Polypharmacy Definitions for Multimorbid Older Adults Need Stronger Foundations to Guide Research, Clinical Practice and Public Health

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants/Population
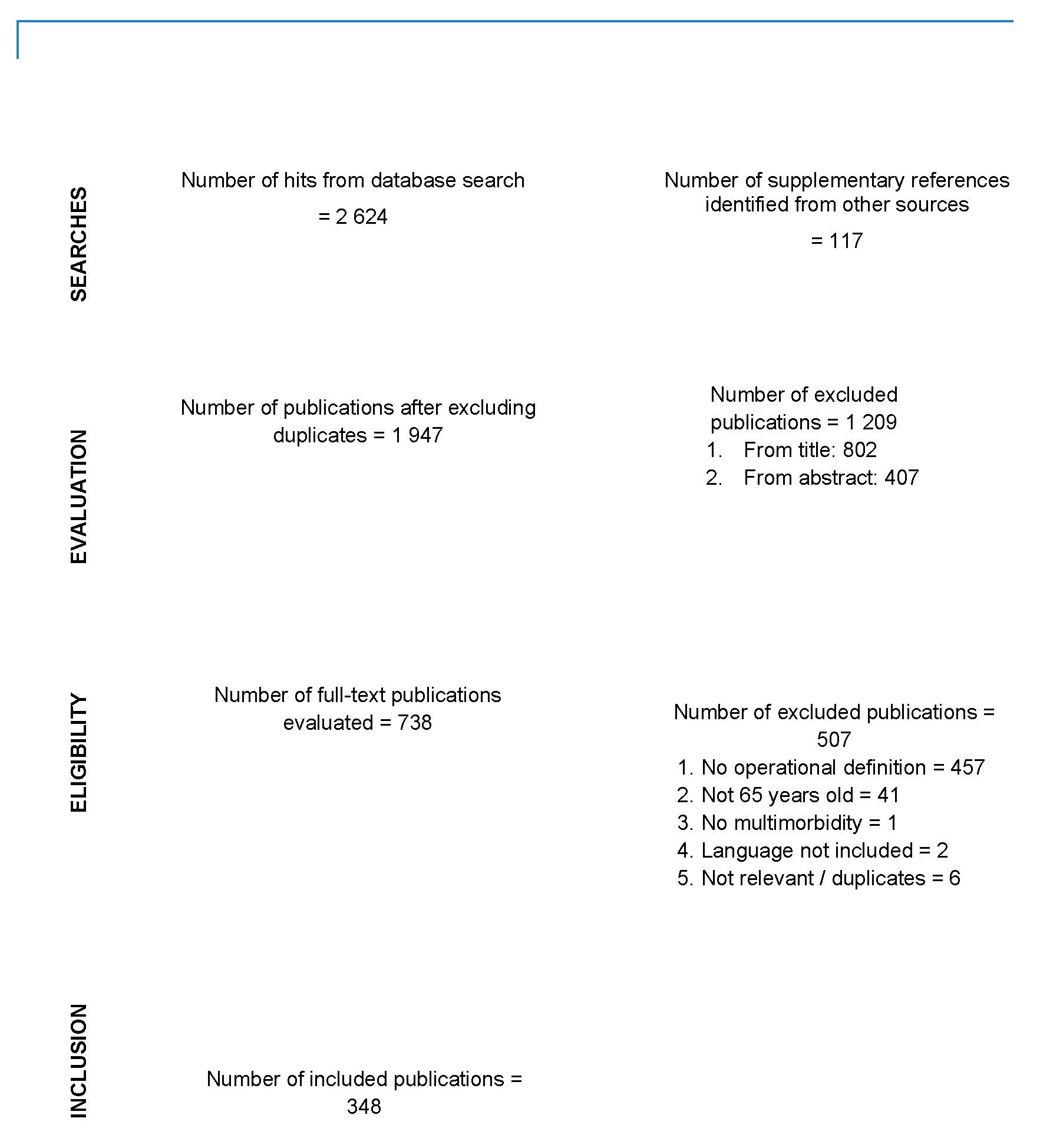
2.2. Searches
2.3. Types of Publications Included
2.4. Selection of Publications
- (1)
- The publication did not provide any operational definition of polypharmacy. For example, defining polypharmacy only as “large number of medications” did not qualify. To be considered operational, the definition could involve a specific number of medications (e.g., 5 or more) or indicate a specific condition (e.g., complex medication regimen with at least one inappropriate medication).
- (2)
- The targeted population did not include people 65 years and over.
- (3)
- The publication referred to polypharmacy used for the treatment of a single medical condition in the absence of multimorbidity.
2.5. Data Extraction
3. Results
3.1. Definitions Retrieved
3.2. Methodological Foundation or Conceptual Basis Underpinning Definitions
4. Discussion
4.1. Examination of the Various Definitions Retrieved (Objective 1)
4.2. Issues Related to the Foundations that Support the Choice of Definitions (Objective 2)
4.3. Contentious Aspects Related to the Definitions of Polypharmacy
4.4. Recommendations to Advance towards Consensus Definitions of Polypharmacy in Multimorbid Older Adults
4.5. Limitations of the Present Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Christensen, L.D.; Reilev, M.; Juul-Larsen, H.G.; Jorgersen, L.M.; Kaae, S.; Andersen, O.; Pottegard, A.; Petersen, J. Use of prescription drugs in the older adult population—A nationwide pharmacoepidemiological study. Eur. J. Clin. Pharmacol. 2019, 75, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Midao, L.; Giardini, A.; Menditto, E.; Kardas, P.; Costa, E. Polypharmacy prevalence among older adults based on survey of health, ageing and retirement in Europe. Arch. Gerontol. Geriatr. 2018, 79, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Canadian Institute for Health Information. Drug Use among Seniors in Canada, 2016; CIHI: Ottawa, ON, Canada, 2018. [Google Scholar]
- Hilmer, S.N.; Gnjidic, D. The effects of polypharmacy in older adults. Clin. Pharmacol. Ther. 2009, 85, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Rankin, A.; Cadogan, C.A.; Patterson, S.M.; Kerse, N.; Cardwell, C.R.; Bradley, M.C.; Ryan, C.; Hugues, C. Intervention to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst. Rev. 2018, 9, CD008165. [Google Scholar] [CrossRef]
- Sirois, C.; Émond, V. Polypharmacy: Methodological challenges to consider. J. Popul. Ther. Clin. Pharmacol. 2015, 22, e285–e291. [Google Scholar]
- Masnoon, N.; Shakib, S.; Kalisch-Ellet, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef]
- Bushardt, R.L.; Massey, E.B.; Simpson, T.W.; Ariail, J.C.; Simpson, K.N. Polypharmacy: Misleading, but manageable. Clin. Interv. Aging 2008, 3, 383–389. [Google Scholar] [CrossRef]
- Frazier, S.C. Health outcomes and polypharmacy in elderly individuals: An integrated literature review. J. Gerontol. Nurs. 2005, 31, 4–11. [Google Scholar] [CrossRef]
- Fulton, M.M.; Allen, E.R. Polypharmacy in the elderly: A literature review. J. Am. Acad. Nurse Pract. 2005, 17, 123–132. [Google Scholar] [CrossRef]
- Sirois, C.; Laroche, M.L.; Guénette, L.; Kröger, E.; Cooper, D.; Émond, V. Polypharmacy in multimorbid older adults: Protocol for a systematic review. Syst. Rev. 2017, 6, 104. [Google Scholar] [CrossRef] [PubMed]
- Age Care Branch of the Department of Human Services (Victoria). Public Sector Residential Age Care Quality of Care Performance Indicator Project Report; The Aged Care Branch of the Department of Human Services: Victoria, Australia, 2004; ISBN 07311 6198 X. [Google Scholar]
- Bjerrum, L.; Rosholm, J.U.; Hallas, J.; Kragstrup, J. Methods for estimating the occurrence of polypharmacy by means of a prescription database. Eur. J. Clin. Pharmacol. 1997, 53, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Waite, L.; Seibel, M.J.; McLachlan, A.J.; Cumming, R.G.; Handelsman, D.J.; Le Couteur, D.G. Polypharmacy cutoff and outcomes: Five or more medicines were used to identify community dwelling older men at risk of different adverse outcomes. J. Clin. Epidemiol. 2012, 65, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.I.; Johnell, K.; Weitoft, G.R.; Thorslund, M.; Fastbom, J. The influence of educational level on polypharmacy and inappropriate drug use: A register-based study of more than 600,000 older people. J. Am. Geriatr. Soc. 2008, 57, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, E.R.; Cafiero, A.C.; Hanlon, J.T. Polypharmacy in elderly patients. Am. J. Geriatr. Pharmacother. 2007, 5, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Jyrkkä, J.; Enlund, H.; Korhonen, M.J.; Sulkava, R.; Hartikainen, S. Polypharmacy status as an indicator of mortality in an elderly population. Drugs Aging 2009, 26, 1039–1048. [Google Scholar] [CrossRef]
- Kaufman, D.W.; Kelly, J.P.; Rosenberg, L.; Anderson, T.E.; Mitchell, A.A. Recent patterns of medication use in the ambulatory adult population of the United States: The Slone survey. JAMA 2002, 287, 337–344. [Google Scholar] [CrossRef]
- Onder, G.; Liporeti, R.; Fialova, D.; Topinkova, E.; Tosato, M.; Danese, P.; Gallo, P.F.; Carpenter, I.; Finne-Soveri, H.; Gindin, J.; et al. Polypharmacy in nursing home in Europe: Results from the SHELTER study. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 698–704. [Google Scholar] [CrossRef]
- Viktil, K.K.; Blix, H.S.; Moger, T.A.; Reikvam, A. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br. J. Clin. Pharmacol. 2007, 63, 187–195. [Google Scholar] [CrossRef]
- Hovstadius, B.; Petersson, G. Factors leading to excessive polypharmacy. Clin. Geriatr. Med. 2012, 28, 159–172. [Google Scholar] [CrossRef]
- Duerden, M.; Avery, T.; Payne, R. Polypharmacy and Medicines Optimization. Making It Safe and Sound. The King’s Fund 2013. Available online: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/polypharmacy-and-medicines-optimisation-kingsfund-nov13.pdf (accessed on 9 May 2016).
- Lai, S.W.; Liao, K.F.; Liao, C.C.; Muo, C.H.; Liu, C.S.; Sung, F.C. Polypharmacy correlates with increased risk for hip fracture in the elderly: A population-based study. Medicine 2010, 89, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, J.; Friedman, C.; Hripcsak, G.; Cabrera, M. Pharmacogenetic polymorphism as an independent risk factor for frequent hospitalizations in older adults with polypharmacy: A pilot study. Pharmgenom. Pers. Med. 2016, 9, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F.; van den Bussche, H.; Wiese, B.; Schön, G.; Koller, D.; Eisele, M.; Glaeske, G.; Scherer, M.; Kaduszkiewicz, H. Impact of geriatric comorbidity and polypharmacy on cholinesterase inhibitors prescribing in dementia. BMC Psychiatry 2011, 11, 190. [Google Scholar] [CrossRef] [PubMed]
- Hopcroft, P.; Peel, N.M.; Poudel, A.; Scott, I.A.; Gray, L.C.; Hubbard, R.E. Prescribing for older people discharged from the acute sector to residential aged-care facilities. Int. Med. J. 2014, 44, 1034–1037. [Google Scholar] [CrossRef] [PubMed]
- Sganga, F.; Landi, F.; Ruggiero, C.; Corsonello, A.; Vetrano, D.L.; Lattanzio, F.; Cherubini, A.; Bernabei, R.; Onder, G. Polypharmacy and health outcomes among older adults discharged from hospital: Results from the CRIME study. Geriatr. Gerontol. Int. 2015, 15, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Sganga, F.; Vetrano, D.L.; Volpato, S.; Cherubini, A.; Ruggiero, C.; Corsonello, A.; Fabbietti, P.; Lattanzio, F.; Bernabei, R.; Onder, G. Physical performance measures and polypharmacy among hospitalized older adults: Results from the CRIME study. J. Nutr. Health Aging 2014, 18, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Maggiore, R.J.; Dale, W.; Gross, C.P.; Feng, T.; Tew, W.P.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Lichtman, S.M.; Gajra, A.; et al. Polypharmacy and potentially inappropriate medication use in older adults with cancer undergoing chemotherapy: Effect on chemotherapy-related toxicity and hospitalization during treatment. J. Am. Geriatr. Soc. 2014, 62, 1505–1552. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.P.; Jamsen, K.M.; Shakib, S.; Singhal, N.; Prowse, R.; Bell, J.S. Polypharmacy cut-point in older people with cancer: How many medictions are too many? Support Care Cancer 2016, 24, 1831–1840. [Google Scholar] [CrossRef]
- Hudhra, K.; Garcia-Caballos, M.; Casado-Fernandez, E.; Jucja, B.; Shabani, D.; Bueno-Cavanillas, A. Polypharmacy and potentially inappropriate prescriptions identified by Beers and STOPP criteria in co-morbid older patients at hospital discharge. J. Eval. Clin. Pract. 2016, 22, 189–193. [Google Scholar] [CrossRef]
- Hofer-Duckelmann, C. Gender and polypharmacotherapy in the elderly: A clinical challenge. Handb. Exp. Pharmacol. 2012, 214, 169–182. [Google Scholar] [CrossRef]
- Sirois, C.; Lunghi, C.; Laroche, M.L.; Maheux, A.; Frini, A. The delicate choice of optimal basic therapy for multimorbid older adults: A cross-sectional survey. Res. Soc. Adm. Pharm. 2019, 15, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Bronskill, S.E.; Gill, S.S.; Paterson, J.M.; Bell, C.M.; Anderson, G.M.; Rochon, P.A. Exploring variation in rates of polypharmacy across long term care homes. J. Am. Med. Dir. Assoc. 2012, 13, 309. [Google Scholar] [CrossRef] [PubMed]
- Wieseler, C. When should iatrogenic polypharmacy be considered a disease? AMA J. Ethics 2018, 20, E1133–E1138. [Google Scholar] [CrossRef] [PubMed]
- Sirois, C.; Simard, M.; Gosselin, E.; Gagnon, M.E.; Roux, B.; Laroche, M.L. Mixed bag “Polypharmacy”: Methodological pitfalls/challenges of this exposure definition. Curr. Epidemiol. Rep. 2019, 6, 390–401. [Google Scholar] [CrossRef]


{kind=link}
| Definition (Cut-Off) | Research (N = 243) n (%) | Clinical Practice (N = 88) n (%) | Public Health (N = 17) n (%) | TOTAL (N = 348) n (%) |
|---|---|---|---|---|
| Number of medications (continuous variable) | 4 (1.7%) [3; 1.3%] | 2 (2.3%) [2; 2.3%] | 1 (5.9%) [1; 5.9%] | 7 (2.0%) [6; 1.7%] |
| Single cut-off | ||||
| ≥2 medications | 1 (0.4%) [0] | 10 (11.4%) [3; 3.4%] | 1 (5.9%) [0] | 12 (3.4%) [3; 0.8%] |
| ≥3 medications | 3 (1.3%) [1; 0.4%] | 8 (9.1%) [5; 5.7%] | 0 | 11 (3.2%) [6; 1.7%] |
| ≥4 medications | 19 (7.8%) [18; 7.4%] | 23 (26.1%) [14; 15.9%] | 1 (5.9%) [1; 5.9%] | 43 (12.4%) [33; 13.6%] |
| ≥5 medications | 115 (47.3%) [110; 45.3%] | 46 (52.3%) [34; 38.6%] | 7 (41.2%) [5; 29.4%] | 168 (48.3%) [149; 42.8%] |
| ≥6 medications | 25 (10.3%) [24; 9.9%] | 13 (14.8%) [5; 5.7%] | 2 (11.8%) [1; 5.9%] | 41 (11.8%) [31; 8.9%] |
| ≥7 medications | 8 (3.3%) [8; 3.3%] | 2 (2.3%) [1; 1.1%] | 1 (5.9%) [1; 5.9%] | 11 (3.2%) [10; 2.9%] |
| ≥8 medications | 6 (2.5%) [6; 2.5%] | 1 (1.1%) [1; 1.1%] | 1 (5.9%) [0] | 8 (2.3%) [7; 2.0%] |
| ≥9 medications | 9 (3.7%) [8; 3.3%] | 8 (9,1%) [4; 4.5%] | 2 (11.8%) [2; 11.8%] | 19 (5,5%) [14; 4.0%] |
| ≥10 medications | 9 (3.7%) [9; 3.7%] | 8 (9.1%) [4; 4.5%] | 5 (29.4%) [5; 29.4%] | 22 (6.3%) [18; 5.2%] |
| >10 medications | 0 | 0 | 3 (17.6%) [1; 5.9%] | 3 (0.9%) [1; 0.3%] |
| ≥20 medications (extreme polypharmacy) | 0 | 1 (1.1%) [0] | 2 (11.8%) [0] | 3 (0.9%) [0] |
| Other threshold (≥13 and ≥17) | 2 (0.8%) [2; 0.8%] | 0 | 0 | 2 (0.5%) [2; 0.5%] |
| Specific threshold according to measured outcome (e.g., 3.5, 4.5, 5.5, 6.5 medications) | 11 (4.5%) [11; 4.5%] | 0 | 0 | 11 (3.2%) [11; 3.2%] |
| Range of medication (e.g., 2–9 or 4–9 medications) | 1 (0.4%) [1; 0.4%] | 1 (1.1%) [1; 1.1%] | 0 [0] | 2 (0.6%) [2; 0.6%] |
| Categorization | ||||
| Number of medications categorized into: 1. 0–4 medications, 5–9 medications, 10–14 medications, ≥15 medications | 1 (0.4%) [1; 0.4%] | 0 | 0 | 1 (0.3%) [1; 0.3%] |
| 2. 0–4 medications, 5–8 medications, ≥9 medications | 1 (0.4%) [1; 0.4%] | 1 (1.1%) [0] | 0 | 2 (0.6%) [1; 0.3%] |
| 3. 0–5 medications, 6–8 medications, 9–11 medications, ≥12 medications | 0 | 1 (1.1%) [1; 1.1%] | 0 | 1 (0.3%) [1; 0.3%] |
| 4. 5–7 medications, 8–10 medications, ≥11 medications | 0 | 0 | 1 (5.9%) [1; 5.9%] | 1 (0.3%) [1; 0.3%] |
| 5. Tertiles: <4 medications, 4–6 medications, ≥7 medications | 1 (0.4%) [1; 0.4%] | 0 | 0 | 1 (0.3%) [1; 0.3%] |
| 6. Quartiles: 0–6 medications, 7–9 medications, 10–13 medications, ≥14 medications | 1 (0.4%) [1; 0.4%] | 0 | 0 | 1 (0.3%) [1; 0.3%] |
| PP: ≥5 medications, EPP: ≥10 medications | 18 (7.4%) [18; 7.4%] | 1 (1.1%) [0] | 2 (11.8%) [1; 5.9%] | 21 (6.0%) [19; 5.5%] |
| PP: ≥6 medications, Hyper-PP: ≥10 medications | 2 (0.8%) [2; 0.8%] | 0 | 2 (0.6%) [2; 0.6%] | |
| PP: 2–9 medications, EPP: ≥10 medications | 0 | 1 (1.1%) [0] | 0 | 1 (0.3%) [0] |
| PP: 5–9 medications, EPP or High-level PP: ≥10 medications | 10 (4.1%) [10; 4.1%] | 0 | 1 (5.9%) [1; 5.9%] | 11 (3.2%) [10; 2.9%] |
| PP: 6–9 medications, EPP: ≥10 medications | 7 (2.9%) [7; 2.9%] | 3 (3.4%) [0] | 0 | 10 (2.9%) [7; 1.0%] |
| PP: 5–10 medications, EPP or Extreme PP: ≥11 medications | 2 (0.8%) [2; 0.8%] | 0 | 0 | 2 (0.6%) [2; 0.6%] |
| PP: 6–10 medications, EPP: ≥11 medications | 1 (0.4%) [1; 0.4%] | 1 (1.1%) [1; 1.1%] | 0 | 2 (0.6%) [2; 0.6%] |
| Minor PP: 2–4 medications, Major PP: ≥5 medications | 3 (1.2%) [2; 0.8%] | 6 (6.8%) [1; 1.1%] | 1 (5.9%) [0] | 10 (2.9%) [3; 0.9%] |
| Mild PP: 1–4 medications, Moderate PP: 5–9 medications, Severe PP: ≥10 medications | 1 (0.4%) [1; 0.4%] | 0 | 0 | 1 (0.3%) [1; 0.3%] |
| Mild PP: 2–3 medications, Moderate PP: 4–5 medications, Severe PP: ≥6 medications | 1 (0.4%) [1; 0.4%] | 3 (3.4%) [1; 1.1%] | 0 | 4 (1.1%) [2; 0.6%] |
| Mild PP: 2–3 medications, Moderate PP: 4–6 medications, Severe PP: ≥7 medications | 1 (0.4%) [1; 0.4%] | 0 | 0 | 1 (0.3%) [1; 0.3%] |
| Mild PP: 7–9 medications, Moderate PP: 10–13 medications, Severe PP: ≥14 medications | 1 (0.4%) [1; 0.4%] | 0 | 0 | 1 (0.3%) [1; 0.3%] |
| Definition | Research (N = 243) n (%) | Clinical Practice (N = 88) n (%) | Public Health (N = 17) n (%) | TOTAL (N = 348) n (%) |
|---|---|---|---|---|
| Inappropriate medications | 4 (1.6%) [4; 1.6%] | 24 (27.3%) [14; 15.9%] | 0 | 28 (8.0%) [18; 5.2%] |
| More medications than clinically indicated or Unnecessary medications (overuse) or presence of medications with no clinical indications or for which a safer alternative drug exists | 8 (3.3%) [6; 2.5%] | 34 (38.6%) [15; 17.0%] | 0 | 42 (12.1%) [21; 6.0%] |
| Excessive medications | 1 (0.4%) [0] | 3 (3.4%) [3; 3.4%] | 0 | 4 (1.1%) [3; 0.9%] |
| Drug-drug interactions or unsuitable combination of drugs | 3 (1.2%) [3; 1.2%] | 3 (3.4%) [1; 1.1%] | 0 | 6 (1.7%) [4; 1.1%] |
| Medication prescribed to treat the side effect of another medication | 0 | 2 (2.3%) [2; 2.3%] | 0 | 2 (0.6%) [2; 0.6%] |
| Drugs that do not match the diagnosis | 0 | 2 (2.3%) [2; 2.3%] | 0 | 2 (0.6%) [2; 0.6%] |
| Duplication of medications | 1 (0.4%) [1; 0.4%] | 9 (10.2%) [5; 5.7%] | 1 (5.9%) [1; 5.9%] | 11 (3.2%) [7; 2.0%] |
| Drugs with lack of effectiveness | 2 (0.8%) [2; 0.8%] | 3 (3.4%) [1; 1.1%] | 0 | 5 (1.4%) [3; 0.9%] |
| Availability of an equally effective, lower-cost alternative | 1 (0.4%) [1; 0.4%] | 1 (1.1%) [1; 1.1%] | 0 | 2 (0.6%) [2; 0.6%] |
| Quantitative + Qualitative elements | ||||
| ≥3 psychotic medications | 0 | 0 | 2 (11.8%) [2; 11.8%] | 2 (0.6%) [2; 0.6%] |
| ≥5 medications and ≥1 psychotropic medication | 1 (0.4%) [1; 0.4%] | 0 | 0 | 1 (0.3%) [1; 0.3%] |
| ≥5 medications, ≥2 narcotics, ≥2 benzodiazepines, ≥3 oral antidiabetic or the use of sildenafil with a nitrate | 0 | 1 (1.1%) [1; 1.1%] | 0 | 1 (0.3%) [1; 0.3%] |
| Other definitions ‡ | 3 (1.2%) [3; 1.2%] | 16 (18.2%) [14; 15.9%] | 4 (23.5%) [4; 23.5%] | 23 (6.6%) [21; 6.0%] |
| Research (N = 236) n (%) | Clinical Practice (N = 82) n (%) | Public Health (N = 17) n (%) | Total (N = 335) n (%) | |
|---|---|---|---|---|
| Type of medication included | ||||
| Prescription ‡ | 141 (59.7) | 30 (36.6) | 14 (82.4) | 185 (55.2) |
| OTC/complementary/Alternative medications § | 44 (18.6) | 14 (17.1) | 3 (17.6) | 61 (18.2) |
| No information reported on the type of medications included | 97 (41.1) | 52 (63.4) | 3 (17.6) | 152 (45.4) |
| Type of use included | ||||
| Chronic, regular or long-term drugs | 53 (22.5) | 12 (14.6) | 9 (52.9) | 74 (22.1) |
| As needed or short-term drugs¶ | 27 (11.4) | 1 (1.2) | 3 (17.6) | 31 (9.3) |
| No information reported on type of use | 169 (71.6) | 70 (85.4) | 7 (41.2) | 246 (73.4) |
| Administration route included | ||||
| Topical, dermatologic /eye or nose drops/mouthwash†† | 12 (5.1) | 0 | 2 (11.8) | 14 (4.2) |
| Injectable agents ‡‡ | 4 (1.7) | 0 | 1 (5.9) | 5 (1.5) |
| No information reported on type of administration route | 209 (88.6) | 81 (98.8) | 12 (70.6) | 302 (90.1) |
| Medications-related issues | ||||
| Combination drugs counted as more than one medication | 11 (4.7) | 0 | 2 (11.8) | 13 (3.9) |
| Method to define exposure | ||||
| Simultaneous use at a given time (simultaneous) | 117 (49.6) | 30 (36.6) | 6 (35.3) | 153 (45.7) |
| Simultaneous use over a period of time (continuous) | 24 (10.2) | 3 (3.7) | 2 (11.8) | 29 (8.7) |
| Total number of medications over a period (cumulative) | 15 (6.4) | 4 (4.9) | 9 (52.9) | 28 (8.4) |
| Other definitions | 19 (8.1) | 1 (1.2) | 0 | 20 (6.0) |
| Not reported specifically | 71 (30.1) | 47 (57.3) | 4 (23.5) | 122 (36.4) |
| Research (N = 240) † n (%) | Clinical Practice (N = 72) † n (%) | Public Health (N = 17) n (%) | Total (N = 329) † n (%) | |
|---|---|---|---|---|
| Theoretical/Methodological | 28 (11.7%) | 1 (1.4%) | 6 (35.3%) | 35 (10.6%) |
| Reference to previous work | 108 (45%) | 42 (58.3%) | 7 (41.2%) | 157 (47.7%) |
| None provided | 119 (49.5%) | 30 (41.7%) | 5 (29.4%) | 154 (46.8%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sirois, C.; Domingues, N.S.; Laroche, M.-L.; Zongo, A.; Lunghi, C.; Guénette, L.; Kröger, E.; Émond, V. Polypharmacy Definitions for Multimorbid Older Adults Need Stronger Foundations to Guide Research, Clinical Practice and Public Health. Pharmacy 2019, 7, 126. https://doi.org/10.3390/pharmacy7030126
Sirois C, Domingues NS, Laroche M-L, Zongo A, Lunghi C, Guénette L, Kröger E, Émond V. Polypharmacy Definitions for Multimorbid Older Adults Need Stronger Foundations to Guide Research, Clinical Practice and Public Health. Pharmacy. 2019; 7(3):126. https://doi.org/10.3390/pharmacy7030126
Chicago/Turabian StyleSirois, Caroline, Nelia Sofia Domingues, Marie-Laure Laroche, Arsène Zongo, Carlotta Lunghi, Line Guénette, Edeltraut Kröger, and Valérie Émond. 2019. "Polypharmacy Definitions for Multimorbid Older Adults Need Stronger Foundations to Guide Research, Clinical Practice and Public Health" Pharmacy 7, no. 3: 126. https://doi.org/10.3390/pharmacy7030126