
Populations in Low-Magnesium Areas Were Associated with Higher Risk of Infection in COVID-19’s Early Transmission: A Nationwide Retrospective Cohort Study in the United States

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data and Study Population
2.2. Measures of Variables
2.3. Statistical Analysis
2.4. Sensitivity Analysis
3. Results
3.1. The Baseline Characteristics of the COVID-19 Cumulative Incidence and the Environmental Magnesium Concentrations
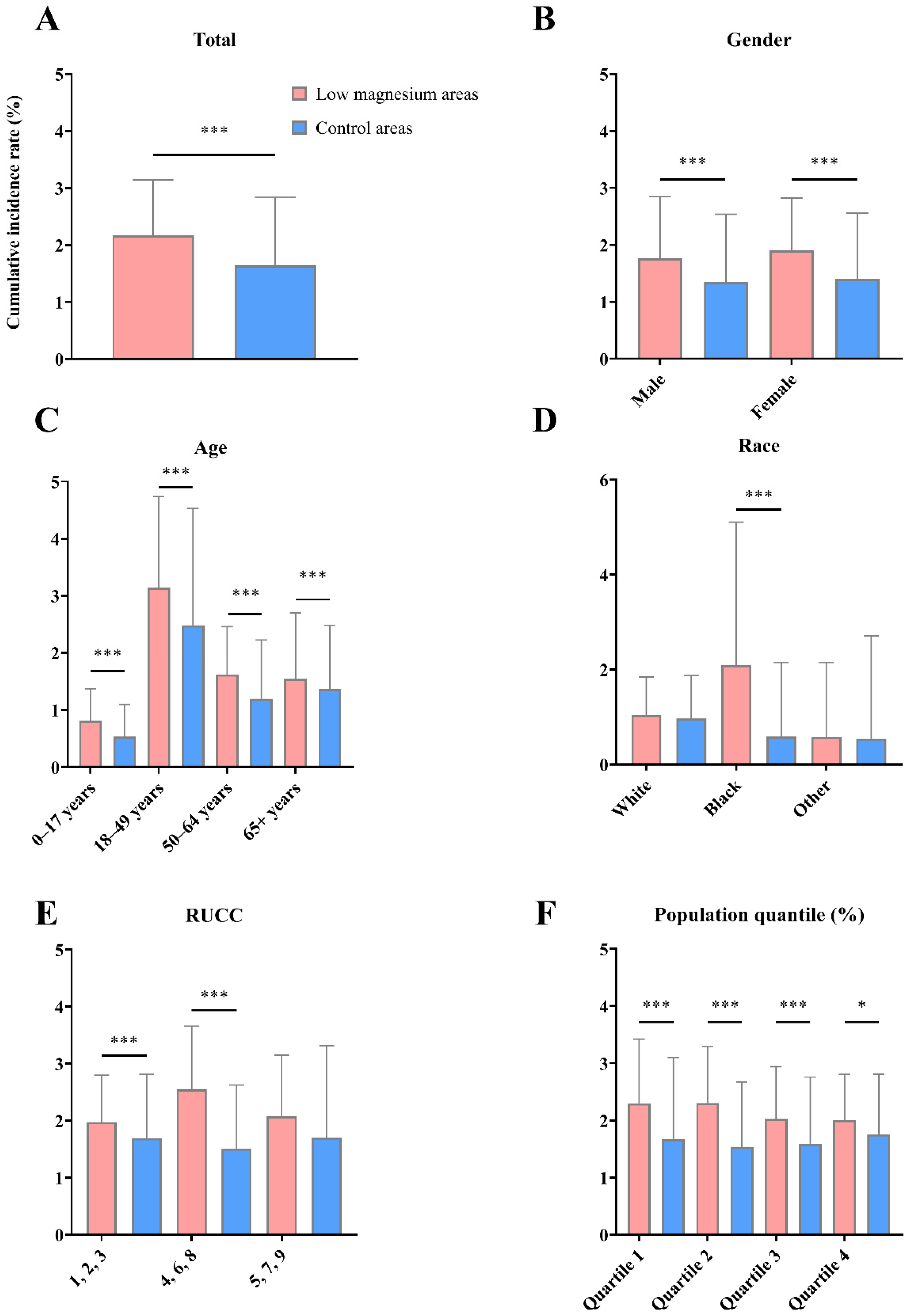
3.2. Baseline Characteristics and the COVID-19 Infectious Risk in the Cohorts of Low-Magnesium Areas and Control Areas
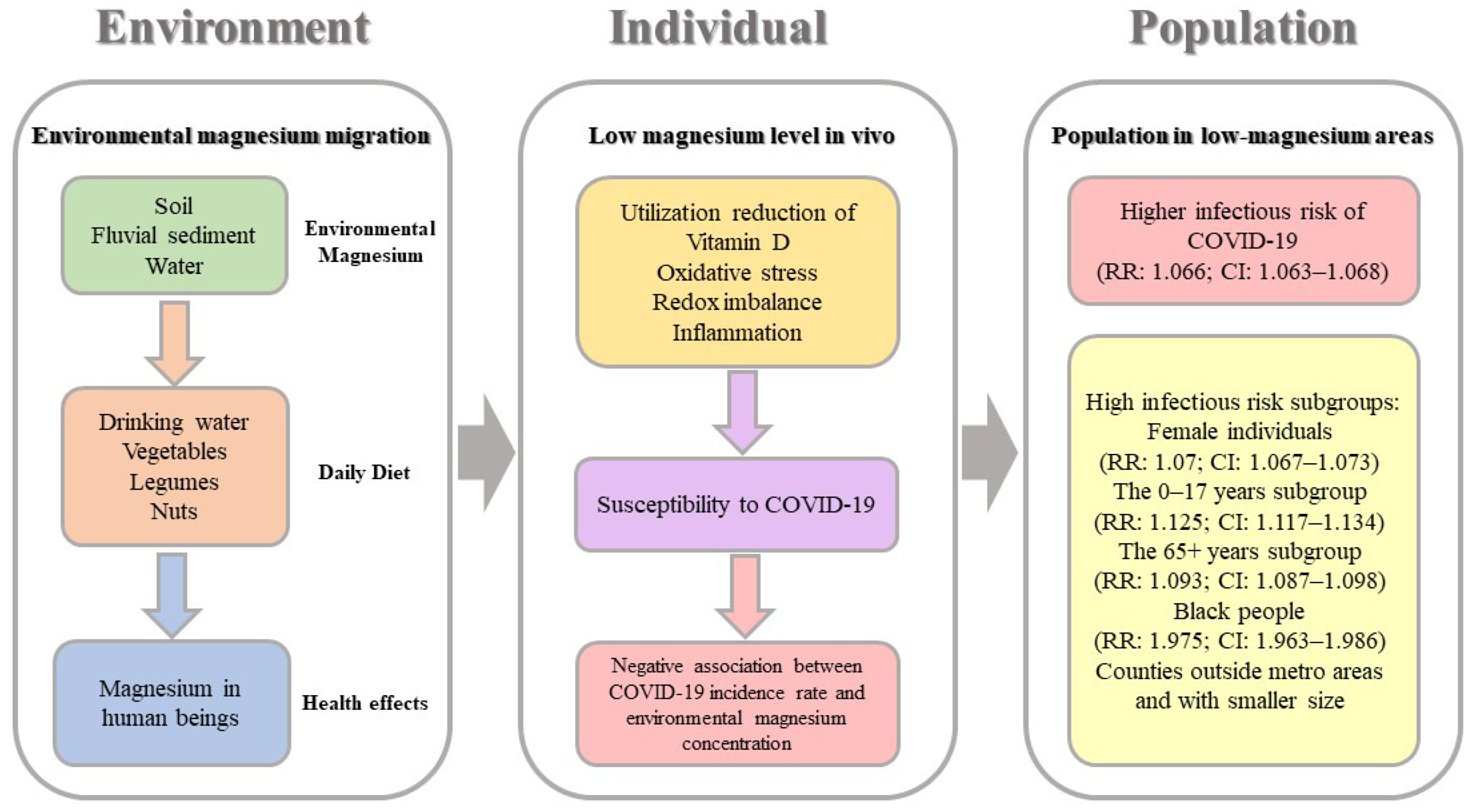
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rodriguez-Leyva, D.; Pierce, G.N. The Impact of Nutrition on the COVID-19 Pandemic and the Impact of the COVID-19 Pandemic on Nutrition. Nutrients 2021, 13, 1752. [Google Scholar] [CrossRef] [PubMed]
- Moscatelli, F.; Sessa, F.; Valenzano, A.; Polito, R.; Monda, V.; Cibelli, G.; Villano, I.; Pisanelli, D.; Perrella, M.; Daniele, A.; et al. COVID-19: Role of Nutrition and Supplementation. Nutrients 2021, 13, 976. [Google Scholar] [CrossRef] [PubMed]
- McAuliffe, S.; Ray, S.; Fallon, E.; Bradfield, J.; Eden, T.; Kohlmeier, M. Dietary micronutrients in the wake of COVID-19: An appraisal of evidence with a focus on high-risk groups and preventative healthcare. BMJ Nutr. Prev. Health 2020, 3, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Galanakis, C.M.; Aldawoud, T.; Rizou, M.; Rowan, N.J.; Ibrahim, S.A. Food Ingredients and Active Compounds against the Coronavirus Disease (COVID-19) Pandemic: A Comprehensive Review. Foods 2020, 9, 1701. [Google Scholar] [CrossRef]
- Butler, M.J.; Barrientos, R.M. The impact of nutrition on COVID-19 susceptibility and long-term consequences. Brain Behav. Immun. 2020, 87, 53–54. [Google Scholar] [CrossRef]
- Jayawardena, R.; Sooriyaarachchi, P.; Chourdakis, M.; Jeewandara, C.; Ranasinghe, P. Enhancing immunity in viral infections, with special emphasis on COVID-19: A review. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 367–382. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef]
- de Baaij, J.H.F.; Hoenderop, J.G.J.; Bindels, R.J.M. Magnesium in Man: Implications for Health and Disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- Fiorentini, D.; Cappadone, C.; Farruggia, G.; Prata, C. Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to Its Deficiency. Nutrients 2021, 13, 1136. [Google Scholar] [CrossRef]
- Maier, J.A.; Castiglioni, S.; Locatelli, L.; Zocchi, M.; Mazur, A. Magnesium and inflammation: Advances and perspectives. Semin. Cell Dev. Biol. 2021, 115, 37–44. [Google Scholar] [CrossRef]
- Calder, P.C.; Carr, A.C.; Gombart, A.F.; Eggersdorfer, M. Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect against Viral Infections. Nutrients 2020, 12, 1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Roche, L.; Mesta, F. Oxidative Stress as Key Player in Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Suhail, S.; Zajac, J.; Fossum, C.; Lowater, H.; McCracken, C.; Severson, N.; Laatsch, B.; Narkiewicz-Jodko, A.; Johnson, B.; Liebau, J.; et al. Role of Oxidative Stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) Infection: A Review. Protein J. 2020, 39, 644–656. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.J.; Cheng, Y.X.; Wu, Y.T. Understanding SARS-CoV-2-Mediated Inflammatory Responses: From Mechanisms to Potential Therapeutic Tools. Virol. Sin. 2020, 35, 266–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damayanthi, H.D.W.T.; Prabani, K.I.P. Nutritional determinants and COVID-19 outcomes of older patients with COVID-19: A systematic review. Arch. Gerontol. Geriatr. 2021, 95, 104411. [Google Scholar] [CrossRef] [PubMed]
- Gasmi, A.; Tippairote, T.; Mujawdiya, P.K.; Peana, M.; Menzel, A.; Dadar, M.; Benahmed, G.; Bjørklund, G. Micronutrients as immunomodulatory tools for COVID-19 management. Clin. Immunol. 2020, 220, 108545. [Google Scholar] [CrossRef]
- Tang, C.F.; Ding, H.; Jiao, R.Q.; Wu, X.X.; Kong, L.D. Possibility of magnesium supplementation for supportive treatment in patients with COVID-19. Eur. J. Pharmacol. 2020, 886, 173546. [Google Scholar] [CrossRef]
- Beigmohammadi, M.T.; Bitarafan, S.; Abdollahi, A.; Amoozadeh, L.; Salahshour, F.; Soltani, D.; Motallebnejad, Z. The association between serum levels of micronutrients and the severity of disease in patients with COVID-19. Nutrition 2021, 91–92, 111400. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Bao, X.; Bi, J.; Lin, Y.; Shan, C.; Fan, X.; Wang, X.; Bian, J. Serum magnesium in patients with severe acute respiratory syndrome coronavirus 2 from Wuhan, China. Magnes Res. 2021, 34, 103–113. [Google Scholar]
- Skalny, A.V.; Timashev, P.S.; Aschner, M.; Aaseth, J.; Chernova, L.N.; Belyaev, V.E.; Glybochko, P.V.; Grabeklis, A.R.; Notova, S.V.; Lobinski, R.; et al. Serum Zinc, Copper, and Other Biometals Are Associated with COVID-19 Severity Markers. Metabolites 2021, 11, 244. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Guerrero-Romero, F.; Barbagallo, M. Magnesium in Infectious Diseases in Older People. Nutrients 2021, 13, 180. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Ho, L.P.; Kalimuddin, S.; Cherng, B.P.Z.; Teh, Y.E.; Thien, S.Y.; Ng, H.J.; Wong, H.M.; Wen, P.J.; Chandran, M.; et al. Cohort study to evaluate the effect of vitamin D, magnesium, and vitamin B-12 in combination on progression to severe outcomes in older patients with coronavirus (COVID-19). Nutrition 2020, 79–80, 111017. [Google Scholar] [CrossRef] [PubMed]
- Pourdowlat, G.; Mousavinasab, S.R.; Farzanegan, B.; Kashefizadeh, A.; Meybodi, Z.A.; Jafarzadeh, M.; Baniasadi, S. Evaluation of the efficacy and safety of inhaled magnesium sulphate in combination with standard treatment in patients with moderate or severe COVID-19: A structured summary of a study protocol for a randomised controlled trial. Trials 2021, 22, 60. [Google Scholar] [CrossRef]
- Marque, S.; Jacqmin-Gadda, H.; Dartigues, J.F.; Commenges, D. Cardiovascular mortality and calcium and magnesium in drinking water: An ecological study in elderly people. Eur. J. Epidemiol. 2003, 18, 305–309. [Google Scholar] [CrossRef]
- Rylander, R. Environmental magnesium deficiency as a cardiovascular risk factor. J. Cardiovasc. Risk 1996, 3, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Galan, P.; Arnaud, M.J.; Czernichow, S.; Delabroise, A.M.; Preziosi, P.; Bertrais, S.; Hercberg, S.; Franchisseur, C.; Maurel, M.; Favier, A. Contribution of mineral waters to dietary calcium and magnesium intake in a French adult population. J. Am. Diet. Assoc. 2002, 102, 1658–1662. [Google Scholar] [CrossRef]
- Davies, B.E. The UK geochemical environment and cardiovascular diseases: Magnesium in food and water. Environ. Geochem. Health 2015, 37, 411–427. [Google Scholar] [CrossRef]
- Ferrandiz, J.; Abellán, J.J.; Gómez-Rubio, V.; López-Quílez, A.; Sanmartín, P.; Abellán, C.; Martínez-Beneito, M.A.; Melchor, I.; Vanaclocha, H.; Gil, J.M.; et al. Spatial analysis of the relationship between mortality from cardiovascular and cerebrovascular disease and drinking water hardness. Environ. Health Perspect. 2004, 112, 1037–1044. [Google Scholar] [CrossRef] [Green Version]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef]
- Monarca, S.; Donato, F.; Zerbini, I.; Calderon, R.L.; Craun, G.F. Review of epidemiological studies on drinking water hardness and cardiovascular diseases. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 495–506. [Google Scholar] [CrossRef]
- Rubenowitz, E.; Axelsson, G.; Rylander, R. Magnesium in drinking water and body magnesium status measured using an oral loading test. Scand. J. Clin. Lab. Investig. 1998, 58, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Marles, R.J. Mineral nutrient composition of vegetables, fruits and grains: The context of reports of apparent historical declines. J. Food Compos. Anal. 2017, 56, 93–103. [Google Scholar] [CrossRef]
- Mayer, A.M.B.; Trenchard, L.; Rayns, F. Historical changes in the mineral content of fruit and vegetables in the UK from 1940 to 2019: A concern for human nutrition and agriculture. Int. J. Food Sci. Nutr. 2021, 1–12. [Google Scholar] [CrossRef]
- Olza, J.; Aranceta-Bartrina, J.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y. Calcium and magnesium in drinking water and risk of death from cerebrovascular disease. Stroke 1998, 29, 411–414. [Google Scholar] [CrossRef] [Green Version]
- Sengupta, P. Potential health impacts of hard water. Int. J. Prev. Med. 2013, 4, 866–875. [Google Scholar]
- Piuri, G.; Zocchi, M.; Della Porta, M.; Ficara, V.; Manoni, M.; Zuccotti, G.V.; Cazzola, R.; Pinotti, L.; Maier, J.A. Magnesium in Obesity, Metabolic Syndrome, and Type 2 Diabetes. Nutrients 2021, 13, 320. [Google Scholar] [CrossRef] [PubMed]
- Saris, N.E.L.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium: An update on physiological, clinical and analytical aspects. Clin. Chim. Acta 2000, 294, 1–26. [Google Scholar] [CrossRef]
- Trapani, V.; Rosanoff, A.; Baniasadi, S.; Barbagallo, M.; Castiglioni, S.; Guerrero-Romero, F.; Maier, J.A.; Iotti, S.; Mazur, A.; Micke, O.; et al. The relevance of magnesium homeostasis in COVID-19. Eur. J. Nutr. 2022, 61, 625–636. [Google Scholar] [CrossRef]
- Verma, H.; Garg, R. Effect of magnesium supplementation on type 2 diabetes associated cardiovascular risk factors: A systematic review and meta-analysis. J. Hum. Nutr. Diet. 2017, 30, 621–633. [Google Scholar] [CrossRef]
- Morabito, R.; Remigante, A.; Marino, A. Protective Role of Magnesium against Oxidative Stress on SO4(=) Uptake through Band 3 Protein in Human Erythrocytes. Cell Physiol. Biochem. 2019, 52, 1292–1308. [Google Scholar] [PubMed]
- Shin, H.J.; Na, H.S.; Do, S.H. Magnesium and Pain. Nutrients 2020, 12, 2184. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.; Mamun, A.; Dominic, A.; Le, N.T. SARS-CoV-2 Mediated Endothelial Dysfunction: The Potential Role of Chronic Oxidative Stress. Front. Physiol. 2021, 11, 1752. [Google Scholar] [CrossRef] [PubMed]
- Kempuraj, D.; Selvakumar, G.P.; Ahmed, M.E.; Raikwar, S.P.; Thangavel, R.; Khan, A.; Zaheer, A.; Zaheer, S.A.; Lyer, S.S.; Burton, C.; et al. COVID-19, Mast Cells, Cytokine Storm, Psychological Stress, and Neuroinflammation. Neuroscientist 2020, 26, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Cumpstey, A.F.; Clark, A.D.; Santolini, J.; Jackson, A.A.; Feelisch, M. COVID-19: A Redox Disease-What a Stress Pandemic Can Teach Us About Resilience and What We May Learn from the Reactive Species Interactome About Its Treatment. Antioxid. Redox Signal. 2021, 35, 1226–1268. [Google Scholar] [CrossRef] [PubMed]
- Diao, B.; Wang, C.; Tan, Y.; Chen, Y.; Liu, Y.; Ning, L.; Chen, Y.; Chen, L.; Li, M.; Liu, Y.; et al. Reduction and Functional Exhaustion of T Cells in Patients with Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef] [PubMed]
- Paul, B.D.; Lemle, M.D.; Komaroff, A.L.; Snyder, S.H. Redox imbalance links COVID-19 and myalgic encephalomyelitis/chronic fatigue syndrome. Proc. Natl. Acad. Sci. USA 2021, 118, e2024358118. [Google Scholar] [CrossRef] [PubMed]
- Saleh, J.; Peyssonnaux, C.; Singh, K.K.; Edeas, M. Mitochondria and microbiota dysfunction in COVID-19 pathogenesis. Mitochondrion 2020, 54, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Uwitonze, A.M.; Razzaque, M.S. Role of Magnesium in Vitamin D Activation and Function. J. Am. Osteopath. Assoc. 2018, 118, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Reddy, P.; Edwards, L.R. Magnesium Supplementation in Vitamin D Deficiency. Am. J. Ther. 2019, 26, e124–e132. [Google Scholar] [CrossRef]
- Meltzer, D.O.; Best, T.J.; Zhang, H.; Vokes, T.; Arora, V.; Solway, J. Association of Vitamin D Status and Other Clinical Characteristics with COVID-19 Test Results. JAMA Netw. Open 2020, 3, e2019722. [Google Scholar] [CrossRef] [PubMed]
- Benskin, L.L. A Basic Review of the Preliminary Evidence That COVID-19 Risk and Severity Is Increased in Vitamin D Deficiency. Front. Public Health 2020, 8, 513. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 62, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Vabret, N.; Britton, G.J.; Gruber, C.; Hegde, S.; Kim, J.; Kuksin, M.; Laserson, U.; Levantovsky, R.; Malle, L.; Moreira, A.; et al. Immunology of COVID-19: Current State of the Science. Immunity 2020, 52, 910–941. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables a | Mean | SD | Min | P25 | P50 | P75 | Max | p-Value b |
|---|---|---|---|---|---|---|---|---|
| Total | 1.772 | 1.17 | 0.000839 | 0.951 | 1.574 | 2.303 | 9.265 | |
| Gender | 0.0579 | |||||||
| Male | 1.451 | 1.18 | 0 | 0.616 | 1.234 | 1.971 | 8.172 | |
| Female | 1.531 | 1.119 | 0 | 0.694 | 1.386 | 2.123 | 8.076 | |
| Age | <0.0001 | |||||||
| 0–17 years | 0.601 | 0.579 | 0 | 0.17 | 0.45 | 0.887 | 3.632 | |
| 18–49 years | 2.646 | 1.965 | 0 | 1.269 | 2.286 | 3.5 | 17.611 | |
| 50–64 years | 1.302 | 1 | 0 | 0.609 | 1.129 | 1.727 | 7.510 | |
| 65+ years | 1.51 | 1.134 | 0 | 0.693 | 1.269 | 2.132 | 7.797 | |
| Race | <0.0001 | |||||||
| White | 0.984 | 0.881 | 0 | 0.372 | 0.76 | 1.341 | 7.151 | |
| Black | 0.971 | 2.128 | 0 | 0 | 0 | 0.975 | 21.809 | |
| Other | 0.553 | 2.031 | 0 | 0 | 0 | 0.41 | 48.663 | |
| RUCC | 0.966 | |||||||
| 1,2,3 | 1.765 | 1.056 | 0.000839 | 1.051 | 1.587 | 2.241 | 8.190 | |
| 4,6,8 | 1.779 | 1.201 | 0.0318 | 0.867 | 1.628 | 2.456 | 6.256 | |
| 5,7,9 | 1.783 | 1.519 | 0.0193 | 0.665 | 1.466 | 2.43 | 9.265 | |
| Population | 0.1944 | |||||||
| Quartile 1 | 1.857 | 1.373 | 0.0318 | 0.888 | 1.535 | 2.541 | 9.265 | |
| Quartile 2 | 1.713 | 1.148 | 0.0546 | 0.867 | 1.528 | 2.25 | 6.256 | |
| Quartile 3 | 1.704 | 1.122 | 0.000839 | 0.947 | 1.511 | 2.133 | 8.190 | |
| Quartile 4 | 1.813 | 1.003 | 0.0367 | 1.12 | 1.688 | 2.349 | 6.622 |
| Counties Count | Mean | SD | Min | P25 | P50 | P75 | Max | |
|---|---|---|---|---|---|---|---|---|
| All areas | 1510 | 0.64 | 0.599 | 0.005 | 0.231 | 0.496 | 0.871 | 4.995 |
| Low-magnesium areas | 378 | 0.111 | 0.0717 | 0.005 | 0.0401 | 0.106 | 0.177 | 0.231 |
| Control areas | 1132 | 0.816 | 0.593 | 0.231 | 0.421 | 0.638 | 1.015 | 4.995 |
| Variables | Low-Magnesium Areas | Control Areas | p-Value a | ||
|---|---|---|---|---|---|
| COVID-19 Cases | Population | COVID-19 Cases | Population | ||
| Total | 1,114,254 | 56,338,459 | 4,287,229 | 230,988,044 | <0.01 |
| Gender | |||||
| Male | 489,331 | 27,520,526 | 1,960,303 | 112,780,099 | <0.01 |
| Female | 555,367 | 28,609,448 | 2,127,123 | 117,242,538 | <0.01 |
| Age | |||||
| 0–17 years | 92,620 | 12,788,830 | 337,425 | 52,434,286 | <0.01 |
| 18–49 years | 609,514 | 20,056,491 | 2,409,001 | 82,231,744 | <0.01 |
| 50–64 years | 219,764 | 14,309,969 | 852,002 | 58,670,963 | <0.01 |
| 65+ years | 163,735 | 9,183,169 | 614,444 | 37,651,051 | <0.01 |
| Race | |||||
| White | 431,091 | 42,719,296 | 1,560,526 | 175,149,390 | <0.01 |
| Black | 173,282 | 7,634,778 | 359,800 | 31,302,641 | <0.01 |
| Other | 53,822 | 5,984,384 | 294,488 | 24,536,014 | <0.01 |
| RUCC | |||||
| 1,2,3 | 952,050 | 49,644,619 | 3,945,039 | 208,483,711 | <0.01 |
| 4,6,8 | 131,092 | 5,123,285 | 240,718 | 16,317,202 | <0.01 |
| 5,7,9 | 30,195 | 1,517,173 | 102,389 | 6,240,513 | <0.01 |
| Population | |||||
| Quartile 1 | 68,193 | 2,930,828 | 119,727 | 7,213,034 | <0.01 |
| Quartile 2 | 93,784 | 4,054,703 | 207,971 | 13,603,546 | <0.01 |
| Quartile 3 | 198,560 | 9,942,781 | 456,803 | 28,670,078 | <0.01 |
| Quartile 4 | 752,800 | 39,356,765 | 3,503,645 | 181,554,768 | <0.01 |
| Variables | RR | 95% CI | PAF (%) | 95% CI |
|---|---|---|---|---|
| Total | 1.066 | 1.063–1.068 | 1.27 | 1.228–1.312 |
| Gender | ||||
| Male | 1.023 | 1.02–1.026 | 0.448 | 0.387–0.51 |
| Female | 1.07 | 1.067–1.073 | 1.354 | 1.294–1.413 |
| Age | ||||
| 0–17 years | 1.125 | 1.117–1.134 | 2.4 | 2.248–2.553 |
| 18–49 years | 1.037 | 1.034–1.04 | 0.727 | 0.672–0.783 |
| 50–64 years | 1.058 | 1.053–1.062 | 1.116 | 1.022–1.21 |
| 65+ years | 1.093 | 1.087–1.098 | 1.782 | 1.671–1.894 |
| Race | ||||
| White | 1.133 | 1.129–1.136 | 2.534 | 2.464–2.605 |
| Black | 1.975 | 1.963–1.986 | 16.044 | 15.889–16.199 |
| Other | 0.753 | 0.746–0.760 | −5.079 | −5.222–−4.920 |
| RUCC | ||||
| 1,2,3 | 1.013 | 1.011–1.016 | 0.258 | 0.215–0.301 |
| 4,6,8 | 1.734 | 1.723–1.746 | 14.93 | 14.731–15.13 |
| 5,7,9 | 1.213 | 1.198–1.229 | 3.999 | 3.722–4.278 |
| Population | ||||
| Quartile 1 | 1.402 | 1.389–1.415 | 10.401 | 10.099–10.704 |
| Quartile 2 | 1.513 | 1.501–1.525 | 10.537 | 10.325–10.749 |
| Quartile 3 | 1.253 | 1.247–1.26 | 6.125 | 5.977–6.274 |
| Quartile 4 | 0.991 | 0.989–0.994 | −0.158 | −0.201–−0.114 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, J.; Tang, L.; Liu, X.; Li, Y.; Chen, J.; Huang, W.; Liu, M. Populations in Low-Magnesium Areas Were Associated with Higher Risk of Infection in COVID-19’s Early Transmission: A Nationwide Retrospective Cohort Study in the United States. Nutrients 2022, 14, 909. https://doi.org/10.3390/nu14040909
Tian J, Tang L, Liu X, Li Y, Chen J, Huang W, Liu M. Populations in Low-Magnesium Areas Were Associated with Higher Risk of Infection in COVID-19’s Early Transmission: A Nationwide Retrospective Cohort Study in the United States. Nutrients. 2022; 14(4):909. https://doi.org/10.3390/nu14040909
Chicago/Turabian StyleTian, Jing, Liwei Tang, Xinwei Liu, Yulan Li, Jinghong Chen, Weiren Huang, and Min Liu. 2022. "Populations in Low-Magnesium Areas Were Associated with Higher Risk of Infection in COVID-19’s Early Transmission: A Nationwide Retrospective Cohort Study in the United States" Nutrients 14, no. 4: 909. https://doi.org/10.3390/nu14040909