
Reduction in Maternal Energy Intake during Lactation Decreased Maternal Body Weight and Concentrations of Leptin, Insulin and Adiponectin in Human Milk without Affecting Milk Production, Milk Macronutrient Composition or Infant Growth

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
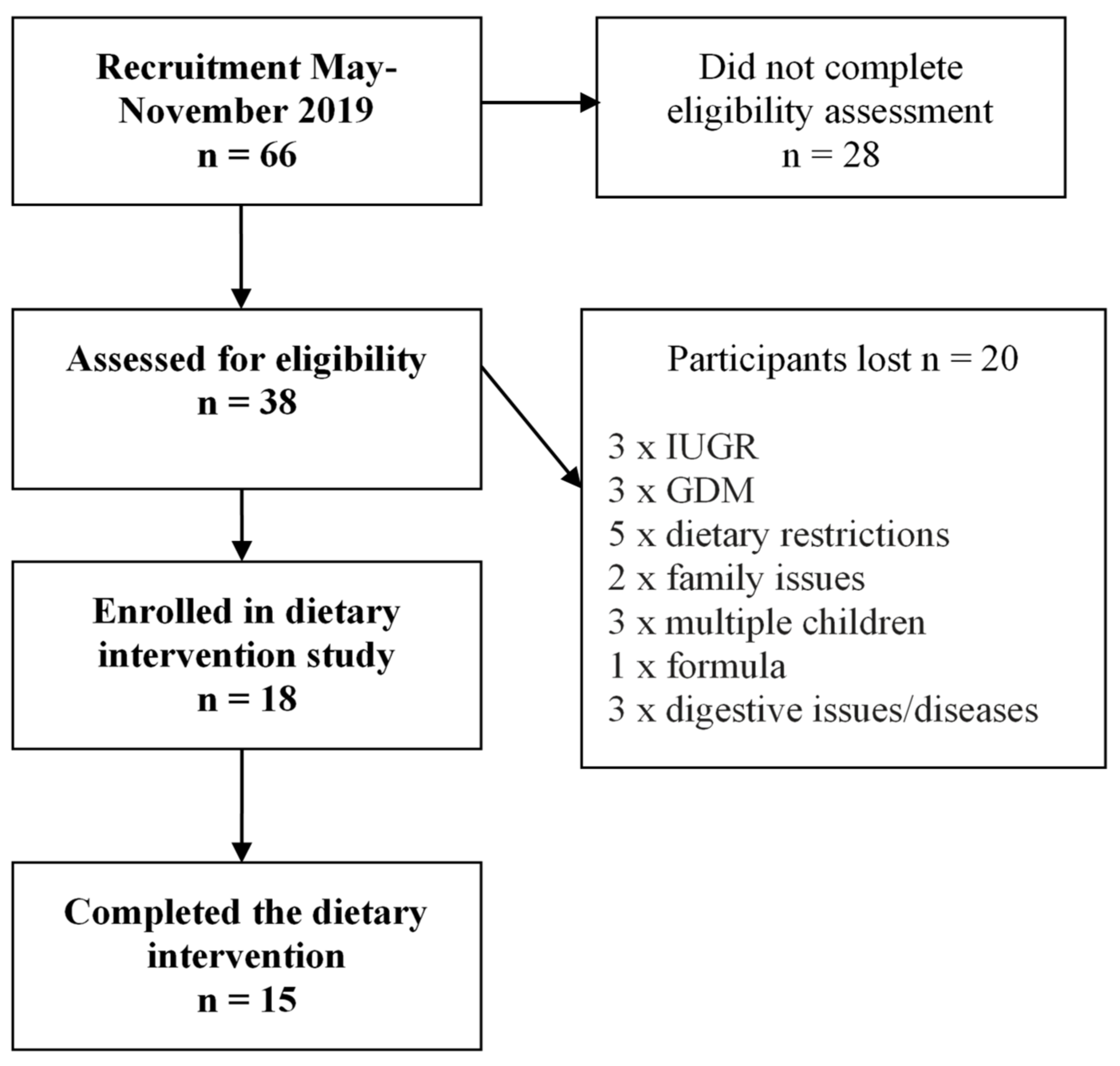
2.2. Study Participants
2.3. Dietary Assessment
2.4. Dietary Intervention
2.5. Anthropometry Measurements
2.6. Body Composition Measurements
2.7. Human Milk Sample Collection
2.8. 24 h Milk Production and Milk Intake
2.9. Calculated Intake of Human Milk Macronutrients
2.10. Sample Preparation
2.11. Macronutrient Measurements
2.12. Metabolic Hormone Measurements
2.13. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Dietary Intake before and during Dietary Intervention
3.3. Effect of the Dietary Intervention on HM Macronutrient and Metabolic Hormone Composition
3.4. Effect of the Dietary Intervention on HM Production and Intake of Macronutrients and Metabolic Hormones
3.5. Effect of the Dietary Intervention on Maternal Anthropometrics and Infant Growth
3.6. Associations between HM Composition and Production at Baseline, Maternal Body Composition and Infant Growth and Changes in HM Metabolic Hormones and Dietary Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Breastfeeding. Available online: https://www.who.int/nutrition/topics/exclusive_breastfeeding/en/ (accessed on 15 January 2020).
- Fields, D.A.; George, B.; Williams, M.; Whitaker, K.; Allison, D.B.; Teague, A.; Demerath, E.W. Associations between human breast milk hormones and adipocytokines and infant growth and body composition in the first 6 months of life. Pediatr. Obes. 2017, 12, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Grote, V.; Verduci, E.; Scaglioni, S.; Vecchi, F.; Contarini, G.; Giovannini, M.; Koletzko, B.; Agostoni, C. Breast milk composition and infant nutrient intakes during the first 12 months of life. Eur. J. Clin. Nutr. 2016, 70, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dritsakou, K.; Liosis, G.; Valsami, G.; Polychronopoulos, E.; Skouroliakou, M. The impact of maternal-and neonatal-associated factors on human milk’s macronutrients and energy. J. Matern. Fetal Neonatal Med. 2017, 30, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Grunewald, M.; Hellmuth, C.; Kirchberg, F.F.; Mearin, M.L.; Auricchio, R.; Castillejo, G.; Korponay-Szabo, I.R.; Polanco, I.; Roca, M.; Vriezinga, S.L. Variation and Interdependencies of Human Milk Macronutrients, Fatty Acids, Adiponectin, Insulin, and IGF-II in the European PreventCD Cohort. Nutrients 2019, 11, 2034. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.; Rong, S.S.; Sun, X.; Ding, G.; Wan, W.; Zou, L.; Wu, S.; Li, M.; Wang, D. Associations of breast milk adiponectin, leptin, insulin and ghrelin with maternal characteristics and early infant growth: A longitudinal study. Br. J. Nutr. 2018, 120, 1380–1387. [Google Scholar] [CrossRef] [Green Version]
- Bravi, F.; Wiens, F.; Decarli, A.; Dal Pont, A.; Agostoni, C.; Ferraroni, M. Impact of maternal nutrition on breast-milk composition: A systematic review. Am. J. Clin. Nutr. 2016, 104, 646–662. [Google Scholar] [CrossRef] [Green Version]
- Mohammad, M.A.; Sunehag, A.L.; Haymond, M.W. Effect of dietary macronutrient composition under moderate hypocaloric intake on maternal adaptation during lactation. Am. J. Clin. Nutr. 2009, 89, 1821–1827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prentice, P.; Ong, K.K.; Schoemaker, M.H.; van Tol, E.A.; Vervoort, J.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Breast milk nutrient content and infancy growth. Acta Paediatr. 2016, 105, 641–647. [Google Scholar] [CrossRef] [Green Version]
- Huseinovic, E.; Winkvist, A.; Bertz, F.; Hellebö Johansson, E.; Brekke, H. Dietary assessment among women with overweight and obesity in early postpartum. J. Hum. Nutr. Diet. 2016, 29, 411–417. [Google Scholar] [CrossRef]
- Blumfield, M.L.; Hure, A.J.; MacDonald-Wicks, L.K.; Patterson, A.J.; Smith, R.; Collins, C.E. Disparities exist between National food group recommendations and the dietary intakes of women. BMC Women’s Health 2011, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Vithayathil, M.; Gugusheff, J.; Gibson, R.; Ong, Z.; Muhlhausler, B. Effect of a maternal cafeteria diet on the fatty acid composition of milk and offspring red blood cells. Prostaglandins Leukot. Essent. Fat. Acids 2016, 109, 58–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolls, B.; Gurr, M.; Van Duijvenvoorde, P.; Rolls, B.J.; Rowe, E. Lactation in lean and obese rats: Effect of cafeteria feeding and of dietary obesity on milk composition. Physiol. Behav. 1986, 38, 185–190. [Google Scholar] [CrossRef]
- Castro, H.; Pomar, C.A.; Palou, A.; Picó, C.; Sánchez, J. Offspring predisposition to obesity due to maternal-diet-induced obesity in rats is preventable by dietary normalization before mating. Mol. Nutr. Food Res. 2017, 61, 1600513. [Google Scholar] [CrossRef] [PubMed]
- Leghi, G.E.; Lai, C.T.; Narayanan, A.; Netting, M.J.; Dymock, M.; Rea, A.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. Daily variation of macronutrient concentrations in mature human milk over 3 weeks. Sci. Rep. 2021, 11, 10224. [Google Scholar] [CrossRef]
- Food Standards Australia New Zealand. Sugar. 2019. Available online: https://www.foodstandards.gov.au/consumer/nutrition/Pages/Sugar.aspx (accessed on 10 May 2021).
- Onis, M.; Onyango Adelheid, W.; Martorell, R. WHO Child Growth Standards. Acta Paediatr. Int. J. Paediatr. 2006, 95, 5–101. [Google Scholar]
- Schlaff, R.A.; Baruth, M.; Deere, S.J.; Boggs, A.; Odabasic, A. Associations between prenatal diet quality and gestational weight gain. Nutr. Health 2020, 26, 13–18. [Google Scholar] [CrossRef]
- Widaman, A.M.; Keim, N.L.; Burnett, D.J.; Miller, B.; Witbracht, M.G.; Widaman, K.F.; Laugero, K.D. A potential tool for clinicians; evaluating a computer-led dietary assessment method in overweight and obese women during weight loss. Nutrients 2017, 9, 218. [Google Scholar] [CrossRef] [Green Version]
- Gridneva, Z.; Rea, A.; Hepworth, A.R.; Ward, L.C.; Lai, C.T.; Hartmann, P.E.; Geddes, D.T. Relationships between breastfeeding patterns and maternal and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Anthro for Personal Computers, Version 3.2.2, 2011: Software for Assessing Growth and Development of the World’s Children. 2010. Available online: http://www.who.int/childgrowth/software/en/ (accessed on 21 May 2020).
- Arthur, P.; Hartmann, P.; Smith, M. Measurement of the milk intake of breast-fed infants. J. Pediatr. Gastroenterol. Nutr. 1987, 6, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.C.; Mitoulas, L.R.; Cregan, M.D.; Ramsay, D.T.; Doherty, D.A.; Hartmann, P.E. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics 2006, 117, 387–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butte, N.; Wong, W.; Patterson, B.W.; Garza, C.; Klein, P. Human-milk intake measured by administration of deuterium oxide to the mother: A comparison with the test-weighing technique. Am. J. Clin. Nutr. 1988, 47, 815–821. [Google Scholar] [CrossRef] [PubMed]
- George, A.D.; Gay, M.C.; Murray, K.; Muhlhausler, B.S.; Wlodek, M.E.; Geddes, D.T. Human milk sampling protocols affect estimation of infant lipid intake. J. Nutr. 2020, 150, 2924–2930. [Google Scholar] [CrossRef]
- Lucas, A.; Gibbs, J.; Lyster, R.; Baum, J. Creamatocrit: Simple clinical technique for estimating fat concentration and energy value of human milk. Br. Med. J. 1978, 1, 1018–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier, P.P.; Engstrom, J.L.; Zuleger, J.L.; Motykowski, J.E.; Vasan, U.; Meier, W.A.; Hartmann, P.E.; Williams, T.M. Accuracy of a user-friendly centrifuge for measuring creamatocrits on mothers’ milk in the clinical setting. Breastfeed. Med. 2006, 1, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Mitoulas, L.R.; Kent, J.C.; Cox, D.B.; Owens, R.A.; Sherriff, J.L.; Hartmann, P.E. Variation in fat, lactose and protein in human milk over 24 h and throughout the first year of lactation. Br. J. Nutr. 2002, 88, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Arthur, P.G.; Smith, M.; Hartmann, P.E. Milk lactose, citrate, and glucose as markers of lactogenesis in normal and diabetic women. J. Pediatr. Gastroenterol. Nutr. 1989, 9, 488–496. [Google Scholar] [CrossRef]
- The R Foundation. A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 21 June 2020).
- Yahvah, K.M.; Brooker, S.L.; Williams, J.E.; Settles, M.; McGuire, M.A.; McGuire, M.K. Elevated dairy fat intake in lactating women alters milk lipid and fatty acids without detectible changes in expression of genes related to lipid uptake or synthesis. Nutr. Res. 2015, 35, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B. Human Milk Lipids. Ann. Nutr. Metab. 2016, 69 (Suppl. S2), 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauman, D.E.; Currie, W.B. Partitioning of nutrients during pregnancy and lactation: A review of mechanisms involving homeostasis and homeorhesis. J. Dairy Sci. 1980, 63, 1514–1529. [Google Scholar] [CrossRef]
- Rakicioglu, N.; Samur, G.; Topcu, A.; Topcu, A.A. The effect of Ramadan on maternal nutrition and composition of breast milk. Pediatr. Int. 2006, 48, 278–283. [Google Scholar] [CrossRef]
- Bener, A.; Galadari, S.; Gillett, M.; Osman, N.; Al-Taneiji, H.; Al-Kuwaiti, M.; Al-Sabosy, M. Fasting during the holy month of Ramadan does not change the composition of breast milk. Nutr. Res. 2001, 21, 859–864. [Google Scholar] [CrossRef]
- Khin-Maung-Naing; Tin-Tin-O; Kywe-Thein, M.S.; Nwe-New-Hlaing. Study on lactation performance of Burmese mothers. Am. J. Clin. Nutr. 1980, 33, 2665–2668. [Google Scholar] [CrossRef] [Green Version]
- Bautista, C.; Montaño, S.; Ramirez, V.; Morales, A.; Nathanielsz, P.; Bobadilla, N.; Zambrano, E. Changes in milk composition in obese rats consuming a high-fat diet. Br. J. Nutr. 2016, 115, 538–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hue-Beauvais, C.; Miranda, G.; Aujean, E.; Jaffrezic, F.; Devinoy, E.; Martin, P.; Charlier, M. Diet-induced modifications to milk composition have long-term effects on offspring growth in rabbits. J. Anim. Sci. 2017, 95, 761–770. [Google Scholar] [CrossRef]
- Purcell, R.H.; Sun, B.; Pass, L.L.; Power, M.L.; Moran, T.H.; Tamashiro, K.L. Maternal stress and high-fat diet effect on maternal behavior, milk composition, and pup ingestive behavior. Physiol. Behav. 2011, 104, 474–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luoto, R.; Laitinen, K.; Nermes, M.; Isolauri, E. Impact of maternal probiotic-supplemented dietary counseling during pregnancy on colostrum adiponectin concentration: A prospective, randomized, placebo-controlled study. Early Hum. Dev. 2012, 88, 339–344. [Google Scholar] [CrossRef]
- Smith-Kirwin, S.M.; O′Connor, D.M.; De Johnston, J.; Lancey, E.D.; Hassink, S.G.; Funanage, V.L. Leptin expression in human mammary epithelial cells and breast milk. J. Clin. Endocrinol. Metab. 1998, 83, 1810–1813. [Google Scholar] [CrossRef]
- Van Harmelen, V.; Reynisdottir, S.; Eriksson, P.; Thörne, A.; Hoffstedt, J.; Lönnqvist, F.; Arner, P. Leptin secretion from subcutaneous and visceral adipose tissue in women. Diabetes 1998, 47, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Newburg, D.S.; Woo, J.G.; Morrow, A.L. Characteristics and potential functions of human milk adiponectin. J. Pediatr. 2010, 156, S41–S46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- Juanola-Falgarona, M.; Salas-Salvadó, J.; Ibarrola-Jurado, N.; Rabassa-Soler, A.; Díaz-López, A.; Guasch-Ferré, M.; Hernández-Alonso, P.; Balanza, R.; Bulló, M. Effect of the glycemic index of the diet on weight loss, modulation of satiety, inflammation, and other metabolic risk factors: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Ley, S.H.; Hanley, A.J.; Sermer, M.; Zinman, B.; O′Connor, D.L. Associations of prenatal metabolic abnormalities with insulin and adiponectin concentrations in human milk. Am. J. Clin. Nutr. 2012, 95, 867–874. [Google Scholar] [CrossRef] [Green Version]
- Savino, F.; Lupica, M.; Benetti, S.; Petrucci, E.; Liguori, S.A.; Cordero di Montezemolo, L. Adiponectin in breast milk: Relation to serum adiponectin concentration in lactating mothers and their infants. Acta Paediatr. 2012, 101, 1058–1062. [Google Scholar] [CrossRef]
- Young, B.; Patinkin, Z.; Palmer, C.; de la Houssaye, B.; Barbour, L.; Hernandez, T.; Friedman, J.; Krebs, N. Human milk insulin is related to maternal plasma insulin and BMI: But other components of human milk do not differ by BMI. Eur. J. Clin. Nutr. 2017, 112, 548–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savino, F.; Sardo, A.; Rossi, L.; Benetti, S.; Savino, A.; Silvestro, L. Mother and infant body mass index, breast milk leptin and their serum leptin values. Nutrients 2016, 8, 383. [Google Scholar] [CrossRef] [PubMed]
- Kugananthan, S.; Gridneva, Z.; Lai, C.T.; Hepworth, A.R.; Mark, P.J.; Kakulas, F.; Geddes, D.T. Associations between maternal body composition and Appetite Hormones and Macronutrients in Human Milk. Nutrients 2017, 9, 252. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.; Goruk, S.; Becker, A.; Subbarao, P.; Mandhane, P.; Turvey, S.; Lefebvre, D.; Sears, M.; Field, C.; Azad, M. Adiponectin, leptin and insulin in breast milk: Associations with maternal characteristics and infant body composition in the first year of life. Int. J. Obes. 2018, 42, 36–43. [Google Scholar] [CrossRef]
- Mazzocchi, A.; Giannì, M.L.; Morniroli, D.; Leone, L.; Roggero, P.; Agostoni, C.; de Cosmi, V.; Mosca, F. Hormones in Breast Milk and Effect on Infants’ Growth: A Systematic Review. Nutrients 2019, 11, 1845. [Google Scholar] [CrossRef] [Green Version]
- Neville, C.E.; McKinley, M.C.; Holmes, V.A.; Spence, D.; Woodside, J.V. The effectiveness of weight management interventions in breastfeeding women—A systematic review and critical evaluation. Birth 2014, 41, 223–236. [Google Scholar] [CrossRef]
- Antonakou, A.; Papoutsis, D.; Panou, I.; Chiou, A.; Matalas, A. Role of exclusive breastfeeding in energy balance and weight loss during the first six months postpartum. Clin. Exp. Obstet. Gynecol. 2013, 40, 485–488. [Google Scholar] [PubMed]
- Peila, C.; Gazzolo, D.; Bertino, E.; Cresi, F.; Coscia, A. Influence of Diabetes during Pregnancy on Human Milk Composition. Nutrients 2020, 12, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bachour, P.; Yafawi, R.; Jaber, F.; Choueiri, E.; Abdel-Razzak, Z. Effects of smoking, mother’s age, body mass index, and parity number on lipid, protein, and secretory immunoglobulin A concentrations of human milk. Breastfeed. Med. 2012, 7, 179–188. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample Type | Frequency of Collection | Time of Collection | Procedure | Total N |
|---|---|---|---|---|
| Daily | Once a day (1 sample per breast) | Morning before the first morning feed | Prefeed samples from both breasts | 42 (21 samples per breast) |
| Intensive sampling | Once a week (2 samples per breast) | One in the afternoon and one in the evening in addition to daily sample | Prefeed samples from both breasts | 12 (6 samples per breast) |
| Characteristics | Mean ± SD | Range |
|---|---|---|
| Mothers | ||
| Age (years) | 32 ± 3 | 27–37 |
| Pre-pregnancy weight 2 (kg) | 69.4 ± 10.8 | 55–89 |
| Pre-pregnancy BMI 2 (kg/m2) | 25.1 ± 4.1 | 17.2–32.7 |
| Current weight (kg) | 71.4 ± 10.3 | 54.4–80.7 |
| Current BMI (kg/m2) | 25.8 ± 4.1 | 17.1–33.0 |
| Infants | ||
| Age (months) | 3.1 ± 0.8 | 1.6–4.9 |
| Sex 2 (M/F) | 8/6 | - |
| Birth weight 2 (kg) | 3.6 ± 0.4 | 2.9–4.3 |
| Birth length 2 (cm) | 51.1 ± 1.7 | 48–53 |
| Current weight (kg) | 6.1 ± 1.0 | 4.6–7.6 |
| Current length (cm) | 60.3 ± 3.3 | 55.2–65.5 |
| Week 1 Baseline 2 | Week 2 Intervention | Week 3 Intervention | Intervention Phase Combined | |
|---|---|---|---|---|
| Energy (kcal) | 2525 ± 579 | 1716 ± 84 * | 1678 ± 134 * | 1697 ± 104 * |
| Protein (%en) | 17 ± 3 | 22 ± 1 * | 22 ± 1 * | 22 ± 1 * |
| Protein (g) | 105 ± 24 | 93 ± 8 * | 91 ± 8 * | 92 ± 7 * |
| Carbohydrate (%en) | 40 ± 5 | 47 ± 2 * | 47 ± 2 * | 47 ± 2 * |
| Carbohydrate (g) | 254 ± 62 | 202 ± 12 * | 196 ± 15 * | 199 ± 12 * |
| Fibre (g) | 29 ± 7 | 34 ± 3 * | 32 ± 3 | 33 ± 3 * |
| Total sugars (g) | 116 ± 45 | 83 ± 5 * | 80 ± 8 * | 82 ± 5 * |
| Fat (%en) | 40 ± 6 | 27 ± 2 * | 28 ± 2 * | 28 ± 2 * |
| Fat (g) | 114 ± 38 | 52 ± 5 * | 52 ± 7 * | 52 ± 6 * |
| Saturated fat (%en) | 14 ± 9 | 9 ± 1 * | 9 ± 1 * | 9 ± 1 * |
| Saturated fat (g) | 46 ± 17 | 17 ± 2 * | 17 ± 3 * | 17 ± 2 * |
| Macronutrient and Metabolic Hormones | Baseline Period | Intervention Phase | p Value | |
|---|---|---|---|---|
| Week 1 | Week 2 | Week 3 | ||
| Fat (g/L) | 34 ± 13 | 34 ± 16 | 35 ± 14 | 0.63 |
| Protein (g/L) | 8 ± 3 | 8 ± 2 | 8 ± 3 | 0.30 |
| Lactose (g/L) | 65 ± 22 | 61 ± 20 | 63 ± 23 | 0.75 |
| Leptin (ng/mL) | 0.25 ± 0.17 | 0.23 ± 0.18 | 0.20 ± 0.17 * | <0.0001 |
| Insulin (µIU/mL) | 28.70 ± 20.79 | 18.91 ± 12.28 * | 21.49 ± 13.88 * | <0.0001 |
| Adiponectin (ng/mL) | 12.63 ± 6.44 | 11.80 ± 5.24 | 11.35 ± 5.56 * | 0.048 |
| Anthropometry and Body Composition | Baseline Period | Intervention Phase | PE ± SE 1 | p | |
|---|---|---|---|---|---|
| Week 1 | Week 2 2 | Week 3 | |||
| Mothers | |||||
| Weight (kg) | 71.4 ± 10.3 | 70.6 ± 10.3 | 70.1 ± 9.8 * | −1.39 ± 0.35 | 0.002 |
| BMI (kg/m2) | 25.8 ± 4.1 | 25.6 ± 4.1 | 24.3 ± 4.0 * | −0.50 ± 0.13 | 0.002 |
| Fat-free mass (kg) | 44.2 ± 4.7 | 45.2 ± 4.6 | 44.5 ± 4.0 | 0.32 ± 0.58 | 0.60 |
| Fat mass (kg) | 27.2 ± 7.1 | 25.4 ± 6.7 | 25.5 ± 6.5 * | −1.70 ± 0.54 | 0.007 |
| Fat mass (%) | 37.6 ± 5.4 | 35.5 ± 5.0 | 35.9 ± 4.9 | - | - |
| Fat mass to fat-free mass ratio | 0.61 ± 0.1 | 0.56 ± 0.1 | 0.57 ± 0.1 * | −0.05 ± 0.02 | 0.031 |
| Infants | |||||
| Weight (kg) | 6.1 ± 1.0 | 6.3 ± 1.0 * | 6.5 ± 1.0 * | 0.43 ± 0.05 | <0.001 |
| Length (cm) | 60.3 ± 3.3 | 61.1 ± 3.0 * | 61.9 ± 3.1 * | 1.53 ± 0.15 | <0.001 |
| Head circumference (cm) | 40.4 ± 2.0 | 40.8 ± 1.7 * | 41.4 ± 1.6 * | 0.99 ± 0.14 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leghi, G.E.; Netting, M.J.; Lai, C.T.; Narayanan, A.; Dymock, M.; Rea, A.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. Reduction in Maternal Energy Intake during Lactation Decreased Maternal Body Weight and Concentrations of Leptin, Insulin and Adiponectin in Human Milk without Affecting Milk Production, Milk Macronutrient Composition or Infant Growth. Nutrients 2021, 13, 1892. https://doi.org/10.3390/nu13061892
Leghi GE, Netting MJ, Lai CT, Narayanan A, Dymock M, Rea A, Wlodek ME, Geddes DT, Muhlhausler BS. Reduction in Maternal Energy Intake during Lactation Decreased Maternal Body Weight and Concentrations of Leptin, Insulin and Adiponectin in Human Milk without Affecting Milk Production, Milk Macronutrient Composition or Infant Growth. Nutrients. 2021; 13(6):1892. https://doi.org/10.3390/nu13061892
Chicago/Turabian StyleLeghi, Gabriela E., Merryn J. Netting, Ching T. Lai, Ardra Narayanan, Michael Dymock, Alethea Rea, Mary E. Wlodek, Donna T. Geddes, and Beverly S. Muhlhausler. 2021. "Reduction in Maternal Energy Intake during Lactation Decreased Maternal Body Weight and Concentrations of Leptin, Insulin and Adiponectin in Human Milk without Affecting Milk Production, Milk Macronutrient Composition or Infant Growth" Nutrients 13, no. 6: 1892. https://doi.org/10.3390/nu13061892