
Shared Odds of Borrelia and Rabies Virus Exposure in Serbia

 ,
,  ,
,  , ,
, ,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Design and Sampling Strategy
2.3. Selection of Samples in PEP and PrEP Groups
2.4. Selection of Healthy Blood Donor Samples
2.5. Borrelia Culture and IFAT Antigen Preparation
2.6. Detection of Anti-Borrelia Antibodies by IFAT
2.7. Data Analysis
3. Results
3.1. Association between Borrelia Seroprevalence and Risk of Rabies Exposure
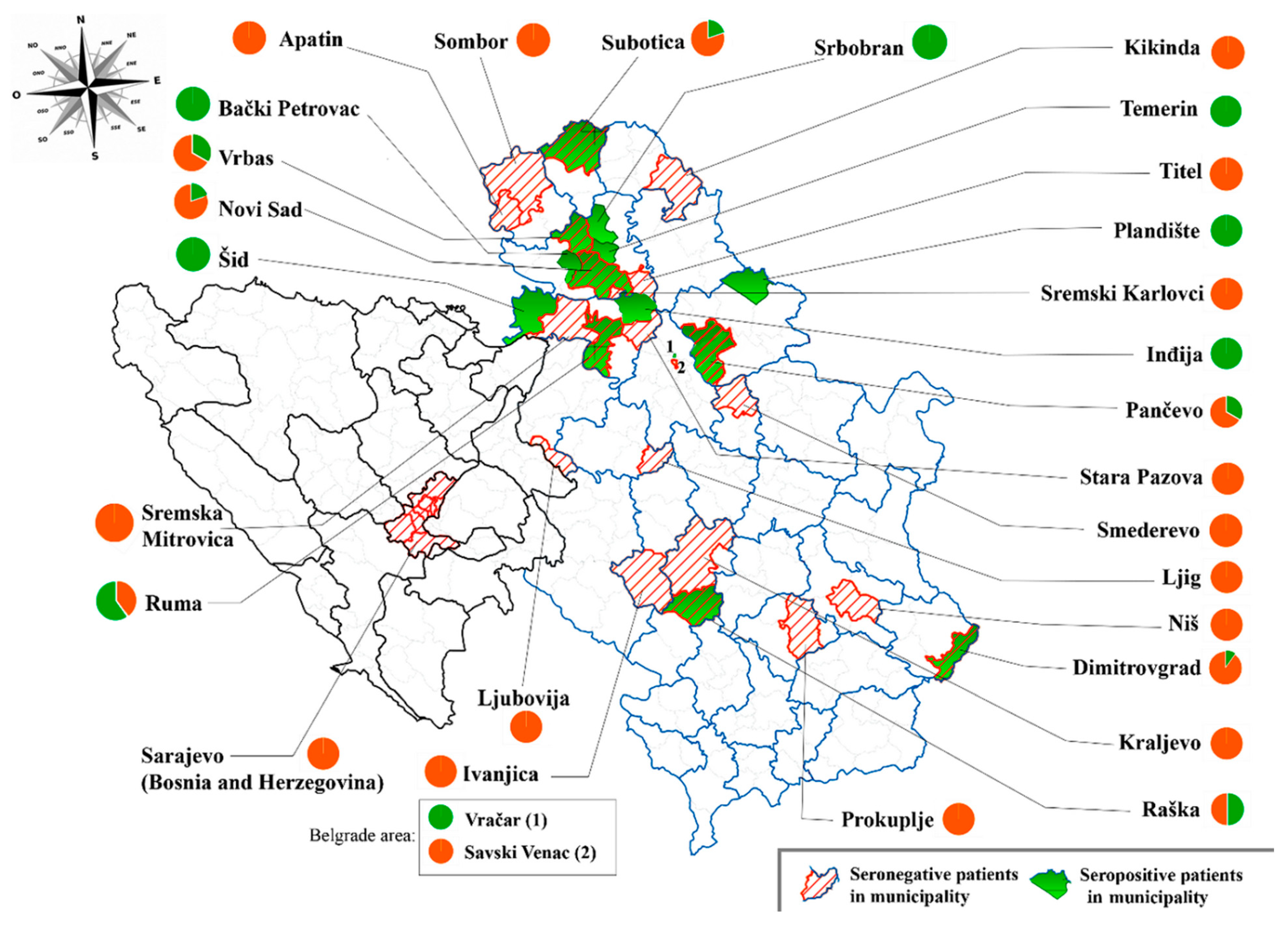
3.2. Association between Regional Distribution of Borrelia spp. Seroprevalence and Rabies Virus Exposure Risk
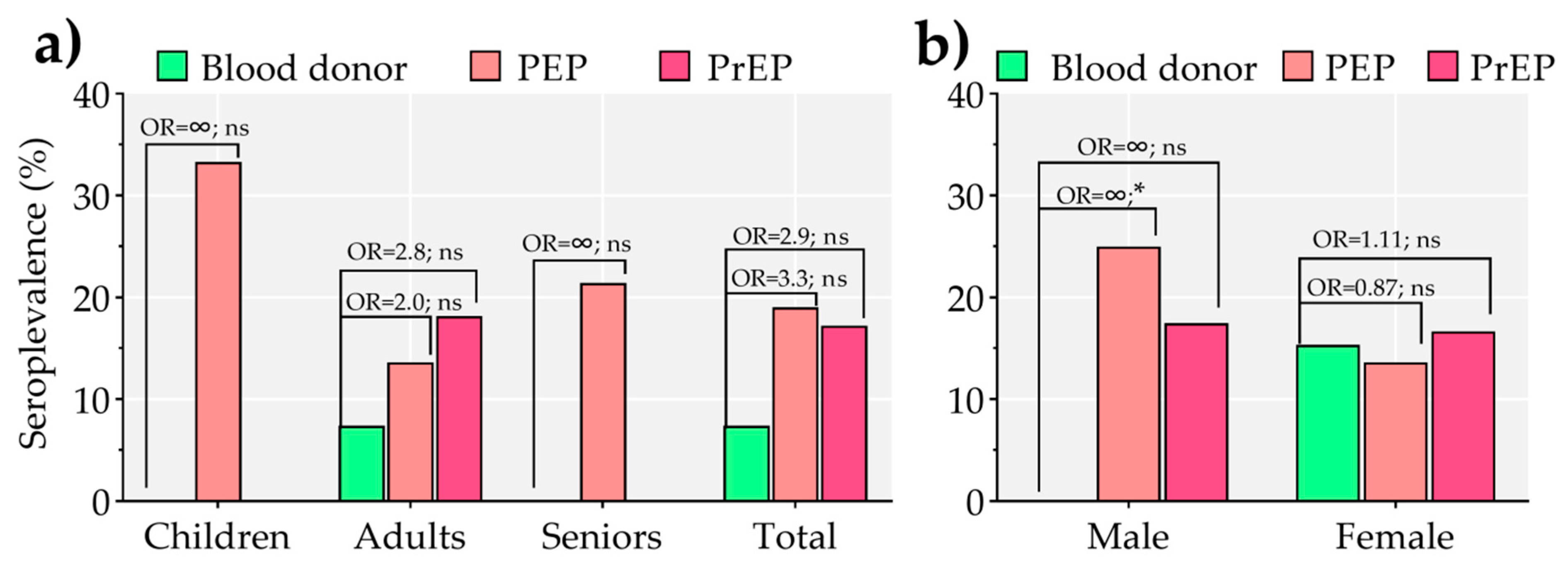
3.3. Association between Borrelia spp. Seroprevalence and Rabies Virus Exposure Risk According to Age and Gender
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Madison-Antenucci, S.; Kramer, L.D.; Gebhardt, L.L.; Kauffman, E. Emerging Tick-Borne Diseases. Clin. Microbiol. Rev. 2020, 33, e00083-18. [Google Scholar] [CrossRef] [PubMed]
- Mysterud, A.; Jore, S.; Østerås, O.; Viljugrein, H. Emergence of Tick-Borne Diseases at Northern Latitudes in Europe: A Comparative Approach. Sci. Rep. 2017, 7, 16316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medlock, J.M.; Hansford, K.M.; Bormane, A.; Derdakova, M.; Estrada-Peña, A.; George, J.-C.; Golovljova, I.; Jaenson, T.G.T.; Jensen, J.-K.; Jensen, P.M.; et al. Driving Forces for Changes in Geographical Distribution of Ixodes Ricinus Ticks in Europe. Parasites Vectors 2013, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehrmann, S.; Liira, J.; Gärtner, S.; Hansen, K.; Brunet, J.; Cousins, S.A.O.; Deconchat, M.; Decocq, G.; De Frenne, P.; De Smedt, P.; et al. Environmental Drivers of Ixodes Ricinus Abundance in Forest Fragments of Rural European Landscapes. BMC Ecol. 2017, 17, 31. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fons, F.; Fernández-de-Mera, I.G.; Acevedo, P.; Gortázar, C.; de la Fuente, J. Factors Driving the Abundance of Ixodes Ricinus Ticks and the Prevalence of Zoonotic I. Ricinus-Borne Pathogens in Natural Foci. Appl. Environ. Microbiol. 2012, 78, 2669–2676. [Google Scholar] [CrossRef] [Green Version]
- Gray, J.S. The Ecology of Ticks Transmitting Lyme Borreliosis. Exp. Appl. Acarol. 1998, 22, 249–258. [Google Scholar] [CrossRef]
- Gryczyńska, A.; Zgódka, A.; Płoski, R.; Siemiatkowski, M. Borrelia Burgdorferi Sensu Lato Infection in Passerine Birds from the Mazurian Lake Region (Northeastern Poland). Avian Pathol. 2004, 33, 69–75. [Google Scholar] [CrossRef]
- Azagi, T.; Hoornstra, D.; Kremer, K.; Hovius, J.W.R.; Sprong, H. Evaluation of Disease Causality of Rare Ixodes Ricinus-Borne Infections in Europe. Pathogens 2020, 9, 150. [Google Scholar] [CrossRef] [Green Version]
- Rizzoli, A.; Silaghi, C.; Obiegala, A.; Rudolf, I.; Hubálek, Z.; Földvári, G.; Plantard, O.; Vayssier-Taussat, M.; Bonnet, S.; Spitalská, E.; et al. Ixodes Ricinus and Its Transmitted Pathogens in Urban and Peri-Urban Areas in Europe: New Hazards and Relevance for Public Health. Front. Public Health 2014, 2, 251. [Google Scholar] [CrossRef]
- Sykes, R.A.; Makiello, P. An Estimate of Lyme Borreliosis Incidence in Western Europe†. J. Public Health 2017, 39, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Rudenko, N.; Golovchenko, M.; Grubhoffer, L.; Oliver, J.H. Updates on Borrelia Burgdorferi Sensu Lato Complex with Respect to Public Health. Ticks Tick-Borne Dis. 2011, 2, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Banović, P.; Čapo, I.; Ogorelica, D.; Vranješ, N.; Simin, V.; Lalošević, D. Mysterious Path of Borrelia Spielmanii: Spreading without Morphological Alteration of Collagen Type I and IV. Future Microbiol. 2019, 14, 1469–1475. [Google Scholar] [CrossRef]
- Steere, A.C.; Strle, F.; Wormser, G.P.; Hu, L.T.; Branda, J.A.; Hovius, J.W.R.; Li, X.; Mead, P.S. Lyme Borreliosis. Nat. Rev. Dis. Primers 2016, 2, 16090. [Google Scholar] [CrossRef] [PubMed]
- Potkonjak, A.; Savić, S.; Ruzić-Sabljić, E.; Vračar, V.; Lako, B.; Jurišić, A.; Petrović, A.; Rajković, D. Molecular Characterization of Borrelia Strains Isolated from Ticks in Vojvodina. Parasites Vectors 2014, 7, P18. [Google Scholar] [CrossRef] [Green Version]
- Savić, S.; Vidić, B.; Lazić, S.; Lako, B.; Potkonjak, A.; Lepšanović, Z. Borrelia Burgdorferi in Ticks and Dogs in the Province of Vojvodina, Serbia. Parasite 2010, 17, 357–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potkonjak, A.; Petrović, T.; Ristanović, E.; Lalić, I.; Vračar, V.; Savić, S.; Turkulov, V.; Čanak, G.; Milošević, V.; Vidanović, D.; et al. Molecular Detection and Serological Evidence of Tick-Borne Encephalitis Virus in Serbia. Vector-Borne Zoonotic Dis. 2017, 17, 813–820. [Google Scholar] [CrossRef]
- Jovanovic, D.; Atanasievska, S.; Protic-Djokic, V.; Rakic, U.; Lukac-Radoncic, E.; Ristanovic, E. Seroprevalence of Borrelia Burgdorferi in Occupationally Exposed Persons in the Belgrade Area, Serbia. Braz. J. Microbiol. Publ. Braz. Soc. Microbiol. 2015, 46, 807–814. [Google Scholar] [CrossRef] [Green Version]
- Tomanović, S.; Radulović, Ž.; Masuzawa, T.; Milutinović, M. Coexistence of Emerging Bacterial Pathogens in Ixodes Ricinus Ticks in Serbia. Parasite 2010, 17, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Banović, P.; Díaz-Sánchez, A.A.; Galon, C.; Simin, V.; Mijatović, D.; Obregón, D.; Moutailler, S.; Cabezas-Cruz, A. Humans Infested with Ixodes Ricinus Are Exposed to a Diverse Array of Tick-Borne Pathogens in Serbia. Ticks Tick-Borne Dis. 2020, 12, 101609. [Google Scholar] [CrossRef]
- Walker, P.J.; Blasdell, K.R.; Calisher, C.H.; Dietzgen, R.G.; Kondo, H.; Kurath, G.; Longdon, B.; Stone, D.M.; Tesh, R.B.; Tordo, N.; et al. ICTV Virus Taxonomy Profile: Rhabdoviridae. J. Gen. Virol. 2018, 99, 447–448. [Google Scholar] [CrossRef]
- World Health Organisation. WHO Expert Consultation on Rabies: Third Report; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-121021-8. [Google Scholar]
- Picot, V.; Rasuli, A.; Abella-Rider, A.; Saadatian-Elahi, M.; Aikimbayev, A.; Barkia, A.; Benmaiz, S.; Bouslama, Z.; De Balogh, K.; Dehove, A.; et al. The Middle East and Eastern Europe Rabies Expert Bureau (MEEREB) Third Meeting: Lyon-France (7–8 April 2015). J. Infect. Public Health 2017, 10, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Pattanaik, A.; Mani, R.S. WHO’s New Rabies Recommendations: Implications for High Incidence Countries. Curr. Opin. Infect. Dis. 2019, 32, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Taylor, E.; Del Rio Vilas, V.; Scott, T.; Coetzer, A.; Prada, J.M.; Alireza, G.; Alqadi, N.A.; Berry, A.; Bazzal, B.; Barkia, A.; et al. Rabies in the Middle East, Eastern Europe, Central Asia, North Africa: Building. J. Infect. Public Health 2021, in press. [Google Scholar] [CrossRef]
- Barbour, A.G. Isolation and Cultivation of Lyme Disease Spirochetes. Yale J. Biol. Med. 1984, 57, 521–525. [Google Scholar]
- OIE. Manual of Diagnostic Tests and Vaccines for Terrestrial Animals (Mammals, Birds and Bees), 6th ed.; OIE—World Organisation for Animal Health: Paris, France, 2008; ISBN 978-92-9044-718-4. [Google Scholar]
- Poljak, I.; Troselj-Vukić, B.; Miletić, B.; Morović, M.; Ruzić-Sabljić, E.; Vucemilović, A.; Materljan, E. Low Sero-Prevalence of Lyme Borreliosis in the Forested Mountainous Area of Gorski Kotar, Croatia. Croat. Med. J. 2000, 41, 433–436. [Google Scholar] [PubMed]
- De Keukeleire, M.; Vanwambeke, S.O.; Somassè, E.; Kabamba, B.; Luyasu, V.; Robert, A. Scouts, Forests, and Ticks: Impact of Landscapes on Human-Tick Contacts. Ticks Tick-Borne Dis. 2015, 6, 636–644. [Google Scholar] [CrossRef] [PubMed]
- De Keukeleire, M.; Robert, A.; Kabamba, B.; Dion, E.; Luyasu, V.; Vanwambeke, S.O. Individual and Environmental Factors Associated with the Seroprevalence of Borrelia Burgdorferi in Belgian Farmers and Veterinarians. Infect. Ecol. Epidemiol. 2016, 6, 32793. [Google Scholar] [CrossRef] [PubMed]
- Tomao, P.; Ciceroni, L.; D’Ovidio, M.C.; De Rosa, M.; Vonesch, N.; Iavicoli, S.; Signorini, S.; Ciarrocchi, S.; Ciufolini, M.G.; Fiorentini, C.; et al. Prevalence and Incidence of Antibodies to Borrelia Burgdorferi and to Tick-Borne Encephalitis Virus in Agricultural and Forestry Workers from Tuscany, Italy. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2005, 24, 457–463. [Google Scholar] [CrossRef]
- Kalish, R.A.; McHugh, G.; Granquist, J.; Shea, B.; Ruthazer, R.; Steere, A.C. Persistence of Immunoglobulin M or Immunoglobulin G Antibody Responses to Borrelia Burgdorferi 10-20 Years after Active Lyme Disease. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2001, 33, 780–785. [Google Scholar] [CrossRef] [Green Version]
- Borchers, A.T.; Keen, C.L.; Huntley, A.C.; Gershwin, M.E. Lyme Disease: A Rigorous Review of Diagnostic Criteria and Treatment. J. Autoimmun. 2015, 57, 82–115. [Google Scholar] [CrossRef]
- Krstic, M.; Stajkovic, N. Risk for infection by Lyme disease cause in green surfaces maintenance workers in Belgrade. Vojnosanit. Pregl. 2007, 64, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Rojko, T.; Ružić-Sabljić, E.; Strle, F.; Lotrič-Furlan, S. Prevalence and Incidence of Lyme Borreliosis among Slovene Forestry Workers during the Period of Tick Activity. Wien. Klin. Wochenschr. 2005, 117, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Lambin, E.F.; Tran, A.; Vanwambeke, S.O.; Linard, C.; Soti, V. Pathogenic Landscapes: Interactions between Land, People, Disease Vectors, and Their Animal Hosts. Int. J. Health Geogr. 2010, 9, 54. [Google Scholar] [CrossRef] [Green Version]
- Burek, V.; Mišić-mayerus, L.; Maretic, T. Antibodies to Borrelia Burgdorferi in Various Population Groups in Croatia. Scand. J. Infect. Dis. 1992, 24, 683–684. [Google Scholar] [CrossRef]
- Zöldi, V.; Juhász, A.; Nagy, C.; Papp, Z.; Egyed, L. Tick-Borne Encephalitis and Lyme Disease in Hungary: The Epidemiological Situation Between 1998 and 2008. Vector-Borne Zoonotic Dis. 2013, 13, 256–265. [Google Scholar] [CrossRef]
- Hristea, A.; Hristescu, S.; Ciufecu, C.; Vasile, A. Seroprevalence of Borrelia Burgdorferi in Romania. Eur. J. Epidemiol. 2001, 17, 891–896. [Google Scholar] [CrossRef]
- Hrnjaković Cvjetković, I.; Petrović, T.; Petrić, D.; Cvjetković, D.; Kovačević, G.; Radovanov, J.; Jovanović Galović, A.; Pat, A.; Nikolić, N.; Stefan Mikić, S.; et al. Seroprevalence of Mosquito-Born and Tick-Born Microorganisms in Human Population of South Bačka District. Arch. Veter Med. 2016, 9, 23–30. [Google Scholar] [CrossRef]
- Lakos, A.; Igari, Z.; Solymosi, N. Recent Lesson from a Clinical and Seroepidemiological Survey: Low Positive Predictive Value of Borrelia Burgdorferi Antibody Testing in a High Risk Population. Adv. Med. Sci. 2012, 57, 356–363. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Groups | Rabies Virus Exposure Risk | Anti-Borrelia IgG Detection | Borrelia spp. Seroprevalence (%) | CI (95%) | |
|---|---|---|---|---|---|
| Negative | Positive | ||||
| Healthy donors | No | 28 | 2 | 6.67 | 1.16–23.51 |
| “Post-exposure protocol” (PEP) | Yes | 34 | 8 | 19.05 | 9.14–34.63 |
| “Pre-exposure protocol” (PrEP) | Yes | 48 | 10 | 17.24 | 9.00–29.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banović, P.; Díaz-Sánchez, A.A.; Mijatović, D.; Vujin, D.; Horváth, Z.; Vranješ, N.; Budakov-Obradović, Z.; Bujandrić, N.; Grujić, J.; Ghafar, A.; et al. Shared Odds of Borrelia and Rabies Virus Exposure in Serbia. Pathogens 2021, 10, 399. https://doi.org/10.3390/pathogens10040399
Banović P, Díaz-Sánchez AA, Mijatović D, Vujin D, Horváth Z, Vranješ N, Budakov-Obradović Z, Bujandrić N, Grujić J, Ghafar A, et al. Shared Odds of Borrelia and Rabies Virus Exposure in Serbia. Pathogens. 2021; 10(4):399. https://doi.org/10.3390/pathogens10040399
Chicago/Turabian StyleBanović, Pavle, Adrian Alberto Díaz-Sánchez, Dragana Mijatović, Dragana Vujin, Zsolt Horváth, Nenad Vranješ, Zorana Budakov-Obradović, Nevenka Bujandrić, Jasmina Grujić, Abdul Ghafar, and et al. 2021. "Shared Odds of Borrelia and Rabies Virus Exposure in Serbia" Pathogens 10, no. 4: 399. https://doi.org/10.3390/pathogens10040399