
Quality and Quantity of Protein Intake Influence Incidence of Type 2 Diabetes Mellitus in Coronary Heart Disease Patients: From the CORDIOPREV Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Dietary Intervention
2.3. Dietary Intake Assessment
2.4. Laboratory Analysis
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
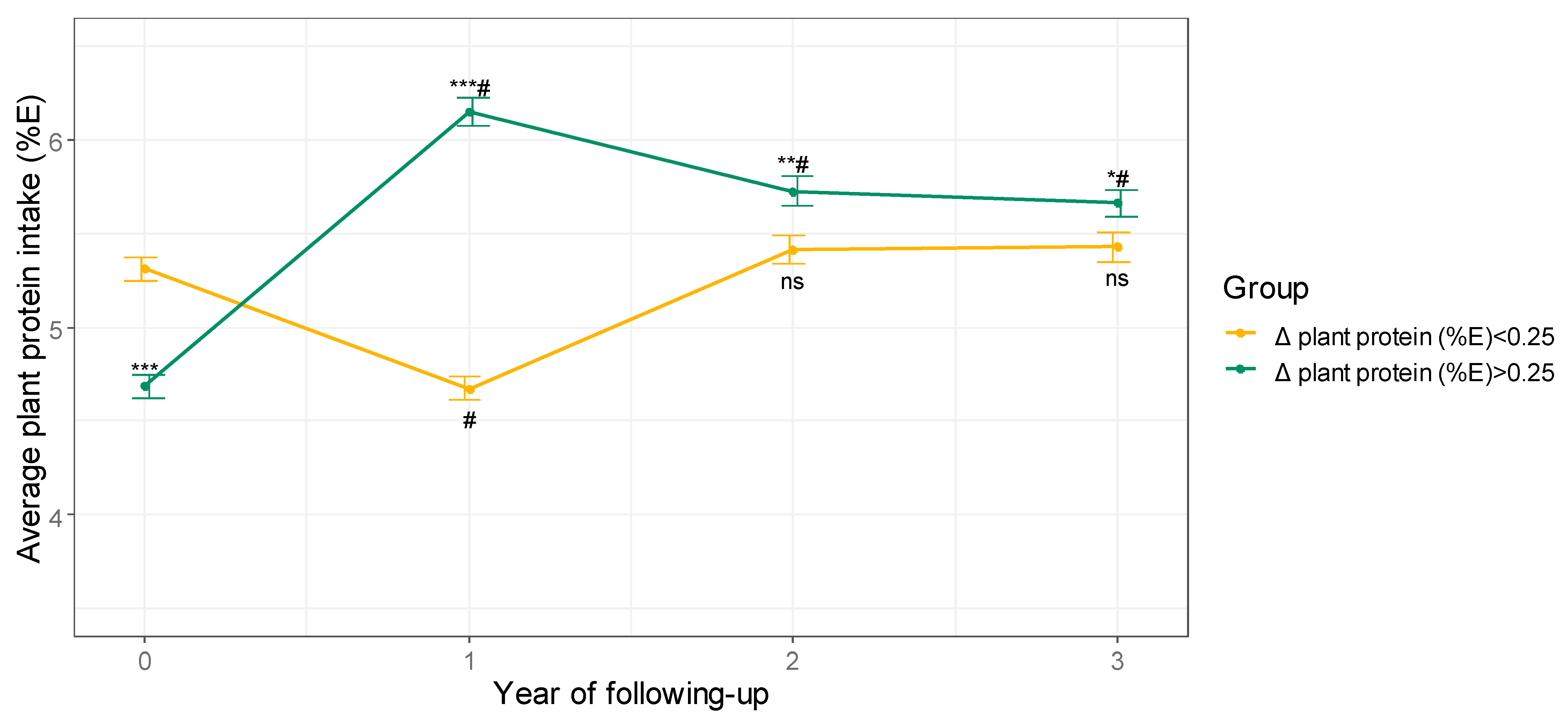
3.2. Plant Protein Intake after Dietary Intervention
3.3. Changes in Energy, Nutrients, and Food Intake
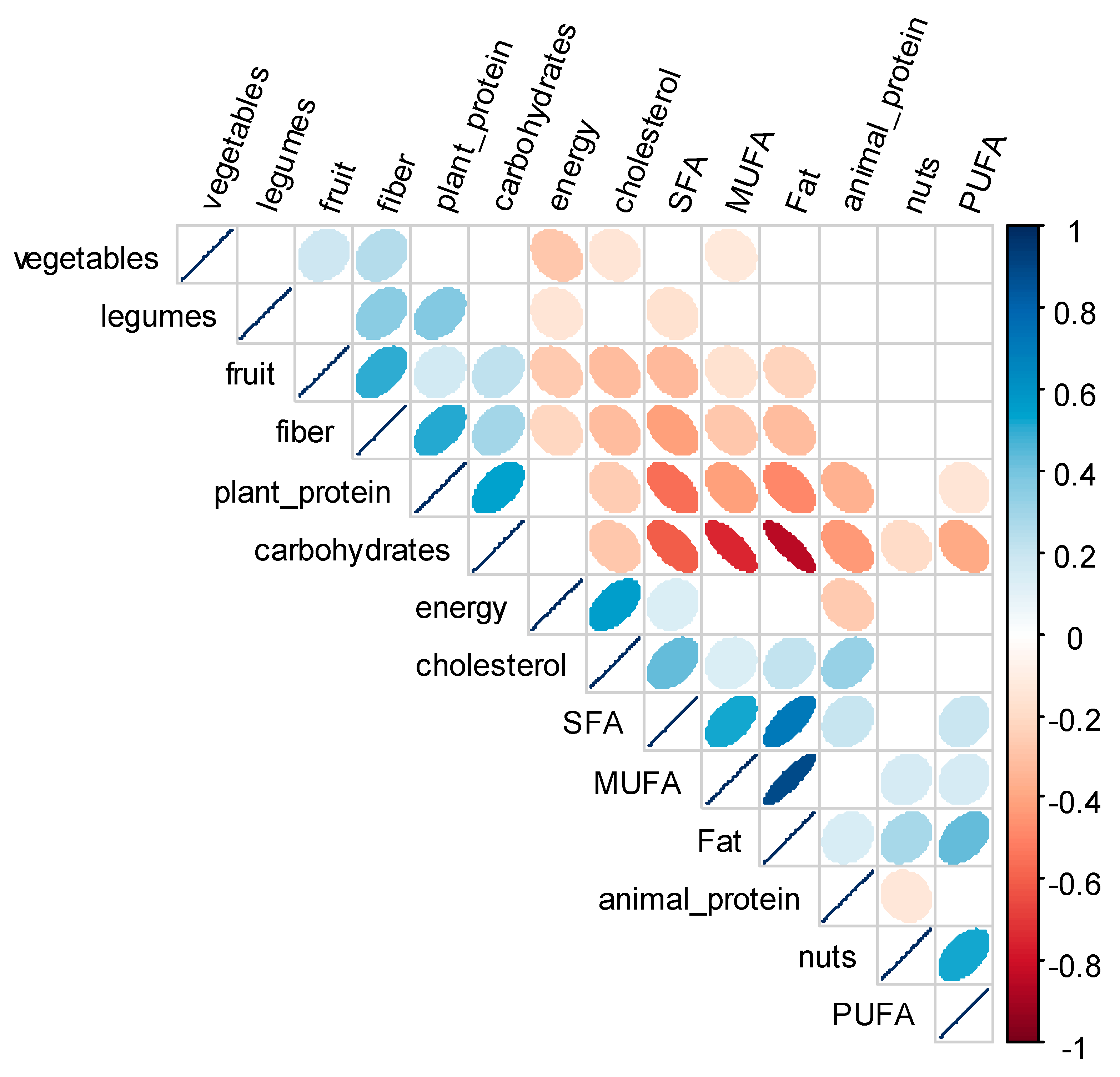
3.4. Correlations between Changes in Energy, Nutrients, and Food Intake
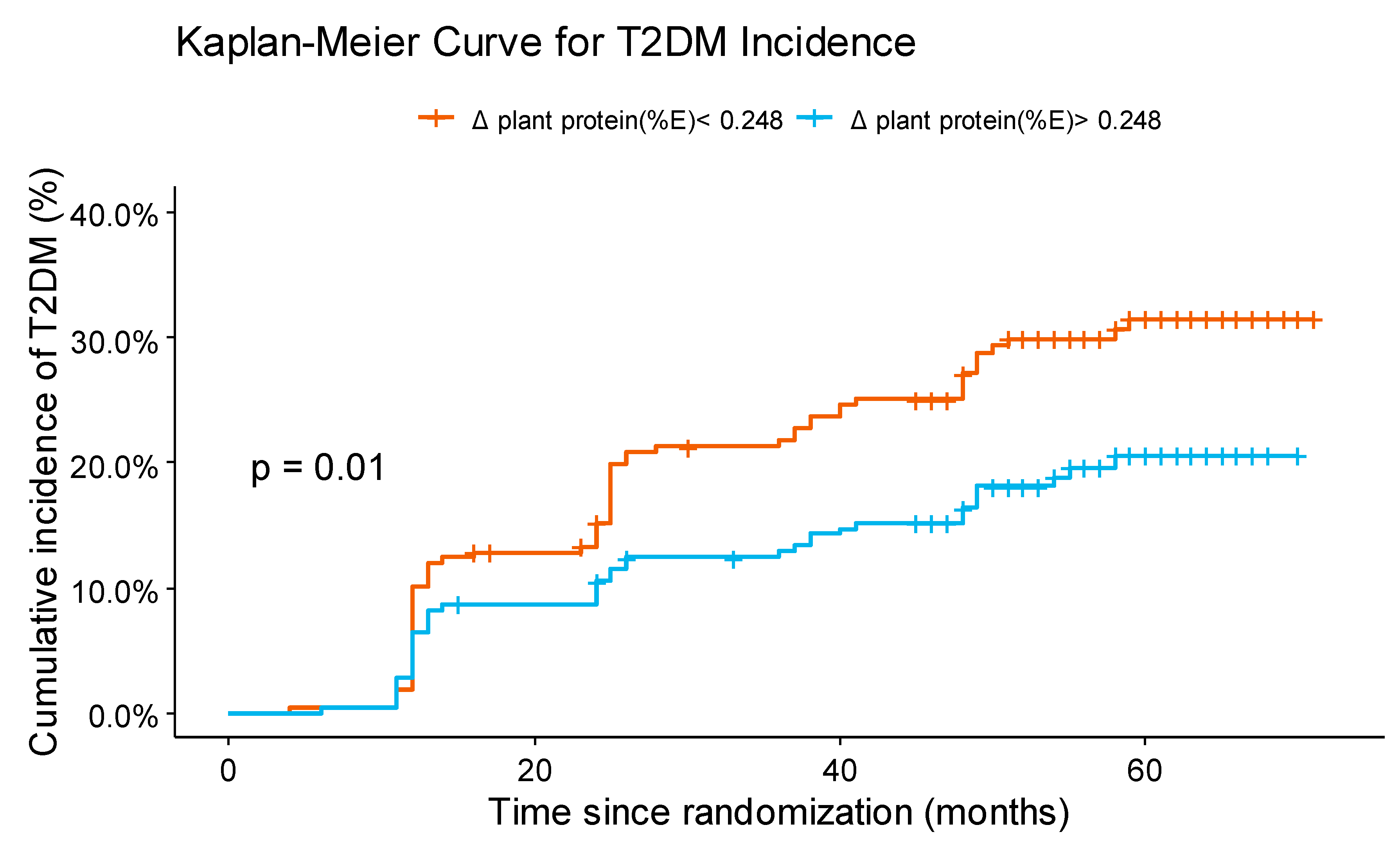
3.5. Change in Plant Protein Intake and T2DM Incidence
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Olesen, K.K.W.; Madsen, M.; Egholm, G.; Thim, T.; Jensen, L.O.; Raungaard, B.; Bøtker, H.E.; Sørensen, H.T.; Maeng, M. Patients with Diabetes Without Significant Angiographic Coronary Artery Disease Have the Same Risk of Myocardial Infarction as Patients without Diabetes in a Real-World Population Receiving Appropriate Prophylactic Treatment. Diabetes Care 2017, 40, 1103–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global Aetiology and Epidemiology of Type 2 Diabetes Mellitus and Its Complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Yau, J.W.; Thor, S.M.; Ramadas, A. Nutritional Strategies in Prediabetes: A Scoping Review of Recent Evidence. Nutrients 2020, 12, 2990. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.-G.; Zhang, Q.-L.; Liu, X.-L.; Wu, H.; Zheng, J.-L.; Xiang, Y.-B. Dietary Protein Intake and Risk of Type 2 Diabetes: A Dose-Response Meta-Analysis of Prospective Studies. Eur. J. Nutr. 2019, 58, 1351–1367. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, A.F.H.; Pedersen, E.; Schwab, U.; Risérus, U.; Aas, A.-M.; Uusitupa, M.; Thanopoulou, A.; Kendall, C.; Sievenpiper, J.L.; Kahleová, H.; et al. The Effects of Different Quantities and Qualities of Protein Intake in People with Diabetes Mellitus. Nutrients 2020, 12, 365. [Google Scholar] [CrossRef] [Green Version]
- Malik, V.S.; Li, Y.; Tobias, D.K.; Pan, A.; Hu, F.B. Dietary Protein Intake and Risk of Type 2 Diabetes in US Men and Women. Am. J. Epidemiol. 2016, 183, 715–728. [Google Scholar] [CrossRef]
- Virtanen, H.E.K.; Koskinen, T.T.; Voutilainen, S.; Mursu, J.; Tuomainen, T.-P.; Kokko, P.; Virtanen, J.K. Intake of Different Dietary Proteins and Risk of Type 2 Diabetes in Men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Br. J. Nutr. 2017, 117, 882–893. [Google Scholar] [CrossRef] [Green Version]
- Budhathoki, S.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Goto, A.; Kotemori, A.; Ishihara, J.; Takachi, R.; Charvat, H.; Mizoue, T.; et al. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality in a Japanese Cohort. JAMA Intern. Med. 2019, 179, 1509–1518. [Google Scholar] [CrossRef]
- Delgado-Lista, J.; Perez-Martinez, P.; Garcia-Rios, A.; Alcala-Diaz, J.F.; Perez-Caballero, A.I.; Gomez-Delgado, F.; Fuentes, F.; Quintana-Navarro, G.; Lopez-Segura, F.; Ortiz-Morales, A.M.; et al. Coronary Diet Intervention with Olive Oil and Cardiovascular Prevention Study (The Cordioprev Study): Rationale, Methods, and Baseline Characteristics. Am. Heart J. 2016, 177, 1–25. [Google Scholar] [CrossRef] [Green Version]
- ADA 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [Green Version]
- Willett, W. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998; ISBN 978-0-19-975403-8. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos. Guia de Prácticas, 16th ed.; Ediciones Pirámide (Grupo Anaya, SA): Madrid, Spain, 2013. [Google Scholar]
- Mataix-Verdu, J.; García-Diz, L.; Mañas-Almendros, M.; Martinez de Vitoria, E.; Llopis-Gonzalez, J. Tabla de Composición de Alimentos Españoles, 5th ed.; Universidad de Granada: Granada, Spain, 2009. [Google Scholar]
- Quintana-Navarro, G.M.; Alcala-Diaz, J.F.; Lopez-Moreno, J.; Perez-Corral, I.; Leon-Acuña, A.; Torres-Peña, J.D.; Rangel-Zuñiga, O.A.; Arenas de Larriva, A.P.; Corina, A.; Camargo, A.; et al. Long-Term Dietary Adherence and Changes in Dietary Intake in Coronary Patients after Intervention with a Mediterranean Diet or a Low-Fat Diet: The CORDIOPREV Randomized Trial. Eur. J. Nutr. 2019. [Google Scholar] [CrossRef]
- Matsuda, M.; DeFronzo, R.A. Insulin Sensitivity Indices Obtained from Oral Glucose Tolerance Testing: Comparison with the Euglycemic Insulin Clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Rojo-Martínez, G.; Valdés, S.; Soriguer, F.; Vendrell, J.; Urrutia, I.; Pérez, V.; Ortega, E.; Ocón, P.; Montanya, E.; Menéndez, E.; et al. Incidence of Diabetes Mellitus in Spain as Results of the Nation-Wide Cohort [email protected] Study. Sci. Rep. 2020, 10, 2765. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.M.; Jeong, J.A.; Jung, K.Y.; Hee, K.S.; Songhee, C.; Sang-Ho, J.; Cheol-Young, P.; Sung-Cheol, Y.; Je, L.W. Park Duk-Woo Time- and Dose-Dependent Association of Statin Use with Risk of Clinically Relevant New-Onset Diabetes Mellitus in Primary Prevention: A Nationwide Observational Cohort Study. J. Am. Heart Assoc. 2019, 8, e011320. [Google Scholar] [CrossRef]
- Rietman, A.; Schwarz, J.; Tomé, D.; Kok, F.J.; Mensink, M. High Dietary Protein Intake, Reducing or Eliciting Insulin Resistance? Eur. J. Clin. Nutr. 2014, 68, 973–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Protein and Amino Acid Requirements in Human Nutrition: Report of a Joint FAO/WHO/UNU Expert Consultation, World Health Organisation, Technical Report Series, No. 935—European Environment Agency. 2007. Available online: https://www.eea.europa.eu/data-and-maps/indicators/13.2-development-in-consumption-of-2/who-2007-protein-and-amino (accessed on 30 December 2020).
- Mariotti, F. Animal and Plant Protein Sources and Cardiometabolic Health. Adv. Nutr. 2019, 10, S351–S366. [Google Scholar] [CrossRef]
- van Nielen, M.; Feskens, E.J.M.; Mensink, M.; Sluijs, I.; Molina, E.; Amiano, P.; Ardanaz, E.; Balkau, B.; Beulens, J.W.J.; Boeing, H.; et al. Dietary Protein Intake and Incidence of Type 2 Diabetes in Europe: The EPIC-InterAct Case-Cohort Study. Diabetes Care 2014, 37, 1854–1862. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Sun, C.; Liu, S.; Li, Y. Dietary Protein Intake and Type 2 Diabetes among Women and Men in Northeast China. Sci. Rep. 2016, 6, 37604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, X.; Scott, D.; Hodge, A.M.; English, D.R.; Giles, G.G.; Ebeling, P.R.; Sanders, K.M. Dietary Protein Intake and Risk of Type 2 Diabetes: Results from the Melbourne Collaborative Cohort Study and a Meta-Analysis of Prospective Studies. Am. J. Clin. Nutr. 2016, 104, 1352–1365. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuenschwander, M.; Barbaresko, J.; Pischke, C.R.; Iser, N.; Beckhaus, J.; Schwingshackl, L.; Schlesinger, S. Intake of Dietary Fats and Fatty Acids and the Incidence of Type 2 Diabetes: A Systematic Review and Dose-Response Meta-Analysis of Prospective Observational Studies. PLoS Med. 2020, 17, e1003347. [Google Scholar] [CrossRef]
- Liu, S.; van der Schouw, Y.T.; Soedamah-Muthu, S.S.; Spijkerman, A.M.W.; Sluijs, I. Intake of Dietary Saturated Fatty Acids and Risk of Type 2 Diabetes in the European Prospective Investigation into Cancer and Nutrition-Netherlands Cohort: Associations by Types, Sources of Fatty Acids and Substitution by Macronutrients. Eur. J. Nutr. 2019, 58, 1125–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, F.; Micha, R.; Wu, J.H.Y.; de Oliveira Otto, M.C.; Otite, F.O.; Abioye, A.I.; Mozaffarian, D. Effects of Saturated Fat, Polyunsaturated Fat, Monounsaturated Fat, and Carbohydrate on Glucose-Insulin Homeostasis: A Systematic Review and Meta-Analysis of Randomised Controlled Feeding Trials. PLoS Med. 2016, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zong, G.; Liu, G.; Willett, W.C.; Wanders, A.J.; Alssema, M.; Zock, P.L.; Hu, F.B.; Sun, Q. Associations between Linoleic Acid Intake and Incident Type 2 Diabetes among U.S. Men and Women. Diabetes Care 2019, 42, 1406–1413. [Google Scholar] [CrossRef]
- Olsson, K.; Ramne, S.; González-Padilla, E.; Ericson, U.; Sonestedt, E. Associations of Carbohydrates and Carbohydrate-Rich Foods with Incidence of Type 2 Diabetes. Br. J. Nutr. 2020. [Google Scholar] [CrossRef]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; et al. Dietary Glycemic Index and Load and the Risk of Type 2 Diabetes: Assessment of Causal Relations. Nutrients 2019, 11, 1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, D.S.; Garvin, J.T.; Xu, H. Carbohydrate Quality, Glycemic Index, Glycemic Load and Cardiometabolic Risks in the US, Europe and Asia: A Dose–Response Meta-Analysis. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 853–871. [Google Scholar] [CrossRef]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate Quality and Human Health: A Series of Systematic Reviews and Meta-Analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [Green Version]
- de Koning, L.; Fung, T.T.; Liao, X.; Chiuve, S.E.; Rimm, E.B.; Willett, W.C.; Spiegelman, D.; Hu, F.B. Low-Carbohydrate Diet Scores and Risk of Type 2 Diabetes in Men. Am. J. Clin. Nutr. 2011, 93, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Ahnen, R.T.; Jonnalagadda, S.S.; Slavin, J.L. Role of Plant Protein in Nutrition, Wellness, and Health. Nutr. Rev. 2019, 77, 735–747. [Google Scholar] [CrossRef] [PubMed]
- de Gavelle, E.; Huneau, J.-F.; Mariotti, F. Patterns of Protein Food Intake Are Associated with Nutrient Adequacy in the General French Adult Population. Nutrients 2018, 10, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, X.; Scott, D.; Hodge, A.; English, D.R.; Giles, G.G.; Ebeling, P.R.; Sanders, K.M. Dietary Protein from Different Food Sources, Incident Metabolic Syndrome and Changes in Its Components: An 11-Year Longitudinal Study in Healthy Community-Dwelling Adults. Clin. Nutr. 2017, 36, 1540–1548. [Google Scholar] [CrossRef]
- Vatanparast, H.; Islam, N.; Shafiee, M.; Ramdath, D.D. Increasing Plant-Based Meat Alternatives and Decreasing Red and Processed Meat in the Diet Differentially Affect the Diet Quality and Nutrient Intakes of Canadians. Nutrients 2020, 12, 2034. [Google Scholar] [CrossRef]
- Phillips, S.M.; Fulgoni, V.L.; Heaney, R.P.; Nicklas, T.A.; Slavin, J.L.; Weaver, C.M. Commonly Consumed Protein Foods Contribute to Nutrient Intake, Diet Quality, and Nutrient Adequacy. Am. J. Clin. Nutr. 2015, 101, 1346S–1352S. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Merino, J.; Sun, Q.; Fitó, M.; Salas-Salvadó, J. Dietary Polyphenols, Mediterranean Diet, Prediabetes, and Type 2 Diabetes: A Narrative Review of the Evidence. Oxidative Med. Cell. Longev. 2017, 2017, 6723931. [Google Scholar] [CrossRef]
- Russell, W.R.; Baka, A.; Björck, I.; Delzenne, N.; Gao, D.; Griffiths, H.R.; Hadjilucas, E.; Juvonen, K.; Lahtinen, S.; Lansink, M.; et al. Impact of Diet Composition on Blood Glucose Regulation. Crit. Rev. Food Sci. Nutr. 2016, 56, 541–590. [Google Scholar] [CrossRef]
- Qian, F.; Liu, G.; Hu, F.B.; Bhupathiraju, S.N.; Sun, Q. Association between Plant-Based Dietary Patterns and Risk of Type 2 Diabetes: A Systematic Review and Meta-Analysis. JAMA Intern. Med. 2019. [Google Scholar] [CrossRef]
- Comerford, K.B.; Pasin, G. Emerging Evidence for the Importance of Dietary Protein Source on Glucoregulatory Markers and Type 2 Diabetes: Different Effects of Dairy, Meat, Fish, Egg, and Plant Protein Foods. Nutrients 2016, 8, 446. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Alonso, P.; Becerra-Tomás, N.; Papandreou, C.; Bulló, M.; Guasch-Ferré, M.; Toledo, E.; Ruiz-Canela, M.; Clish, C.B.; Corella, D.; Dennis, C.; et al. Plasma Metabolomics Profiles Are Associated with the Amount and Source of Protein Intake: A Metabolomics Approach within the PREDIMED Study. Mol. Nutr. Food Res. 2020, 64, e2000178. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Decreased Plant Protein Intake (<P50 [−3.22,0.248]) | Increased Plant Protein Intake (>P50 (0.248,5.57]) | p Value |
|---|---|---|---|
| n | 218 | 218 | |
| Age (years) | 57.4 (0.6) | 58.1 (0.6) | 0.4315 |
| Men/women (n) | 182/36 | 187/31 | 0.5953 |
| Waist circumference (cm) | 103.1 (0.7) | 101.8 (0.7) | 0.1961 |
| BMI (kg/m2) | 30.6 (0.3) | 30.1 (0.3) | 0.2491 |
| TG (mg/dL) | 121.6 (4.2) | 122.8 (4) | 0.6761 |
| Total cholesterol (mg/dL) | 164 (2.4) | 159.1 (2) | 0.1673 |
| c-LDL (mg/dL) | 93.28 (1.81) | 90.79 (1.61) | 0.3964 |
| c-HDL (mg/dL) | 45.14 (0.77) | 43.56 (0.66) | 0.1420 |
| Apo A1 (mg/dL) | 136.4 (1.6) | 131.5 (1.4) | 0.0303 |
| Apo B (mg/dL) | 74 (1.3) | 71.1 (1.1) | 0.1306 |
| hs-CRP (mg/L) | 2.4 (0.1) | 2.1 (0.1) | 0.4369 |
| Glucose (mg/dL) | 94.1 (0.7) | 92.5 (0.7) | 0.1002 |
| HbA1c (%) | 5.94 (0.02) | 5.85 (0.02) | 0.0122 |
| Insulin (mU/L) | 9.05 (0.42) | 8.5 (0.42) | 0.3340 |
| HOMA-IR | 2.9 (0.1) | 2.6 (0.1) | 0.0148 |
| Treatment with statins, % | 83.7 | 90.4 | 0.0064 |
| Hypertension, % | 66.5 | 63.8 | 0.6153 |
| Current smoking, % | 8.25 | 6.9 | 0.7173 |
| Prior smoking, % | 67.0 | 70.2 | 0.5359 |
| Diet (Low-fat/Med diet) | 101/117 | 98/120 | 0.8475 |
| Variable | Baseline | 1 Year of Follow-Up | ||
|---|---|---|---|---|
| n= 436 | Decreased Plant Protein Intake (<P50 [−3.22,0.248]) n = 218 | Increased Plant Protein Intake (>P50 (0.248,5.57]) n = 218 | Between-Group Differences Postintervention (p-Value) | |
| Energy, kcal/d | 2292.3 (24.1) | 1942.4 (34.4) *** | 1890.3 (25.3) *** | 0.3523 |
| Fat (%E) | 36.1 (0.2) | 36.9 (0.4) *** | 32.4 (0.5) *** | <0.001 |
| SFA (%E) | 8.7 (0.1) | 8.3 (0.1) | 6.9 (0.1) *** | <0.001 |
| SFA (% total fat) | 26.8 (0.2) | 24.92 (0.29) *** | 23.94 (0.26) *** | 0.0125 |
| MUFA (%E) | 17.7 (0.2) | 18.3 (0.3) *** | 15.8 (0.3) *** | <0.001 |
| MUFA (% total fat) | 54.2 (0.2) | 54.15 (0.49) | 53.65 (0.45) | 0.4511 |
| PUFA (%E) | 6.2 (0.1) | 6.9 (0.2) *** | 6.5 (0.1) | 0.0348 |
| PUFA (% total fat) | 19.0 (0.2) | 20.94 (0.47) ** | 22.42 (0.42) *** | 0.0186 |
| Protein (%E) | 18.2 (0.1) | 18.3 (0.2) | 18.0 (0.2) | 0.3046 |
| Vegetal protein (%E) | 5.0 (0.0) | 4.67 (0.06) *** | 6.15 (0.08) *** | <0.001 |
| Animal protein (%E) | 12.40 (0.1) | 12.87 (0.22) *** | 11.31 (0.17) *** | <0.001 |
| Carbohydrates (%E) | 42.5 (0.3) | 41.2 (0.5) *** | 46.5 (0.5) *** | <0.001 |
| Cholesterol (mg/d) | 327.1 (4.5) | 273.4 (6.1) *** | 234.4 (4.5) *** | <0.001 |
| Fibre, g/100 kcal | 1.1 (0.0) | 1.22 (0.02) ** | 1.48 (0.03) *** | <0.001 |
| Fruit, g/100 kcal | 16.3 (0.5) | 21.63 (0.77) *** | 22.36 (0.61) *** | 0.1664 |
| Vegetables, g/100 kcal | 11.5 (0.2) | 13.33 (0.44) ** | 13.51 (0.38) *** | 0.5681 |
| Legumes, g/100 kcal | 1.0 (0.0) | 1.1 (0.04) | 1.46 (0.06) *** | <0.001 |
| Tree nuts, g/100 kcal | 0.4 (0) | 0.41 (0.04) | 0.46 (0.04) | 0.2962 |
| Increased Plant Protein Intake (>P50 (0.248,5.57]) | Likelihood Ratio Test | |
|---|---|---|
| Unadjusted model | 0.6008 (0.4064–0.8883) | p = 0.0096 |
| Multivariable model 1 | 0.5981 (0.4043–0.8848) | p = 0.0199 |
| Multivariable model 2 | 0.6385 (0.4257–0.9578) | p = 0.0024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Cruz-Ares, S.; Gutiérrez-Mariscal, F.M.; Alcalá-Díaz, J.F.; Quintana-Navarro, G.M.; Podadera-Herreros, A.; Cardelo, M.P.; Torres-Peña, J.D.; Arenas-de Larriva, A.P.; Pérez-Martínez, P.; Delgado-Lista, J.; et al. Quality and Quantity of Protein Intake Influence Incidence of Type 2 Diabetes Mellitus in Coronary Heart Disease Patients: From the CORDIOPREV Study. Nutrients 2021, 13, 1217. https://doi.org/10.3390/nu13041217
de la Cruz-Ares S, Gutiérrez-Mariscal FM, Alcalá-Díaz JF, Quintana-Navarro GM, Podadera-Herreros A, Cardelo MP, Torres-Peña JD, Arenas-de Larriva AP, Pérez-Martínez P, Delgado-Lista J, et al. Quality and Quantity of Protein Intake Influence Incidence of Type 2 Diabetes Mellitus in Coronary Heart Disease Patients: From the CORDIOPREV Study. Nutrients. 2021; 13(4):1217. https://doi.org/10.3390/nu13041217
Chicago/Turabian Stylede la Cruz-Ares, Silvia, Francisco M. Gutiérrez-Mariscal, Juan F. Alcalá-Díaz, Gracia M. Quintana-Navarro, Alicia Podadera-Herreros, Magdalena P. Cardelo, José D. Torres-Peña, Antonio P. Arenas-de Larriva, Pablo Pérez-Martínez, Javier Delgado-Lista, and et al. 2021. "Quality and Quantity of Protein Intake Influence Incidence of Type 2 Diabetes Mellitus in Coronary Heart Disease Patients: From the CORDIOPREV Study" Nutrients 13, no. 4: 1217. https://doi.org/10.3390/nu13041217