
Pharmacokinetic Drug Interaction Study of Sorafenib and Morphine in Rats

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Reagents
2.3. HPLC-UV Assay of Sorafenib and SR_NO
2.4. UPLC-MS/MS Assay of Morphine and M3G
2.5. Pharmacokinetic Evaluation
2.6. Statistical Analysis
3. Results
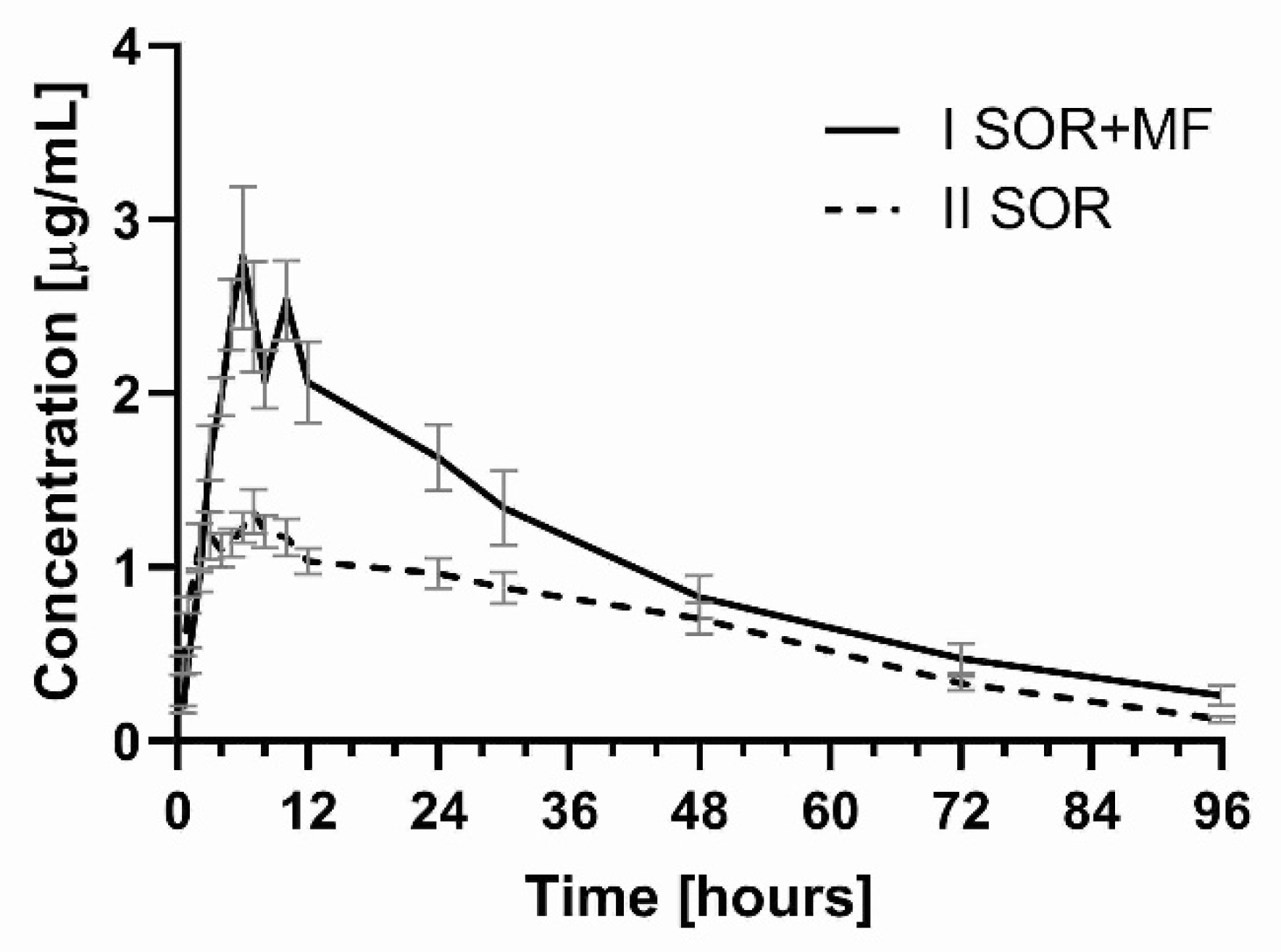
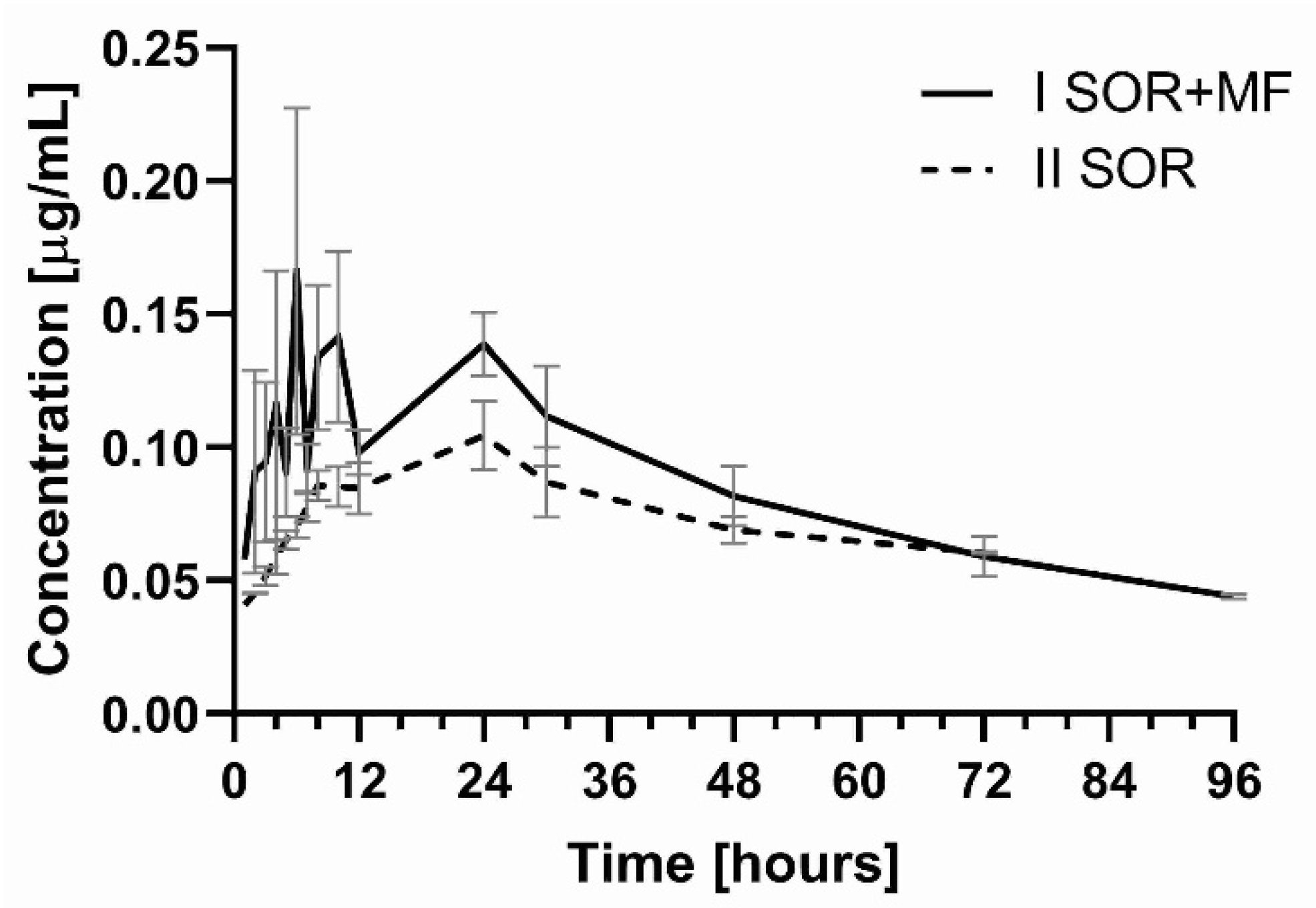
3.1. The Influence of Morphine on the Pharmacokinetics of Sorafenib and SR_NO
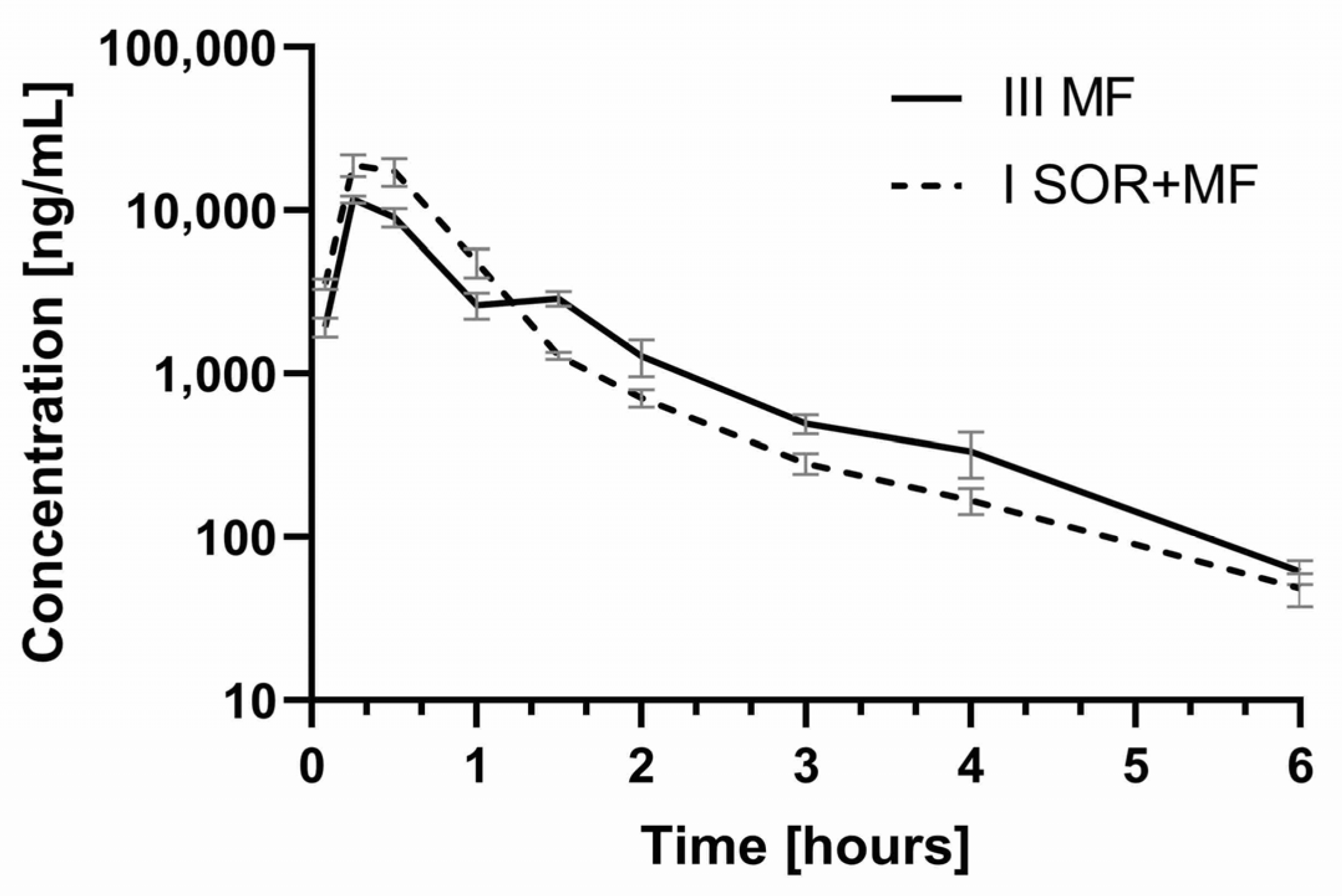
3.2. The Influence of Sorafenib on the Pharmacokinetics of Morphine and M3G
4. Discussion
4.1. The Influence of Morphine on the Pharmacokinetics of Sorafenib and SR_NO
4.2. The Influence of Sorafenib on the Pharmacokinetics of Morphine and M3G
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gress, K.L.; Charipova, K.; Kaye, A.D.; Viswanath, O.; Urits, I. An Overview of Current Recommendations and Options for the Management of Cancer Pain: A Comprehensive Review. Oncol. Ther. 2020, 8, 251–259. [Google Scholar] [CrossRef]
- Karbownik, A.; Miedziaszczyk, M.; Grabowski, T.; Stanisławiak-Rudowicz, J.; Jaźwiec, R.; Wolc, A.; Grześkowiak, E.; Szałek, E. In vivo assessment of potential for UGT-inhibition-based drug-drug interaction between sorafenib and tapentadol. Biomed. Pharmacother. 2020, 130, 110530. [Google Scholar] [CrossRef]
- Gong, L.; Giacomini, M.M.; Giacomini, C.; Maitland, M.L.; Altman, R.B.; Klein, T.E. PharmGKB summary: Sorafenib pathways. Pharm. Genom. 2017, 27, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Bertot, L.C.; Adams, L.A. Trends in hepatocellular carcinoma due to non-alcoholic fatty liver disease. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, J.J.; Purdue, M.P.; Signoretti, S.; Swanton, C.; Albiges, L.; Schmidinger, M.; Heng, D.Y.; Larkin, J.; Ficarra, V. Renal cell carcinoma. Nat. Rev. Dis. Primers 2017, 3, 17009. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; McFadden, D.G.; Durante, C. Thyroid cancer. Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef]
- Miners, J.O.; Chau, N.; Rowland, A.; Burns, K.; MnKinnon, R.A.; Mackenzie, P.I.; Tucker, G.T.; Knights, K.M.; Kichenadasse, G. Inhibition of human UDP-glucuronosyltransferase enzymes by lapatinib, pazopanib, regorafenib and sorafenib: Implications for hyperbilirubinemia. Biochem. Pharmacol. 2017, 129, 85–95. [Google Scholar] [CrossRef]
- Chen, M.; Neul, C.; Schaeffeler, E.; Frisch, F.; Winter, S.; Schwab, M.; Koepsell, H.; Hu, S.; Laufer, S.; Baker, S.D.; et al. Sorafenib activity and disposition in liver cancer does not depend on organic cation transporter 1. Clin. Pharmacol. Ther. 2020, 107, 227–237. [Google Scholar] [CrossRef]
- Vasilyeva, A.; Durmus, S.; Li, L.; Wagenaar, E.; Hu, S.; Gibson, A.A.; Panetta, J.C.; Mani, S.; Sparreboom, A.; Baker, S.D.; et al. Hepatocellular shuttling and recirculation of sorafenib-glucuronide is dependent on Abcc2, Abcc3, and Oatp1a/1b. Cancer Res. 2015, 75, 2729–2736. [Google Scholar] [CrossRef] [Green Version]
- Summary of Product Characteristic for Nexavar 200 mg, European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/product-information/nexavar-epar-product-information_en.pdf (accessed on 6 April 2021).
- Karbownik, A.; Stachowiak, A.; Urjasz, H.; Sobańska, K.; Szczecińska, A.; Grabowski, T.; Stanisławiak-Rudowicz, J.; Wolc, A.; Grześkowiak, E.; Szałek, E. The oxidation and hypoglycaemic effect of sorafenib in streptozotocin-induced diabetic rats. Pharmacol. Rep. 2020, 72, 254–259. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, X.; Huang, X.; Li, Y.; Wu, M.; Liu, J. The drug-drug interaction of sorafenib mediated by P-glicoprotein and CYP3A4. Xenobiotica 2015, 46, 651–658. [Google Scholar] [CrossRef]
- Kimura, Y.; Shibata, M.; Tamada, M.; Ozaki, N.; Arai, K. Pharmacokinetics of Morphine in Rats with Adjuvant-induced Arthritis. In Vivo 2017, 31, 811–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadeyne, C.; Van der Heyden, S.; Gasthuys, F.; Croubels, S.; Schauvliege, S.; Polis, I. The influence of modulation of P-glycoprotein and/or cytochrome P450 3A on the pharmacokinetics and pharmacodynamics of orally administered morphine in dogs. J. Vet. Pharmacol. Ther. 2011, 34, 417–423. [Google Scholar] [CrossRef]
- De Gregori, S.; De Gregori, M.; Ranzani, G.N.; Allegri, M.; Minella, C.; Regazzi, M. Morphine metabolism, transport and brain disposition. Metab. Brain Dis. 2012, 27, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Ing Lorenzini, K.; Girardin, F. Direct-acting antiviral interactions with opioids, alcohol or illicit drugs of abuse in HCV-infected patients. Liver Int. 2020, 40, 32–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schinkel, A.H.; Wagenaar, E.; van Deemter, L.; Mol, C.A.; Borst, P. Absence of the mdr1a P-Glycoprotein in mice affects tissue distribution and pharmacokinetics of dexamethasone, digoxin, and cyclosporin A. J. Clin. Investig. 1995, 96, 1698–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letrent, S.P.; Polli, J.W.; Humphreys, J.E.; Pollack, G.M.; Brouwer, K.R.; Brouwer, K.L. P-glycoprotein-mediated transport of morphine in brain capillary endothelial cells. Biochem. Pharmacol. 1999, 58, 951–957. [Google Scholar] [CrossRef]
- Crowe, A. The influence of P-glycoprotein on morphine transport in Caco-2 cells. Comparison with paclitaxel. Eur. J. Pharmacol. 2002, 440, 7–16. [Google Scholar] [CrossRef]
- Xie, R.; Hammarlund-Udenaes, M.; de Boer, A.G.; de Lange, E.C. The role of P-glycoprotein in blood-brain barrier transport of morphine: Transcortical microdialysis studies in mdr1a (-/-) and mdr1a (+/+) mice. Br. J. Pharmacol. 1999, 128, 563–568. [Google Scholar] [CrossRef] [Green Version]
- Letrent, S.P.; Pollack, G.M.; Brouwer, K.R.; Brouwer, K.L. Effect of GF120918, a potent P-glycoprotein inhibitor, on morphine pharmacokinetics and pharmacodynamics in the rat. Pharm Res. 1998, 15, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Aquilante, C.L.; Letrent, S.P.; Pollack, G.M.; Brouwer, K.L. Increased brain P-glycoprotein in morphine tolerant rats. Life Sci. 2000, 66, PL47–PL51. [Google Scholar] [CrossRef]
- Fujita-Hamabe, W.; Nishida, M.; Nawa, A.; Kobori, T.; Nakamoto, K.; Kishioka, S.; Tokuyama, S. Etoposide modulates the effects of oral morphine analgesia by targeting the intestinal P-glycoprotein. J. Pharm. Pharmacol. 2012, 64, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Seleman, M.; Chapy, H.; Cisternino, S.; Courtin, C.; Smirnova, M.; Schlatter, J.; Chiadmi, F.; Scherrmann, J.M.; Noble, F.; Marie-Claire, C. Impact of P-glycoprotein at the blood-brain barrier on the uptake of heroin and its main metabolites: Behavioral effects and consequences on the transcriptional responses and reinforcing properties. Psychopharmacology 2014, 231, 3139–3149. [Google Scholar] [CrossRef] [PubMed]
- Zong, J.; Pollack, G.M. Morphine antinociception is enhanced in mdr1a gene-deficient mice. Pharm. Res. 2000, 17, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Fudin, J.; Fontenelle, D.V.; Payne, A. Rifampin reduces oral morphine absorption: A case of transdermal buprenorphine selection based on morphine pharmacokinetics. J. Pain Palliat. Care Pharmacother. 2012, 26, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cai, B.; Huang, D.X.; Yang, S.D.; Guo, L. Decreased analgesic effect of morphine, but not buprenorphine, in patients with advanced P-glycoprotein(+) cancers. Pharmacol. Rep. 2012, 64, 870–877. [Google Scholar] [CrossRef]
- Meissner, K.; Avram, M.J.; Yermolenka, V.; Francis, A.M.; Blood, J.; Kharasch, E.D. Cyclosporine-inhibitable blood-brain barrier drug transport influences clinical morphine pharmacodynamics. Anesthesiology 2013, 119, 941–953. [Google Scholar] [CrossRef] [Green Version]
- Drewe, J.; Ball, H.A.; Beglinger, C.; Peng, B.; Kemmler, A.; Schächinger, H.; Haefeli, W.E. Effect of P-glycoprotein modulation on the clinical pharmacokinetics and adverse effects of morphine. Br. J. Clin. Pharmacol. 2000, 50, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Lötsch, J.; Schmidt, R.; Vetter, G.; Schmidt, H.; Niederberger, E.; Geisslinger, G.; Tegeder, I. Increased CNS uptake and enhanced antinociception of morphine-6-glucuronide in rats after inhibition of P-glycoprotein. J. Neurochem. 2002, 83, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Gharavi, R.; Hedrich, W.; Wang, H.; Hassan, H.E. Transporter-Mediated Disposition of Opioids: Implications for Clinical Drug Interactions. Pharm. Res. 2015, 32, 2477–2502. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.J.; Koszdin, K.; Bernards, C.M. Opiate-induced analgesia is increased and prolonged in mice lacking P-glycoprotein. Anesthesiology 2000, 92, 1392–1399. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, C.; Zong, J.; Ducharme, J.; Pollack, G.M. Effect of mdr1a P-glycoprotein gene disruption, gender, and substrate concentration on brain uptake of selected compounds. Pharm. Res. 2001, 18, 957–963. [Google Scholar] [CrossRef]
- Hamabe, W.; Maeda, T.; Kiguchi, N.; Yamamoto, C.; Tokuyama, S.; Kishioka, S. Negative relationship between morphine analgesia and P-glycoprotein expression levels in the brain. J. Pharmacol. Sci. 2007, 105, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Fudin, J.; Fontenelle, D.V.; Fudin, H.R.; Carlyn, C.; Hinden, D.A.; Ashley, C.C. Potential P-glycoprotein pharmacokinetic interaction of telaprevir with morphine or methadone. J. Pain Palliat. Care Pharmacother. 2013, 27, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Tournier, N.; Declèves, X.; Saubaméa, B.; Scherrmann, J.M.; Cisternino, S. Opioid transport by ATP-binding cassette transporters at the blood-brain barrier: Implications for neuropsychopharmacology. Curr. Pharm. Des. 2011, 17, 2829–2842. [Google Scholar] [CrossRef]
- Wandel, C.; Kim, R.; Wood, M.; Wood, A. Interaction of morphine, fentanyl, sufentanil, alfentanil, and loperamide with the efflux drug transporter P-glycoprotein. Anesthesiology 2002, 96, 913–920. [Google Scholar] [CrossRef]
- Tzvetkov, M.V.; dos Santos Pereira, J.N.; Meineke, I.; Saadatmand, A.R.; Stingl, J.C.; Brockmöller, J. Morphine is a substrate of the organic cation transporter OCT1 and polymorphisms in OCT1 gene affect morphine pharmacokinetics after codeine administration. Biochem. Pharmacol. 2013, 86, 666–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatasubramanian, R.; Fukuda, T.; Niu, J.; Mizuno, T.; Chidambaran, V.; Vinks, A.A.; Sadhasivam, S. ABCC3 and OCT1 genotypes influence pharmacokinetics of morphine in children. Pharmacogenomic 2014, 15, 1297–1309. [Google Scholar] [CrossRef] [Green Version]
- Van de Wetering, K.; Zelcer, N.; Kuil, A.; Feddema, W.; Hillebrand, M.; Vlaming, M.L.; Schinkel, A.H.; Beijnen, J.H.; Borst, P. Multidrug resistance proteins 2 and 3 provide alternative routes for hepatic excretion of morphine-glucuronides. Mol. Pharmacol. 2007, 72, 387–394. [Google Scholar] [CrossRef]
- Bourasset, F.; Cisternino, S.; Temsamani, J.; Scherrmann, J.M. Evidence for an active transport of morphine-6-beta-d-glucuronide but not P-glycoprotein-mediated at the blood-brain barrier. J. Neurochem. 2003, 86, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, R.W.F.; Van Gelder, T.; Mathijssen, R.H.J.; Jansman, F.G.A. Drug-drug interactions with tyrosine-kinase inhibitors: A clinical perspective. Lancet Oncol. 2014, 15, 315–326. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, X.; Liu, F.; Wang, M.; Qin, S. The effects of triptolide on the pharmacokinetics of sorafenib in rats and its potential mechanism. Pharm. Biol. 2017, 55, 1863–1867. [Google Scholar] [CrossRef] [Green Version]
- Afify, S.; Rapp, U.R.; Högger, P. Validation of a liquid chromatography assay for the quantification of the Raf kinase inhibitor BAY 43-9006 in small volumes of mouse serum. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2004, 809, 99–103. [Google Scholar] [CrossRef]
- Yu, J.; Petrie, I.D.; Levy, R.H.; Ragueneau-Majlessi, I. Mechanisms and Clinical Significance of Pharmacokinetic-Based Drug-Drug Interactions with Drugs Approved by the U.S. Food and Drug Administration in 2017. Drug Metab. Dispos. 2019, 47, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Y.; Cheng, Z.; Xie, F. Evaluation of Pharmacokinetic Drug-Drug Interactions: A Review of the Mechanisms, In Vitro and In Silico Approaches. Metabolites 2021, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- In Vitro Drug Interaction Studies—Cytochrome P450 Enzyme- and Transporter-Mediated Drug Interactions. Guidance for Industry. U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). January 2020, Clinical Pharmacology. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/vitro-drug-interaction-studies-cytochrome-p450-enzyme-and-transporter-mediated-drug-interactions (accessed on 8 November 2021).
- Cole, S.; Kerwash, E.; Andersson, A. A summary of the current drug interaction guidance from the European Medicines Agency and considerations of future updates. Drug Metab. Pharmacokinet. 2020, 35, 2–11. [Google Scholar] [CrossRef]
- Azam, C.; Claraz, P.; Chevreau, C.; Vinson, C.; Cottura, E.; Mourey, L.; Pouessel, D.; Guibaud, S.; Pollet, O.; Le Goff, M.; et al. Association between clinically relevant toxicities of pazopanib and sunitinib and the use of weak CYP3A4 and P-gp inhibitors. Eur. J. Clin. Pharmacol. 2020, 76, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Oostendorp, R.L.; Buckl, T.; Beijnen, J.H.; van Tellingen, O.; Schellens, J.H. The effect of P-gp (Mdr1a/1b), BCRP (Bcrp1) and P-gp/BCRP inhibitors on the in vivo absorption, distribution, metabolism and excretion of imatinib. Investig. New Drugs 2009, 27, 31–40. [Google Scholar] [CrossRef]
- Teo, Y.L.; Ho, H.K.; Chan, A. Metabolism-related pharmacokinetic drug-drug interactions with tyrosine kinase inhibitors: Current understanding, challenges and recommendations. Br. J. Clin. Pharmacol. 2015, 79, 241–253. [Google Scholar] [CrossRef] [Green Version]
- Campa, D.; Gioia, A.; Tomei, A.; Poli, P.; Barale, R. Association of ABCB1/MDR1 and OPRM1 gene polymorphisms with morphine pain relief. Clin. Pharmacol. Ther. 2008, 83, 559–566. [Google Scholar] [CrossRef]
- Coulbault, L.; Beaussier, M.; Verstuyft, C.; Weickmans, H.; Dubert, L.; Trégouet, D.; Descot, C.; Parc, Y.; Lienhart, A.; Jaillon, P.; et al. Environmental and genetic factors associated with morphine response in the postoperative period. Clin. Pharmacol. Ther. 2006, 79, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, Y.; Kishimoto, S.; Shibatani, N.; Nomura, H.; Ishii, Y.; Onishi, M.; Inotsume, N.; Takeuchi, Y.; Fukushima, S. The pharmacokinetics of morphine and its glucuronide conjugate in a rat model of streptozotocin-induced diabetes and the expression of MRP2, MRP3 and UGT2B1 in the liver. J. Pharm. Pharmacol. 2010, 62, 310–314. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pharmacokinetic Parameters | IISOR (n = 8) | ISOR+MF (n = 8) | p-Value ISOR+MF vs. IISOR | Gmean Ratio * (90% CI) ISOR+MF vs. IISOR |
|---|---|---|---|---|
| sorafenib | ||||
| Cmax (µg/mL) | 1.56 ± 0.35 | 3.25 ± 0.80 | 0.0030 | 2.08 (1.70; 2.55) |
| (22.6) | (24.6) | |||
| Cmax/(D/kg) | 0.03 ± 0.01 | 0.07 ± 0.02 | <0.0001 | 2.13 (1.73; 2.62) |
| (kg × µg/mL/mg) | (23.9) | (23.6) | ||
| AUC0–t | 62.83 ± 16.14 | 97.98 ± 30.17 | 0.0115 | 1.53 (1.16; 2.02) |
| (µg × h/mL) | (25.7) | (30.8) | ||
| AUC0–t/(D/kg) | 1.25 ± 0.32 | 1.99 ± 0.59 | 0.0075 | 1.57 (1.20; 2.05) |
| (µg × h × kg/mL/mg) | (25.4) | (29.7) | ||
| AUC0–∞ (µg × h/mL) | 67.05 ± 16.70 | 109.08 ± 37.18 | 0.0115 | 1.58 (1.17; 2.13) |
| (24.9) | (34.1) | |||
| AUC0–∞/(D/kg) | 1.33 ± 0.33 | 2.21 ± 0.73 | 0.0076 | 1.62 (1.21; 2.16) |
| (µg × h × kg/mL/mg) | (24.9) | (32.9) | ||
| tmax (h) | 5.13 ± 2.17 (42.3) | 7.63 ± 2.72 (35.7) | 0.0616 | 1.54 (1.06; 2.25) |
| ka (h−1) | 0.74 ± 0.31 (42.5) | 0.03 ± 0.01 (20.5) | 0.0008 | 0.03 (0.03; 0.05) |
| kel (h−1) | 0.035 ± 0.01 (30.3) | 0.29 ± 0.16 (53.5) | 0.0008 | 8.16 (5.98; 11.12) |
| t1/2 (h) | 21.89 ± 7.79 (35.6) | 27.31 ± 5.32 (19.5) | 0.0829 | 1.25 (1.02; 1.53) |
| Cl/F (L/h × kg) | 0.80 ± 0.22 (27.1) | 0.51 ± 0.23 (43.8) | 0.0224 | 0.62 (0.46; 0.83) |
| Vd/F (L) | 25.30 ± 11.59 (45.8) | 19.14 ± 5.26 (27.5) | 0.0829 | 0.77 (0.59; 1.01) |
| sorafenib N-oxide | ||||
| Cmax (µg/mL) | 0.11 ± 0.02 (21.8) | 0.27 ± 0.16 (57.5) | 0.0022 | 2.15 (1.50; 3.08) |
| AUC0–t (µg × h/mL) | 4.10 ± 1.56 (38.1) | 6.64 ± 2.44 (36.8) | 0.0268 | 1.64 (1.14; 2.36) |
| AUC0–∞ (µg × h/mL) | 8.61 ± 2.19 (25.4) | 9.39 ± 2.97 (31.6) | 0.1242 | 1.41 (0.95; 2.08) |
| tmax (h) | 16.38 ± 8.21 (50.1) | 14.50 ± 11.40 (78.6) | 0.4531 | 0.76 (0.41; 1.39) |
| kel (h−1) | 0.016 ± 0.010 (60.9) | 0.023 ± 0.012 (51.6) | 0.4001 | 0.80 (0.47; 1.36) |
| t1/2 (h) | 53.31 ± 25.23 (47.3) | 39.30 ± 22.54 (57.4) | 0.4622 | 1.25 (0.73; 2.13) |
| ratio sorafenib N-oxide/sorafenib | ||||
| Cmax (µg/mL) | 0.07 ± 0.02 (26.8) | 0.09 ± 0.07 (76.2) | 0.5280 | 1.03 (0.67; 1.61) |
| AUC0–t (µg × h/mL) | 0.07 ± 0.02 (37.1) | 0.07 ± 0.03 (43.7) | 0.6012 | 1.07 (0.70; 1.65) |
| AUC0–∞ (µg × h/mL) | 0.14 ± 0.05 (38.1) | 0.10 ± 0.07 (64.1) | 0.9176 | 0.89 (0.53; 1.51) |
| Pharmacokinetic Parameters | IIIMF (n = 7) | ISOR+MF (n = 8) | p-Value ISOR+MF vs. IIIMF | Gmean Ratio * (90% CI) ISOR+MF vs. IIIMF |
|---|---|---|---|---|
| morphine | ||||
| Cmax (ng/mL) | 166.83 ± 46.12 | 261.83 ± 47.85 | 0.0018 | 1.59 (1.30; 1.94) |
| (27.6) | (18.3) | |||
| Cmax/(D/kg) | 67.88 ± 18.74 | 106.14 ± 18.96 | 0.0018 | 1.58 (1.30; 1.93) |
| (kg × ng/mL/mg) | (27.6) | (17.9) | ||
| AUC0–t (ng × h/mL) | 169.88 ± 47.37 | 155.40 ± 28.41 | 0.4786 | 0.93 (0.75; 1.16) |
| (27.9) | (18.3) | |||
| AUC0–t/(D/kg) | 69.28 ± 19.99 | 63.06 ± 11.52 | 0.4655 | 0.93 (0.75; 1.16) |
| (ng × h × kg/mL/mg) | (28.9) | (18.3) | ||
| AUC0–∞ (ng × h/mL) | 174.44 ± 46.73 | 162.57 ± 25.89 | 0.5458 | 0.95 (0.78; 1.17) |
| (26.8) | (15.9) | |||
| AUC0–∞/(D/kg) | 71.14 ± 19.75 | 65.96 ± 10.49 | 0.5287 | 0.95 (0.77; 1.17) |
| (ng × h × kg/mL/mg) | (27.8) | (15.9) | ||
| tmax (h) | 0.14 ± 0.16 (110.2) | 0.08 ± 0.00 (0.0) | 0.3559 | 0.77 (0.47; 1.27) |
| kel (h−1) | 0.60 ± 0.18 (29.3) | 0.54 ± 0.41 (76.1) | 0.2976 | 0.75 (0.46; 1.23) |
| t1/2 (h) | 1.22 ± 0.28 (22.7) | 1.91 ± 1.13 (59.3) | 0.2976 | 1.33 (0.82; 2.15) |
| Cl/F (L/h × kg) | 15.05 ± 4.39 (29.2) | 15.51 ± 2.36 (15.2) | 0.8010 | 1.06 (0.86; 1.30) |
| Vd/F (L/kg) | 27.49 ± 13.38 (48.7) | 44.65 ± 29.20 (65.4) | 0.1778 | 1.40 (0.76; 2.60) |
| M3G | ||||
| Cmax (ng/mL) | 9781.28 ± 3184.17 (32.6) | 20,796.81 ± 3657.84,(17.6) | <0.0001 | 2.20 (1.73; 2.80) |
| AUC0–t (ng × h/mL) | 10,035.88 ± 1408.48 (14.0) | 14,734.53 ± 3979.45 (27.0) | 0.0124 | 1.43 (1.14; 1.79) |
| AUC0–∞ (ng × h/mL) | 10,131.53 ± 1393.15 (13.8) | 14,871.32 ± 4001.35 (26.9) | 0.0121 | 1.42 (1.14; 1.79) |
| tmax (h) | 0.46 ± 0.09 (20.4) | 0.34 ± 0.13 (37.6) | 0.0662 | 0.71 (0.53; 0.96) |
| kel (h−1) | 0.73 ± 0.20 (27.6) | 0.68 ± 0.19 (28.0) | 0.6355 | 0.93 (0.69; 1.24) |
| t1/2 (h) | 1.03 ± 0.33 (32.5) | 1.13 ± 0.47 (41.1) | 0.7285 | 1.08 (0.81; 1.45) |
| M3G/morphine | ||||
| Cmax (ng/mL) | 63.87 ± 30.71 (48.1) | 82.18 ± 21.67 (26.4) | 0.2004 | 1.14 (0.78; 1.66) |
| AUC0–t (ng × h/mL) | 64.45 ± 24.06 (37.3) | 97.35 ± 33.05 (34.0) | 0.0488 | 1.38 (0.96; 2.00) |
| AUC0–∞ (ng × h/mL) | 62.88 ± 22.44 (35.7) | 92.80 ± 28.44 (30.7) | 0.0435 | 1.53 (1.10; 2.12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karbownik, A.; Szkutnik-Fiedler, D.; Grabowski, T.; Wolc, A.; Stanisławiak-Rudowicz, J.; Jaźwiec, R.; Grześkowiak, E.; Szałek, E. Pharmacokinetic Drug Interaction Study of Sorafenib and Morphine in Rats. Pharmaceutics 2021, 13, 2172. https://doi.org/10.3390/pharmaceutics13122172
Karbownik A, Szkutnik-Fiedler D, Grabowski T, Wolc A, Stanisławiak-Rudowicz J, Jaźwiec R, Grześkowiak E, Szałek E. Pharmacokinetic Drug Interaction Study of Sorafenib and Morphine in Rats. Pharmaceutics. 2021; 13(12):2172. https://doi.org/10.3390/pharmaceutics13122172
Chicago/Turabian StyleKarbownik, Agnieszka, Danuta Szkutnik-Fiedler, Tomasz Grabowski, Anna Wolc, Joanna Stanisławiak-Rudowicz, Radosław Jaźwiec, Edmund Grześkowiak, and Edyta Szałek. 2021. "Pharmacokinetic Drug Interaction Study of Sorafenib and Morphine in Rats" Pharmaceutics 13, no. 12: 2172. https://doi.org/10.3390/pharmaceutics13122172