi, R.; Russo-Neustadt, A.; Limon, A. Direct evidence for GABAergic activity of Withania somnifera on mammalian ionotropic GABAA and GABArho receptors. J. Ethnopharmacol. 2015, 171, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Langade, D.; Kanchi, S.; Salve, J.; Debnath, K.; Ambegaokar, D. Efficacy and Safety of Ashwagandha (Withania somnifera) Root Extract in Insomnia and Anxiety: A Double-blind, Randomized, Placebo-controlled Study. Cureus 2019, 11, e5797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedurco, M.; Gregorová, J.; Šebrlová, K.; Kantorová, J.; Peš, O.; Baur, R.; Sigel, E.; Táborská, E. Modulatory Effects of Eschscholzia californica Alkaloids on Recombinant GABAAReceptors. Biochem. Res. Int. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.W.; Peng, C.B.; Pei, Z.; Zhang, M.R.; Yun, T.C.; Yang, Z.M.; Xu, F.P. Effects of tenuifolin on rest/wake behaviour in zebrafish. Exp. Ther. Med. 2020, 19, 2326–2334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, X.J.; Wang, G.Y.; Zhang, X.P.; Wang, Q.Q.; Peng, Z.P. Sedative and Hypnotic Effects and Transcriptome Analysis of Polygala tenuifolia in Aged Insomnia Rats. Chin. J. Integr. Med. 2020, 26, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Yoo, D.Y.; Choi, J.H.; Kim, W.; Yoo, K.Y.; Lee, C.H.; Yoon, Y.S.; Won, M.H.; Hwang, I.K. Effects of Melissa officinalis L. (lemon balm) extract on neurogenesis associated with serum corticosterone and GABA in the mouse dentate gyrus. Neurochem. Res. 2011, 36, 250–257. [Google Scholar] [CrossRef]
- Murray, B.J.; Cowen, P.J.; Sharpley, A.L. The effect of Li 1370, extract of Ginkgo biloba, on REM sleep in humans. Pharmacopsychiatry 2001, 34, 155–157. [Google Scholar] [CrossRef] [PubMed]
- Sharpley, A.L.; McGavin, C.L.; Whale, R.; Cowen, P.J. Antidepressant-like effect of Hypericum perforatum (St John’s wort) on the sleep polysomnogram. Psychopharmacology (Berlin) 1998, 139, 286–287. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.A.; Cury, T.C.; Cassettari, B.O.; Takahira, R.K.; Florio, J.C.; Costa, M. Citrus aurantium L. essential oil exhibits anxiolytic-like activity mediated by 5-HT(1A)-receptors and reduces cholesterol after repeated oral treatment. BMC Complementary Altern. Med. 2013, 13, 42. [Google Scholar] [CrossRef] [PubMed]
- Egashira, N.; Nogami, A.; Iwasaki, K.; Ishibashi, A.; Uchida, N.; Takasaki, K.; Mishima, K.; Nishimura, R.; Oishi, R.; Fujiwara, M. Yokukansan enhances pentobarbital-induced sleep in socially isolated mice: Possible involvement of GABA(A)-benzodiazepine receptor complex. J. Pharmacol. Sci. 2011, 116, 316–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozone, M.; Shimazaki, H.; Ichikawa, H.; Shigeta, M. Efficacy of yokukansan compared with clonazepam for rapid eye movement sleep behaviour disorder: A preliminary retrospective study. Psychogeriatrics 2020, 20, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Yi, P.L.; Tsai, C.H.; Chen, Y.C.; Chang, F.C. Gamma-aminobutyric acid (GABA) receptor mediates suanzaorentang, a traditional Chinese herb remedy, -induced sleep alteration. J. Biomed. Sci. 2007, 14, 285–297. [Google Scholar] [CrossRef]
- Pagel, J.F.; Kram, G. Insomnia: Differential Diagnosis and Current Treatment Approach. In GABA and Sleep: Molecular, Functional and Clinical Aspects; Monti, J.M., Pandi-Perumal, S.R., Möhler, H., Eds.; Springer: Basel, Switzerland, 2010; pp. 363–381. [Google Scholar] [CrossRef]
- Chen, H.Y.; Chang, S.S.; Chan, Y.C.; Chen, C.Y. Discovery of novel insomnia leads from screening traditional Chinese medicine database. J. Biomol. Struct. Dyn. 2014, 32, 776–791. [Google Scholar] [CrossRef]
- Kim, J.; Han, M.; Jeon, W.K. Acute and Subacute Oral Toxicity of Mumefural, Bioactive Compound Derived from Processed Fruit of Prunus mume Sieb. et Zucc., in ICR Mice. Nutrients 2020, 12, 1328. [Google Scholar] [CrossRef]
- Srivastava, J.K.; Shankar, E.; Gupta, S. Chamomile: A herbal medicine of the past with bright future. Mol. Med. Rep. 2010, 3, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Savage, K.; Firth, J.; Stough, C.; Sarris, J. GABA-modulating phytomedicines for anxiety: A systematic review of preclinical and clinical evidence. Phytother. Res. 2018, 32, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, M.K.; Kaul, S.C.; Wadhwa, R.; Yanagisawa, M.; Urade, Y. Triethylene glycol, an active component of Ashwagandha (Withania somnifera) leaves, is responsible for sleep induction. PLoS ONE 2017, 12, e0172508. [Google Scholar] [CrossRef] [PubMed]
- Lozada-Lechuga, J.; Villarreal, M.L.; Fliniaux, M.A.; Bensaddek, L.; Mesnard, F.; Gutierrez Mdel, C.; Cardoso-Taketa, A.T. Isolation of jacaranone, a sedative constituent extracted from the flowers of the Mexican tree Ternstroemia pringlei. J. Ethnopharmacol 2010, 127, 551–554. [Google Scholar] [CrossRef]
- Khosravi, M.; Khakpour, S.; Adibi, L.; Jahromy, M.H. A Study of the Effect of Citrus aurantium L. Essential Oil on Anxiety and Its Interaction with GABAergic Pathways in Male Mice. J. Behav. Brain Sci. 2014, 4, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Romero, K.; Goparaju, B.; Russo, K.; Westover, M.B.; Bianchi, M.T. Alternative remedies for insomnia: A proposed method for personalized therapeutic trials. Nat. Sci. Sleep 2017, 9, 97–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leach, M.J.; Page, A.T. Herbal medicine for insomnia: A systematic review and meta-analysis. Sleep Med. Rev. 2015, 24, 1–12. [Google Scholar] [CrossRef]
- Liu, L.; Liu, C.; Wang, Y.; Wang, P.; Li, Y.; Li, B. Herbal Medicine for Anxiety, Depression and Insomnia. Curr. Neuropharmacol. 2015, 13, 481–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, J.; Zheng, X.; Qu, L.; Zhang, H.; Yuan, H.; Hui, J.; Mi, Y.; Ma, P.; Fan, D. Ginsenoside Rg5/Rk1 ameliorated sleep via regulating the GABAergic/serotoninergic signaling pathway in a rodent model. Food Funct. 2020, 11, 1245–1257. [Google Scholar] [CrossRef] [PubMed]
- Lemaire, P.A.; Adosraku, R.K. An HPLC method for the direct assay of the serotonin precursor, 5-hydroxytrophan, in seeds of Griffonia simplicifolia. Phytochem. Anal. 2002, 13, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.; Gray, M.A.; Oliver, C.; Liley, D.T.; Harrison, B.J.; Bartholomeusz, C.F.; Phan, K.L.; Nathan, P.J. The acute effects of L-theanine in comparison with alprazolam on anticipatory anxiety in humans. Hum. Psychopharmacol. 2004, 19, 457–465. [Google Scholar] [CrossRef] [PubMed]
- López, V.; Nielsen, B.; Solas, M.; Ramírez, M.J.; Jäger, A.K. Exploring Pharmacological Mechanisms of Lavender (Lavandula angustifolia) Essential Oil on Central Nervous System Targets. Front. Pharmacol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.M.; Shimizu, M.; Lee, C.J.; Han, D.S.; Jung, C.K.; Jo, J.H.; Kim, Y.M. Hypnotic effects and binding studies for GABA(A) and 5-HT(2C) receptors of traditional medicinal plants used in Asia for insomnia. J. Ethnopharmacol. 2010, 132, 225–232. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The structure of the GABAA receptor and the location of common agonist and antagonist binding sites [26,29,30,31]. Cl−, chlorine ions; GABA, gamma-aminobutyric acid; EtOH, ethanol.

Figure 2.
The structure of the GABAB receptor, its ligand binding site, and the downstream signaling elements [39,40]. GABA, gamma-aminobutyric acid; LB, ligand binding.

Figure 3.
The structure and the ligand-binding site of the GABAC receptor [41]. CACA, cis-4-aminocrotonic acid; GABA, gamma-aminobutyric acid; ρ1–5, GABAC ρ subunits 1–5; TPMPA, (1,2,5,6-tetrahydropyridin-4-yl) methylphosphinic acid.
Figure 3.
The structure and the ligand-binding site of the GABAC receptor [41]. CACA, cis-4-aminocrotonic acid; GABA, gamma-aminobutyric acid; ρ1–5, GABAC ρ subunits 1–5; TPMPA, (1,2,5,6-tetrahydropyridin-4-yl) methylphosphinic acid.

Figure 4.
PRISMA flow diagram. GABA, gamma-aminobutyric acid; PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Figure 4.
PRISMA flow diagram. GABA, gamma-aminobutyric acid; PRISMA, preferred reporting items for systematic reviews and meta-analyses.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Common medicinal plants with known sleep-inducing properties that target GABAergic signaling.
Table 1.
Common medicinal plants with known sleep-inducing properties that target GABAergic signaling.
| Latin and Common Name | Known Chemical Components | Known Effect on Sleep | Target | Model | References |
|---|---|---|---|---|---|
| Individual Plants | |||||
| Valeriana officinalis L. (Valerian) | Alkaloids, terpenes, organic acids and their derivatives, valepotriates, and flavones | Reduces sleep latency, improves subjective measures | GABAA receptor | In vitro studies; clinical studies | [47,48,49,50,51] |
| Magnolia sp. | Magnolol and honokiol | Promotes REM sleep | GABAA receptor | In vitro studies; i.p. administration in mice | [52,53,54] |
| Schisandra chinensis (Turcz.) Baill. (Chinese magnolia-vine, Magnolia berry) | Schizandrin B | Promotes sleep | GABAA receptor | i.p. administration in mice and male rats | [55,56,57] |
| Artemisia sp. | Benzodiazepines | Reduces sleep latency | GABAA receptor | In vitro studies; i.p. administration in male mice | [58,59] |
| Nelumbo nucifera Gaertn. (Lotus) | Nuciferine, alkaloids | Promotes sleep | GABAA receptor | In vitro studies | [60] |
| Moringa oleifera Lam. (Drumstick tree) | Oleic acid, β-Sitosterol, and Stigmasterol | Increases sleep quality | GABAA receptor | p.o. administration in male mice | [61] |
| Piper methysticum L. (Kava-kava) | Kavapyrones | Decreases sleep latency; no effect on NREM sleep | GABAA receptor (not benzodiazepine site) | p.o. administration in mice | [62] |
| Zizyphus jujube (Jujube, or red date) | Sanjoinine A, suanzaorentang | Improves sleep quality, prolonging sleep time and increasing NREM sleep | GABAA receptor; activation of GABA synthesis through enhanced expression of GAD; serotonin receptors | i.p. and p.o. administration in male rats | [63,64] |
| Passiflora incarnata (Passionflower) | Apigenin, alkaloids, flavones | Reduces sleep latency, increases sleep duration | GABAA and GABAB receptors, (and possibly GABAC receptor) | In vitro studies; p.o. administration in mice | [65,66] |
| Withania somnifera L. (Indian ginseng) | Withanolide A, withaferin A | Reduces sleep latency, improves sleep quality | GABAA and GABAC receptors | In vitro studies; clinical studies | [67,68] |
| Eschscholzia californica Cham. (Californian poppy) | Alkaloids | Improves sleep latency and duration | GABAA receptor; serotonin receptor | In vitro studies | [69] |
| Polygala tenuifolia Willd. (Yuan Zhi) | Tenufolin | Increases sleep duration | Increases the levels of GABA and GABA transporter 1 | Zebrafish and rats | [70,71] |
| Melissa officinalis L. (Lemon balm) | Rosmarinic acid | Improves sleep quality | Decreases the level of GABA transaminase | In vitro studies; i.p. administration in mice | [72] |
| Ginkgo biloba L. (Ginkgo) | Ginkgotoxin, flavonoids, terpenoids | Improves subjective sleep quality measures | Inhibition of GAD activity | Clinical studies | [73] |
| Hypericum perforatum L. (St John’s Wort) | Hypericin, pseudohypericin, hyperoside, among others | Increases REM latency and deep sleep | Inhibition of GAD and GABA transporter activity | Clinical studies | [74] |
| Citrus aurantium L. (bitter orange) | Limonene, β-myrcene | Increases sleep duration | Serotonergic system; proposed interaction with GABA receptor binders, such as diazepam | p.o administration in male mice | [75] |
| Plant mixes | |||||
| Yokukansan (Atractylodes lancea rhizoma, Poria sclerotium, Cnidium rhizoma, Japanese Angelica radix, Bupleurum radix, Glycyrrhiza radix, and Uncaria thorn) | Various | Decreases sleep latency, improves dream content in the REM behavior disorder | GABAA receptor | p.o. administration in male mice; clinical studies | [76,77] |
| Suanzaorentang, a traditional Chinese medicine | Various | Increases NREM, no effect on REM sleep | GABAA receptor; serotonergic system | Clinical studies | [64,78] |
Herbal medicines were selected if their proposed mechanism of action involved GABA synthesis, transport, or receptors. GAD, glutamic acid decarboxylase; GABA, gamma-aminobutyric acid; i.p., intraperitoneal; NREM, non-rapid eye movement; p.o., oral; REM, rapid eye movement.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bruni, O.; Ferini-Strambi, L.; Giacomoni, E.; Pellegrino, P. Herbal Remedies and Their Possible Effect on the GABAergic System and Sleep. Nutrients 2021, 13, 530. https://doi.org/10.3390/nu13020530
AMA Style
Bruni O, Ferini-Strambi L, Giacomoni E, Pellegrino P. Herbal Remedies and Their Possible Effect on the GABAergic System and Sleep. Nutrients. 2021; 13(2):530. https://doi.org/10.3390/nu13020530
Chicago/Turabian StyleBruni, Oliviero, Luigi Ferini-Strambi, Elena Giacomoni, and Paolo Pellegrino. 2021. "Herbal Remedies and Their Possible Effect on the GABAergic System and Sleep" Nutrients 13, no. 2: 530. https://doi.org/10.3390/nu13020530
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.