
Comparison of the GLIM, ESPEN and ICD-10 Criteria to Diagnose Malnutrition and Predict 30-Day Outcomes: An Observational Study in an Oncology Population


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
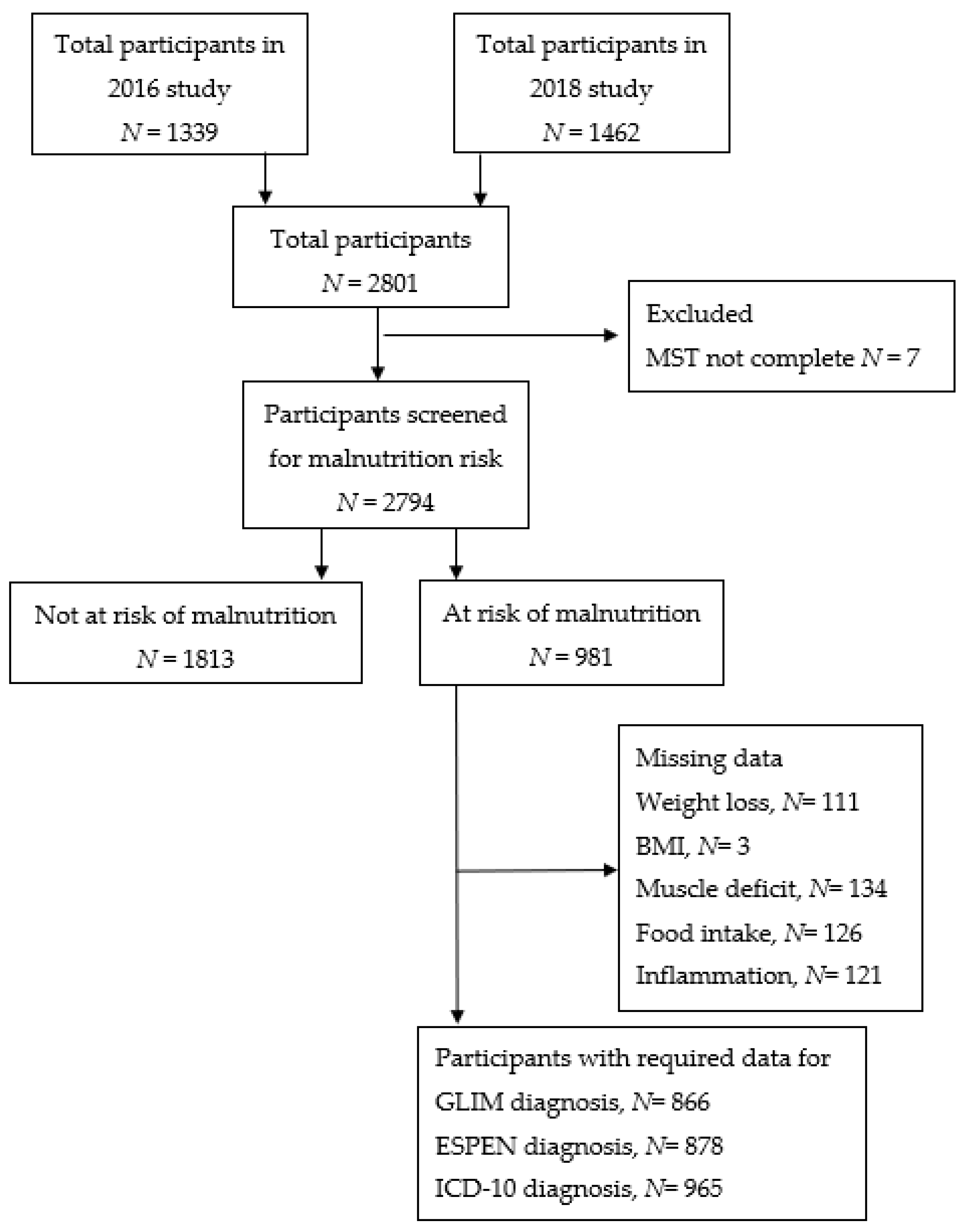
2.2. Participants and Eligibility
2.3. Demographic and Clinical Data
2.4. Malnutrition Screening
2.5. Anthropometry
2.6. Food Intake
2.7. Nutrition Assessment
2.8. Malnutrition Diagnosis
2.9. Statistical Analysis
3. Results
3.1. Malnutrition Prevalence by GLIM, ESPEN and ICD-10
3.2. Agreement between Malnutrition Criteria
3.3. Prediction of 30-Day Mortality
3.4. Prediction of 30-Day Unplanned Admission or Readmission
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agarwal, E.; Ferguson, M.; Banks, M.; Bauer, J.; Capra, S.; Isenring, E. Nutritional status and dietary intake of acute care patients: Results from the Nutrition Care Day Survey 2010. Clin. Nutr. 2012, 31, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segura, A.; Pardo, J.; Jara, C.; Zugazabeitia, L.; Carulla, J.; de las Peñas, R.; García-Cabrera, E.; Azuara, M.L.; Casadó, J.; Gómez-Candela, C. An epidemiological evaluation of the prevalence of malnutrition in Spanish patients with locally advanced or metastatic cancer. Clin. Nutr. 2005, 24, 801–814. [Google Scholar] [CrossRef]
- Marshall, K.M.; Loeliger, J.; Nolte, L.; Kelaart, A.; Kiss, N.K. Prevalence of malnutrition and impact on clinical outcomes in cancer services: A comparison of two time points. Clin. Nutr. 2019, 38, 644–651. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Lucia, S.; Farcomeni, A.; Lorusso, V.; Saracino, V.; Barone, C.; Plastino, F.; Gori, S.; Magarotto, R.; Carteni, G.; et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017, 8, 79884–79896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pressoir, M.; Desné, S.; Berchery, D.; Rossignol, G.; Poiree, B.; Meslier, M.; Traversier, S.; Vittot, M.; Simon, M.; Gekiere, J.P.; et al. Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br. J. Cancer 2010, 102, 966–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuda, Y.; Yamamoto, K.; Hirao, M.; Nishikawa, K.; Maeda, S.; Haraguchi, N.; Miyake, M.; Hama, N.; Miyamoto, A.; Ikeda, M.; et al. Prevalence of Malnutrition Among Gastric Cancer Patients Undergoing Gastrectomy and Optimal Preoperative Nutritional Support for Preventing Surgical Site Infections. Ann. Surg. Oncol. 2015, 22, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Fujiya, K.; Kawamura, T.; Omae, K.; Makuuchi, R.; Irino, T.; Tokunaga, M.; Tanizawa, Y.; Bando, E.; Terashima, M. Impact of Malnutrition After Gastrectomy for Gastric Cancer on Long-Term Survival. Ann. Surg. Oncol. 2018, 25, 974–983. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.F.; Junior, A.A.R.; Campos, F.L.B.; Sousa, R.M.L.; Veloso, H.J.F.; Chein, M.B.C. Scored patient-generated Subjective Global Assessment: Length of hospital stay and mortality in cancer patients. Rev. Nutr. 2017, 30, 545–553. [Google Scholar] [CrossRef] [Green Version]
- Datema, F.R.; Ferrier, M.B.; Baatenburg de Jong, R.J. Impact of severe malnutrition on short-term mortality and overall survival in head and neck cancer. Oral Oncol. 2011, 47, 910–914. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.; Atilla, F.D.; Sahin, F.; Saydam, G. The effect of malnutrition on mortality in hospitalized patients with hematologic malignancy. Supportive Care Cancer 2020, 28, 1441–1448. [Google Scholar] [CrossRef] [PubMed]
- Senesse, P.; Assenat, E.; Schneider, S.; Chargari, C.; Magné, N.; Azria, D.; Hébuterne, X. Nutritional support during oncologic treatment of patients with gastrointestinal cancer: Who could benefit? Cancer Treat. Rev. 2008, 34, 568–575. [Google Scholar] [CrossRef]
- Ross, P.J.; Ashley, S.; Norton, A.; Priest, K.; Waters, J.S.; Eisen, T.; Smith, I.E.; O’Brien, M.E.R. Do patients with weight loss have a worse outcome when undergoing chemotherapy for lung cancers? Br. J. Cancer 2004, 90, 1905–1911. [Google Scholar] [CrossRef] [PubMed]
- Kiss, N.; Loeliger, J.; Findlay, M.; Isenring, E.; Baguley, B.J.; Boltong, A.; Butler, A.; Deftereos, I.; Eisenhuth, M.; Fraser, S.F.; et al. Clinical Oncology Society of Australia: Position statement on cancer-related malnutrition and sarcopenia. Nutr. Diet. 2020, 77, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. International Statistical Classification of Diseases and Related Health Problems 10th Revision. 2019. Available online: https://icd.who.int/browse10/2019/en (accessed on 7 July 2020).
- Keller, H.; de van der Schueren, M.A.; Consortium, G.; Jensen, G.L.; Barazzoni, R.; Compher, C.; Correia, M.I.T.; Gonzalez, M.C.; Jager-Wittenaar, H.; Pirlich, M. Global Leadership Initiative on Malnutrition (GLIM): Guidance on Validation of the Operational Criteria for the Diagnosis of Protein-Energy Malnutrition in Adults. J. Parenter. Enter. Nutr. 2020, 44, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. History of the Development of the ICD. 2018. Available online: https://www.who.int/classifications/icd/en/HistoryOfICD.pdf (accessed on 7 July 2020).
- Contreras-Bolívar, V.; Sánchez-Torralvo, F.J.; Ruiz-Vico, M.; González-Almendros, I.; Barrios, M.; Padín, S.; Alba, E.; Olveira, G. GLIM Criteria Using Hand Grip Strength Adequately Predict Six-Month Mortality in Cancer Inpatients. Nutrients 2019, 11, 2043. [Google Scholar] [CrossRef] [Green Version]
- Yin, L.; Lin, X.; Li, N.; Zhang, M.; He, X.; Liu, J.; Kang, J.; Chen, X.; Wang, C.; Wang, X.; et al. Evaluation of the Global Leadership Initiative on Malnutrition Criteria Using Different Muscle Mass Indices for Diagnosing Malnutrition and Predicting Survival in Lung Cancer Patients. JPEN J. Parenter. Enter. Nutr. 2020, 45, 607–617. [Google Scholar] [CrossRef]
- Steer, B.; Loeliger, J.; Edbrooke, L.; Deftereos, I.; Laing, E.; Kiss, N. Malnutrition Prevalence according to the GLIM Criteria in Head and Neck Cancer Patients Undergoing Cancer Treatment. Nutrients 2020, 12, 3493. [Google Scholar] [CrossRef]
- Ferguson, M.; Capra, S.; Bauer, J.; Banks, M. Development of a valid and reliable malnutrition screening tool for adult acute hospital patients. Nutrition 1999, 15, 458–464. [Google Scholar] [CrossRef]
- Ferguson, M.; Bauer, J.; Gallagher, B.; Capra, S.; Christie, D.; Mason, B. Validation of a malnutrition screening tool for patients receiving radiotherapy. Australas. Radiol. 1999, 43, 325–327. [Google Scholar] [CrossRef]
- Isenring, E.; Cross, G.; Daniels, L.; Kellett, E.; Koczwara, B. Validity of the malnutrition screening tool as an effective predictor of nutritional risk in oncology outpatients receiving chemotherapy. Support. Care Cancer 2006, 14, 1152–1156. [Google Scholar] [CrossRef]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur. J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef]
- Schueren, M.A.E.; Keller, H.; Cederholm, T.; Barazzoni, R.; Compher, C.; Correia, M.I.T.D.; Gonzalez, M.C.; Jager-Wittenaar, H.; Pirlich, M.; Steiber, A.; et al. Global Leadership Initiative on Malnutrition (GLIM): Guidance on validation of the operational criteria for the diagnosis of protein-energy malnutrition in adults. Clin. Nutr. 2020, 39, 2872–2880. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Wie, G.-A.; Cho, Y.-A.; Kim, S.-Y.; Kim, S.-M.; Bae, J.-M.; Joung, H. Prevalence and risk factors of malnutrition among cancer patients according to tumor location and stage in the National Cancer Center in Korea. Nutrition 2010, 26, 263–268. [Google Scholar] [CrossRef]
- Pan, H.; Cai, S.; Ji, J.; Jiang, Z.; Liang, H.; Lin, F.; Liu, X. The impact of nutritional status, nutritional risk, and nutritional treatment on clinical outcome of 2248 hospitalized cancer patients: A multi-center, prospective cohort study in Chinese teaching hospitals. Nutr. Cancer 2013, 65, 62–70. [Google Scholar] [CrossRef]
- Hébuterne, X.; Lemarié, E.; Michallet, M.; de Montreuil, C.B.; Schneider, S.M.; Goldwasser, F. Prevalence of malnutrition and current use of nutrition support in patients with cancer. J. Parenter. Enter. Nutr. 2014, 38, 196–204. [Google Scholar] [CrossRef] [PubMed]
- de Melo Silva, F.R.; de Oliveira, M.G.O.A.; Souza, A.S.R.; Figueroa, J.N.; Santos, C.S. Factors associated with malnutrition in hospitalized cancer patients: A croos-sectional study. Nutr. J. 2015, 14, 1–8. [Google Scholar] [CrossRef] [Green Version]
- de Pinho, N.B.; Martucci, R.B.; Rodrigues, V.D.; D’Almeida, C.A.; Thuler, L.C.; Saunders, C.; Jager-Wittenaar, H.; Peres, W.A. High prevalence of malnutrition and nutrition impact symptoms in older patients with cancer: Results of a Brazilian multicenter study. Cancer 2020, 126, 156–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, A.B.; Reijnierse, E.M.; Lim, W.K.; Maier, A.B. Prevalence of malnutrition comparing the GLIM criteria, ESPEN definition and MST malnutrition risk in geriatric rehabilitation patients: RESORT. Clin. Nutr. 2020, 39, 3504–3511. [Google Scholar] [CrossRef] [PubMed]
- De Groot, L.M.; Lee, G.; Ackerie, A.; van der Meij, B.S. Malnutrition Screening and Assessment in the Cancer Care Ambulatory Setting: Mortality Predictability and Validity of the Patient-Generated Subjective Global Assessment Short form (PG-SGA SF) and the GLIM Criteria. Nutrients 2020, 12, 2287. [Google Scholar] [CrossRef] [PubMed]
- Rondel, A.; Langius, J.; de van der Schueren, M.; Kruizenga, H. The new ESPEN diagnostic criteria for malnutrition predict overall survival in hospitalised patients. Clin. Nutr. 2018, 37, 163–168. [Google Scholar] [CrossRef]
- Sanchez-Rodriguez, D.; Locquet, M.; Bruyère, O.; Lengelé, L.; Cavalier, E.; Reginster, J.-Y.; Beaudart, C. Prediction of 5-year mortality risk by malnutrition according to the GLIM format using seven pragmatic approaches to define the criterion of loss of muscle mass. Clin. Nutr. 2021, 40, 2188–2199. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total N = 2794 a | Female N = 1396 | Male N = 1397 | |
|---|---|---|---|
| N (%) | N (%) | N (%) | |
| Age (years) | |||
| Mean (SD) | 62.7 (14.1) | 60.2(14.6) | 65.2 (13.2) |
| 18–49 years | 470 (16.8) | 319 (22.9) | 151 (10.8) |
| 50–64 years | 917 (32.8) | 483 (34.6) | 434 (31.1) |
| 65–79 years | 1126 (40.3) | 479 (34.3) | 646 (46.2) |
| ≥80 years | 273 (9.8) | 111 (8.0) | 162 (11.6) |
| Unknown | 8 (0.3) | 4 (0.3) | 4 (0.3) |
| Body mass index (kg/m2) | |||
| Mean (SD) | 27.0 (5.9) | 27.2 (6.4) | 26.9 (5.3) |
| <18.5 | 85 (3.0) | 51 (3.7) | 34 (2.4) |
| 18.5–24.9 | 1038 (37.2) | 531 (38.0) | 507 (36.3) |
| 25–29.9 | 957 (34.3) | 425 (30.4) | 531 (38.0 |
| ≥30 | 706 (25.3) | 387 (27.7) | 320 (22.9) |
| Unknown | 8 (0.3) | 2 (0.1) | 5 (0.4) |
| Patient type | |||
| Inpatient | 638 (22.8) | 284 (20.3) | 354 (25.3) |
| Outpatient/day patient | 2156 (77.2) | 1112 (79.7) | 1043 (74.7) |
| Hospital location | |||
| Metropolitan | 2377 | 1206 (86.4) | 1171 (83.8) |
| Regional | 417 | 190 (13.6) | 226 (16.2) |
| Living situation | |||
| Alone | 517 (18.5) | 275 (19.7) | 242 (17.3) |
| Family/carer/residential | 2270 (81.2) | 1119 (80.2) | 1150 (82.6) |
| Unknown | 7 (0.3) | 2 (0.1) | 2 (0.1) |
| Primary malignancy | |||
| Bone and soft tissue | 51 (1.8) | 18 (1.3) | 33 (2.4) |
| Breast | 501 (17.9) | 497 (35.6) | 4 (0.3) |
| Central nervous system | 37 (1.3) | 19 (1.4) | 18 (1.3) |
| Colorectal | 391 (14.0) | 160 (11.5) | 230 (16.5) |
| Endocrine and thyroid | 47 (1.7) | 26 (1.9) | 21 (1.5) |
| Genitourinary | 218 (7.8) | 31 (2.2) | 187 (13.4) |
| Gynaecological | 144 (5.2) | 141 (10.1) | 3 (0.2) |
| Haematological | 527 (18.9) | 199 (14.3) | 328 (23.5) |
| Head and neck | 188 (6.7) | 49 (3.5) | 139 (9.9) |
| Lung | 307 (11.0) | 129 (9.2) | 178 (12.7) |
| Skin and melanoma | 132 (4.7) | 41 (2.9) | 91 (6.5) |
| Upper gastrointestinal | 210 (7.5) | 71 (5.1) | 139 (9.9) |
| Other thoracic or abdominal | 19 (0.7) | 5 (0.4) | 14 (1.0) |
| Cancer of unknown primary | 18 (0.6) | 8 (0.6) | 10 (0.7) |
| Unknown | 4 (0.1) | 2 (0.1) | 2 (0.1) |
| Presence of metastasis | |||
| Yes | 1003 (35.9) | 494 (35.4) | 509 (36.4) |
| No | 1471 (52.6) | 751 (53.8) | 719 (51.5) |
| Uknown | 320 (11.5) | 151 (10.8) | 169 (12.1) |
| Treatment type b | |||
| Chemotherapy | 1920 (68.7) | 1000 (71.6) | 919 (65.8) |
| Radiotherapy | 876 (31.4) | 423 (30.3) | 453 (32.4) |
| Surgery | 655 (23.4) | 377 (27.0) | 277 (19.8) |
| Stem cell transplant | 58 (2.1) | 20 (1.4) | 38 (2.7) |
| Immunotherapy | 170 (6.1) | 76 (5.4) | 94 (6.7) |
| Other | 211 (7.6) | 88 (6.3) | 123 (8.8) |
| Cancer-related management | 76 (2.7) | 37 (2.7) | 39 (2.8) |
| MST c classification | |||
| Not at risk of malnutrition (score < 2) | 1813 (64.9) | 955 (68.4) | 858 (61.4) |
| At risk of malnutrition (score ≥ 2) | 981 (35.1) | 441 (31.6) | 539 (38.6) |
| Diagnostic Criteria | Cut-Off | Prevalence, N (%) |
|---|---|---|
| GLIM | ||
| ≥1 Phenotypic criteria | >5% weight loss in ≤3 months | 619 (23.1) |
| Unintentional weight loss | >10% weight loss in ≥4 months | |
| Low BMI | <20 kg/m2 if <70 years | 202 (7.5) |
| <22 kg/m2 if ≥70 years | ||
| Low muscle mass | Minimum of 4 muscle sites rated mild/moderate or severe | 474 (17.7) |
| AND | ||
| ≥1 Etiologic criteria | ||
| Reduced food intake | ≤50% usual intake for 5–30 days or ≥1 month | 678 (25.3) |
| ≤75% usual intake for ≥1 month | ||
| >75% usual intake for ≥1 month | ||
| Inflammation | Presence of metastatic disease | 399 (14.9) |
| GLIM malnutrition prevalence | 616 (23.0) | |
| GLIM moderate malnutrition prevalence | 296 (11.0) | |
| GLIM severe malnutrition prevalence | 320 (11.9) | |
| ESPEN | ||
| Option 1 | ||
| Low BMI | <18.5 kg/m2 | 66 (2.4) |
| Option 2 | ||
| Unintentional weight loss | >5% weight loss in ≤3 months | 619 (23.0) |
| AND | >10% weight loss in ≥4 months | |
| Low BMI | <20 kg/m2 if <70 years | 202 (7.5) |
| <22 kg/m2 if ≥70 years | ||
| ESPEN malnutrition prevalence | 149 (5.5) | |
| ICD-10 | ||
| Option 1 | ||
| Low BMI | <18.5 kg/m2 | 66 (2.3) |
| Option 2 | ||
| Unintentional weight loss | >5% weight loss | 619 (22.2) |
| AND | ||
| Reduced food intake | Any reduction in food intake | 812 (29.2) |
| AND | ||
| Mild/moderate muscle wasting | Minimum of 4 muscle sites rated mild/moderate or severe | 474 (17.0) |
| ICD-10 malnutrition prevalence | 351 (12.6) |
| ESPEN CRITERIA | |||
| GLIM CRITERIA | Malnourished (143) | Not malnourished (710) | |
| Malnourished (604) | 121 (20.0%) a | 483 (80.0%) a | |
| Not malnourished (249) | 22 (8.8%) b | 227 (91.2%) b | |
| ICD-10 CRITERIA | |||
| GLIM CRITERIA | Malnourished (344) | Not malnourished (465) | |
| Malnourished (573) | 316 (55.1%) a | 257 (44.9%) a | |
| Not malnourished (236) | 28 (11.9%) b | 208 (88.1%) b | |
| ESPEN CRITERIA | |||
| ICD-10 CRITERIA | Malnourished (148) | Not malnourished (726) | |
| Malnourished (351) | 123 (35%) c | 228 (65%) c | |
| Not malnourished (523) | 25 (4.8%) d | 498 (95.2%) d | |
| B | S.E | Wald | df | p | Odds Ratio | 95% CI | Adjusted Odds Ratio b | 95% CI | |
|---|---|---|---|---|---|---|---|---|---|
| Mortality at 30 days | |||||||||
| GLIM a | 0.93 | 0.28 | 10.91 | 1 | 0.001 | 2.53 | 1.46–4.39 | 2.50 | 1.44–4.35 |
| Patient type | 2.10 | 0.29 | 50.91 | 1 | <0.001 | 8.16 | 4.58–14.52 | 8.10 | 4.55–14.43 |
| Metastasis | 1.37 | 0.31 | 20.15 | 1 | <0.001 | 3.95 | 2.17–7.18 | 3.89 | 2.14–7.08 |
| Constant | −5.60 | 0.33 | 291.12 | 1 | <0.001 | 0.004 | 0.001 | ||
| ESPEN a | 0.70 | 0.35 | 4.04 | 1 | 0.044 | 2.01 | 1.02–3.98 | 2.03 | 1.03–4.01 |
| Patient type | 2.31 | 0.27 | 74.73 | 1 | <0.001 | 10.04 | 5.95–16.93 | 9.97 | 5.91–16.83 |
| Metastasis | 1.66 | 0.28 | 35.30 | 1 | <0.001 | 5.24 | 3.03–9.06 | 5.12 | 2.96–8.86 |
| Constant | −5.45 | 0.31 | 311.52 | 1 | <0.001 | 0.004 | 0.002 | ||
| ICD-10 a | 0.85 | 0.29 | 8.87 | 1 | 0.003 | 2.34 | 1.34–4.10 | 2.35 | 1.34–4.13 |
| Patient type | 2.05 | 0.29 | 49.64 | 1 | <0.001 | 7.78 | 4.34–13.78 | 7.76 | 4.39–13.73 |
| Metastasis | 1.41 | 0.29 | 22.91 | 1 | <0.001 | 4.08 | 2.29–7.26 | 4.03 | 2.26–7.16 |
| Constant | −5.42 | 0.32 | 291.65 | 1 | <0.001 | 0.004 | 0.002 | ||
| Unplanned admission or readmission at 30 days | |||||||||
| GLIM a | 0.56 | 0.14 | 15.98 | 1 | <0.001 | 1.76 | 1.33–2.32 | 1.78 | 1.34–2.35 |
| Patient type | 0.63 | 0.14 | 20.87 | 1 | <0.001 | 1.88 | 1.44–2.47 | 1.89 | 1.44–2.48 |
| Metastasis | 0.41 | 0.13 | 9.97 | 1 | 0.002 | 1.50 | 1.17–1.94 | 1.51 | 1.17–1.94 |
| Constant | −2.35 | 0.10 | 530.54 | 1 | <0.001 | 0.09 | 0.12 | ||
| ESPEN a | 0.07 | 0.26 | 0.08 | 1 | 0.772 | 1.08 | 0.65–1.79 | 1.08 | 0.65–1.79 |
| Patient type | 0.75 | 0.13 | 31.99 | 1 | <0.001 | 2.12 | 1.63–2.75 | 2.12 | 1.63–2.75 |
| Metastasis | 0.55 | 0.12 | 20.06 | 1 | <0.001 | 1.74 | 1.37–2.22 | 1.74 | 1.37–2.22 |
| Constant | −2.28 | 0.10 | 530.11 | 1 | <0.001 | 0.10 | 0.12 | ||
| ICD-10 a | 0.45 | 0.17 | 7.12 | 1 | 0.008 | 1.57 | 1.13–2.20 | 1.59 | 1.14–2.21 |
| Patient type | 0.69 | 0.14 | 24.46 | 1 | <0.001 | 1.99 | 1.52–2.62 | 2.00 | 1.52–2.63 |
| Metastasis | 0.53 | 0.13 | 17.31 | 1 | 0.001 | 1.70 | 1.32–2.17 | 1.70 | 1.32–2.18 |
| Constant | −2.33 | 0.10 | 525.20 | 1 | <0.001 | 0.10 | 0.12 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poulter, S.; Steer, B.; Baguley, B.; Edbrooke, L.; Kiss, N. Comparison of the GLIM, ESPEN and ICD-10 Criteria to Diagnose Malnutrition and Predict 30-Day Outcomes: An Observational Study in an Oncology Population. Nutrients 2021, 13, 2602. https://doi.org/10.3390/nu13082602
Poulter S, Steer B, Baguley B, Edbrooke L, Kiss N. Comparison of the GLIM, ESPEN and ICD-10 Criteria to Diagnose Malnutrition and Predict 30-Day Outcomes: An Observational Study in an Oncology Population. Nutrients. 2021; 13(8):2602. https://doi.org/10.3390/nu13082602
Chicago/Turabian StylePoulter, Shay, Belinda Steer, Brenton Baguley, Lara Edbrooke, and Nicole Kiss. 2021. "Comparison of the GLIM, ESPEN and ICD-10 Criteria to Diagnose Malnutrition and Predict 30-Day Outcomes: An Observational Study in an Oncology Population" Nutrients 13, no. 8: 2602. https://doi.org/10.3390/nu13082602