
The Challenge of Medication-Induced Dry Mouth in Residential Aged Care


1
Sir John Walsh Research Institute, Faculty of Dentistry, University of Otago, Dunedin 9054, New Zealand
2
Department of Public Health, Wellington School of Medicine, Faculty of Medicine, University of Otago, Wellington 6021, New Zealand
3
School of Pharmacy, University of Queensland, Brisbane 4102, Australia
*
Author to whom correspondence should be addressed.
Pharmacy 2021, 9(4), 162; https://doi.org/10.3390/pharmacy9040162
Submission received: 24 August 2021
/
Revised: 29 September 2021
/
Accepted: 30 September 2021
/
Published: 1 October 2021
(This article belongs to the Special Issue Improving Geriatric Care through Pharmacy Practice)
Abstract
:With a reported prevalence between 20% and 30%, dry mouth is more common among older people than any other age group. The major risk factor for dry mouth is polypharmacy. Older people take more medications than any other age group, not only for symptomatic relief of various age-associated chronic diseases, but also to reduce the likelihood of the complications that may arise from those conditions. Most aged care residents take even more medications than older people who are living in their own homes. The greater the number of medications taken, the greater the associated anticholinergic burden, and the more likely it is that the individual will suffer from dry mouth. The condition not only affects the dentition and ability to wear dentures, but also the sufferers’ quality of life. Treating dry mouth is a considerable challenge for clinicians. As medication use is by far the most important risk factor, there is a need for pharmacists, doctors and dentists to work together to prevent this from occurring. Medication review and deprescribing is a key strategy, but there have not yet been any randomised control trials of its efficacy in reducing the occurrence of dry mouth.
1. Introduction
Dry mouth is particularly common in residential aged care, reported in about one in three residents in a recent New Zealand (NZ) national survey [1]. The aim of this paper is to raise pharmacists’ awareness of the problem and to suggest ways in which they can work with dental personnel to ameliorate this.
2. Occurrence and Impact of Dry Mouth
Dry mouth is common among older people, affecting between 20% and 30% of those over 65 [2,3]. There are two aspects to the condition. Salivary gland hypofunction (SGH) is the state of having low salivary flow, while xerostomia refers to the subjective sensation of dry mouth. Thus, the former is a sign, and the latter a symptom (or set of symptoms). The extent to which they coincide is controversial, but the epidemiological evidence suggests that they are far from concordant [4].
By no means a trivial condition, dry mouth has a considerable impact on sufferers (Table 1). Not only is it one of the major contributors to impaired oral-health-related quality of life (OHRQoL) among adults of any age [5,6,7,8,9,10,11], but sufferers of dry mouth have difficulty eating and swallowing, halitosis, poor sleep, and considerably higher tooth decay rates [12], along with difficulty wearing dental prostheses (partial or complete dentures).
3. Causes of Dry Mouth
Medications are the most important risk factor for chronic dry mouth [2]. Although a small proportion of people suffer from the condition as a result of autoimmune conditions such as Sjögren’s syndrome, or as a side-effect of radiotherapy for head/neck cancer, more than 95% of the population burden of dry mouth arises as a result of medication use.
Drugs that are putative causes of dry mouth are referred to as “xerogenic”. Lists of xerogenic medications have been published [13,14,15] but are of limited utility because they are too inclusive and largely based on case reports. Medication classes for which there is sound evidence of xerogenicity include antidepressants, anticholinergics, opioids and bronchodilators (Table 2).
Other factors being equal, people taking large numbers of different medications have higher rates of dry mouth. That is, the greater the number and dosage of drugs being taken, the greater the severity of dry mouth (and other side-effects). In the NZ national survey of residential aged care, xerostomia was more common among those taking 5–9 medications and more so in those on 10+ medications, as well as in those taking antidepressants or bronchodilators [1]. Other studies have also observed differences in the occurrence of dry mouth by the total number of medications taken [16,17]. This leads into the notion of polypharmacy.
4. Polypharmacy
Polypharmacy is defined as the taking of five or more medications, whether they have been prescribed or purchased over the counter or online [18]. Since ageing is associated with progressively greater multi-morbidity (concurrent long-term health problems), older people tend to take a lot of medications [19]. A population-based study of community-dwelling Australians aged 70 or older reported the prevalence of polypharmacy to be 36%, with higher rates among older age groups [20]. Polypharmacy is most evident in residential aged care, where, for example, a national survey of facilities in NZ found the prevalence of polypharmacy to be 73% (and found that one in five residents were taking 10 or more medications, and no-one was taking none) [21]. Antihypertensives, analgesics and antireflux drugs were the most common types of medication.
Polypharmacy has become more common in recent decades, reflecting increased prescribing based on multiple clinical practice guidelines, each focusing on a single condition [19]. In many cases, of course, the number of medications being taken by an individual is entirely appropriate and safe, but polypharmacy is also a known risk factor for drug-related harms, falls, cognitive decline and frailty [19,22,23]. It also increases the risk of drug interactions [24], medication error [19], and the chance of important conditions going untreated [25]. Moreover, some medications taken by older people may no longer have any therapeutic or preventive effect. Health systems also suffer from the economic impacts of unnecessary prescribing and having to manage the consequent adverse events [26,27]. Recognition of the perils of polypharmacy has forged the practice of deprescribing, which is the planned and supervised process of dose reduction or stopping of medication that might be causing harm or is no longer beneficial (https://deprescribing.org/what-is-deprescribing, accessed on 20 August 2021).
5. Treating Dry Mouth and Reducing Unnecessary Medication Use
Dry mouth is difficult to treat. Broadly speaking, the therapeutic options are palliation (treating the symptoms), stimulation (increasing salivary gland output) or regeneration (growing new secretory tissue). The latter remains a theoretical possibility at this stage, while stimulation has had mixed outcomes. Palliative approaches can be inconsistent and unpredictable, as shown in Cochrane reviews [28,29,30], which have examined the evidence for the different therapeutic approaches. There is strong evidence for the efficacy of stimulation using systemic pilocarpine (in individually titrated doses of, typically, 2–5 mg) in treating dry mouth arising from Sjögren’s syndrome or from therapeutic radiation for head/neck cancer treatment, but those states comprise only a very small proportion of the population burden arising from dry mouth [31].
Given that the bulk of the population-attributable risk for dry mouth arises from medications (and polypharmacy in particular)—and that the evidence for stimulatory approaches to treating medication-related dry mouth is not strong—there is a need to examine alternative ways to prevent or ameliorate it by reducing the occurrence of polypharmacy in residential aged care.
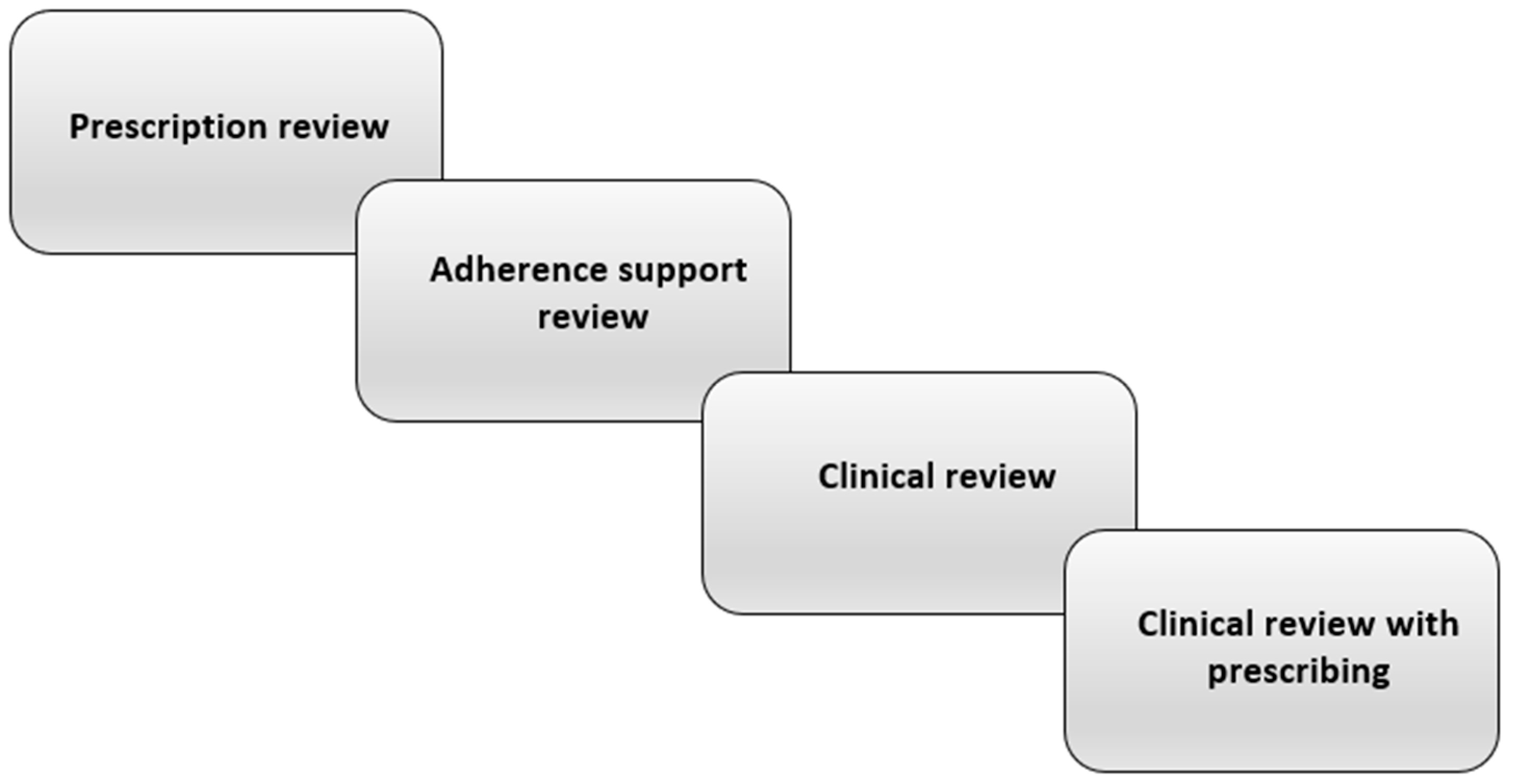
Accordingly, interventions aiming to reduce the occurrence of dry mouth through medication review and deprescribing (and thereby reducing polypharmacy) would be a key strategy with important benefits, not only for older people and residential aged care facilities, but also for the wider health system. What is medication review? It involves a systematic, critical assessment of a patient’s medicines, which aims to arrive at an agreement with the patient on treatment, optimising the impact of medicines, and minimising medication-related problems and waste. An essential part of that process is medication reconciliation, the assembling of an accurate and complete inventory of all medications taken, regardless of source [32]. Medication review itself can have four levels [33] (Figure 1). (a) Prescription review considers the technical features of the prescription itself. (b) Adherence support review is undertaken with the patient present and focuses on medication-taking, particularly knowledge and adherence. (c) Clinical review involves the clinical notes and the patient, considering their use of medications with respect to their clinical condition. (d) Clinical review with prescribing is an extension of the former but including the authority to prescribe. Levels (c) and (d) closely involve the patient’s physician; overall, the focus should be on assessing the medication’s risks and benefits, and initiating deprescribing for those where the former outweigh the latter.
A useful distinction in undertaking medication review can be made between drugs being taken for control of disease and/or symptoms and those taken for preventive reasons, despite a degree of overlap [34]. In a recent investigation of medications causing dry mouth in a national survey of residential aged care in New Zealand, the types most strongly associated with dry mouth were antidepressants, corticosteroids, anticholinergics and bronchodilators [1]. These are prescribed largely for symptom control rather than disease control in older people, and so any deprescribing moves would need to be informed by considering the benefit:harm ratio and the likelihood of withdrawal reactions or disease rebound on cessation, along with patient and physician preferences [35].
In the context of dry mouth, this medication review aims to identify and eliminate specific drug categories which are known to be associated with the condition. Pharmacists can play an important role in the above process, particularly through working together with dentists, since medical practitioners may be more likely to act upon recommendations made by two practitioners from different fields.
6. The Need for Interventional Studies in Residential Aged Care
To date, there have been no interventional studies examining the efficacy of medication review for reducing the severity of dry mouth in residential aged care. What form could such an investigation take? The gold standard design would be a parallel randomised control study, where residents are randomly allocated to either medication review or some form of placebo consultation. There is the possibility of more nuanced comparisons, with recommendations from either a pharmacist alone or a combination of a pharmacist and a dentist. Allocation would need to be done at the level of the individual resident. Alternatively, allocation could be done at the facility level, but that would require a larger study and complicate the analyses because the unit of analysis would need to be the facility. A design which could be used in that case is the stepped wedge cluster randomised trial, treating each facility as a cluster, with no cluster exposed at first, then clusters randomly assigned to cross from the control (no intervention) to the intervention. By the end of the trial, all clusters would have been exposed to both the control and intervention conditions [36].
The outcome variables could be (a) the facility’s acceptance of deprescribing recommendations, and (b) dry mouth among residents. Dry mouth symptoms (and unstimulated salivary flow, if resources permit) would be measured at baseline (pre-intervention) and at follow-up (post-intervention). Given the chronic nature of dry mouth and the exposure to the medications responsible, the length of time between the intervention and the follow-up assessment would need to be six months, to allow for (i) adequate tapering and “wash-out” of the responsible medications, and (ii) recovery of the salivary system. For measuring xerostomia symptoms, an established and validated scale such as the Summated Xerostomia Inventory (SXI) would be useful [37], because it assigns participants to a place on a continuum of dry mouth severity, enabling the computation of an effect size for the observed change in symptoms arising from the intervention. Given that the minimally important difference (MID) for the SXI is 4, the proportion improving by the MID in the intervention and control groups would be able to be compared. Similarly, unstimulated flow rates pre- and post-intervention could be compared, along with effect sizes.
Such a design is, of course, not the only one which could be used to determine the efficacy of medication review and deprescribing in treating dry mouth, and it would be worth considering and investigating the feasibility of other approaches. It is hoped that this review raises awareness of the issue of dry mouth in residential aged care and provides some impetus towards the development of multidisciplinary collaborations between pharmacists and dentists, which aim to ameliorate and further investigate the problem.
7. Conclusions
Pharmacists and health practitioners are likely to be aware of the role of polypharmacy in falls and confusion, but they may not be cognisant of drug-induced dry mouth, its significance for oral health, and its negative impact on quality of life. Thus, there is a need for pharmacy and oral health personnel to work more closely—along with general practitioners, geriatricians and nurses—to raise awareness of xerostomia and ensure that sufferers are appropriately managed and advised. Practitioners should routinely enquire about dry mouth when assessing residents, and specific enquiries about dry mouth should be included in the standard medical histories for new admissions. Given that the major risk factor for dry mouth is polypharmacy, pharmacists, doctors and dentists should work together to prevent this from occurring, or at least reduce its severity. Key strategies are medication review and deprescribing. There is also a need for interventional studies to determine the efficacy of those strategies in reducing the occurrence of dry mouth.
Author Contributions
All authors contributed substantially to the work reported. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Thomson, W.M.; Ferguson, C.A.; Janssens, B.E.; Kerse, N.M.; Ting, G.S.; Smith, M.B. Xerostomia and polypharmacy among dependent older New Zealanders: A national survey. Age Aging 2021, 50, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Agostini, B.A.; Cericato, G.O.; Silveira, E.R.; Nascimento, G.G.; Costa, F.S.; Thomson, W.M.; Demarco, F.F. How common is dry mouth? Systematic review and meta-regression analysis of prevalence estimates. Braz. Dent. J. 2018, 29, 606–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamieson, L.M.; Thomson, W.M. Xerostomia: Its prevalence and associations in the adult Australian population. Aust. Dent. J. 2020, 65, S67–S70. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.; Wolff, A.; Narayana, N.; Dawes, C.; Aframian, D.; Lynge Pedersen, A.M.; Vissink, A.; Aliko, A.; Sia, Y.W.; Joshi, R.K.; et al. World Workshop on Oral Medicine VI: A systematic review of medication-induced salivary gland dysfunction: Prevalence, diagnosis, and treatment. Clin. Oral Investig. 2016, 22, 365–382. [Google Scholar] [CrossRef] [PubMed]
- Locker, D. Dental status, xerostomia and the oral health-related quality of life of an elderly institutionalized population. Spec. Care Dent. 2003, 23, 86–93. [Google Scholar] [CrossRef]
- Gerdin, E.W.; Einarson, S.; Jonsson, M.; Aronsson, K.; Johansson, I. Impact of dry mouth conditions on oral health-related quality of life in older people. Gerodontology 2005, 22, 219–226. [Google Scholar] [CrossRef]
- Thomson, W.M.; Lawrence, H.P.; Broadbent, J.M.; Poulton, R. The impact of xerostomia on oral-health-related quality of life among younger adults. Health Qual. Life Outcomes 2006, 4, 86. [Google Scholar] [CrossRef] [Green Version]
- Ikebe, K.; Matsuda, K.; Morii, K.; Wada, M.; Hazeyama, T.; Nokubi, T.; Ettinger, R.L. Impact of dry mouth and hyposalivation on oral health-related quality of life of elderly Japanese. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 216–222. [Google Scholar] [CrossRef]
- Owens, J.; Gibson, B.J.; Periyakaruppiah, K.; Baker, S.R.; Robinson, P.G. Impairment effects, disability and dry mouth: Exploring the public and private dimensions. Health 2014, 18, 509–525. [Google Scholar] [CrossRef]
- Enoki, K.; Ikebe, K.; Matsuda, K.; Yoshida, M.; Maeda, Y.; Thomson, W.M. Influence of xerostomia on oral health-related quality of life in the elderly: A 5-year longitudinal study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 716–721. [Google Scholar] [CrossRef]
- Benn, A.M.L.; Broadbent, J.M.; Thomson, W.M. Occurrence and impact of xerostomia among dentate adult New Zealanders: Findings from a national survey. Aust. Dent. J. 2015, 60, 362–367. [Google Scholar] [CrossRef]
- Thomson, W.M.; Spencer, A.J.; Slade, G.D.; Chalmers, J.M. Is medication a risk factor for dental caries among older people? Evidence from a longitudinal study in South Australia. Community Dent. Oral Epidemiol. 2002, 30, 224–232. [Google Scholar] [CrossRef]
- Grad, H.; Grushka, M.; Yanover, L. Drug induced xerostomia: The effects and treatment. J. Can. Dent. Assoc. 1985, 4, 296–300. [Google Scholar]
- Handelman, S.L.; Baric, J.M.; Espeland, M.A.; Berglund, K.L. Prevalence of drugs causing hyposalivation in an institutionalized geriatric population. Oral Surg. Oral Med. Oral Pathol. 1986, 62, 26–31. [Google Scholar] [CrossRef]
- Sreebny, L.M.; Schwartz, S.S. A reference guide to drugs and dry mouth—2nd edition. Gerodontology 1997, 14, 33–47. [Google Scholar] [CrossRef]
- Smidt, D.; Torpet, L.A.; Nauntofte, B.; Heegaard, K.M.; Pedersen, A.M.L. Associations between labial and whole salivary flow rates, systemic diseases and medications in a sample of older people. Community Dent. Oral Epidemiol. 2010, 38, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Johanson, C.N.; Osterberg, T.; Lernfelt, B.; Ekstrom, J.; Birkhed, D. Salivary secretion and drug treatment in four 70-year-old Swedish cohorts during a period of 30 years. Gerodontology 2015, 32, 202–210. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Couteur, D.G.; McLachlan, A.J.; Hilmer, S.N. Polypharmacy in older people. When should you deprescribe? MedicineToday 2016, 17, 16–24. [Google Scholar]
- Page, A.T.; Falster, M.O.; Litchfield, M.; Pearson, S.; Etherton-Beer, C. Polypharmacy among older Australians, 2006–2017: A population-based study. Med. J. Aust. 2019, 211, 71–75. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, C.A.; Thomson, W.M.; Smith, M.B.; Kerse, N.M.; Peri, K.; Gribben, B. Medication taking in a national sample of dependent older people. Res. Soc. Admin. Pharm. 2020, 16, 299–307. [Google Scholar] [CrossRef]
- Fried, T.R.; Leary, J.; Towle, V.; Goldstein, M.K.; Trentalange, M.; Martin, D.K. Health Outcomes Associated with Polypharmacy in Community-Dwelling Older Adults: A Systematic Review. J. Am. Geriatr. Soc. 2014, 62, 2261–2272. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez-Valencia, M.; Izquierdo, M.; Cesari, M.; Casas-Herrero, A.; Inzitari, M.; Martinez-Velilla, N. The relationship between frailty and polypharmacy in odler people: A systematic review. Br. J. Clin. Pharmacol. 2018, 84, 1432–1444. [Google Scholar] [CrossRef] [Green Version]
- Guthrie, B.; Makubate, B.; Hernandez-Santiago, V.; Dreischulte, T. The rising tide of polypharmacy and drug-drug interactions: Population database analysis 1995–2010. BMC Med. 2015, 13, 74. [Google Scholar] [CrossRef] [Green Version]
- Kuijpers, M.A.J.; van Marum, R.J.; Egberts, A.C.G.; Jansen, P.A.F.; OLDY Study Group. Relationship between polypharmacy and underprescribing. Br. J. Clin. Pharmacol. 2007, 65, 130–133. [Google Scholar] [CrossRef] [Green Version]
- Morgan, S.G.; Hunt, J.; Rioux, J.; Proulx, J.; Weymann, D.; Tannenbaum, C. Frequency and cost of potentially inappropriate prescribing for older adults: A cross-sectional study. CMAJ Open 2016, 4, E346–E351. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, M.N.; O’Sullivan, D.; Gallagher, P.F.; Eustace, J.; Byrne, S.; O’Mahony, D. Prevention of Hospital-Acquired Adverse Drug Reactions in Older People Using Screening Tool of Older Persons’ Prescriptions and Screening Tool to Alert to Right Treatment Criteria: A Cluster Randomized Controlled Trial. J. Am. Geriatr. Soc. 2016, 64, 1558–1566. [Google Scholar] [CrossRef]
- Furness, S.; Worthington, H.V.; Bryan, G.; Birchenough, S.; McMillan, R. Interventions for the management of dry mouth: Topical therapies. Cochrane Database Syst. Rev. 2011, 12, CD008934. [Google Scholar] [CrossRef]
- Furness, S.; Bryan, G.; McMillan, R.; Birchenough, S.; Worthington, H.V. Interventions for the management of dry mouth: Non-pharmacological interventions. Cochrane Database Syst. Rev. 2013, 9, CD009603. [Google Scholar]
- Riley, P.; Glenny, A.M.; Hua, F.; Worthington, H.V. Pharmacological interventions for preventing dry mouth and salivary gland dysfunction following radiotherapy. Cochrane Database Syst. Rev. 2017, 7, CD012744. [Google Scholar] [CrossRef] [Green Version]
- United States Surgeon General. The 2020 Surgeon General’s Report on Oral Health; Department of Health and Human Services: Washington, DC, USA, 2021.
- Geurts, M.M.E.; Talsma, J.; Brouwers, J.R.B.J.; de Gier, J.J. Medication review and reconciliation with cooperation between pharmacist and general practitioner and the benefit for the patient: A systematic review. Br. J. Clin. Pharmacol. 2012, 74, 16–33. [Google Scholar] [CrossRef] [Green Version]
- Hatah, E.; Braund, R.; Tordoff, J.; Duffull, S.B. A systematic review and meta-analysis of pharmacist-led fee-for-services medication review. Br. J. Clin. Pharmacol. 2014, 77, 102–115. [Google Scholar] [CrossRef] [Green Version]
- Scott, I.A.; Hilmer, S.N.; Reeve, E.; Potter, K.; Le Couteur, D.; Rigby, D.; Gnjidic, D.; Del Mar, C.B.; Roughead, E.E.; Page, A.; et al. Reducing inappropriate polypharmacy: The process of deprescribing. JAMA Intern. Med. 2015, 175, 827–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huiskes, V.J.B.; Burger, D.M.; van den Ende, C.H.M.; van den Bemt, B.J.F. Effectiveness of medication review: A systematic review and meta-analysis of randomized controlled trials. BMC Fam. Pract. 2017, 18, 5. [Google Scholar] [CrossRef] [Green Version]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: Rationale, design, analysis, and reporting. BMJ 2015, 350, h391. [Google Scholar] [CrossRef] [Green Version]
- Thomson, W.M.; van der Putten, G.-J.; de Baat, C.; Ikebe, K.; Matsuda, K.; Enoki, K.; Hopcraft, M.; Long, G. Shortening the Xerostomia Inventory. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 322–327. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
The levels of pharmacist-led medication review [33].
Figure 1.
The levels of pharmacist-led medication review [33].


{kind=link}
Table 1.
Overview of dry mouth’s impacts on sufferers.
| Physical and Functional Impacts | Psychosocial Impacts |
|---|---|
| Difficulty eating/swallowing | Symptoms of dry mouth |
| More tooth decay | Compromised quality of life |
| Problems with dentures | Halitosis |
| Infections—salivary glands, mucosa | Poor sleep |
| Compromised taste sensation | Distress |
Table 2.
The main medication classes known to be associated with dry mouth (adapted from Villa et al. [4]).
Table 2.
The main medication classes known to be associated with dry mouth (adapted from Villa et al. [4]).
| Medication Type | Mechanism of Action |
|---|---|
| Gastrointestinal agents e.g., Hyoscine, hyoscyamine, belladonna alkaloids, atropine | Block muscarinic receptors |
| Antiemetics e.g., prochlorperazine, | Block dopamine D2, serotonin types 2–4, histamine type 1 and acetylcholine receptors |
| Appetite suppressants/stimulants e.g., Phentermine, sibutramine | Inhibit CNS uptake of norepinephrine, serotonin and dopamine |
| Cardiovascular agents e.g., Atenolol, metoprolol, prazosin, clonidine | Block α1- and β2-adrenergic receptors |
| Urological e.g., Oxybutynin, propantheline, darifenacin, solifenacin, tolterodine, mirabegron | Block muscarinic receptors and α1-adrenergic receptors |
| Muscle relaxants Cyclobenzaprine, orphenadrine | Act as α1-adrenergic receptor agonists, and H2 histamine blockers |
| Analgesics e.g., Opioids, tramadol, gabapentin, pregabalin. | Block noradrenaline reuptake in the CNS and so inhibit the salivary reflex arc |
| Anticonvulsants e.g., Carbamazepine | Act centrally to reduce neurotransmitter release |
| Sedatives—benzodiazepines & Z-drugs e.g., Zolpidem, zopiclone | Enhance GABA effect in CNS, reduce the salivary secretory reflex, and block muscarinic, α1- and β2-adrenergic receptors |
| Antipsychotics e.g., Olanzapine, clozapine, amisulpiride | Block neurotransmitter uptake (various) |
| Antidepressants e.g., Tricyclics (e.g., amitriptyline), SSRIs and SNRIs | Anticholinergic; increase serototinn and noradrenaline at the synaptic cleft. |
| Bronchodilators e.g., Ipratropium, tiotropium, salbutamol, salmeterol, eformoterol, umeclidinium | 2 types: β agonists and antimuscarininc, Block muscarinic receptors M1 and M3, |
| Antihistamines- sedating only e.g., Diphenhydramine, doxylamine, chlorpheniramine, promethazine | Central inhibitory action on histamine type 1 and muscarinic receptors |
| CNS Stimulants e.g., Caffeine, pseudoephedrine, amphetamines | α1 and α2 agonists. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Thomson, W.M.; Smith, M.B.; Ferguson, C.A.; Moses, G. The Challenge of Medication-Induced Dry Mouth in Residential Aged Care. Pharmacy 2021, 9, 162. https://doi.org/10.3390/pharmacy9040162
AMA Style
Thomson WM, Smith MB, Ferguson CA, Moses G. The Challenge of Medication-Induced Dry Mouth in Residential Aged Care. Pharmacy. 2021; 9(4):162. https://doi.org/10.3390/pharmacy9040162
Chicago/Turabian StyleThomson, William Murray, Moira B. Smith, Catherine Anna Ferguson, and Geraldine Moses. 2021. "The Challenge of Medication-Induced Dry Mouth in Residential Aged Care" Pharmacy 9, no. 4: 162. https://doi.org/10.3390/pharmacy9040162
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.