
Child and Adult Care Food Program Participation Benefits, Barriers and Facilitators for Independent Child Care Centers in California
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection, Recruitment, and Enrollment
2.2. Surveys, Focus Groups and Structured Interviews
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
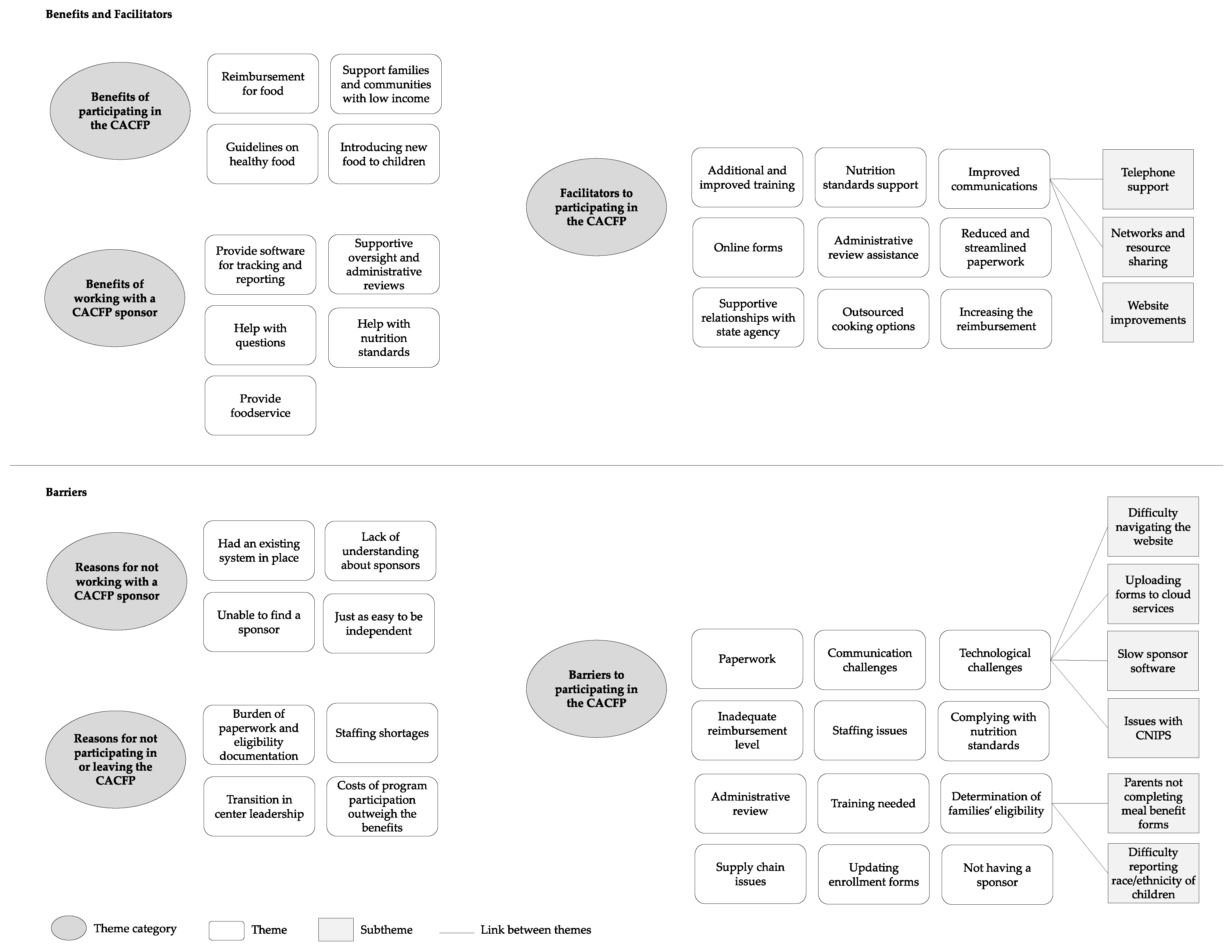
3.2. Summary of Themes and Subthemes
3.2.1. Benefits of Participating in the CACFP
3.2.2. Benefits of Working with a CACFP Sponsoring Organization
3.2.3. Barriers Related to Participating in the CACFP
3.2.4. Reasons Why Some Independent Centers Do Not Participate in the CACFP or Have Left the Program
3.2.5. Reasons Independent Centers Do Not Work with a CACFP Sponsoring Organization
3.2.6. Facilitators to Participating in the CACFP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coleman-Jensen, A.; Rabbit, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2021. Available online: https://www.ers.usda.gov/webdocs/publications/104656/err-309.pdf?v=3317.9 (accessed on 4 October 2022).
- Gundersen, C.; Ziliak, J.P. Food Insecurity and Health Outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, P.; Chung, R.; Frank, D.A. Association of Food Insecurity with Children’s Behavioral, Emotional and Academic Outcomes: A Systematic Review. J. Dev. Behav. Pediatr. 2017, 38, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Natzke, L. Early Childhood Program Participation: 2019. Available online: https://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=2020075REV (accessed on 4 October 2022).
- Council on Community Pediatrics; Committee on Nutrition. Promoting Food Security for All Children. Pediatrics 2015, 136, 1431–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- USDA Food and Nutrition Services. Child and Adult Care Food Program. Available online: https://www.fns.usda.gov/cacfp (accessed on 25 August 2022).
- Ritchie, L.D.; Boyle, M.; Chandran, K.; Spector, P.; Whaley, S.E.; James, P.; Samuels, S.; Hecht, K.; Crawford, P. Participation in the child and adult care food program is associated with more nutritious foods and beverages in child care. Child. Obes. 2012, 8, 224–229. [Google Scholar] [CrossRef]
- Erinosho, T.; Vaughn, A.; Hales, D.; Mazzucca, S.; Gizlice, Z.; Ward, D. Participation in the Child and Adult Care Food Program Is Associated with Healthier Nutrition Environments at Family Child Care Homes in Mississippi. J. Nutr. Educ. Behav. 2018, 50, 441–450. [Google Scholar] [CrossRef]
- Gurzo, K.; Lee, D.L.; Ritchie, K.; Yoshida, S.; Homel Vitale, E.; Hecht, K.; Ritchie, L.D. Child Care Sites Participating in the Federal Child and Adult Care Food Program Provide More Nutritious Foods and Beverages. J. Nutr. Educ. Behav. 2020, 52, 697–704. [Google Scholar] [CrossRef]
- Chriqui, J.F.; Leider, J.; Schermbeck, R.M.; Sanghera, A.; Pugach, O. Changes in Child and Adult Care Food Program (CACFP) Practices at Participating Childcare and Education Centers in the United States Following Updated National Standards, 2017–2019. Nutrients 2020, 12, 2818. [Google Scholar] [CrossRef]
- Korenman, S.; Abner, K.S.; Kaestner, R.; Gordon, R.A. The Child and Adult Care Food Program and the Nutrition of Preschoolers. Early Child. Res. Q. 2013, 28, 325–336. [Google Scholar] [CrossRef] [Green Version]
- Heflin, C.; Arteaga, I.; Gable, S. The Child and Adult Care Food Program and Food Insecurity. Soc. Serv. Rev. 2015, 89, 77–98. [Google Scholar] [CrossRef] [Green Version]
- USDA Food and Nutrition Services. Child Nutrition Tables. Available online: https://www.fns.usda.gov/pd/child-nutrition-tables (accessed on 25 August 2022).
- Bauer, K.W.; Chriqui, J.F.; Andreyeva, T.; Kenney, E.L.; Stage, V.C.; Dev, D.; Lessard, L.; Cotwright, C.J.; Tovar, A. A Safety Net Unraveling: Feeding Young Children during COVID-19. Am. J. Public Health 2021, 111, 116–120. [Google Scholar] [CrossRef]
- Homel Vitale, E. Access to Food in Early Care Continues to Decline. Available online: https://nourishca.org/publications/report/access-to-food-in-early-care-continues-to-decline/ (accessed on 25 August 2022).
- Andreyeva, T.; Henderson, K.E. Center-Reported Adherence to Nutrition Standards of the Child and Adult Care Food Program. Child. Obes. 2018, 14, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Andreyeva, T.; Sun, X.; Cannon, M.; Kenney, E.L. The Child and Adult Care Food Program: Barriers to Participation and Financial Implications of Underuse. J. Nutr. Educ. Behav. 2022, 54, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Schermbeck, R.M.; Kim, M.; Chriqui, J.F. Independent Early Childhood Education Centers’ Experiences Implementing the Revised Child and Adult Care Food Program Meal Pattern Standards: A Qualitative Exploratory Study. J. Acad. Nutr. Diet. 2021, 121, 678–687.e1. [Google Scholar] [CrossRef]
- AB-89 Budget Act of 2020—California Legislative Information. Available online: https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201920200AB89 (accessed on 25 August 2022).
- California Department of Social Services. CACFP Manual Terms, Definitions and Acronyms. Available online: https://cdss.ca.gov/cacfp/resources/cacfp-manual-terms-definitions-and-acronyms (accessed on 25 August 2022).
- California Department of Social Services. CACFP Administrative Manual Section 1.3. Available online: https://cdss.ca.gov/cacfp/resources/cacfp-administrative-manual-section-13 (accessed on 25 August 2022).
- Chriqui, J.F.; Schermbeck, R.M.; Leider, J. Food Purchasing and Preparation at Child Day Care Centers Participating in the Child and Adult Care Food Program in the United States, 2017. Child. Obes. 2018, 14, 375–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Washington State Department of Health. Guidelines for Using Rural-Urban Classification Systems for Community Health Assessment. Available online: https://doh.wa.gov/sites/default/files/legacy/Documents/1500/RUCAGuide.pdf (accessed on 25 August 2022).
- Foley, G.; Timonen, V. Using Grounded Theory Method to Capture and Analyze Health Care Experiences. Health Serv. Res. 2015, 50, 1195–1210. [Google Scholar] [CrossRef] [Green Version]
- Organisation for Economic Co-operation and Development. Education at a Glance 2016, OECD Indicators. Available online: http://edukacjaidialog.pl/_upload/file/2016_10/education_at_a_glance_2016.pdf (accessed on 4 October 2022).
- Green, R.; Bergmeier, H.; Chung, A.; Skouteris, H. How are health, nutrition, and physical activity discussed in international guidelines and standards for children in care? A narrative review. Nutr. Rev. 2022, 80, 919–930. [Google Scholar] [CrossRef]
- Johnston, C.; Kearney, J.; Hayes, N.; Slattery, C.G.; Corish, C. Healthy incentive scheme in the Irish full-day-care pre-school setting. Proc. Nutr. Soc. 2014, 73, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Buttivant, H.; Knai, C. Improving food provision in child care in England: A stakeholder analysis. Public Health Nutr. 2012, 15, 554–560. [Google Scholar] [CrossRef] [Green Version]
- Neelon, S.E.; Burgoine, T.; Hesketh, K.R.; Monsivais, P. Nutrition practices of nurseries in England. Comparison with national guidelines. Appetite 2015, 85, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Gerritsen, S.; Dean, B.; Morton, S.M.B.; Wall, C.R. Do Childcare Menus Meet Nutrition Guidelines? Quantity, Variety and Quality of Food Provided in New Zealand Early Childhood Education Services. Aust. N. Z. J. Public Health 2017, 41, 345–351. [Google Scholar] [CrossRef]
- Spence, A.; Love, P.; Byrne, R.; Wakem, A.; Matwiejczyk, L.; Devine, A.; Golley, R.; Sambell, R. Childcare Food Provision Recommendations Vary across Australia: Jurisdictional Comparison and Nutrition Expert Perspectives. Int. J. Environ. Res. Public Health 2020, 17, 6793. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| CACFP Group | Total in CDSS Database | Sent Recruitment Materials | Agreed to Participate | Participated |
|---|---|---|---|---|
| Independent centers contracting directly with the state (FG1) | 342 (including 1 tribal and 5 military) | 102 (including 1 tribal and 5 military) | 22 | 10 |
| Independent centers working with a sponsoring organization (FG2) | 182 (0 tribal and 0 military) | 100 | 15 | 6 |
| Sponsors of independent centers (FG3) | 10 | 10 | 5 | 5 |
| Characteristic (n (%)) | Focus Group 1 (n = 10) | Focus Group 2 (n = 6) | Focus Group 3 (n = 5) |
|---|---|---|---|
| Job title | |||
| Center owner | 4 (40) | 4 (67) | -- |
| Director or site supervisor | 8 (80) | 2 (33) | 3 (60) |
| Other | 1 (10) | 1 (17) | 4 (80) |
| Sex, female | 10 (100) | 6 (100) | 4 (80) |
| Race/ethnicity | |||
| American Indian or Alaskan Native | 1 (10) | 0 (0) | 0 (0) |
| Asian or Other Pacific Islander | 1 (10) | 0 (0) | 1 (20) |
| Black or African American | 3 (30) | 1 (17) | 2 (40) |
| Hispanic or Latinx | 2 (20) | 1 (17) | 1 (20) |
| White | 3 (30) | 4 (67) | 1 (20) |
| Education | |||
| High school graduate | 0 (0) | 0 (0) | 1 (20) |
| Some college or Associates degree | 4 (40) | 1 (17) | 1 (20) |
| Bachelor’s degree | 3 (30) | 5 (83) | 0 (0) |
| Master’s degree or higher | 3 (30) | 0 (0) | 3 (60) |
| English preferred language | 10 (100) | 5 (83) | 5 (100) |
| Site type | |||
| For profit | 4 (40) | -- | 0 (0) |
| Government/Military | 1 (10) | -- | 0 (0) |
| Non-profit | 4 (40) | -- | 5 (100) |
| Tribal | 1 (10) | -- | -- |
| Program type | |||
| Infant/Toddler Center | 6 (60) | 2 (33) | -- |
| Preschool Age Center | 10 (100) | 6 (100) | -- |
| School Age Center | 2 (20) | 4 (67) | -- |
| Metropolitan areas served 2 | |||
| Urban | 8 (80) | 5 (83) | -- |
| Suburban | 1 (10) | 1 (17) | -- |
| Rural | 1 (10) | 0 (0) | -- |
| CDSS CACFP Regions served 3 | |||
| Northern | 3 (30) | 1 (17) | 3 (60) |
| Central | 3 (30) | 2 (33) | 1 (20) |
| Los Angeles | 2 (20) | 1 (17) | 2 (40) |
| Southern | 3 (30) | 2 (33) | 2 (40) |
| Years in operation | |||
| 1 to <3 years | 1 (10) | 1 (17) | 0 (0) |
| 3 to <5 years | 1 (10) | 1 (17) | 0 (0) |
| 5 to <10 years | 1 (10) | 0 (0) | 3 (60) |
| 10+ years | 7 (70) | 4 (67) | 2 (40) |
| Years of CACFP participation | |||
| 1 to <3 years | 3 (30) | 3 (50) | -- |
| 3 to <5 years | 0 (0) | 2 (33) | -- |
| 5 to <10 years | 2 (20) | 1 (17) | -- |
| 10+ years | 5 (50) | 0 (0) | -- |
| No. staff in organization (Mean (SD)) | 14 (7) | 14 (8) | 82 (100) |
| Staff preferred language or Language organization supports for center directors (Mean % (SD)) | |||
| English | 80 (0.2) | 79.5 (18.7) | 5 (100) |
| Spanish | 12 (0.2) | 11 (9.6) | 4 (80) |
| Chinese | 3 (0.1) | 2 (5.3) | 0 (0) |
| Other | 5 (0.1) | 0 (0) | 2 (40) |
| No. children at center (Mean (SD)) | |||
| 0–5 months | 1 (2) | 1 (2) | -- |
| 6–11 months | 3 (3) | 1 (2) | -- |
| 12–23 months | 8 (7) | 7 (8) | -- |
| 24–35 months | 11 (9) | 21 (12) | -- |
| 3–5 years | 34 (16) | 51 (37) | -- |
| 6+ years | 5 (10) | 8 (12) | -- |
| Child preferred language (Mean % (SD)) | |||
| English | 70 (23.0) | 79 (24.6) | -- |
| Spanish | 21 (25.0) | 17 (20.4) | -- |
| Chinese | 5 (8.7) | 4 (10.2) | -- |
| Other | 4 (6.3) | 0 (0) | -- |
| Children qualify for subsidies (Mean % (SD)) | 46 (29.0) | 31 (15.4) | -- |
| Type of child care offered | |||
| Full day | 4 (40) | 1 (17) | -- |
| Half- and Full day | 6 (60) | 5 (83) | -- |
| Responsible for menu planning | |||
| Director or site supervisor | 6 (60) | 5 (83) | -- |
| Center teacher or teacher’s aide | 0 (0) | 0 (0) | -- |
| Cook or chef | 4 (40) | 1 (17) | -- |
| Dietitian | 0 (0) | 1 (17) | -- |
| Other | 1 (10) | 1 (17) | -- |
| Responsible for CACFP administrative paperwork | |||
| Director or site supervisor | 8 (80) | 4 (67) | -- |
| Center teacher or teacher’s aide | 4 (40) | 0 (0) | -- |
| Cook or chef | 3 (30) | 0 (0) | -- |
| Dietitian | 0 (0) | 0 (0) | -- |
| Other | 1 (10) | 3 (50) | -- |
| Sponsor provides foodservice | 0 (0) | 1 (17) | 3 (60) |
| Meals, snacks provided by center | |||
| Breakfast | 8 (80) | 6 (100) | -- |
| Lunch | 10 (10) | 4 (67) | -- |
| Supper | 0 (0) | 1 (17) | -- |
| Mid-morning snack | 6 (60) | 0 (0) | -- |
| Mid-afternoon snack | 10 (100) | 5 (83) | -- |
| Evening snack | 1 (10) | 0 (0) | -- |
| Food preparation location (does not include food from parents) | |||
| On site (at center) | 9 (90) | 4 (67) | -- |
| Central kitchen operated by center(s) | 1 (10) | 1 (17) | -- |
| Other | 0 (0) | 1 (17) | -- |
| Response when asked about where they receive support for the CACFP | |||
| CACFP Roundtable | 4 (40) | 0 (0) | 4 (80) |
| National CACFP Sponsors Association | 0 (0) | 0 (0) | 1 (20) |
| National CACFP Forum | 1 (10) | 0 (0) | 2 (40) |
| USDA Team Nutrition | 1 (10) | 0 (0) | 3 (60) |
| Institute of Child Nutrition | 0 (0) | 0 (0) | 1 (20) |
| CDSS or CDE | 5 (50) | 0 (0) | 5 (100) |
| Other | 0 (0) | 1 (17) | 0 (0) |
| Theme | Illustrative Quotes |
|---|---|
| Reimbursement for food | “Probably the main reason why we participate in the program [CACFP] is to subsidize the cost.”—FG1_6 |
| “I wanted to make sure to be able to continue to provide lunches for the children and not have to increase the parents’ tuition to cover the cost of that.”—FG1_9 | |
| “It [CACFP] helps us offset the cost of the food, the cost of food is rising…”—FG2_1 | |
| Supporting families and communities with low income | “The kids that typically attend here are low-income and on subsidy programs… it really helped the families.”—FG1_8 |
| “[We have] a large number of students on low income, subsidized, who needed the lunch program.”—FG1_11 | |
| Guidelines on healthy food | “We like the guidelines for food. It keeps healthy food in our center, as opposed to having parents bring whatever they want, which may not be nutritious.”—FG1_2 |
| “I like the technical assistance. I like knowing that I’m serving the correct portions, the enhanced menu items, the different kinds of vegetables and whole grains.”—FG1_1 | |
| “They [the sponsor] have a dietitian that helps look over our menus just to validate the nutrition level and monitor all the food groups… and keeping us on track with the healthiest options that we can serve.”—FG2_3 | |
| Introducing new foods to children | “…introducing new foods to kids, which is great, because I have picky eaters.”—FG2_3 |
| Theme | Illustrative Quotes |
|---|---|
| Provide software for tracking and reporting | “[The sponsor] provides us with a system called Kid Kare that helps to keep track of all of the food that we’ve served.”—FG2_2 |
| Supportive oversight and administrative reviews | “They [the sponsor] see if there was anything that we might have missed, like expired enrollment forms are an easy one to miss.”—FG2_2 |
| “They [the sponsor] also oversee the audits [administrative reviews]. They come in and kind of do little control checks on our service, cleanliness, temperature checks, lots of things. They help us ensure that we have the accurate meal benefit forms filled out and that we’re accessing the reimbursements for all the kids. And they help process the payments.”—FG2_3 | |
| Help with questions | “They’re [the sponsor] always there if I need to reach out and have questions.”—FG2_4 |
| Help with nutrition standards | “They [the sponsor] also help with providing us with the food service guidelines, and they give us lots of handouts and just healthy meal ideas.”—FG2_2 |
| Provide foodservice | “We receive our food from a food vendor [the sponsor] … we do the count, and we give them the count. They have the children’s names, and they bring the food and serve breakfast, lunch and snacks every day.”—FG2_7 |
| Theme | Illustrative Quotes |
|---|---|
| Paperwork | “My challenge is the paperwork… getting it uploaded to the site… for me, it’s just not very intuitive.”—FG1_6 |
| “We implement a lot of technological resources to reduce paperwork. But for those centers that are still running, with paper driven operations, it’s paperwork. There’s a lot of moving pieces, a lot of ways to mess up, and small technological, for small technical aspects of the program that can end up costing the center their reimbursements.”—FG3_5 | |
| “I have no program [for streamlining the paperwork]. I have to do everything, write it out… I’ve been doing the claims and everything by hand.”—FG3_6 | |
| Communication challenges | “So sometimes going back and forth over email, they’ll [the sponsor] send me an email, sometimes, I may not understand what they’re talking about. So, it’s a lot of back-and-forth emails.”—FG2_1 |
| “I would say the greatest technological barrier is information, transferring of information, receiving information, receiving two different answers for the same question from two different people [State analysts].”—FG3_2 | |
| “I’ve been starting to get these emails where they [state agency] start sending you these things like notices, and I’ll click into the links, but I still have trouble where to be guided on what to click on to read what they are telling me… I go to the link, and I still am unable to locate where that information is.”—FG3_6 | |
| Technological challenges | |
| Subtheme 1. Difficulty navigating the website | “…when I go to find a form. They’re not alphabetical. They’re listed by form number. And it’s so frustrating to have to read all of those to find the one I want because it wastes so much time.”—FG1_1 |
| “I would like to be able to access any new policy or new procedures that we have more easily. I mean, I’ve searched for like an hour or so. And I didn’t find anything today.”—FG1_5 | |
| Subtheme 2. CNIPS difficult to use, has outdated information and infrastructure | “I rarely go to that website [CNIPS]. Because it’s hard. For me, the whole program is kind of difficult, because they send out things and they have you do these classes once a year, but they’re not really helpful.”—FG1_3 |
| “[I wish] that you could just keep the previous year’s information [in CNIPS] and not have to go back… a lot of the stuff is a repeat.”—FG3_3 | |
| “I think there’s ways that for a sponsor, it [CNIPS] can be more streamlined. There’s a lot of bottlenecks between submission to the state agency, and then the timeframe it takes for an analyst to get back to the sponsor… for timing purposes, it becomes a little difficult.”—FG3_5 | |
| Subtheme 4. Slow software provided by sponsoring organization | “The system [Kid Kare software] is very, very slow. And so, it’s very time consuming.”—FG2_4 |
| “It’s very slow…but there’s a lot of [data] input that you have to put in for each child and it can take a long time to do that when the program [Kid Kare by Minute Menu] is running very slow.”—FG2_5 | |
| Subtheme 5. Uploading forms to cloud-based file hosting service 2 | “And we’ve had to create Dropboxes now. There’s just a little bit more expense when you add the technological piece. So, sometimes building into your budget, I had to add more staff, if we were going to add the technology piece, and then the equipment piece and the cost. I mean, five Dropboxes, and then you add 40 Dropboxes, it does add a little bit.”—FG3_1 |
| Inadequate reimbursement level 3 | “We came about $4000 shy of being fully reimbursed for the food we served, much less any of the staff salaries or equipment or expenses.”—FG1_1 |
| “It’s sufficient [the reimbursement], but it doesn’t cover everything. It doesn’t cover the time for the work being done. Paperwork or the cook.”—FG1_2 | |
| “I think it [the reimbursement level] should be a little higher, because food is very expensive… they’re asking you to buy these products, certain products, but it’s really hard to be able to have enough money to buy the better products…because it’s expensive.”—FG1_3 | |
| “I wish that we would be reimbursed for everybody. It would be nice because it’s overall beneficial for all the kids and just because a child’s income level is higher it doesn’t mean they’re eating a balanced meal at home at all or exposed to different kinds of foods.”—FG2_5 | |
| Staffing issues | “We were short-staffed… we didn’t have enough staff and found that the time that goes in to do the administrative work and counting correctly and training [is a barrier].”—FG1_10 |
| “The staffing has been just a nightmare [during the COVID-19 pandemic] … we’re just not able to find staffing… my directors have literally ended up doing cooking and cleaning to maintain this program.”—FG1_11 | |
| “The staffing… [is a barrier centers experience when participating in CACFP].”—FG3_2 | |
| Complying with nutrition standards | “So, I’ve looked at their [the CACFP] buying guides, their meal patterns… I still find them both to be very difficult when I go to the store to choose what they’re saying that I can do, or just finding foods. Especially now finding foods that fits into the categories that they want.”—FG1_3 |
| “One of the biggest challenges is the constant changing of what we can serve or what we can’t serve.”—FG2_2 | |
| “Some of the things that the kids like, is not something that they’re able to prepare for the kids just because of the rules that they [the CACFP] have to follow… sometimes it doesn’t give you all the flexibility that you like.”—FG2_7 | |
| “The ability to have the centers that we serve understand the processes. We have such a hard time just getting across simple requirements, that CDE and now CDSS pass on to us that we must pass on to them. And it’s a barrier because even though they want the food. We can’t get the buy in from the centers.”—FG3_2 | |
| Administrative review | “The very first review that I had after my first year was extremely intimidating, because I didn’t ever have anyone come in because of the pandemic and show me anything. So, we were trying to do this via email and whatnot.”—FG1_9 |
| “It’s kind of hard on the monitoring [administrative review] … [the sponsor] only have a sampling of some of us who will be chosen for the monitoring [administrative review]. So, we don’t actually always see the state [agency]. But that’s why they come out and do their checks, and kind of do their own version of it. So, I only see it speaking for myself through the eyes of the sponsor”—FG2_3 | |
| Determination of families’ CACFP eligibility 4 | |
| Subtheme 1. Difficulty reporting race/ethnicity of children | “One of the challenges that came up on my last review was having to put a number for the nationality/race information. On the packet that you give to the parents, it states that portion is optional to fill out…. Upon review, I told her [CACFP state monitor] I don’t have an exact number, because we have families that I don’t feel comfortable assuming I know what they are. We have many Native Americans and honestly looking at them, I wouldn’t be able to assume that. So, I was really uncomfortable giving that information to them [CACFP state monitor] … I said, “Some of them opted out, they didn’t fill in the information.” And she basically told me to guess, and I don’t think that’s fair to put on us.”—FG1_9 |
| “I was told that we weren’t we were not supposed to discriminate, but then they’re [CACFP state monitor] making us guess [race/ethnicity]. But I can’t get at somebody’s nationality or ethnicity based on what they look like. And that’s discrimination in itself I thought. Either they should just not ask us, not force us to guess on it… or just not ask at all.”—FG1_10 | |
| Subtheme 2. Parents not completing meal benefit forms | “A lot of parents don’t want to complete the form [meal benefit form] because they don’t want to put their income down.”—FG2_4 |
| Training needed | “Understanding it to the level that we feel that we’re confident and can do it right. So, for me, that has been very hard to make sure that my cook knows what to do, my teachers know what to do, as well as myself, the administration part. Because of the pandemic, we’ve had very little contact with the state [agency] at all as to what to do. And this is our first time, so it’s very tough.”—FG1_8 |
| “Training is always an issue. Our teachers have the basic training, and they don’t think [nutrition] is as important as everything else.”—FG1_2 | |
| Supply chain issues | “We can’t find certain items at the grocery store… we want to buy the whole grain pasta. They don’t have it, or there’s just certain things sometimes the store runs out of. So, we go to grocery stores, we don’t have Sysco deliver or anything like that… And sometimes they don’t have the items on the shelves. So that is a challenge… Also, even paper products like plates and cups and spoons run out, too, not just food, but items that we need for the food program.”—FG1_4 |
| “It’s been hard for certain vendors to get certain products, so it’s been a little dicey with certain items to use lately.”—FG3_6 | |
| Updating enrollment forms | “It’s just keeping up with all of the dates, when children withdraw. We get a lot of withdrawals and re-enroll.”—FG1_8 |
| Not having a sponsor | “One of my greatest challenges is being my own sponsor. It’s because I’ve also done it the other way, I know how they both work, it is a lot more work [not participating in the CACFP through a sponsor].”—FG1_9 |
| Theme | Illustrative Quotes |
|---|---|
| Burden of paperwork and eligibility documentation | “It’s the paperwork… Just having a center allow us to look at their enrollment records is a task… Because once we start asking for paperwork… for meal benefit forms to be completed, they [centers] want to opt out, or [centers say] “I don’t want the service… we can’t afford to be a center that won’t comply”. But then that’s why they [centers] pull back because we request too much information from them in their eyes. Or too much at one time, I guess I should say… or the parents don’t want to complete the forms [meal benefit form, enrollment form]. They [parents] don’t want you to have their information.”—FG3_2 |
| “And then also eligibility documentation, a lot of parents don’t understand it, they don’t want to fill it out. And they’re less than forthcoming about the information on the eligibility documents… “– FG3_5 | |
| Staffing shortages | “We’re serving about 90 lunches a day. And when my directors are being pulled in to do that, the rest of the school is falling apart. So, we considered very seriously in this last month, not continuing with [the] program [CACFP] just because we don’t have the manpower to keep administering it… all of the manpower and payroll involved is starting to become just not just worth it, not doable, not sustainable. So, we’ve reconsidered the food program recently.”—FG1_11 |
| Transition in center leadership | “When I came, they had discontinued [participating in the CACFP] …I think it’s because they did a transfer of staff, of directors…So, I decided to start it back up.”—FG1_5 |
| Costs of program participation outweigh the benefits | “If they’re [centers] not staying abreast of what they’re doing wrong, a review of three months of paperwork can turn into 12 months and go back three years. And so, all of a sudden, now they [centers] owe money back to the state agency, and they’re looking at it like, ‘Well, this was a lot of work, really, for nothing in the end, and it cost me money. So why continue to go forward with it?’”—FG3_5 |
| Theme | Illustrative Quotes |
|---|---|
| Had an existing system in place | “The school used to be a Head Start state preschool, and they’ve dealt directly with the state so we just kind of followed in line with the previous blueprint of the school.”—FG1_8 |
| “We just took over from a school and adopted what they were doing, they did all their own administration of the program, they kind of trained us on how to do it.”—FG1_11 | |
| Lack of understanding about sponsors | “In [my county], only family child care providers could use the sponsoring agency.”—FG1_1 |
| “I wasn’t aware of the other sponsoring agencies out there… had I known that there was a sponsor, I probably would have preferred that over dealing directly with the state.”—FG1_8 | |
| Unable to find a sponsor | “I was told that I had to be my own sponsor. That was the only option because I was not family child care any longer.”—FG1_9 |
| “I talked to two different sponsors. A lot of them are just serving family centers (family child care homes), not center based. So, I wasn’t able to find anybody who could help us. I just decided to learn it myself.”—FG1_10 | |
| Just as easy to be independent | “[Our director] did have a sponsoring agency. And then she figured out that she was still doing all the work and providing data to them. So, then she just figured that she could just do it herself. So, she became independent.”—FG1_4 |
| Theme | Illustrative Quotes |
|---|---|
| Improved communications | |
| Subtheme 1. Telephone support | “One time I was calling for something… I thought it was our analyst number, and it said, ‘I’m not available if you need help call this person, this person’… I call those numbers and it said, ‘If this is an emergency and you need an answer right away, call this person.’ It kept giving me phone numbers. And I was like, ‘Wow!’”—FG1_4 |
| “If there’s an open helpline where somebody could just answer a phone call to answer a simple question that we have, when we’re either filling out a paper for paperwork or whatnot, on the regulations and procedures, I think that would really help.”—FG1_9 | |
| “I think for us, a lot of things have to do with you can’t call them and talk to them. Everything is via email… it’s a lot of back-and-forth emails, and then there’s really no support over the phone.”—FG2_1 | |
| Subtheme 2. Networks and resource sharing | “Maybe have quarterly meetings with all of us. Because we’re all experiencing many similar things…So with the CACFP, that would be very helpful [for them to] regionalize. Even if we were all to get on a Zoom meeting together and [say], “You are region one, you are region two, you are region three,” and we all would have one liaison or analysts that we can go to for technical and training assistance… There are so many divisions and arms under CDSS. So, if the CDSS CACFP had its own website… and update the listserv.”—FG3_1 |
| “I was fortunate enough to be on a coalition…it pulled a whole bunch of us together to say, ‘Who are we missing? How can we reach the people that aren’t participating? And can we develop them into their own sponsors?’… I would love to see that for California, to know who else is out there. Or maybe we do Northern California and Southern California, we can split it up. But I think that’s great, because if nothing else, know that you’re not alone… So, anything where you can interact with the state and other organizations that are involved”—FG3_4 | |
| Subtheme 3. Website improvements | “The website could be better. It’s just not as user friendly as I’d like.”—FG1_2 |
| “I think a chat option [on the website] would be kind of nice.”—FG1_4 | |
| Additional and improved training | “I do appreciate that they have a lot of stuff on YouTube for the CACFP and different little things that I have watched…. but having some in-person training. There’s nothing like it, then having somebody to actually converse with.”—FG1_8 |
| “Because my director had she not had experience at our previous school, I probably would have not kept moving forward with it [the CACFP]. Because it would seem so daunting. And there was just nobody to really… nobody could explain it to me. I feel like some of the trainings I took were not helpful in the administration of the program. It was like, ‘Great, I’m learning about portions and nutrition.’ But it didn’t really break down a lot of the administrative stuff that I had to do.”—FG1_11 | |
| “If there were common questions that a lot of people have that maybe they can do like a video on a step-by-step or go over that and then we’re not having to read a huge book.”—FG2_5 | |
| “In the beginning [when initially participating in the CACFP] more hands-on training…”—FG1_9` | |
| “If the state [CDSS] could maybe develop some kind of a video or webinar, a walk-through orientation…”—FG3_1 | |
| “It’s hard to effectively run the programs, when the changes that are being made, there’s no training.”—FG3_2 | |
| Nutrition standards support | “The recipes, all the emails, I read them all… We get a lot of information to be able to continue to be effective, and in a meal planning, and keeping the kids having different recipes, healthy ways to prepare the food. Everything you guys send is very, very helpful…everything’s online, the Food Buying Guide, all those things that are online, those resources are really very good. Because they’re on our computers. It’s not a big book anymore that we have to handle. Those resources are great.”—FG1_4 |
| “Their [the state agency’s] explanation…is difficult to translate from what they’re saying to what you’re actually reading in the grocery store… examples of menus. I feel like I have no understanding when I go into their website of how to make sure that they’re getting the right amount…”—FG1_3 | |
| “It would be extremely helpful to get a sample menu or a couple of different meal suggestions on not only what they’re [the USDA] changing, but also a balance of the other components of a meal in terms of what they see as being a really healthy balance. And even some menu suggestions.”—FG2_3 | |
| Online forms | “I wish [the enrollment forms] could be more electronic. …being able to have [the things that we have to submit monthly] on a digital platform and we can fill that information out and just as many forms as possible over into the digital world than paper would be great.”—FG1_8 |
| “The [form] that lists the children’s names and their eligibility like free reduced, what have you, that would be great if we could, that can be like saved in the program somewhere… As of right now I go through, I type in everyone’s name. And then the next month, if I add anyone, I have to type a whole new one. It would be nice if there was like an electronic way to have that in there that made it simpler to add and delete children, and then print that out for each month.”—FG1_9 | |
| “If there was some type of app that [parents] could just fill out from their phone with the paperwork that might be easier.”—FG2_7 | |
| Administrative review assistance | “I think the best technical assistance we get is during the audits [administrative reviews] … They also provide us with really important information that every auditor [reviewer] has given different perspectives on different things and they’ve all enhanced how we were able to perform for the next audit [review].”—FG1_1 |
| “…when I first got audited [reviewed], how to better prepare somebody for that.”—B6 | |
| “I think it would be very helpful that we get the instrument that says, ‘Here’s what the Administrative Review [is], here’s all the documents, here’s your evidence, and so on and so forth.’”—FG3_1 | |
| “…training before the Administrative Review.”—FG3_1 | |
| Reduced and streamlined paperwork | “…be able to continue streamlining services so that it’s not new methods. There’s so much that always changes and that were responsible for. So, trying to keep it streamlined… just making it a little more user friendly…. making it quicker and a little easier for us, because we have a lot on our plate.”—FG2_3 |
| “…with our CACFP, the child care enrollment… all the things that we have to look at, at the center, in order to sponsor them. Because they’re now under CDSS. If that information is approved for CDSS, we shouldn’t have to go back and double check and triple check… CDE would ask us to verify enrollment for each child [for CDSS child care licensing]. It seems like we have to do now two extra steps for the daycare center just to be sure that they qualify for the CACFP when they already qualified for the CACFP. But then we have to now do an extra step to go through their records, to see that we have everything we need. And I think if they’re already under CDSS, I don’t see why we should have to do the extra step.”—FG3_2 | |
| “I could go on and on about streamlining services, getting rid of half the paperwork that exists.”—FG3_4 | |
| Supportive relationships with state agency | “…having some field visits, not so much of a compliance, regulatory, “I got you”, but rather, “Wow, this is a great job, this is right, you’re on the right track.” And then providing links directly and resources for those centers.”—FG3_1 |
| “It would be very helpful if information came to us not in the way of “Here’s what you did wrong.” But to prevent us from doing something the wrong way, or in a non-compliant way, because it’s not intentional.”—FG3_2 | |
| “I really had a good relationship with several of them [state agency analysts], and I felt like I could call and get a good answer, and I could get the support I needed… it’s the unknown right now of what it’s going to look like as we move forward… it’s just building up those relationships again… instead of getting my hand slapped. If it was just, ‘I just want to come and see you and see how you’re doing and see how I can help you.’ Rather than the ‘No, no, no.’… I think there’s also the whole image, like a marketing image. So, people aren’t so frightened to participate [in the CACFP], that they will get their hand slapped. I think that more partnership with the Food Program, the USDA and the state of California wants us to feed children, and we all want children to be healthy, and developmentally capable, and all these other things, so that they can learn and grow and be healthy, and productive members of society.”—FG3_4 | |
| “…leading with a softer approach and understanding. Not necessarily coming in and wielding a sword is the best option. The state agency probably needs to support the sponsors more because we have the ability to be more involved [with centers] than the state agency can.”—FG3_5 | |
| Outsourced cooking options | “I know that some places do the food delivery through a centralized kitchen…I would love to do that…would be so much easier to just outsource it. And I don’t know how to do that.”—FG1_1 |
| Increasing the reimbursement | “Give more money toward it!”—FG1_6 |
| “More money coming towards, what we get back, what we get.”—FG1_7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.L.; Homel Vitale, E.; Marshall, S.K.-D.; Hecht, C.; Beck, L.T.; Ritchie, L.D. Child and Adult Care Food Program Participation Benefits, Barriers and Facilitators for Independent Child Care Centers in California. Nutrients 2022, 14, 4449. https://doi.org/10.3390/nu14214449
Lee DL, Homel Vitale E, Marshall SK-D, Hecht C, Beck LT, Ritchie LD. Child and Adult Care Food Program Participation Benefits, Barriers and Facilitators for Independent Child Care Centers in California. Nutrients. 2022; 14(21):4449. https://doi.org/10.3390/nu14214449
Chicago/Turabian StyleLee, Danielle L., Elyse Homel Vitale, Samantha Kay-Daleiden Marshall, Christina Hecht, Lindsay T. Beck, and Lorrene D. Ritchie. 2022. "Child and Adult Care Food Program Participation Benefits, Barriers and Facilitators for Independent Child Care Centers in California" Nutrients 14, no. 21: 4449. https://doi.org/10.3390/nu14214449